
Abstract
Context:
Anecdotal reports and preliminary clinical observations suggest potential benefits of homeopathic medicines in hemorrhoids, but high-quality evidence remains limited.
Objective:
To evaluate whether individualized homeopathic medicinal products (IHMPs) are superior to placebo in reducing anorectal symptom severity and improving quality of life over 3 months in adults with hemorrhoids, and to assess their safety and tolerability.
Design:
Three-month, double-blind, randomized (1:1), placebo-controlled trial.
Setting:
Surgery, PG3, and research outpatients of a tertiary homeopathic medical college hospital in West Bengal, India.
Patients:
One hundred and thirty-four adults with grade I–III hemorrhoids.
Intervention:
IHMPs (verum; n = 67) or identical-looking placebos (control; n = 67) both administered alongside standard concomitant care including sitz baths, pelvic floor exercises, and dietary advice.
Main Outcome Measures:
The primary outcome was the change in the Anorectal Symptom Severity and Quality-of-Life (ARSSQoL) total score over 3 months. Secondary outcomes included ARSSQoL subscales, numeric rating scales (NRSs), and EQ-5D-5L questionnaire and visual analog scale. Outcomes were assessed monthly for up to 3 months. The primary analysis compared model-based estimates of change over time between groups using repeated measures analysis of variance; the secondary analyses comprised multivariate linear mixed models, Bayesian hierarchical modeling, and sensitivity analyses under intention-to-treat and per-protocol frameworks.
Results:
After 3 months, IHMPs demonstrated significantly greater improvement than placebo in ARSSQoL total (mean group difference −6.5, 95% confidence interval −8.7, −4.2; p < 0.001), with large effect sizes. Most ARSSQoL subscales, NRSs, and EQ-5D-5L scores favored IHMPs. Multivariate and Bayesian analyses confirmed consistent intervention-by-time effects, with a high probability of directional superiority for IHMPs in symptom reduction and self-rated health, while sensitivity analyses showed the findings to be robust to protocol deviations. Kent’s repertory was the most frequently used in remedy selection. Nitricum acidum emerged as the most effective remedy. No treatment-related serious adverse events were observed.
Conclusion:
In this randomized, double-blind trial, IHMPs were associated with greater reductions in the ARSSQoL improvements in quality of life compared with placebo over 3 months. Although the magnitude and consistency of effects across multiple analytic approaches suggest potential clinical relevance, the absence of a validated minimal clinically important difference for the ARSSQoL warrants cautious interpretation. Further independent replications and methodological refinement of outcome thresholds are needed.
Introduction
Hemorrhoidal disease is a common chronic anorectal condition that significantly affects symptom burden and quality of life in adults. Hemorrhoids are classified as internal and external, based on their location with respect to the dentate line. 1 The vascular cushions’ expansion and distal displacement are indicative of hemorrhoids. With an estimated prevalence rate ranging from 4.4% to 39%, it is the most prevalent proctological condition, with a significant medical, social, and economic issue.2–4 An online survey among adults of different nationalities across the world has found the prevalence of hemorrhoids to be around 11%, with most suffering from low-severity disease (71%). 5 Though constipation is believed to be one of the major risk factors, hemorrhoids and constipation have different epidemiological characteristics. 6 Bleeding, pain, pruritus, fecal seepage, prolapse, and mucus discharge are the commonly encountered symptoms. 7 A systematic literature review has pointed out that constipation, straining during bowel movements, incomplete bowel emptying, and hard stool are all associated with an increased risk of hemorrhoids, but a high total fiber intake is associated with a decreased risk. 8 Recurrence rates following surgery or phlebotonics ranged from 0% to 56.5%. Risk factors often play an important role in recurrence. First-line treatment usually includes changing one’s diet to include enough liquids and fiber consumption, preventing straining, and minimizing extended periods spent on the toilet. 9 Dietary and lifestyle modifications are considered the best preventive measures. 10
Treatment options primarily depend on the type and severity of the hemorrhoids, the patient’s preference, and the medical professional’s experience. In the treatment of hemorrhoids, postprocedural pain and disease recurrence continue to be the most difficult issues. Several treatment approaches have been used thus far, including rubber band ligation, cryotherapy, sclerotherapy, and infrared coagulation. A lot of published trials have poor quality.11,12
According to one study, hemorrhoids were one of the most common clinical diseases seen in homeopathic hospital outpatients in West Bengal, India. The condition was successfully treated with a success rate ranging from 60.3% to 82.3%. 13 In a single-arm clinical trial with classical homeopathic treatment, patients with hemorrhoids were found to be improved considerably as per symptom severity and anoscopic scores. 14 When compared with a placebo in acute attacks, a single-blind randomized controlled trial (RCT) demonstrated the efficacy of homeopathic treatment for hemorrhoids. 15 In another recent RCT, individualized homeopathic medicinal products (IHMPs) were superior to placebo in the short-term treatment of hemorrhoids of grades I–III. 16
This trial was designed as a replication of the study by Koley et al. 16 The primary objective of the study was to detect the differences between IHMPs and placebo in the Anorectal Symptom Severity and Quality-of-Life questionnaire (ARSSQoL) 17 scores following a 3-month intervention. The ARSSQoL numeric rating scales (NRSs), the EQ-5D-5L questionnaire (EQQ), and the EQ visual analog scales (EQ-VASs) 18 were also compared for differences. In addition, the safety and tolerability of IHMPs were assessed by keeping track of adverse and significant adverse events.
Methods
Hypothesis
Based on prior preliminary and randomized evidence, we hypothesized that IHMPs, when administered alongside standard concomitant care, would result in greater reductions in anorectal symptom severity and improvements in health-related quality of life compared with placebo over 3 months. We further hypothesized that IHMPs would be safe and well-tolerated, with no excess of adverse events compared with placebo.
Trial design
In the surgery, PG3, and research outpatient departments of D. N. De Homoeopathic Medical College and Hospital in West Bengal, India, a 3-month, double-blind, randomized (1:1), placebo-controlled study with two parallel arms was carried out.
Trial subjects
Patients with primary hemorrhoids (ICD-10-CM code K64.8) grades I–III, diagnosed by a conventional surgeon, with or without anitis, for at least 3 months, regardless of sex, age between 18 and 65, and literacy in English, Bengali, and/or Hindi were the inclusion criteria. Patients who were already receiving conservative treatment for hemorrhoids were to be enrolled after ceasing all medication completely and following a 4-week wash-out period if the patient’s problems persisted or reappeared, and they met the eligibility requirements. Exclusion criteria were the patients who refused to give consent to participate in the trial and refused to follow trial procedures; were too ill for consultation; had grade IV hemorrhoids; anal fissure and fistula; hypertrophic anal papillae; inflammatory bowel disease; coagulation disorders; a history of leukemic disorders; patients with obstruction of portal circulation; patients in need of immediate surgical intervention or who had recently undergone rectal surgery; patients with unstable mental health diagnoses; patients with uncontrolled or life-threatening systemic illnesses affecting the quality of life or any organ failure; patients with substance abuse and/or dependence, pregnant, puerperal, and nursing women; patients who concurrently participated in any other clinical trial; and the patients undergoing homeopathic treatment for any chronic disease within last 6 months.
Interventions
The subjects were randomized to receive either control (identical-looking placebos plus concurrent care) or verum (IHMPs plus concomitant care). Following homeopathic principles, IHMPs were prescribed in centesimal potencies (30, 200, and 1000cH), one to four doses, once to twice daily as needed, depending on the specific needs of the patients and conditions. Until the next scheduled visit, known (uncoded) placebos were administered. Each dosage consisted of six to eight cane sugar globules (no. 20), treated with the prescribed medication (kept in 90% v/v ethanol), and administered orally on an empty stomach. The dosage was repeated based on each patient’s needs. Patients were instructed to suck the globules rather than swallow them whole and to refrain from eating, drinking, brushing their teeth, or smoking for 30 min after taking the globules. Moreover, the trial subjects were told not to use coffee, mint, or any other food or beverage that contained medication during the experiment. A 3-month follow-up period was given to every participant. It was not possible to arrange coded LM (50 millesimal) potencies due to infrastructure limitations. Similar to verum, placebos were administered to the control group. Six to eight nonmedicated cane sugar globules (no. 20) wet with rectified spirit made up the placebo. The medications and placebos were repackaged in matching glass bottles, labeled with the name, potency, and code of the medication, and dispensed based on a list of random numbers. The blinded pharmacist was the only one with access to the coded bottles; the trial subjects were not. All of the trial subjects, regardless of the codes they were given, were urged to take a sitz bath at least once a day, practice good hygiene locally, treat constipation or diarrhea, and stop bad defecation habits such as skipping meals, ignoring the urge to pass stool, spending a lot of time in the bathroom, straining, and not exercising. They were instructed to drink plenty of water, eat foods high in natural fiber (such as whole-grain bread, ripe papaya, unpeeled fruits, and green leafy vegetables), and refrain from using a lot of spices. Hahnemann Publishing Company Pvt. Ltd., a company accredited by Good Manufacturing Practices in Kolkata, was the source of all the medications. All the medicines were prepared and dispensed in accordance with the standards of the Homeopathic Pharmacopoeia of India.
Case-taking was conducted using a structured classical homeopathic approach, encompassing presenting complaints, associated modalities, concomitant symptoms, past medical history, and relevant mental and general characteristics. All consultations followed a standardized case-record format to ensure consistency across trial subjects. Repertorization was performed in the majority of the cases using Kent’s repertory as the primary reference, supplemented by other standard repertories when clinically indicated. Rubrics were selected based on characteristics, individualizing symptoms, with pathological symptoms considered supportive rather than decisive. Final remedy selection was guided by repertorial analysis in conjunction with materia medica confirmation and agreement among three homeopaths. Repertorization was performed using software (Rapid Aid to Drug Aimed Research (RADAR®), version 10.0.028 (ck), Archibel 2009, Belgium, and HOMPATH ZOMEO®, version 3.0, Mumbai, India). Potency selection followed predefined principles based on symptom intensity, susceptibility, chronicity, and prior response to treatment. Centesimally prepared potencies were used throughout the study, with potency escalation considered only in cases of partial response without aggravation. Remedy repetition or change was guided by prespecified clinical criteria, including symptom progression, emergence of new characteristic symptoms, lack of response after adequate observation, or sustained improvement. Changes were made only when clinically indicated and were implemented using matched-coded preparations to maintain blinding. As needed, subsequent visits involved adjusting the medications, potencies, and dosages following the traditional homeopathic principles. Three of the homeopaths had been teaching classical homeopathy for more than 20 years and held a master’s degree in homeopathy. The remaining homeopaths were the organization’s postgraduate trainees. Each of the participating homeopaths was a member of their state council. Before trial initiation, practitioners underwent protocol-specific training to standardize case-taking, repertorization, and decision-making principles. Regular monitoring meetings were held to ensure adherence to the study protocol, while allowing individualized prescribing within the defined framework. Follow-up visits and weekly phone calls guaranteed adherence to suggestions. A medication accountability journal was kept, which tracked the dosages taken, globules returned, and adherence to the accompanying care instructions. Regarding following the recommended concomitant care measures and following the prescribed treatment regimens, there was no documented difference in compliance across the groups. Initial consultations and follow-up assessments, including case-taking and documentation, were conducted by postgraduate trainees in homeopathy using a standardized case-record format. All cases were subsequently reviewed by a panel of three senior homeopathic physicians. Final decisions regarding remedy selection, potency, repetition, or modification were made only after confirmation by at least one senior physician. This supervisory framework ensured consistency in prescribing while preserving individualized case management. Discrepancies between trainee assessments and senior physician recommendations were resolved through consensus discussion. All prescriptions were reviewed and confirmed by the senior homeopathic physicians before dispensing; no prescription was implemented without senior confirmation. This confirmation applied to initial prescriptions as well as to any subsequent changes in remedy, potency, or repetition during follow-up.
Outcome measures
The ARSSQoL questionnaire total served as the main indicator of success. 17 It was a self-administered, prevalidated questionnaire that was offered in Hindi and English to patients. It comprised 16 questions with four-point Likert scale response categories ranging from 0 to 3 (never = 0, slightly = 1, moderately = 2, extremely = 3). A total score was calculated by adding up all of the question answers; this score may be anything between 0 and 48. Higher scores were associated with more pain and a lower standard of living. Questionnaires were divided into five domains: psychological impact (numbers 1–10); symptom intensity (numbers 2, 3, 5, 7, 8, 16); concern (numbers 6–9); itching (number 4); and bleeding (number 1) within each domain. The baseline and up to3 months of monthly measurements were made of the scores. The EQQ and the ARSSQoL NRSs were the secondary outcomes. Six 0–10 NRSs (0 = no complaints; 10 = maximum severity) on the ARSSQoL questionnaire allowed trial subjects to score the degree of six hemorrhoidal symptoms: bleeding, pain, itching, heaviness, mucus discharge, and swelling. 18 For a maximum of 3 months, the scores were tested at baseline and once each month. By email, the primary author granted the necessary authorization for the use of the questionnaire. Five factors made up the EQQ: mobility, self-care, regular activities, pain/discomfort, and anxiety/depression. There were five levels for each dimension: low issues (1), moderate problems (2), severe problems (3), extreme problems (4), and no problems (1). 18 As a result, the raw total score varied from 5 to 25. The patient’s self-rated health was measured using the EQ-VAS, which produced a vertical VAS with endpoints identified as the poorest and best possible health. The VAS ranged from 0 to 100. The license required to use the tool was received from the EuroQol Research Foundation on August 9, 2021, under registration number 43724.
Timeline
For a maximum of 3 months, all the results were measured at monthly intervals.
Sample size
The minimal clinically important difference (MCID) data of the ARSSQoL questionnaire were not estimated. Consequently, the sample size calculation was based on effect size assumptions derived from prior randomized trials in hemorrhoids using the same outcome measure. The lack of a validated MCID should be considered when interpreting the clinical relevance of the observed effects. Available data from the conducted trials of homeopathy in hemorrhoids by Koley et al. lead to a very small sample size of 10 (5 × 2) only. As replication of the said trial was aimed at, from a rational point of view, a similar study size was targeted. Accounting for an expected attrition rate of up to 5%, assuming a medium effect size (Cohen’s d) of 0.5 of IHMPs against placebos, 1:1 allocation, and detecting a target difference of 1.4 between two independent means of ARSSQoL scores after 3 months of intervention through two-tailed independent sample t-test, a study with 2 × 67 trial subjects would result in 82% power based on a two-sided significance level of 5%.
Randomization
The randomization sequence was generated using a computer-based random number algorithm by an independent statistician not involved in participant recruitment, treatment, outcome assessment, or data analysis. A block size of 10 was used to create a random sequence using the permuted block randomization approach in a 1:1 manner under strict confidentiality using the Research Randomizer (https://randomizer.org/). To accommodate the final sample size, an additional block of size 4 was generated. The full randomization list was accessible only to a designated pharmacy coordinator responsible for investigational product preparation and was not available to investigators, treating physicians, outcome assessors, or trial subjects. To reduce selection bias, trial subjects were randomized evenly (1:1) to the verum and control groups. By eliminating unneeded variables, the block randomization method has the potential to homogenize the data and produce a consistent distribution of the crucial parameters connected to the outcome. Once a participant was assigned to a code, that code did not change during the 3-month intervention; therefore, crossover was not permitted. This random number chart was given to the blinded pharmacist to distribute medication. Another impartial third party coded similar amber-colored glass vials as “1” or “2,” denoting either medications or identical-looking placebos with varying potencies (30, 200, and 1000CH). The random number chart determined which participant would get the vials in a sequential order. After the data set was frozen, the codes were cracked after the trial. The correspondence between numerical codes and treatment identity was recorded in a master code file, which was securely stored and inaccessible to study personnel.
Blinding
Throughout the experiment, everyone involved—trial subjects, treating physicians, pharmacists, outcome assessors, and data entry operators—remained blinded. By asking the trial subjects which group they thought they were in, the blinding was verified both before and after the study. The case files were kept private by the research assistants once the final prescription was determined. The blinded pharmacist was tasked with dispensing the prescribed medications from the coded vials and maintaining assigned codes following the random number chart. He had access only to participant codes and vial numbers and did not know whether a given code represented verum or placebo. The medications were not disclosed to the trial subjects; instead, they were written on a piece of paper, sealed inside an opaque envelope, and given to the pharmacist. Verum and placebo medications were prepared in advance in identical vials that were indistinguishable in appearance, labeling, taste, and packaging. Each vial was assigned a unique sequential identification number corresponding to the randomization sequence. Medications were dispensed strictly in numerical order according to participant enrollment, ensuring that treatment allocation remained concealed. To prevent mix-ups, verum and placebo vials were stored in separate, access-restricted containers and handled exclusively by the designated pharmacy coordinator. Double-checking procedures were implemented during labeling and dispensing, whereby vial numbers were cross-verified against the dispensing log before release. Investigators and clinical staff received only the sequential vial number and had no access to treatment codes. A predefined emergency unblinding procedure was established for individual trial subjects in the event of a medical emergency where knowledge of the treatment assignment was deemed essential for patient management. Sealed code-break envelopes corresponding to each vial number were maintained by the principal investigator and could be opened only after documented justification.
Allocation concealment
Trial subjects were screened, enrolled, and assigned serial numbers by blinded postgraduate trainees and registration counter workers. The blinded homeopaths then conducted interviews with the blinded subjects to determine the prescription. As a result, allocation concealment was accomplished by keeping the random number sequence a secret from both the trial recruiters and the treating physicians. The vials were prepared in advance according to the computer-generated randomization list and were sequentially numbered, ensuring that trial subjects were assigned to treatment groups in the predetermined order and that allocation concealment was maintained throughout the trial. Sequential numbering was implemented by an independent pharmacist not involved in participant enrollment, assessment, or data analysis. No instances of accidental unblinding or medication mix-up were reported, and no emergency code-breaks were required during the study.
Statistical methods
The intention-to-treat (ITT) strategy was used, and predicted values using linear regression models were used to fill in the missing values. Shapiro–Wilk tests, Q-Q plots, and histograms were used to analyze the distribution of the data. Descriptive statistics were used to present sociodemographic information or baseline confounders. Data distribution was visualized using violin plots at different time points (Supplementary Fig. S1). Descriptive statistics were used to present the intragroup changes, including the mean and 95% confidence intervals (CIs). The primary analysis evaluated between-group differences in the ARSSQoL total score over time using a two-way repeated measures analysis of variance (ANOVA), with treatment group (IHMPs vs. placebo) as the between-subject factor and time (baseline, months 1–3) as the within-subject factor. The group × time interaction term was used to estimate differential change over time between groups. Model-based estimates derived from this analysis constituted the primary inferential results. Analyses were conducted under an ITT framework, with missing values imputed using linear regression models. In addition, independent sample t-tests were used to compare the mean estimates obtained separately for each month. The explanation is that ANOVA is superior to t-tests in terms of lowering inflated type I errors caused by multiple testing. The effect sizes were reported using partial eta-squared (small effect, 0.01–0.059; moderate effect, 0.06–0.137; and large effect, > 0.138) and Cohen’s d (little effect, 0.2; medium effect, 0.5; large effect, 0.8). A two-tailed p value< 0.05 was deemed statistically significant. Effect sizes were visualized using forest plots (Supplementary Fig. S2). A multivariate linear mixed model (MLMM) was employed, accounting for the fixed effects for intervention (homeopathy vs. placebo), time, and outcome, as well as all possible two- and three-way interactions. Degrees of freedom were estimated using Satterthwaite’s method. Post hoc pairwise comparisons were performed using estimated marginal means to determine group differences at each specific time point. A Bayesian hierarchical linear mixed model was implemented using Markov Chain Monte Carlo sampling (4 chains and 2000 iterations) to evaluate the longitudinal treatment effect. The model utilized a Gaussian likelihood with a three-way interaction between intervention (homeopathy vs. placebo), time (baseline to month 3), and outcomes. Convergence was verified using the Gelman–Rubin diagnostic (R-hat ≈ 1.00 for all parameters) and effective sample size. Inference was based on the median of the posterior distribution and the 95% highest density interval. The probability of direction (pd) was also reported, which represents the probability that a treatment effect exists in the observed direction. To ensure the reliability of the findings, a sensitivity analysis was conducted comparing two different patient populations at the 3-month endpoint. The ITT analysis included the total randomized sample (n = 134). The per-protocol (PP) analysis (n = 131) excluded three participants identified as protocol violators. A result was considered robust if the magnitude of the effect size and the statistical significance (CI excluding zero) remained consistent across both analysis sets. The most effective medicines were visualized using radar charts. The data were analyzed using the Statistical Package for Social Sciences (version 23.0; IBM Corp., IBM SPSS Statistics for Windows, Armonk, NY: USA) and using R, version 4.5.1 (2025-06-13 ucrt), The R Foundation for Statistical Computing, Platform: x86_64-w64-mingw32/x64, Vienna, Austria, within the RStudio environment, version 2026.01.0392.
Adverse events
During the trial, the trial subjects were instructed by the investigators to report any adverse drug reactions, suspected adverse reactions (SARs), unexpected adverse events, unexpected SAR, treatment-emergent adverse events, and serious adverse events (SAEs). 19 In addition, they were instructed to report any unpleasant aggravations (homeopathic, medicinal, or disease symptoms) either in person or over the phone. Homeopathic aggravations were defined a priori as a transient worsening of presenting symptoms with a simultaneous feeling of well-being following remedy administration and were actively monitored at each follow-up visit. Adverse events were also actively monitored at each follow-up visit and through spontaneous participant reporting. All adverse events were recorded irrespective of their suspected relationship to the investigational product and were classified by type, severity (mild, moderate, and severe), and seriousness. Investigators assessed relatedness to the study intervention. SAEs were predefined and monitored throughout the trial duration. As “rescue remedies,” some (uncoded) IHMPs were applied to treat acute illnesses that were most likely unconnected to the trial. Although the additional homeopathic treatment may have confounded the trial-specific medications, these were “short-acting” remedies chosen based on the “acute totality” of the patients, so it was unlikely that they would influence the trial-specific medications’ effects.20,21 The treating physicians reevaluated the patients after the acute stages of the illness had passed. Either the identical trial medication with the same code was given again, or different medications were administered based on the patient’s symptomatology and what the doctors deemed to be appropriate for the patient’s situation.
Trial reporting
It adhered to the CONSORT and RedHot guidelines22,23 (Supplementary Data S1and S2: CONSORT and RedHot checklists).
Results
Participant flow
A total of 168 patients were screened according to the prespecified inclusion and exclusion criteria. Thirty-four were excluded for various reasons; 134 met the eligibility criteria and were enrolled subsequently. Baseline sociodemographic and outcome data were obtained, and the patients were randomized to either IHMPs plus concomitant care (verum; n = 67) or identical-looking placebos plus concomitant care (control; n = 67). The outcome data were recorded at baseline and every month up to 3 months. During treatment, 3 dropped out, 1 in the verum and 2 in the control; 131 completed the trial (Fig. 1).
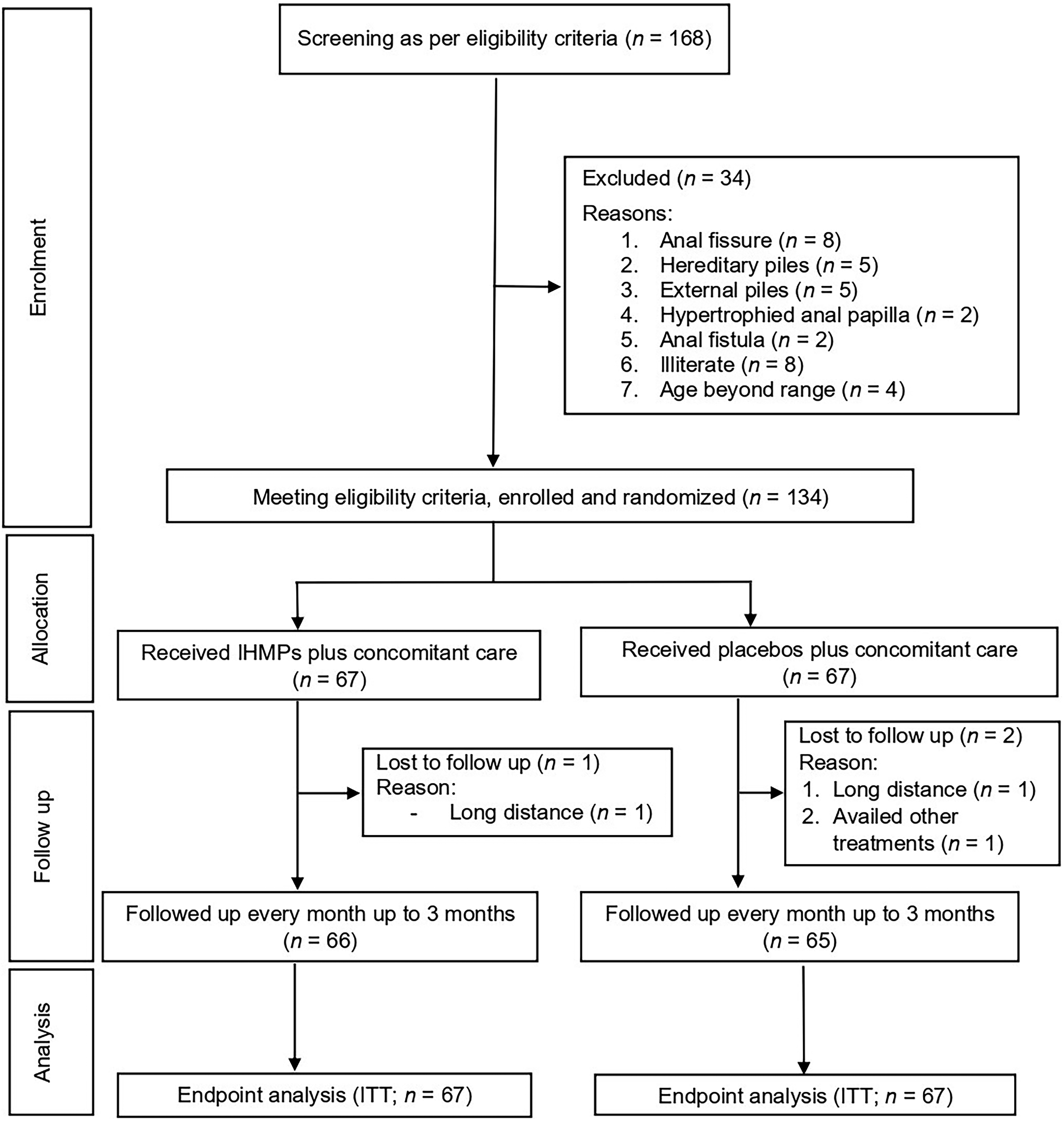
CONSORT study flow.
Recruitment
From the end of April 2022 until mid-May 2023, a total of 134 patients were enrolled in the trial. Follow-up of the last enrolled participant was completed by mid-August 2023.
Baseline data
The distribution of the sociodemographic factors has been presented in Table 1.
Comparison of the Sociodemographic Characteristics Between Groups at Baseline (n = 134)
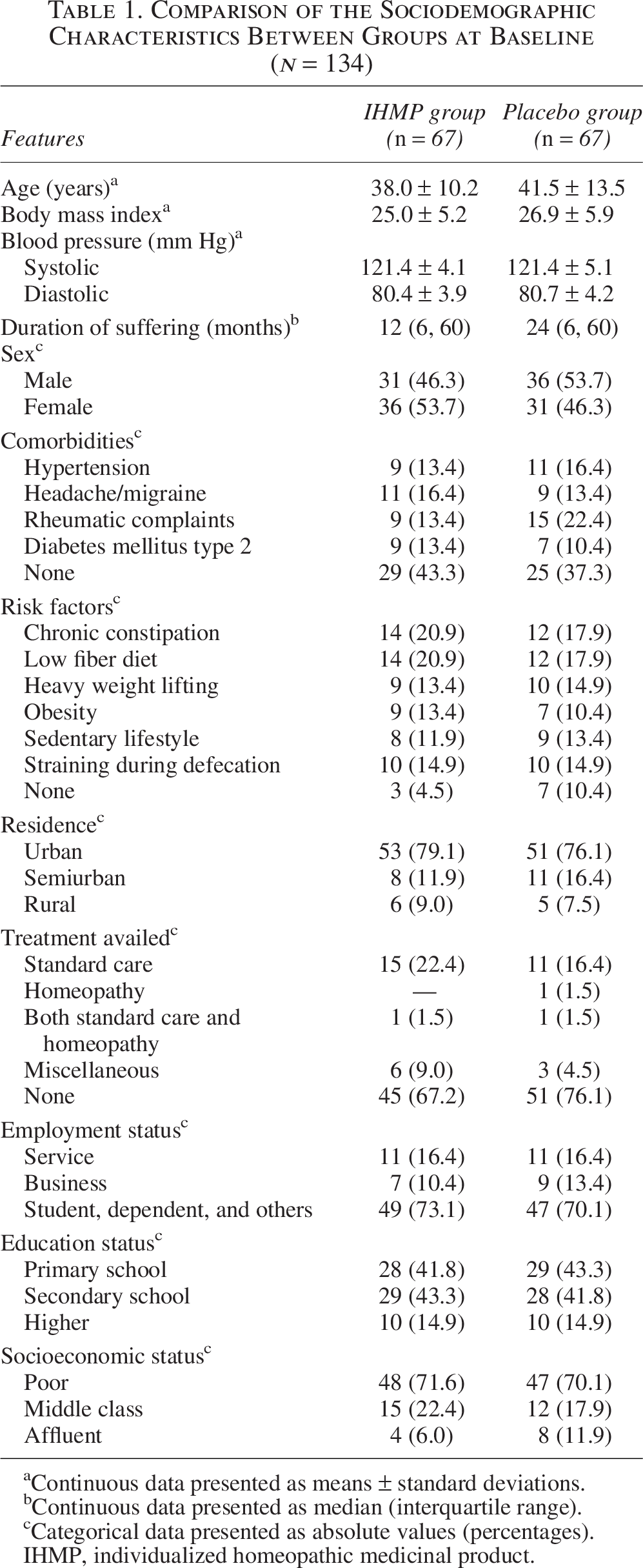
Continuous data presented as means ± standard deviations.
Continuous data presented as median (interquartile range).
Categorical data presented as absolute values (percentages).
IHMP, individualized homeopathic medicinal product.
Numbers analyzed
Outcomes from 66/67 trial subjects in the IHMP group and 65/67 trial subjects in the placebo group were complete, respectively; the remainder dropped out of the trial. The data from all 134 randomized trial subjects (IHMPs: n = 67; placebos: n = 67) were entered into the final analyses (Fig. 1).
Estimation of outcomes
ARSSQoL: After 3 months of intervention, between-group differences in ARSSQoL total scores over time were statistically significant with large effect size, as demonstrated by the group × time interaction in the repeated measures ANOVA, indicating greater reductions in the IHMP group compared with placebo (mean group difference −6.5, 95% CI –8.7, –4.2, Cohen’s d = 0.980, p < 0.001; F1,132 = 15.765, partial η2 = 0.107, p < 0.001). Although a validated MCID for the ARSSQoL total score is not currently available, the observed between-group mean difference (−6.5 points on a 0–48 scale) exceeded conventional distribution-based thresholds and was associated with large effect sizes, suggesting potential clinical relevance. Still, in the absence of a validated MCID for the ARSSQoL, the clinical significance of the 6.5-point between-group difference cannot be conclusively established. Except for the itching subscale (p = 0.126, Cohen’s d = 0.307, partial η2 = 0.004), the rest of the subscales revealed statistical significance favoring IHMPs against placebos: bleeding (P = 0.008, Cohen’s d = 0.526, partial η2 = 0.013), psychological impact (p < 0.001, Cohen’s d = 0.999, partial η2 = 0.105), symptom severity (p < 0.001, Cohen’s d = 1.056, partial η2 = 0.125), and concern (p = 0.024, Cohen’s d = 0.442, partial η2 = 0.007) (Table 2). ARSSQoL-NRS: All the NRSs measuring the severity of symptoms yielded statistical significance favoring IHMPs against placebos with medium to large effect sizes: bleeding (p = 0.002, Cohen’s d = 0.580, partial η2 = 0.017), pain (p < 0.001, Cohen’s d = 0.931, partial η2 = 0.096), itching (p = 0.027, Cohen’s d = 0.446, partial η2 = 0.005), heaviness (p = 0.002, Cohen’s d = 0.517, partial η2 = 0.036), discharge (p = 0.025, Cohen’s d = 0.399, partial η2 = 0.006), and swelling (p < 0.001, Cohen’s d = 0.733, partial η2 = 0.073) (Table 3). EQ-5D-5L: Both the EQ-5D-5L VASs and questionnaire scores demonstrated statistical significance favoring IHMPs against placebos: VASs (mean group difference 15.0, 95% CI 8.4, 21.6, d = 0.784, p < 0.001; F1,132 = 10.014, partial η2 = 0.071, p = 0.002) and questionnaire scores (mean group difference −2.1, 95% CI –3.0, –1.2, d = 0.889, p < 0.001; F1,132 = 10.946, partial η2 = 0.077, p = 0.001) (Table 4). MLMM outcomes: A highly significant three-way interaction was identified between intervention, time, and outcome (F6,1188 = 25.18, P < 0.001), indicating that the therapeutic effect of homeopathy over time varied significantly across the different quality-of-life scales. A significant overall intervention-by-time interaction was also observed (F3,1188 = 5.33, p = 0.001). At baseline, there was no significant difference between the groups in the ARSSQoL total (p = 0.994). However, the groups began to diverge by month 2, with the homeopathy group showing significantly lower (improved) scores compared with placebo (mean difference = −5.82, p = 0.005). This effect was maintained and strengthened at month 3, where homeopathy demonstrated a significant clinical advantage (mean difference = −6.47, p = 0.002). For the EQVAS, homeopathy showed a rapid and highly significant improvement compared with the placebo. While groups were comparable at baseline (p = 0.058), the homeopathy group reported significantly higher health status by month 1 (p < 0.001). By the end of month 3, the homeopathy group’s EQVAS scores were 15.03 points higher than the placebo group (p < 0.001). In contrast, the EQQ did not show a statistically significant difference between groups at any time point throughout the 3-month follow-up (p > 0.05), suggesting that while trends favored the intervention, they did not reach statistical significance on this specific scale (Supplementary Tables S1and S2, Supplementary Fig. S3). Bayesian hierarchical model: It confirmed that homeopathy had a high probability of clinical superiority over placebo for symptom reduction (ARSSQoL) and general health status (EQVAS) in patients with piles, while EQQ scores remained statistically comparable between groups. By month 3, the posterior difference in ARSSQoL scores was −6.47 (95% CI −10.1, −2.9). The pd was 99.98%, indicating a near-certainty that the homeopathy group experienced a greater reduction in symptoms compared with the placebo group. The homeopathy group showed a credible improvement starting as early as month 1 in EQVAS. By month 3, the posterior difference was + 15.03 (95% CI +10.5, + 19.8, pd = 100%). This suggested that patients in the homeopathy group reported significantly higher quality of life than those in the placebo group. Conversely, the model showed high uncertainty regarding the EQQ scale. While the median difference favored homeopathy (−2.11), the 95% credible interval crossed zero ([−5.5, 1.2]), and the pd was only 83.4% (Supplementary Tables S3and S4, Supplementary Fig. S4). Sensitivity analysis: It demonstrated that the study findings were highly robust. The exclusion of protocol violators in the PP analysis resulted in only negligible changes to the effect size estimates across all three outcomes. For the ARSSQoL, Cohen’s d shifted only slightly from 0.988 in the ITT set to 0.977 in the PP set, maintaining a “large” effect size in both scenarios. Across all measures, the 95% CIs for both the ITT and PP analyses remained entirely above the zero-threshold. This indicated that the statistical significance of homeopathy’s superiority over placebo was reliable and consistent and not dependent on the inclusion or exclusion of protocol violators (Supplementary Table S5, Supplementary Fig. S5).
Comparison of the ARSSQoL Questionnaire Scores Between Groups at Baseline and at Different Time Points (n = 134)
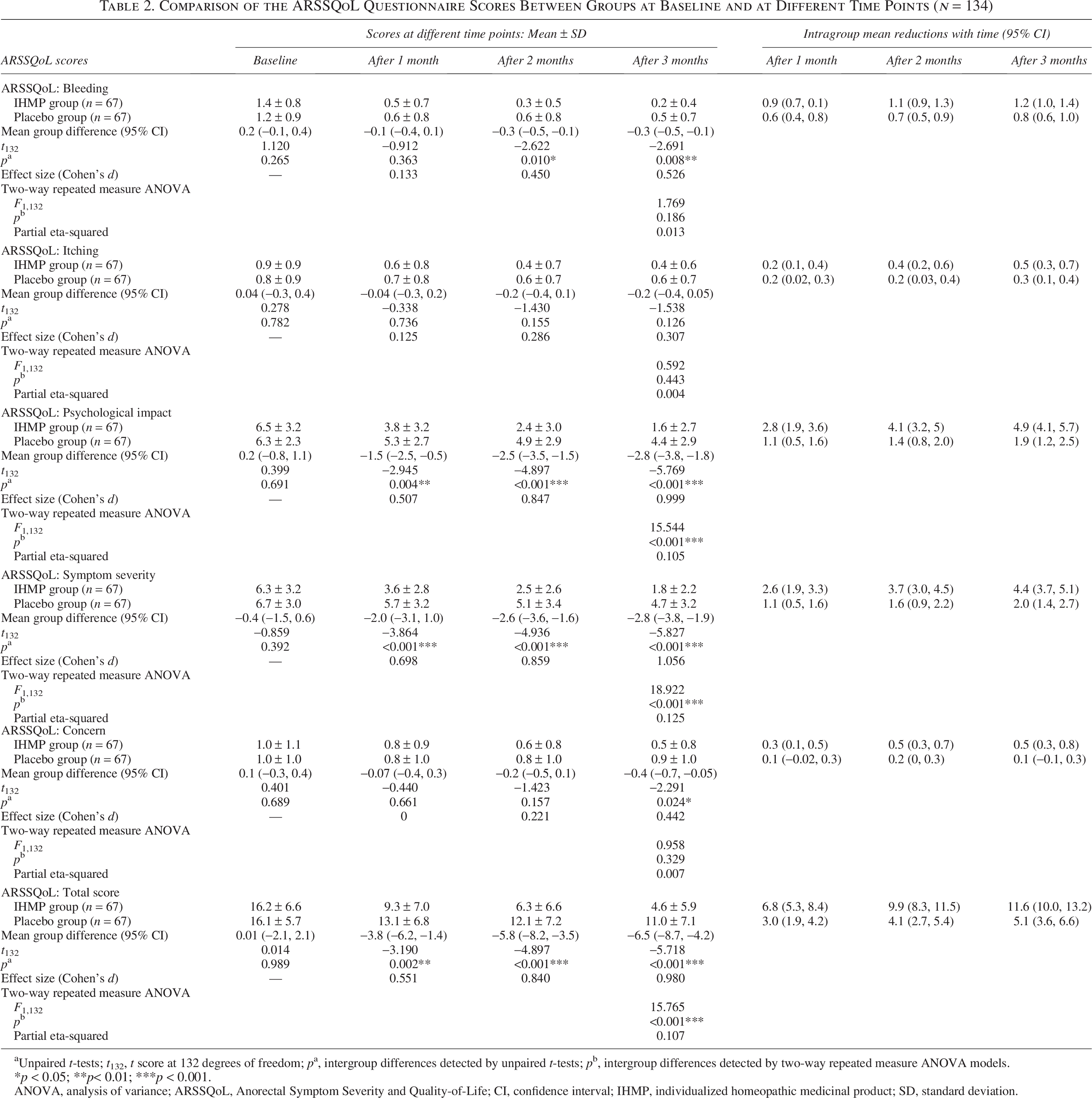
Unpaired t-tests; t132, t score at 132 degrees of freedom; pa, intergroup differences detected by unpaired t-tests; pb, intergroup differences detected by two-way repeated measure ANOVA models.
*p < 0.05; **p< 0.01; ***p < 0.001.
ANOVA, analysis of variance; ARSSQoL, Anorectal Symptom Severity and Quality-of-Life; CI, confidence interval; IHMP, individualized homeopathic medicinal product; SD, standard deviation.
Comparison of the ARSSQoL NRSs Between Groups at Baseline and at Different Time Points (n = 134)
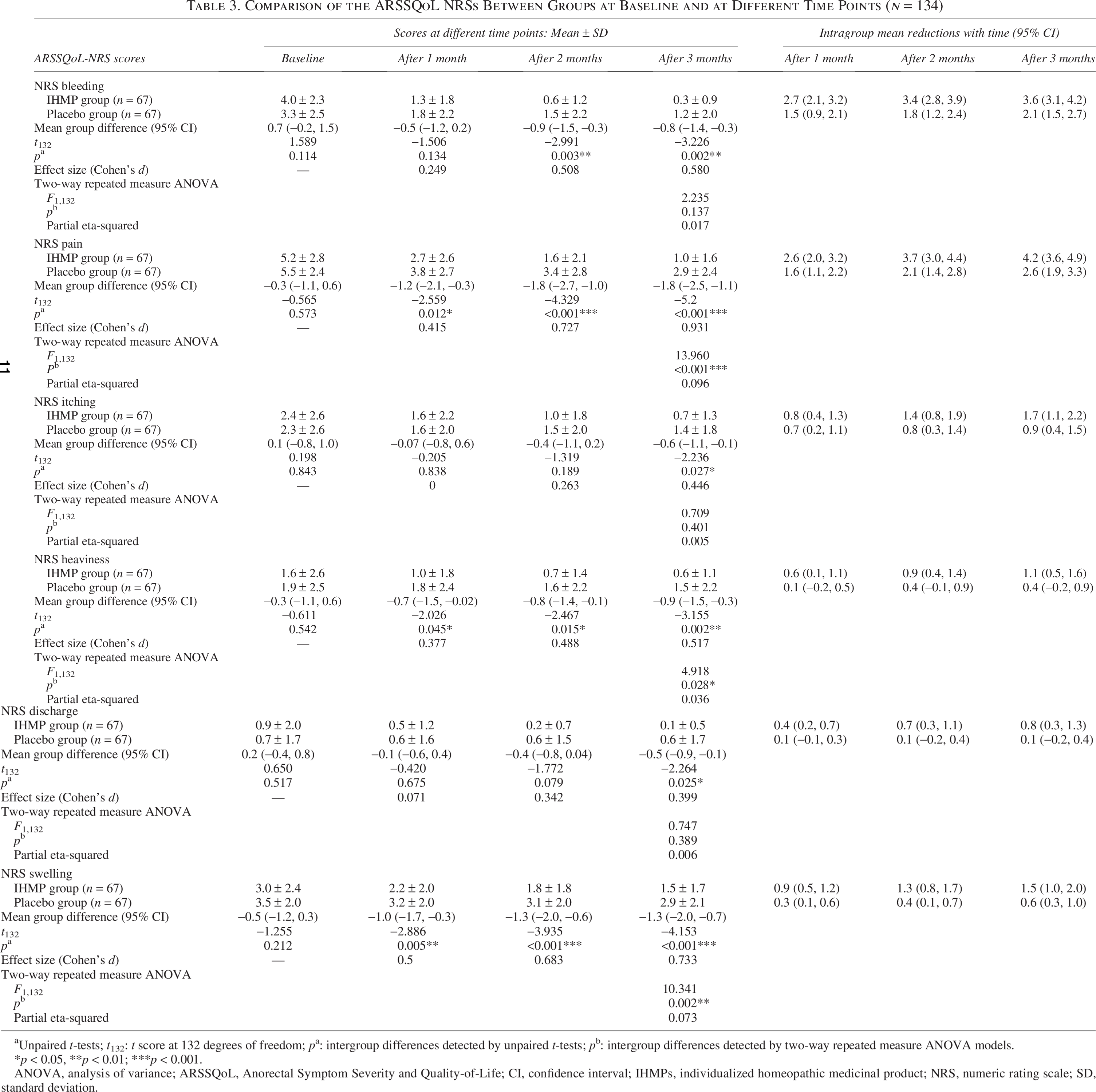
Unpaired t-tests; t132: t score at 132 degrees of freedom; pa: intergroup differences detected by unpaired t-tests; pb: intergroup differences detected by two-way repeated measure ANOVA models.
*p < 0.05, **p < 0.01; ***p < 0.001.
ANOVA, analysis of variance; ARSSQoL, Anorectal Symptom Severity and Quality-of-Life; CI, confidence interval; IHMPs, individualized homeopathic medicinal product; NRS, numeric rating scale; SD, standard deviation.
Comparison of the EQ-5D-5L Scores Between Groups at Baseline and at Different Time Points (n = 134)
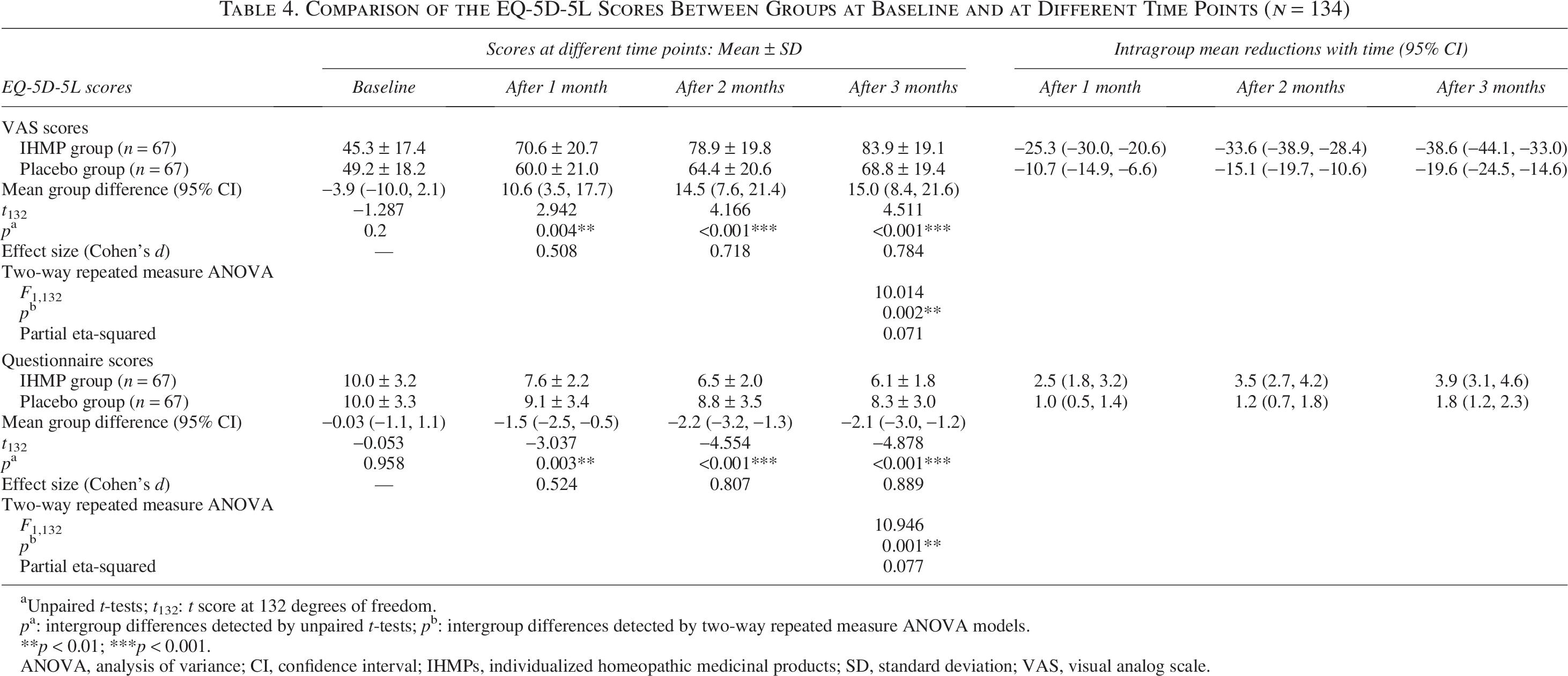
Unpaired t-tests; t132: t score at 132 degrees of freedom.
pa: intergroup differences detected by unpaired t-tests; pb: intergroup differences detected by two-way repeated measure ANOVA models.
**p < 0.01; ***p < 0.001.
ANOVA, analysis of variance; CI, confidence interval; IHMPs, individualized homeopathic medicinal products; SD, standard deviation; VAS, visual analog scale.
Medicines used
Twenty-one different medicines were indicated at baseline in the two groups. Sulfur (n = 26, 19.4%), Pulsatilla nigricans (n = 17, 12.7%), Natrum muriaticum (n = 16, 11.9%), Aesculus hippocastanum (n = 15, 11.2%), and phosphorus (n = 13, 9.7%) were the most frequently prescribed medicines (Table 5); the majority of the potencies prescribed at baseline were 200cH (n = 96, 71.6%), followed by 30cH (n = 34, 25.4%), 6cH (n = 3, 2.2%), and 1000cH (n = 1, 0.8%). The indications of the most frequently prescribed remedies have been appended (Supplementary Data S3). The radar plots revealed distinct patterns of effects of different medicines used in the trial (Supplementary Fig. S6). While multiple medicines contributed to the overall positive results of the intervention group, specific medicines demonstrated superior peaks of improvement. The most significant reduction in the ARSSQoL total was associated with Nitricum acidum, which showed the largest mean improvement. Other highly effective medicines for this outcome included Arsenicum album, Lachesis mutus, and Hamamelis virginiana. For the EQQ, Ratanhia peruviana and N. acidum demonstrated the most substantial improvements. L. mutus and H. virginiana also showed strong performance, indicating these medicines were particularly effective at addressing the broader functional dimensions of health measured by the EQQ. Regarding EQVAS, N. acidum, R. peruviana, and H. virginiana again emerged as the top performers. In addition, Collinsonia canadensis showed a notable peak in EQVAS improvement, suggesting a strong impact on the patients’ subjective sense of well-being. Thus, across all three clinical dimensions, N. acidum was consistently the most effective medicine. Kent’s repertory was the most frequently used. In the verum group, 60 cases were repertorized by using the Kentian (2nd) method, and 59 cases were in the placebo group. Seven cases in the verum group were repertorized by using Boericke’s method, and eight cases in the placebo group. All the cases were repertorized by using the new system and the total addition process.
Prescribed Medicines in the Two Groups at Baseline (n = 134)
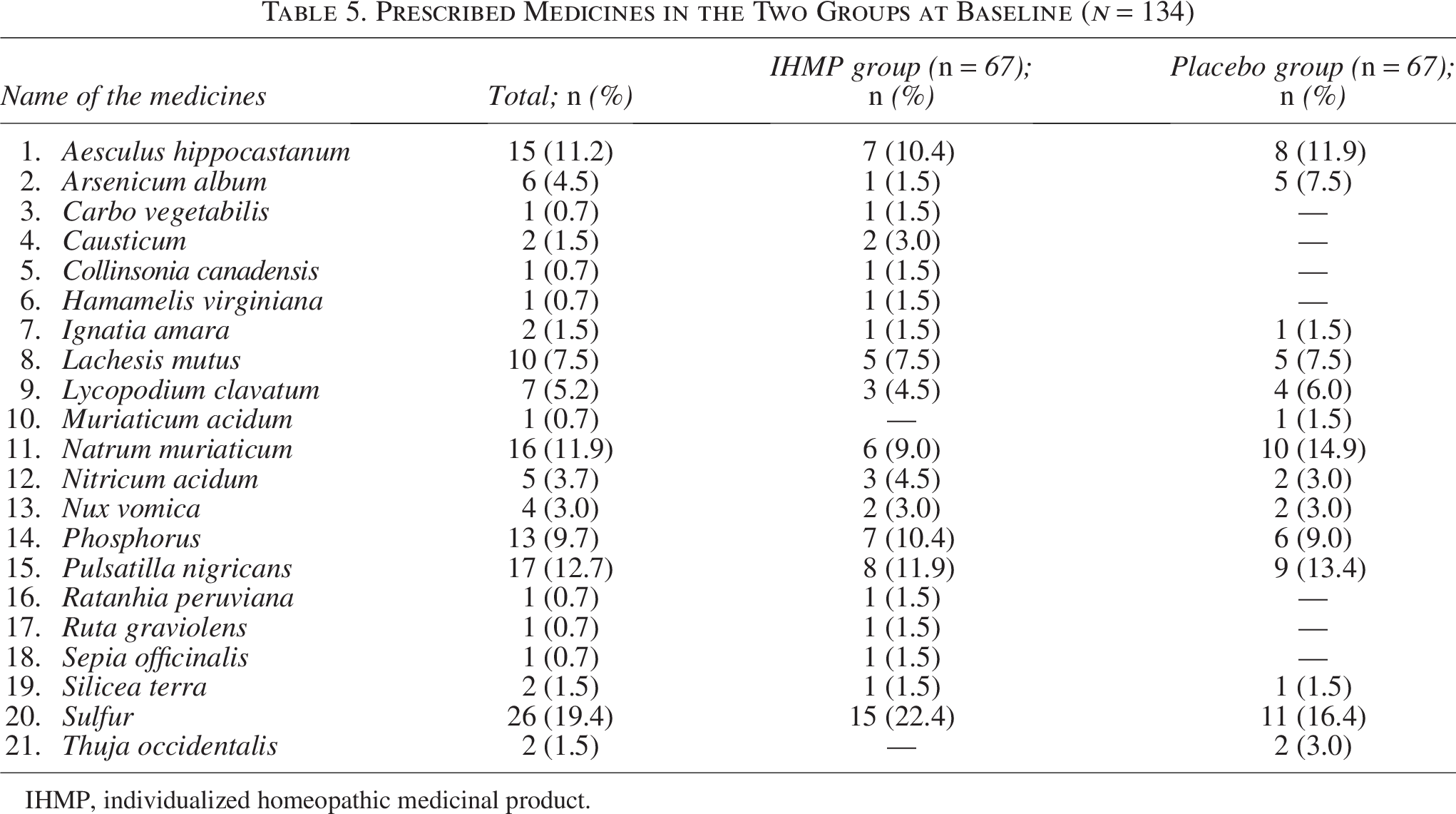
IHMP, individualized homeopathic medicinal product.
Adverse events
Three adverse events were reported in the verum group—one case of injury in the right leg after falling and was prescribed Arnica montana 200cH twice for 2 days. For a case of high fever associated with cough and cold after getting wet in the rain, Rhus toxicodendron 200cH was prescribed twice for 3 days; for a case of panaritium with much pain and swelling, Myristica sebifera 200cH potency was prescribed twice for 3 days. Two adverse events were reported in the control group: a case of diarrhea and another case of a cut injury. The former was prescribed Aloe socotrina 200cH twice for 2 days; the latter was given a mother tincture of Calendula officinalis, which healed the wound promptly. No homeopathic aggravations were reported in either the IHMP or placebo groups during the study period. All reported adverse events in both the IHMP and placebo groups were assessed by investigators as unrelated to the study intervention, and no SAEs or treatment-related harms were observed (Table 6).
Adverse Events Reported During the Trial
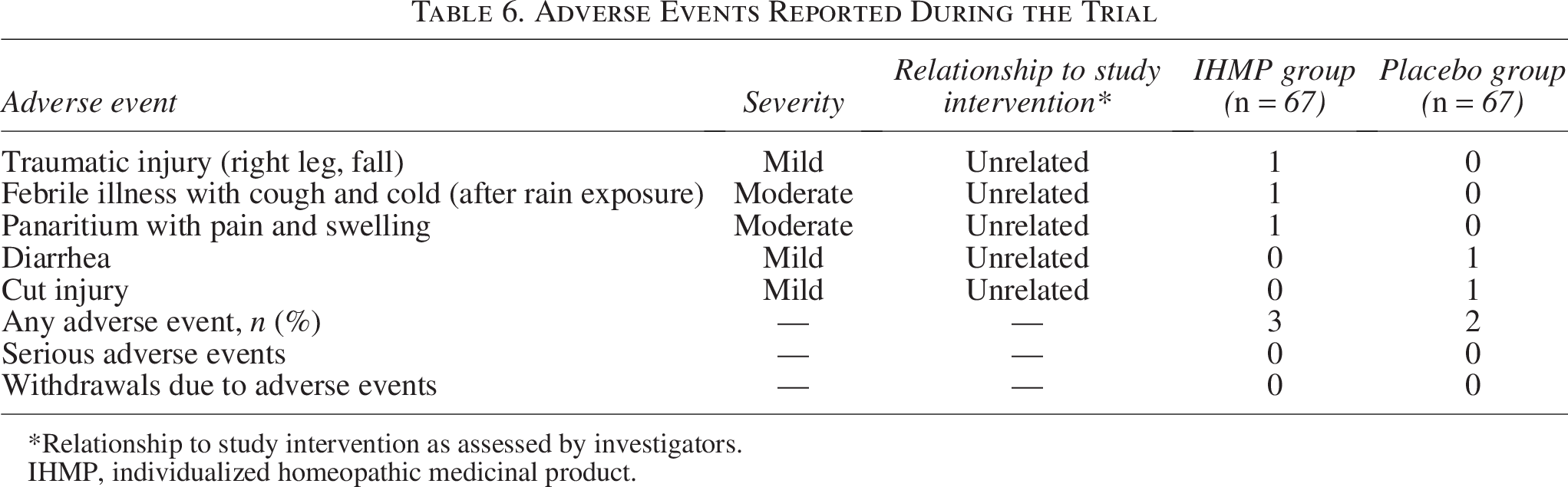
*Relationship to study intervention as assessed by investigators.
IHMP, individualized homeopathic medicinal product.
Discussion
A 3-month, double-blind RCT was conducted on 134 patients with hemorrhoids to detect the differences between IHMPs and identical-looking placebos. Trial subjects were randomized to receive either verum (IHMPs plus concomitant care; n = 67) or control (placebos plus concomitant care; n = 67). Concomitant care measures comprised of sitz baths, pelvic floor exercises, and dietary management. The ARSSQoL questionnaire and EQ-5D-5L were used as the primary and secondary outcomes, respectively, all measured at baseline and monthly intervals, up to 3 months. Group differences were statistically significant in both the outcomes and most of its subscales, favoring IHMPs over placebos after 3 months of the intervention. In addition to the prespecified repeated measures analyses, advanced longitudinal modeling approaches provided convergent support for the primary findings. MLMMs demonstrated a significant intervention × time interaction across outcomes, indicating that symptom severity and quality-of-life trajectories diverged over time in favor of IHMPs, with clear separation from placebo emerging by month 2 and persisting through month 3. Bayesian hierarchical modeling further corroborated these results, showing a very high probability of directional superiority of IHMPs over placebo for ARSSQoL and EQVAS outcomes, with posterior estimates closely aligned with the frequentist analyses. Sensitivity analyses comparing ITT and PP populations yielded nearly identical effect sizes and CIs, indicating that the observed treatment effects were robust and not driven by protocol deviations or missing data assumptions. The most often prescribed medicines were sulfur, P. nigricans, N. muriaticum, A. hippocastanum, phosphorus, and L. mutus. Exploratory radar chart analyses suggested heterogeneity in outcome-specific responses across individualized remedies, with N. acidum showing the most consistent and pronounced improvements across symptom severity and quality-of-life measures, while other frequently prescribed medicines demonstrated more domain-specific patterns of benefit, underscoring the individualized and nonuniform nature of treatment effects within the intervention group. The repertory of Kent and O. E. Boericke was mostly used for repertorization. As the majority of the cases were abundant in mental and physical general symptoms, Kent’s repertory was applicable in most of the cases. Importantly, none of the adverse events observed during the trial were considered causally related to the homeopathic preparations, supporting the safety profile observed in this study.
The major strength of the trial included an adequately large sample size, permuted block randomization, double-blinding, allocation concealment, placebo control, and use of several outcomes, measured repeatedly, thus enabling robust analysis with an ITT approach. The application of complementary frequentist, multivariate mixed-effects, Bayesian hierarchical, and sensitivity analyses represents a key methodological strength of this trial, as the convergence of findings across these independent analytic frameworks substantially strengthens the robustness and credibility of the observed treatment effects. The trial was ethically sound, addressing all possible ethical concerns. The concomitant nonpharmacological measures might have reduced group differences; however, those were necessary to confront the ethical issues of a placebo-controlled trial. The mode of prescription was individualized and represented the state-of-the-art practice of classical homeopathy, as was advocated by Hahnemann. The precision of prescription was augmented further by the use of consensus methods among the prescribers.
Several limitations should be considered when interpreting these findings. First, the generalizability of the results may be limited, as the study was conducted in a single outpatient setting with trial subjects who met specific inclusion criteria. Replication across different clinical settings, health care systems, and patient populations is required before broader inferences can be made. Second, although statistically significant differences were observed for the primary outcome, some secondary outcomes were associated with wide CIs, reflecting imprecision and uncertainty in the magnitude of effect. The study was powered for the primary endpoint and not for all secondary comparisons; therefore, estimates for secondary outcomes should be interpreted cautiously. Third, the analysis involved multiple secondary and domain-specific outcomes without formal adjustment for multiplicity. While this approach was prespecified and intended to explore outcome patterns rather than to support confirmatory inference, it increases the risk of type I error. Accordingly, findings related to secondary outcomes should be considered exploratory. Fourth, individualized prescribing was performed by trained practitioners following standardized principles; however, practitioner variability in case analysis and remedy selection cannot be entirely excluded. Such variability reflects real-world clinical practice but may contribute to heterogeneity in treatment effects and should be examined in future multicenter studies with prespecified strategies to assess interpractitioner consistency. Finally, interpretation of the present findings should consider the absence of an empirically established MCID for the ARSSQoL total score. While statistical significance alone does not imply clinical importance, the magnitude of the observed between-group difference, together with large effect sizes, suggests that the improvements may be clinically meaningful. However, without an anchor-based MCID derived from patient-centered outcomes, definitive conclusions regarding clinical importance cannot be drawn. Future studies should prioritize establishing an MCID for the ARSSQoL to enable more precise interpretation of treatment effects. Another disadvantage might be the generalizability issues, that is, trial subjects who volunteered for participation might not be typical of the population of interest. Nevertheless, by randomly allocating trial subjects to active treatment and placebo groups, the trial provided the fundamental context for using evidence-based medicine.
In 278 patients experiencing acute episodes of hemorrhoidal problems, a single-blind, randomized, placebo-controlled trial utilizing 50 millesimal potencies of IHMPs was carried out. 15 The patients were followed for 3 months, but no validated outcomes related to the condition were seen. The sample size was relatively large, and the trial was multicentric; however, it was prone to subjective biases because it was a single-blind trial. In contrast to RCTs, a 6-month single-arm trial of IHMPs in centesimal potencies using a pre–post comparison design on 52 patients with hemorrhoids had methodological flaws. 14 This trial had the advantage of an extended follow-up duration of 6 months. To contextualize the present findings, we compared the primary outcome with results from a previously published RCT by Koley et al., which employed a similar RCT design, patient population of n = 140, and the same outcomes, measured at the same intervals up to 3 months, and used a similar sort of homeopathic interventions in centesimal potencies. 16 When the primary outcome estimates from both trials were pooled using a random-effect forest plot model, the direction and magnitude of effect remained consistent with the findings of the current study (−6.06, 95% CI −7.69, −4.43, z = 7.29, p < 0.001, Fig. 2). This exploratory pooled comparison is intended to provide contextual support rather than a formal meta-analytic estimate and should be interpreted cautiously. Nonetheless, the concordance of results across two independent trials strengthens confidence in the observed pattern of benefit. A full systematic review and meta-analysis incorporating all eligible trials was beyond the scope of the present study and warrants separate investigation. Phosphorus, sulfur, Nux vomica, N. acidum, N. muriaticum, and Lycopodium clavatum were among the most frequently prescribed medicines in all these trials.
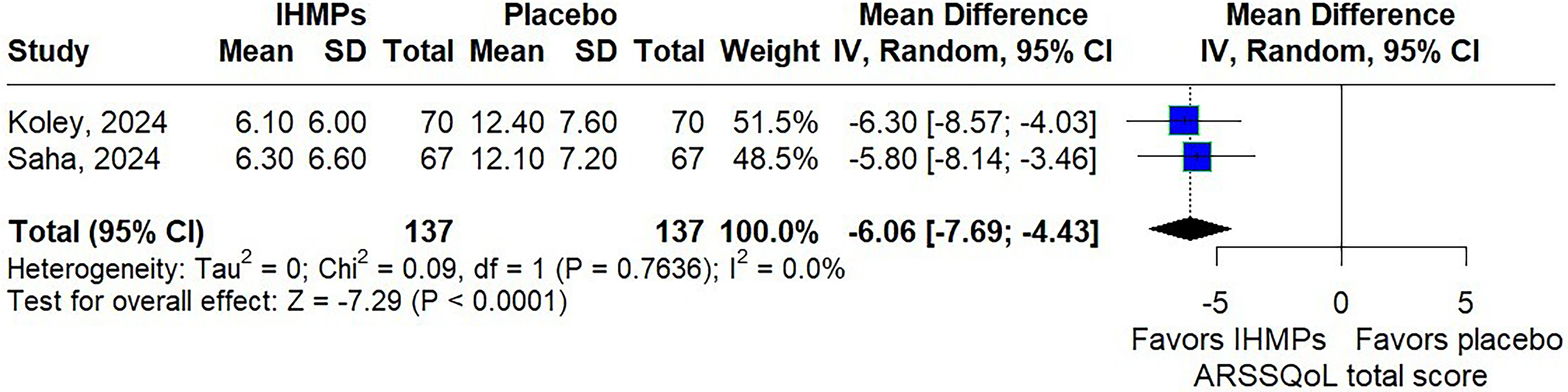
Forest plot of piles RCTs. RCT, randomized controlled trial.
Future trials should aim at further but independent replications, using the same or different sets of outcome measures, and the use of LM potencies.
Conclusion
In this 3-month, double-blind, randomized, placebo-controlled trial involving 134 patients with hemorrhoids, IHMPs were associated with greater reductions in anorectal symptom severity and improvements in health-related quality of life compared with placebo when administered alongside standard concomitant care. These findings were consistent across repeated measures, multivariate mixed-effects, Bayesian hierarchical, and sensitivity analyses, indicating that the observed effects were robust to different analytic assumptions. Although the magnitude of benefit suggests potential clinical relevance, interpretation remains constrained by the absence of a validated MCID for the ARSSQoL instrument. Accordingly, while the results support the superiority of IHMPs over placebo within the study context, independent replications in diverse settings and further work to establish clinically meaningful thresholds for outcome measures are required before definitive clinical conclusions can be drawn.
Footnotes
Acknowledgments
The heads of the academic and hospital divisions of the institutions are acknowledged by the authors for enabling us to carry out the trial successfully. The authors express their gratitude to pharmacists, patients, staff, and other colleagues and postgraduate trainees for their unwavering support and genuine involvement in the research.
Authors’ Contributions
A.S.: Conceptualization, methodology, software, validation, investigation, data curation, writing—original draft, writing—review and editing, and project administration. S.M.A., R.K.P., S.G., S.S., S.B., and S.K.M.: Conceptualization, methodology, investigation, resources, supervision, data curation, and writing—review and editing. S.M., I.H., M.K., A.G., S.D., and D.C.: Conceptualization, methodology, investigation, data curation, and writing—review and editing. S.A.R., P.G., and S.S.: Conceptualization, methodology, resources, and writing—review and editing. M.K. and S.S.: Conceptualization, methodology, formal analysis, visualization, software, writing—original draft, and writing—review and editing.
Data Availability Statement
This article contains all of the data that were collected or examined during the trial. The corresponding author can be contacted with any additional queries.
Conflict of Interest Statement
None stated. The final report of the project was submitted as the postgraduate dissertation work of the first author to the West Bengal University of Health Sciences, Kolkata.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The institution played no role in the conceptualization, conduct, analysis of the study results, or the preparation and publication of the article.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.