
Abstract
Objective:
Distal radius fracture (DRF) is the most frequent injury to the upper limb. Complications include nonunion, wrist stiffness and instability, local discomfort, and tendon irritation. The purpose of the current open-label clinical study was to evaluate the safety, efficacy, and tolerability of CL16019, an herbal formulation of Cissus quadrangularis and Boswellia serrata extract, in accelerating fracture healing in volunteers with DRFs.
Methods:
Fifty participants (both male and female; age: 30–50 years) with type I, IIA, or IIB DRFs (as per Lidstrom classification) were equally randomized and treated with standard treatment (ST) or ST + CL16019 for 60 days. The primary efficacy outcome was the radiographical bone fracture healing rate as scored by the Radius Union Scoring System (RUSS). Pain, swelling, and tenderness were among the clinical characteristics evaluated using the visual analog scale (VAS). Wrist function improvements were assessed using the Patient-Rated Wrist Evaluation Questionnaire (PRWEQ). The intergroup and intragroup results were analyzed using a paired t-test and an analysis of covariance model, respectively.
Results:
The RUSS scores for the ST and ST + CL16019 groups at the end of the trial were 5.54 ± 1.77 and 7.96 ± 0.20, respectively, with a p-value <0.0001. In addition, the CL16019 volunteers showed substantial (p < 0.05) declines in their VAS and PRWEQ scores. The ST + CL16019 group demonstrated higher Physician Global Assessment and Subject Global Assessment scores.
Conclusions:
Supplementation of CL16019 along with standard therapy was found to enhance the bone fracture healing rate, possibly by accelerating the callus formation rate and enhancing cortical bridging. These findings imply that CL16019 might be a good adjunctive in addition to ST for the faster healing of DRFs. The trial was registered with the Clinical Trial Registry of India (CTRI) with the registration number CTRI/2021/12/039006, on December 29, 2021.
Introduction
Distal radius fracture (DRF), commonly known as wrist fracture, is the most frequent upper extremity injury in both young adults and the elderly. Indeed, DRFs account for over 15% of orthopedic fractures. 1 Nonsurgical treatment methods, such as closed reduction and cast immobilization, have been traditionally used for the treatment of DRFs. The standard treatment (ST) for DRFs includes surgical reduction and internal fixation, followed by physical therapy to realign broken bones and stabilize the fractures. Despite surgical and nonsurgical treatment, patients often suffer from certain common complications such as wrist stiffness and instability, nonunion, tendon irritation, infection, and local pain.2,3 Literature suggests a complication rate of approximately 37% following surgery for DRF. 4
Several local and systemic factors, such as blood supply, periosteal excision or stripping, and infection at the site of fracture, considerably affect the healing of bone fractures. Early mobilization protocols and rehabilitation therapies have been recommended to improve positive outcomes of DRF.5,6 However, 5%–10% of DRFs fail to heal normally, resulting in prolonged healing time or nonunion of fractures. 7 Pharmacological therapy using opioids and nonsteroidal anti-inflammatory drugs to manage postsurgery pain is usually associated with an increased risk for adverse effects. 8 Currently, available biological adjuvant therapies, including stem cells, growth factors, anabolic agents, and collagen-based matrices, have been suggested to promote bone repair and fracture healing. However, these therapies require standard optimization and are concerned with some safety issues. 9 This necessitates the development of alternative complementary therapies to manage pain, accelerate bone healing, and improve wrist function in patients with DRFs. 10
Accumulating preclinical and clinical studies have demonstrated the osteogenic potential of different extracts and formulations derived from medicinal herbs, implying their beneficial role in the healing and acceleration of bone fractures.3,11–13 The World Health Organization estimates that about 70%–80% of the global population relies on complementary and alternative medicines derived mainly from medicinal herbs for their health care needs.14,15 For instance, Boswellia serrata (BS; Burseraceae family) gum resin has been widely used in traditional medicine systems, including Ayurveda, to treat various ailments. Its gum resin has been demonstrated to possess multiple pharmacological properties, such as anti-inflammatory, antiarthritic, and analgesic activity. 16 Clinical trials have shown that BS extract was well tolerated by patients with osteoarthritis, except for minor gastrointestinal events.17–19 Aflapin®, a BS formulation of 20% 3-O-acetyl-11-keto-β-boswellic acid (AKBA), showed significant anti-inflammatory effects than the BS extracts. 5-Lipoxygenase enzyme catalyzes the synthesis of inflammation-associated leukotrienes from arachidonic acid. Previous studies reported that mice lacking 5-lipoxygenase enzyme accelerate the fracture healing, suggesting a critical role of 5-lipoxygenase in bone healing process. 20 Ten days supplementation of BS extract (60 mg a day), standardized to 76% of AKBA, reduced the soreness of muscle and joint, promoted the functional recovery of muscle, and reduced inflammatory biomarkers such as C-reactive protein (CRP) and interleukin-6 following exercise-induced delayed onset of muscle soreness in males. 18 Long-term supplementation of Aflapin® (100 mg a day) increased the cartilage volume, thickness, and joint space of tibiofemoral joints in subjects with moderate to severe knee osteoarthritis. Subjects reported significant improvements in their mobility and physical function. In addition, serum levels of high-sensitive CRP, matrix metalloproteinase-3, Fibulin-3, type II collagen degradation peptide in serum, and cross-linked C-terminal telopeptide of type II collagen in urine. 19 In vivo toxicity studies further revealed that Aflapin® did not exert signs of toxicity, indicating its safety.21–23
Cissus quadrangularis (CQ), a medicinal herb belonging to the Vitaceae family, is widely used in India, Africa, and Thailand due to its diverse biological activities, including antioxidant, anti-inflammatory, anti-obesity, and anti-hemorrhoidal effects.24–27 CQ has been known for its bone-healing properties for many centuries; it has been prescribed by bone setters in the crude form in both topical and oral formulations. 28 Accumulating research data also suggest the bone health-promoting potential of CQ extracts.29–31 Clinical trials have reported that oral intake of CQ extracts significantly delayed bone loss in postmenopausal women with osteopenia. 29 Intriguingly, clinical studies demonstrated that CQ extracts not only increased the osteogenic potential of distracted bone but also promoted bone density. 32 These data suggest the remarkable potential of CQ to enhance the rate of new bone formation. 32 Combinatorial supplementation of CQ extract together with other herbal extracts has been demonstrated to substantially promote healing of bone fractures clinically. 33 In this context, the present randomized, open-label study was designed to evaluate the efficacy and tolerability of CL16019, a proprietary formulation comprising CQ and BS (or Aflapin®) extracts in accelerating bone fracture healing in subjects with DRF.
Material and Methods
Study design and ethical approval
The present study was a prospective, multicentric, randomized, open-label clinical study aimed to evaluate the safety and efficacy of CL16019 (Ostibind™ or Ogenic® Elements) in accelerating bone fracture healing rate in participants with DRF.
Study centers
This multicenter clinical study protocol was approved by the Institutional Ethics Committees of Vijaya Super Speciality Hospital, Nellore, Andhra Pradesh (ECR/453/Inst/AP/2013/RR-19; Approval No. VEC/22/10/CLS/BF; October 22, 2021), NUHA Hospitals, Guntur, Andhra Pradesh (ECR/1593/Inst/AP/2021; Approval No. NEC/22/CLS/BF/MM-013; January 24, 2022), and Pranaam Hospital, Hyderabad, Telangana (ECR/1460/Inst/TG/2020; Approval No. IEC/PRNM/007; 29 January 2022). All three participating centers are multispecialty hospitals with advanced surgical facilities, dedicated trauma care units, and comprehensive clinical services. Each center maintains a 24-h emergency department and specialized teams for managing complex cases, enabling high standards of patient care and robust clinical research conduct. This study was also registered (Ref: CTRI/2021/12/039006) at the Clinical Trial Registry of India (study initiation date: February 09, 2022, and completion date: October 16, 2022). All volunteers were thoroughly informed about the study’s objectives, potential risks, and both direct and indirect benefits prior to participation. The information was presented in clear and understandable language, and participants were given sufficient time to ask questions and seek clarification. They were assured of the confidentiality of their personal data and informed of their right to withdraw from the study at any point without any consequences. Only after confirming their understanding and voluntary consent did they sign the informed consent form. The entire process was conducted in accordance with the highest ethical standards in human research.
Investigational product
CL16019 was a proprietary herbal formulation containing standardized CQ and BS extracts in a 5:1 ratio. C. quadrangularis extract is produced from aerial parts of the plant using 90% aqueous ethanol as extraction medium (4 volumes) at 60–70°C. B. serrata extract is a commercially available ingredient called Aflapin® marketed globally by PLT Health Solutions, USA, standardized to contain at least 20% AKBA. It is a novel synergistic composition containing B. serrata extract enriched with AKBA and B. serrata nonvolatile oil (PCT application # PCT/IN2009/000505). CL16019 is standardized to contain NLT 0.05% sterols and steroids and NLT 3% of AKBA by high performance liquid chromatography (HPLC). It is manufactured in the GMP facility of Chemiloids, Vijayawada.
Study population
Sixty male and female volunteers aged between 30 and 50 years of age who visited outpatient departments (OPDs) of study centers for the management of unilateral or bilateral DRFs were screened. The volunteers were screened as per the inclusion and exclusion criteria (Supplementary Table S1). Fifty participants with radiologically confirmed DRF of type I, IIA, or IIB category (as per Lidstorm classification) were included in the current study. All patients confirmed their willingness to receive a closed reduction or immobilization for fracture.
Sample size
The sample size was calculated using a two-sided t-test of size 5% (α = 0.05). The mean difference in the Radius Union Scoring System (RUSS) scores between the groups was assumed to be 0.9 with a standard deviation of 0.94. From these assumptions, the total sample size was calculated as 24 patients per group to obtain a power of 90% to meet the primary objective. The difference in change from the baseline mean RUSS is arrived at based on a previous clinical study. 34
Randomization and treatment
During their OPD visit to the orthopedic departments of the study centers, patients underwent digital radiographical examinations for the confirmation of DRF. Volunteers who met the eligibility criteria were fully informed about the study, provided written informed consent, and were randomly assigned to one of two study groups (n = 25 each): ST or CL16019 + ST. Randomization was performed using a computer-generated allocation sequence (PROC PLAN, SAS®) by an independent individual with no contact with the investigators. Participants were randomized in a 1:1 ratio, and allocation concealment was ensured through sequentially numbered, opaque, sealed envelopes, maintained until assignment to minimize selection bias despite the open-label design. The randomization schedule was prepared for the planned sample size of 50 participants, resulting in 25 assignments per group. Each participant received a randomized number sequentially from a confidential randomization list. After physician examination, volunteers received necessary immobilization or reduction. Volunteers in both groups received ST at the discretion of the physician. ST included Aceclofenac (100 mg) + Paracetamol (500 mg) daily for 5 days, Pantoprazole (40 mg) daily for 5 days, Trypsin-Chymotrypsin (100,000 IU) three times daily for the next 3 days, Elemental Calcium Carbonate (500 mg), and Vitamin D3 (250 IU) OD for the first 30 days. Volunteers in the ST + CL16019 group received CL16019 tablet (600 mg) to be consumed daily after breakfast along with the ST therapy for 60 days. Volunteers were supplied with CL16019 at randomization visit, that is, the 1st day of the OPD visit and visit 2 (day 30). At every visit, body weight and vital signs (blood pressure, heart rate, mouth temperature, and respiration rate after 5 min of sitting) were noted. Participant adherence to the intervention was monitored by counting the pills returned at days 30 and 60. No concomitant medication other than ST was allowed during the study. None of the participants required or sought rescue medication during the study period.
Study outcomes
Radiological assessment for improvement in fracture healing (RUSS)
RUSS is a simple, validated scoring system to assess the radiographical union of DRFs, which can be managed without surgical intervention and can be managed by simple fixation. Briefly, a set of radiographs was analyzed for four cortical scores ranging from 0 to 2 by independent evaluators who are blinded to the treatment arms. There are no callus formation and a visible fracture line; the RUSS score is 0. The presence of a callus with a visible fracture line is indicated with a score of “1.” A score of “2” denotes cortical bridging in the absence of a distinct fracture line. 35 Scores of four cortices were summed, and the total RUSS scores for each participant were reported at baseline, days 30, and 60.
Pain, swelling, and tenderness
Volunteers were evaluated for pain, swelling, and tenderness at baseline, days 7, 15, 30, 45, and 60. At each visit, volunteers were asked to rate their perception of pain, swelling, and tenderness using a 10-mm visual analog scale (VAS), where “0” indicated no pain/swelling/tenderness and “10” represented the worst possible severity.
Patient-Rated Wrist Evaluation Questionnaire
Patient-Rated Wrist Evaluation Questionnaire (PRWEQ) is a 15-item self-administered questionnaire designed to measure wrist pain and disability in activities of daily living. The PRWEQ consists of two subscales, that is, pain and function. The pain subscale includes five items, while the subscale function is separated into six specific activities and four usual activities. At baseline and on days 30 and 60, volunteers scored each item of PRWEQ on a 10-point ordinal scale. The score of the pain subscale is the sum of the five items divided by two, with the score ranging from 0 (indicating no pain) to 50 (worst pain). The “function” subscale score is calculated by the sum of the 10 items divided by two. The total score of the PRWEQ is the sum of the scores of both subscales, with the total score ranging from zero (no disability) to 100 (worst disability). A score of 0 indicates no disability, while a score of 100 indicates the lowest functional score. 36
Grip strength
A digital handheld dynamometer (Inco Instruments and Medical Devices Private Limited, India) was used to evaluate the grip strength of the volunteers on day 60. Each participant underwent a grip strength assessment using the hand in which the fracture had occurred. Care was taken to ensure they maintain a similar position at each measurement. Each participant was asked to perform the assessment three times, maintaining a similar position at each measurement, and the average was reported.
Physician Global Assessment (PGA) and Subject Global Assessment (SGA)
The response of both ST and ST + CL16019 therapies was assessed using the Physician Global Assessment (PGA) and Subject Global Assessment (SGA) scales, as per the physician and the participants, respectively, on days 30 and 60. The number of participants showing one through seven on each scale, which stand for very much improved, much improved, minimally improved, no change, minimally worse, much worse, and very much worse, was noted.
Bone formation biomarkers analysis
Fasting blood samples were collected at baseline, days 30, and 60 and were analyzed for bone-specific alkaline phosphatase (BAP; CUSABIO® #CSB-E09033h) and parathyroid hormone (PTH: Abcam #ab230931) using commercially available ELISA kits. The analytical sensitivities were 7.8 and 0.761 pg/mL for BAP and PTH, respectively.
Liquid chromatography–mass spectrometry/mass spectrometry
The plasma concentrations of 11-keto-β-boswellic acid (KBA) and AKBA were analyzed by Waters TQ-S liquid chromatography–mass spectrometry/mass spectrometry (LC–MS/MS) with MassLynx software. Plasma samples were collected at baseline, days 30, and 60, and serum phytoconstituent levels were extracted by a liquid–liquid extraction method. Plasma samples were mixed with the water in a ratio of 1:3 and extracted with the solvent mixture (ethyl acetate: n-hexane [90:10]). Vortexed and centrifuged the samples for 10 min at 1756 × g. The solvent used for the extraction was separated and evaporated under a stream of nitrogen, and the residue was reconstituted with 0.300 mL of methanol, and 5 μL was injected into the LC–MS/MS. All calibration curves and quality control samples were prepared in plasma by spiking standard solutions. Correlation coefficients for KBA and AKBA achieved r2 values >0.990. The chromatographic separation of KBA and AKBA was achieved using Waters BEH C18, 1.7 µm, 50 × 2.1 mm (Waters Corporation, Milford, MA) and 5 mM ammonium acetate: acetonitrile (23:77) at a flow rate of 0.400 mL/min. The analytes were detected in the multiple reaction monitoring with negative ionization mode. The mass spectrometer transitions (precursor/product) were as follows: KBA (469.4786/391.37), AKBA (511.4967/59.0418), and IS acetyl-11-keto-β-boswellic acid D3 (514.4967/62.0345). The optimized parameters for the ionization source included a capillary voltage set at 2.2 kV, a cone voltage of 30 V, a desolvation temperature of 500°C, a nebulizer gas flow rate of 7 bar, desolvation gas flow rate of 1000 L/h, and cone gas flow of 150 L/h. Using the optimized method, the obtained limits of quantification for KBA and AKBA were 2.304 ng/mL. Each calibration curve was analyzed individually by using least square weighted linear regression (1/x2).
Safety assessments
At every visit, participants were allowed to take a 5-min rest in a seating position, and an automated blood pressure monitor was used to monitor resting blood pressure and pulse rate. A digital pulse oximeter and tympanic thermometer were used to measure respiratory rate and body temperature. Participants underwent a noninvasive physical examination by a study physician for general appearance (eyes, ears, nose, mouth, and throat), respiratory, gastrointestinal, skin, and musculoskeletal symptoms. Serum from fasting blood samples was analyzed for hematology, biochemistry, and coagulation outcomes at every visit.
Adverse events
Incidences of adverse events (AEs) were recorded at every visit by questioning the volunteers in a nonleading manner. The date, duration, description of the event, actions taken, outcome, and the opinion of the investigator were recorded. As mentioned in the study protocol, the AEs and adverse drug reactions (ADRs) were summarized by system organ class and preferred term using Medical Dictionary for Regulatory Activities, and the incidence of AEs and ADRs was compared across the treatment groups.
Statistical analysis
Efficacy analysis was conducted for 49 participants who consumed at least one dose of the study supplement and had at least one post-baseline efficacy evaluation as per-protocol population. Safety analysis was based on the population of participants who received at least one dose of study supplement as intent-to-treat population. Missing values were handled using last observation carry forward. Baseline demographics, vital signs, and laboratory parameters were analyzed using a two-sample t-test. Paired t-test and the analysis of covariance for comparison of within the groups and between-the-group differences. Baseline measurements were included as covariates to adjust for initial differences and improve the accuracy of group comparisons. The post hoc comparisons were made using Bonferroni multiple comparison test. p < 0.05 was considered statistically significant. SAS 9.4 (SAS Institute, NC, USA) was used for the statistical analysis.
Results
A total of 60 volunteers with DRFs were vetted; of these, 33 males and 17 females who qualified for the study criteria were enrolled and equally randomized to ST and ST + CL16019 groups to receive the allocated intervention. One participant in the ST group was lost-to-follow-up from the study. The consort flow diagram is provided in Figure 1.
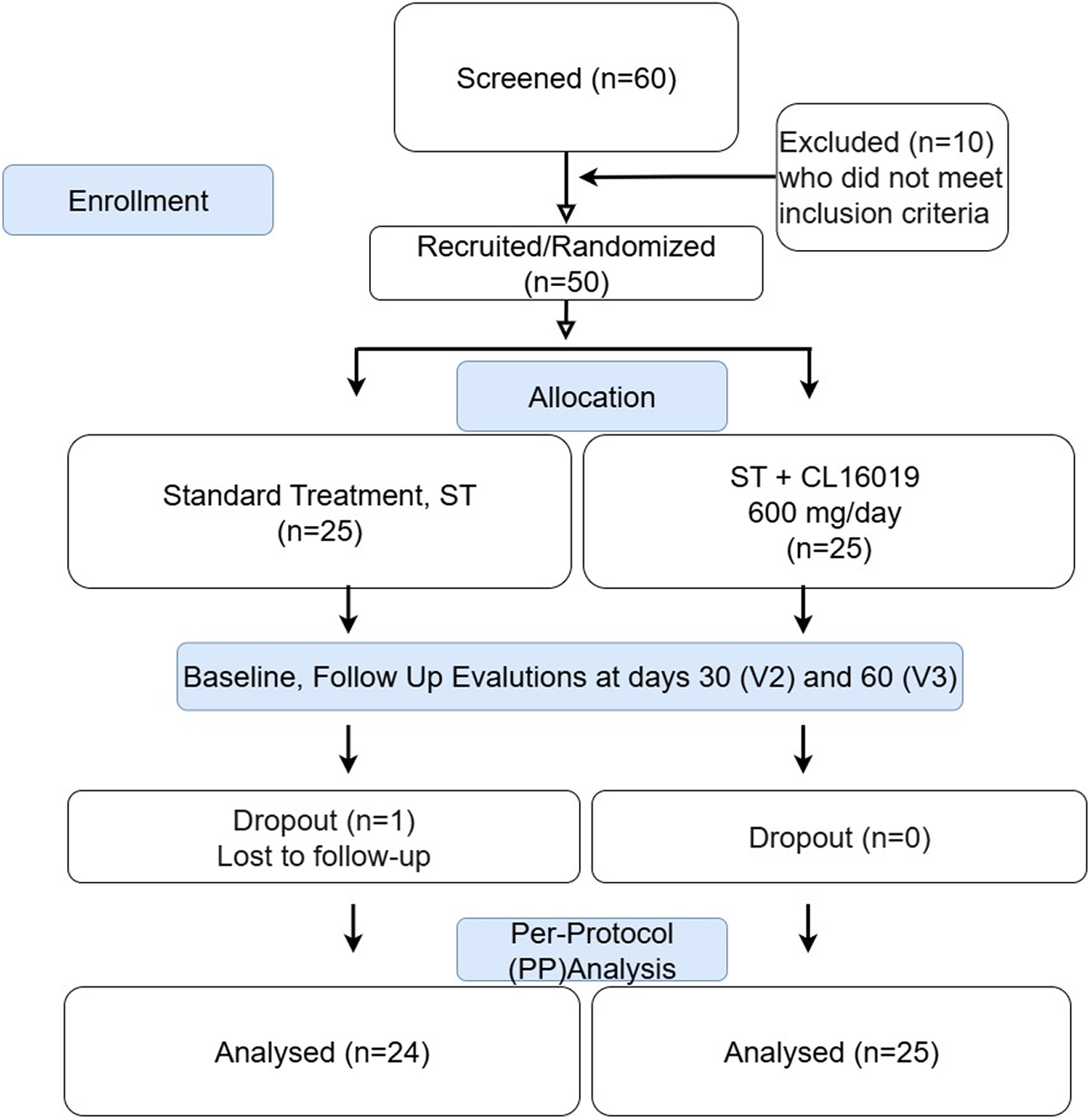
Consort flow diagram.
Both the treatment groups were balanced for the reported baseline demographics, as presented in Table 1. Volunteers demonstrated good compliance as majority of them consumed more than 90% of the investigational product during the entire study duration. A total of six minor deviations is reported. The average RUSS scores increased from zero to 1.13 ± 1.60 (p = 0.0003 vs. baseline) and 3.76 ± 1.20 (p < 0.0001 vs. baseline) in the ST and ST + CL16019 groups, respectively, by day 30. At the end of the trial, the ST group’s RUSS scores were 5.54 ± 1.77, while the ST + CL16019 group scores were 7.96 ± 0.20 (p < 0.0001) for both groups versus respective baseline values. On days 30 and 60, the ST + CL16019 group’s RUSS scores were significantly greater than those of the ST group (Table 2; Fig. 2). The anteroposterior and lateral radiographs representing DRFs with a RUSS score of 0 are given in Figure 3A, where the fracture lines are visible at the medial, lateral, anterior, and posterior cortices. The anteroposterior and lateral radiographs of a DRF with a RUSS score of 6 or greater are shown in Figure 3B. Cortical bridging without a clear fracture line is demonstrated on medial, lateral, anterior, and posterior cortices at day 60 in the CL16019 + ST group subject (Fig. 3B).
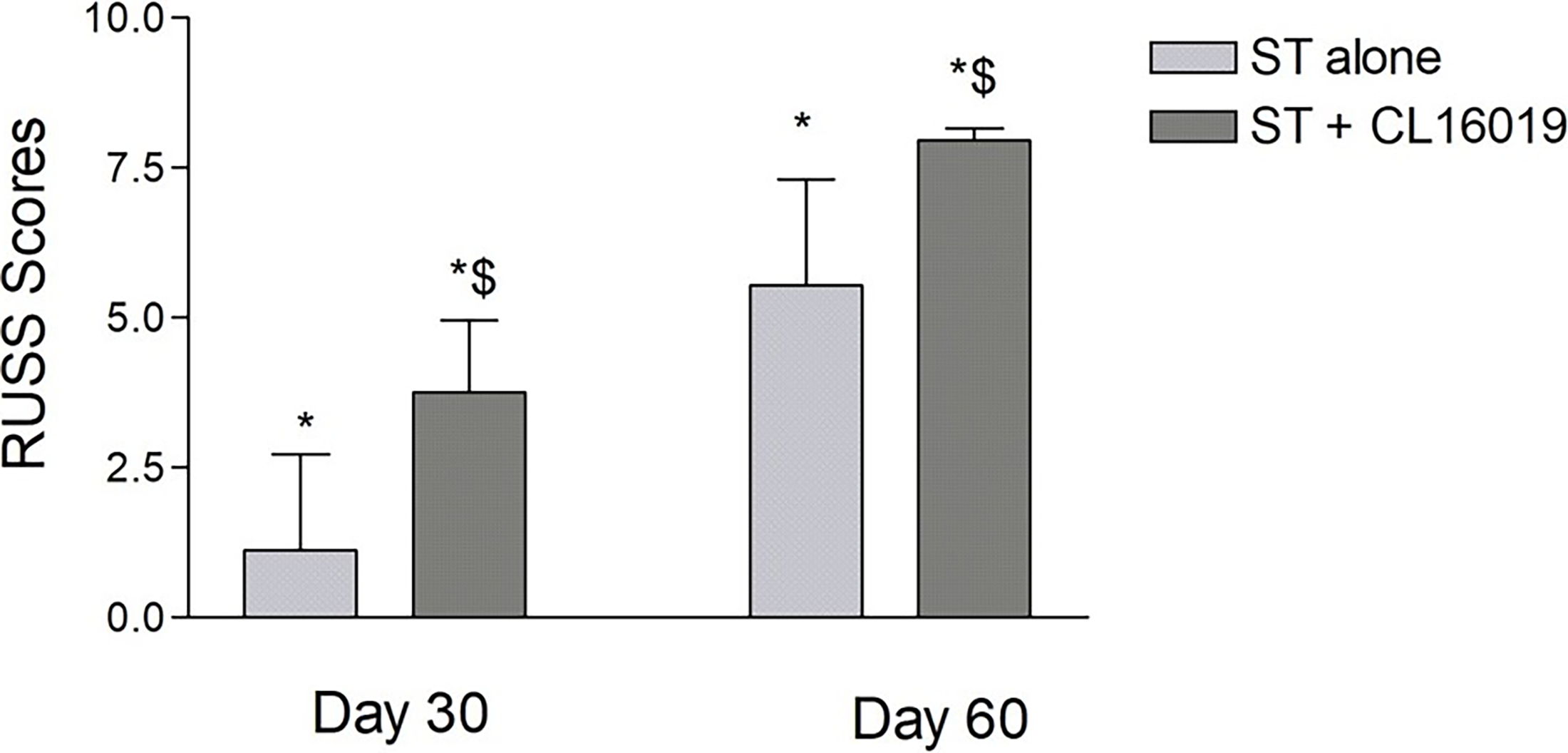
RUSS scores (mean ± SD) at days 30 and 60. *Indicates significance (p < 0.05) in intragroup comparison (vs. baseline) analyzed using paired t-test. $Indicates significance (p < 0.05) in intergroup comparison (vs. ST alone) analyzed using ANCOVA model. ANCOVA, analysis of covariance; RUSS, Radius Union Scoring System; SD, standard deviation; ST, standard treatment.
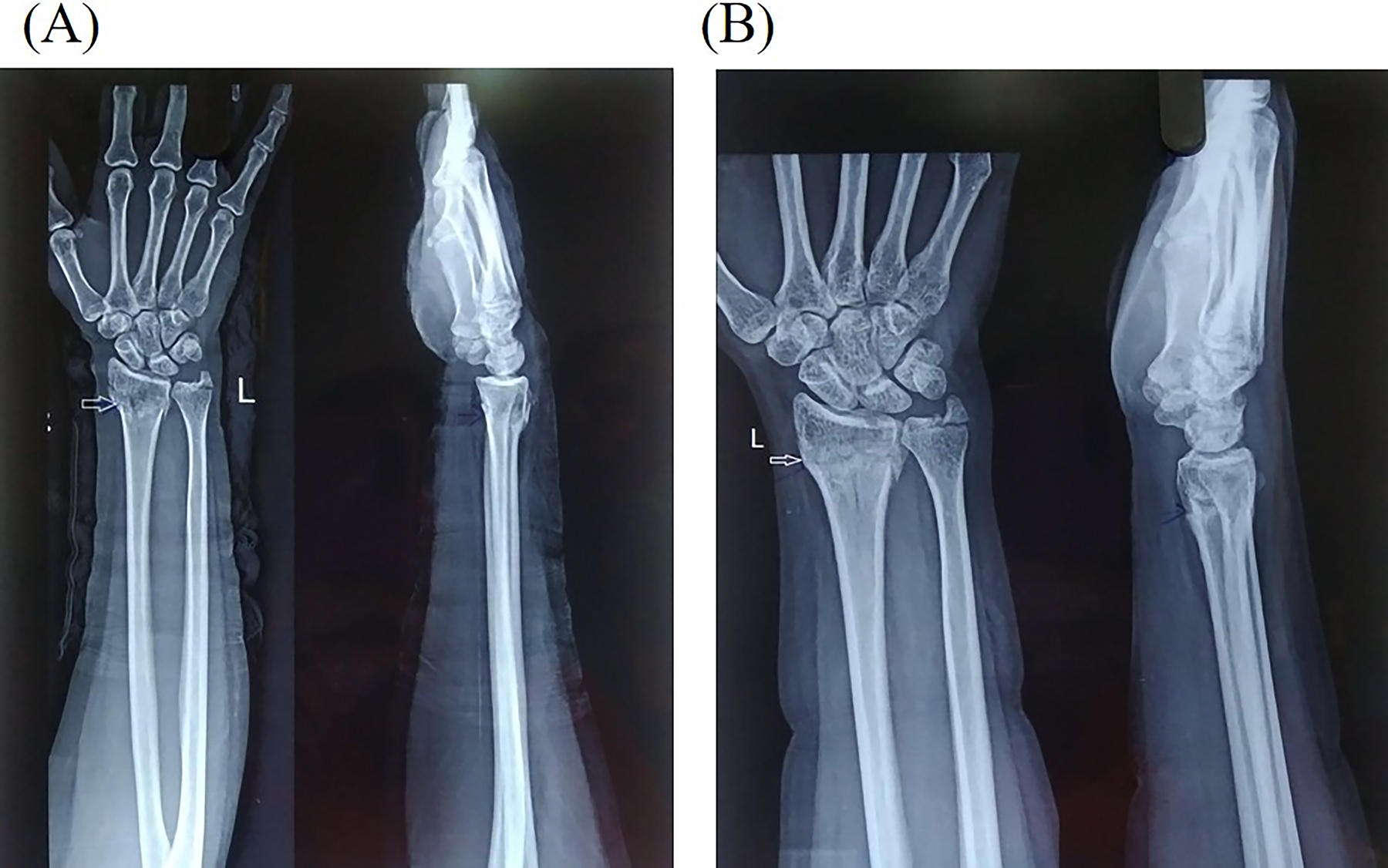
Radiographs:
Demographic Characteristics
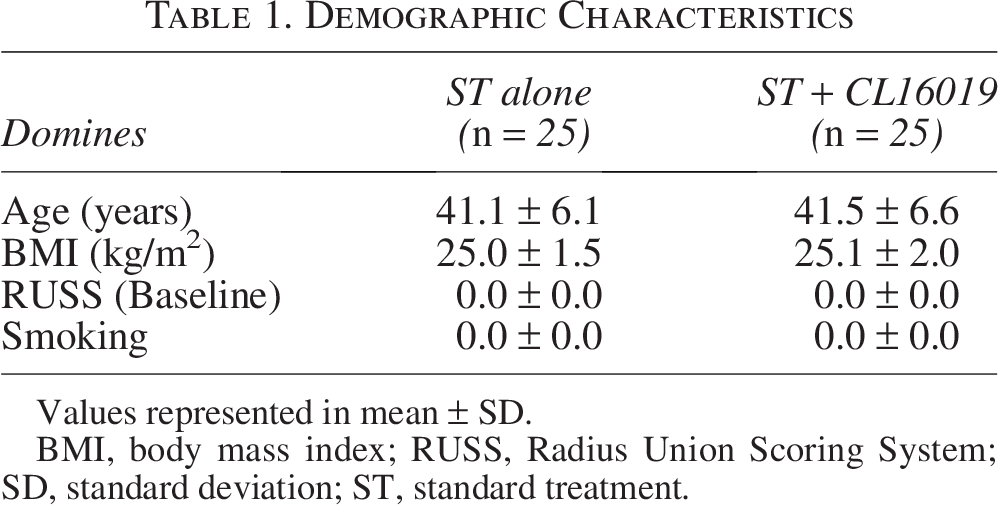
Values represented in mean ± SD.
BMI, body mass index; RUSS, Radius Union Scoring System; SD, standard deviation; ST, standard treatment.
Radiological Assessment for Improvement in Fracture Healing Using Radius Union Scoring System (RUSS)
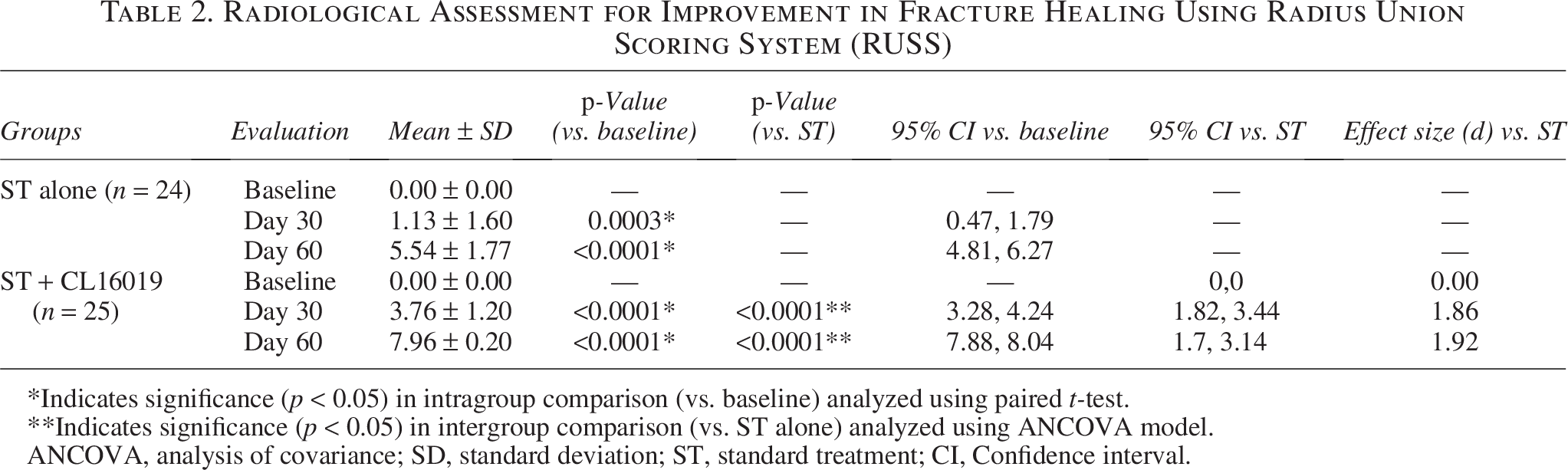
*Indicates significance (p < 0.05) in intragroup comparison (vs. baseline) analyzed using paired t-test.
**Indicates significance (p < 0.05) in intergroup comparison (vs. ST alone) analyzed using ANCOVA model.
ANCOVA, analysis of covariance; SD, standard deviation; ST, standard treatment; CI, Confidence interval.
Participants were assessed for pain, swelling, and tenderness due to their DRFs on baseline, days 7, 15, 30, 45, and 60. Participants in both the ST and ST + CL16019 groups reported significant decreases in their levels of pain, tenderness, and swelling on their respective evaluation days. For pain, the ST + CL16019 group improved from 8.56 to 7.68 by day 7 (p < 0.0001), while ST alone improved from 8.67 to 7.96 (p = 0.0004); by day 15, the difference became significant (6.76 vs. 7.42, p = 0.0245), and by day 60, pain reduced more dramatically with CL16019 (2.92 vs. 4.54, p < 0.0001). Similar trends were seen for swelling, where early reductions were significant in both groups (day 7: 7.20 vs. 7.58), but the difference reached significance by day 45 (4.16 vs. 5.13, p = 0.0171) and day 60 (2.96 vs. 4.29, p = 0.0046). For tenderness, both groups improved by day 7 (6.96 vs. 7.29), with statistically significant group differences emerging at day 45 (3.60 vs. 5.08, p < 0.0001) and further widening by day 60 (2.68 vs. 4.38, p = 0.0002). These results underscored the early onset and sustained efficacy of CL16019 as an effective adjunct therapy (Table 3).
Assessment of Pain, Swelling, and Tenderness Using Visual Analog Scale (VAS)
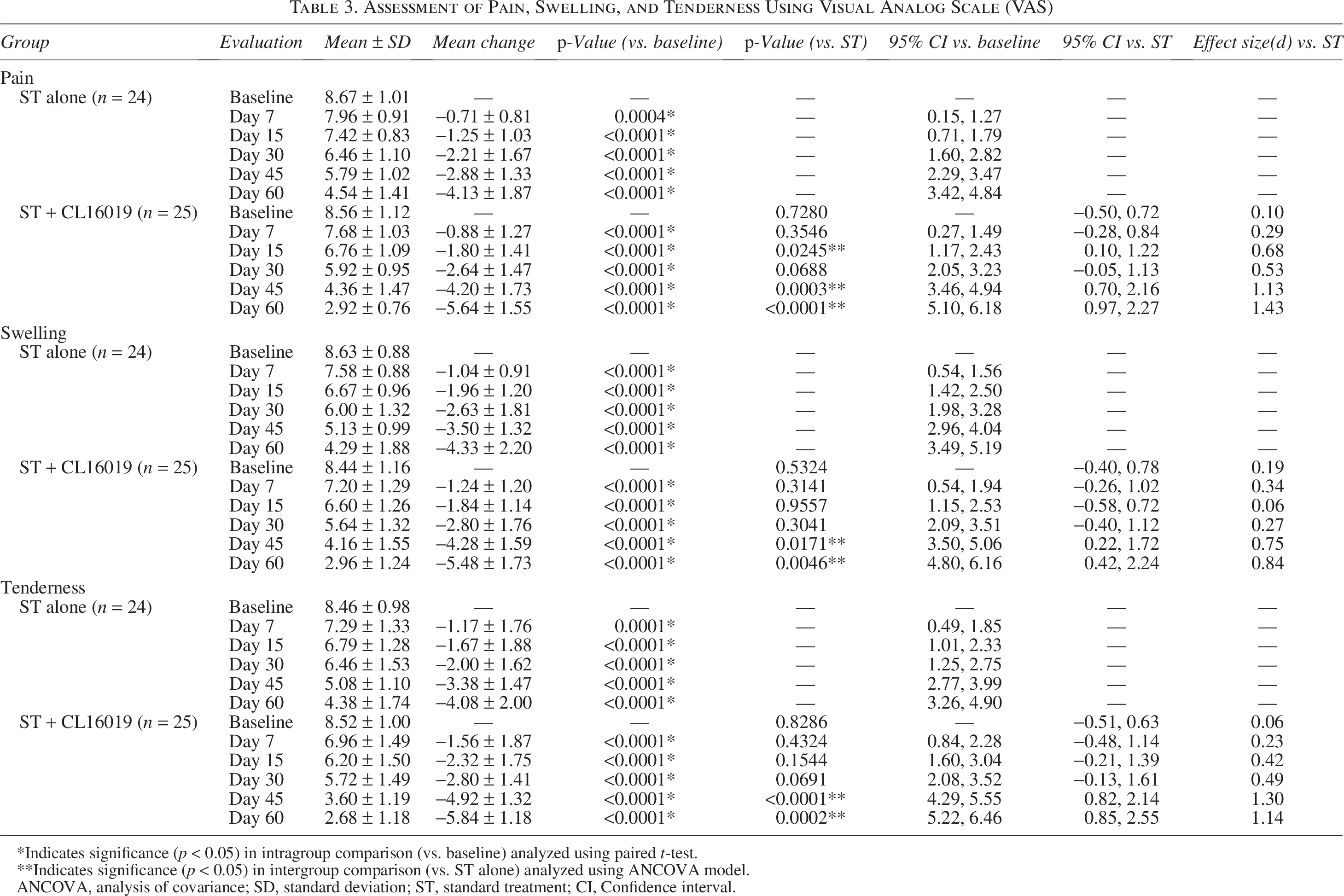
*Indicates significance (p < 0.05) in intragroup comparison (vs. baseline) analyzed using paired t-test.
**Indicates significance (p < 0.05) in intergroup comparison (vs. ST alone) analyzed using ANCOVA model.
ANCOVA, analysis of covariance; SD, standard deviation; ST, standard treatment; CI, Confidence interval.
The degree of improvements in pain, specific function, and usual activities assessed using PRWEQ scores in the ST and ST + CL16019 groups on days 30 and 60 are presented in Table 4. At day 60, the PRWEQ pain subscore was greatly reduced in the ST + CL16019 group compared with the ST group (19.60 ± 5.84 vs. 23.71 ± 9.65). The ST + CL16019 group had greater improvements than ST group in “specific activities scores” (27.96 ± 11.35 vs. 21.40 ± 8.27; p = 0.0334) by day 60. In addition, significantly better improvements were observed in the ST + CL16019 group in “usual activities” scores (18.25 ± 7.57 vs. 13.80 ± 5.44; p = 0.0199) and total PRWEQ scores (46.81 ± 18.76 vs. 37.20 ± 12.24; p = 0.0508) by day 60.
Assessment of Wrist Function Using Patient-Rated Wrist Evaluation Questionnaire (PRWEQ)
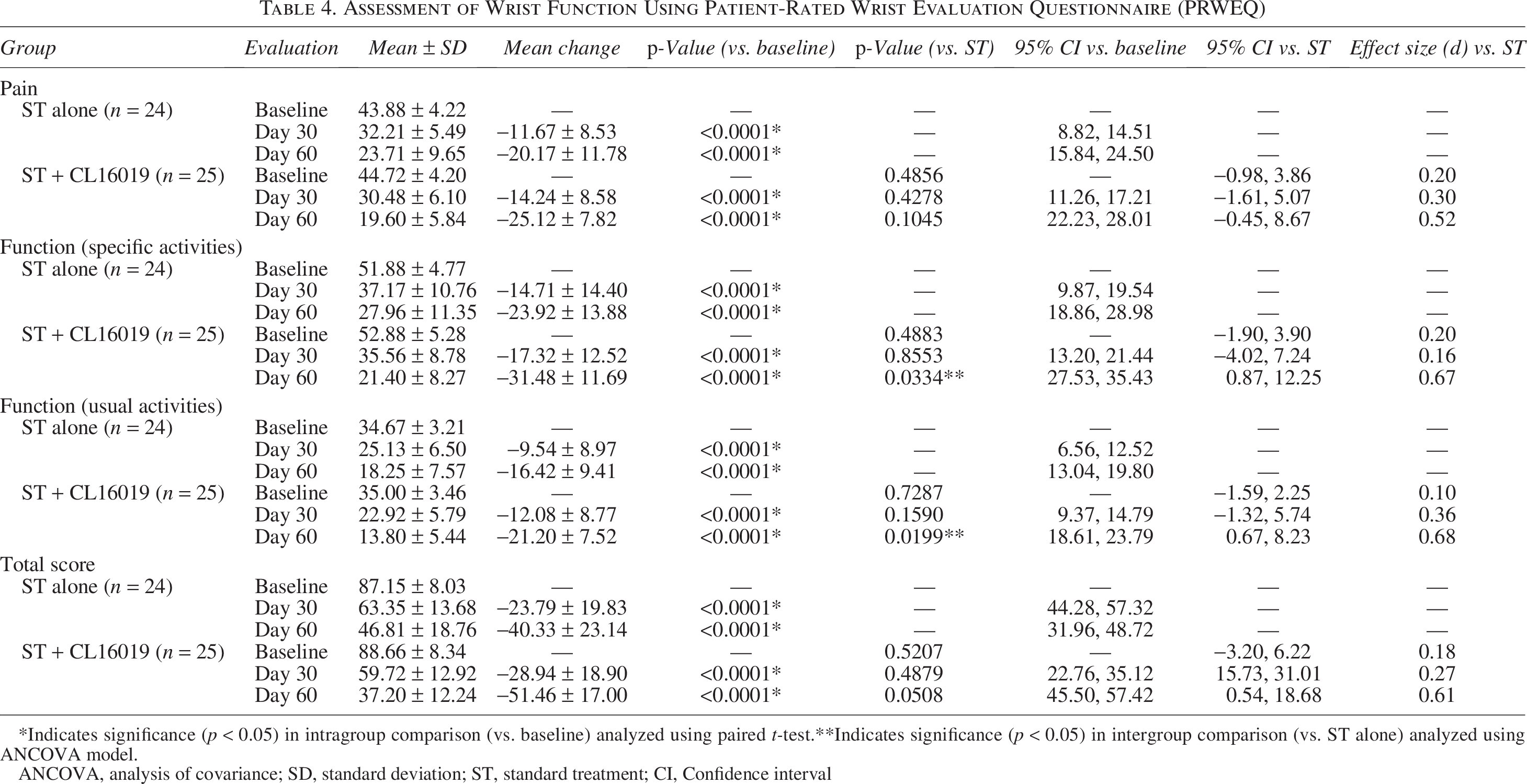
*Indicates significance (p < 0.05) in intragroup comparison (vs. baseline) analyzed using paired t-test.**Indicates significance (p < 0.05) in intergroup comparison (vs. ST alone) analyzed using ANCOVA model.
ANCOVA, analysis of covariance; SD, standard deviation; ST, standard treatment; CI, Confidence interval
Handgrip strength measurements at day 60 were not significantly different between the groups (Table 5). As presented in Table 6, the serum BAP and PTH levels were increased in both the ST and ST + CL16019 groups compared with respective baseline values, which was statistically significant only in the ST + CL16019 group. Considering the therapeutic response as per physician, all the participants in the ST + CL16019 group had “much improvement” at day 60, while only 16% of participants in the ST group showed such effect. Similarly, as per the participants’ assessment, 88% of participants in the ST + CL16019 group had “much improvement” at day 60, while only 24% of participants in the ST group showed such effect.
Assessment Hand Grip Strength (kg)
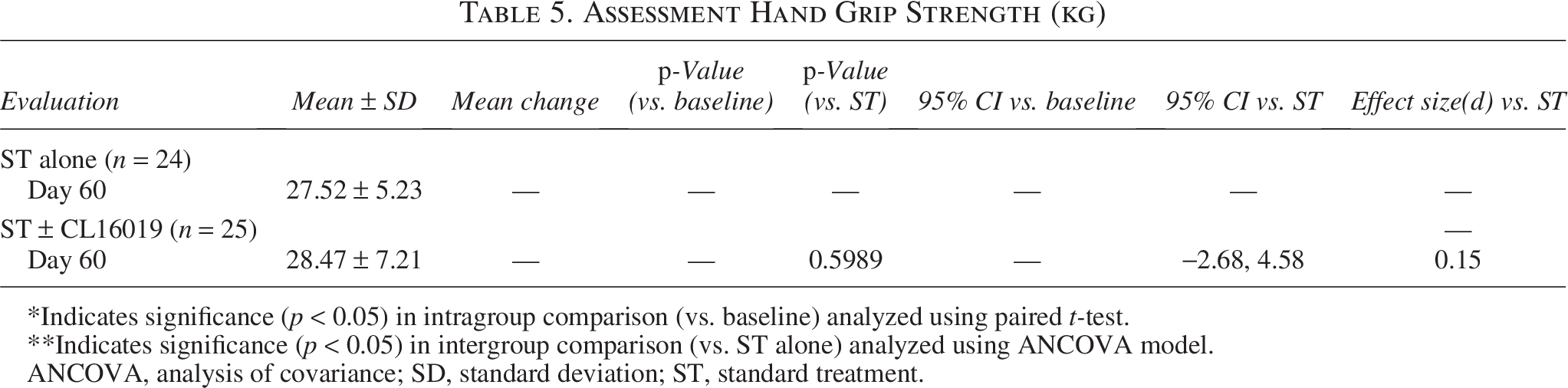
*Indicates significance (p < 0.05) in intragroup comparison (vs. baseline) analyzed using paired t-test.
**Indicates significance (p < 0.05) in intergroup comparison (vs. ST alone) analyzed using ANCOVA model.
ANCOVA, analysis of covariance; SD, standard deviation; ST, standard treatment.
Assessment of Biomarkers and Phytochemical Constituents in Plasma
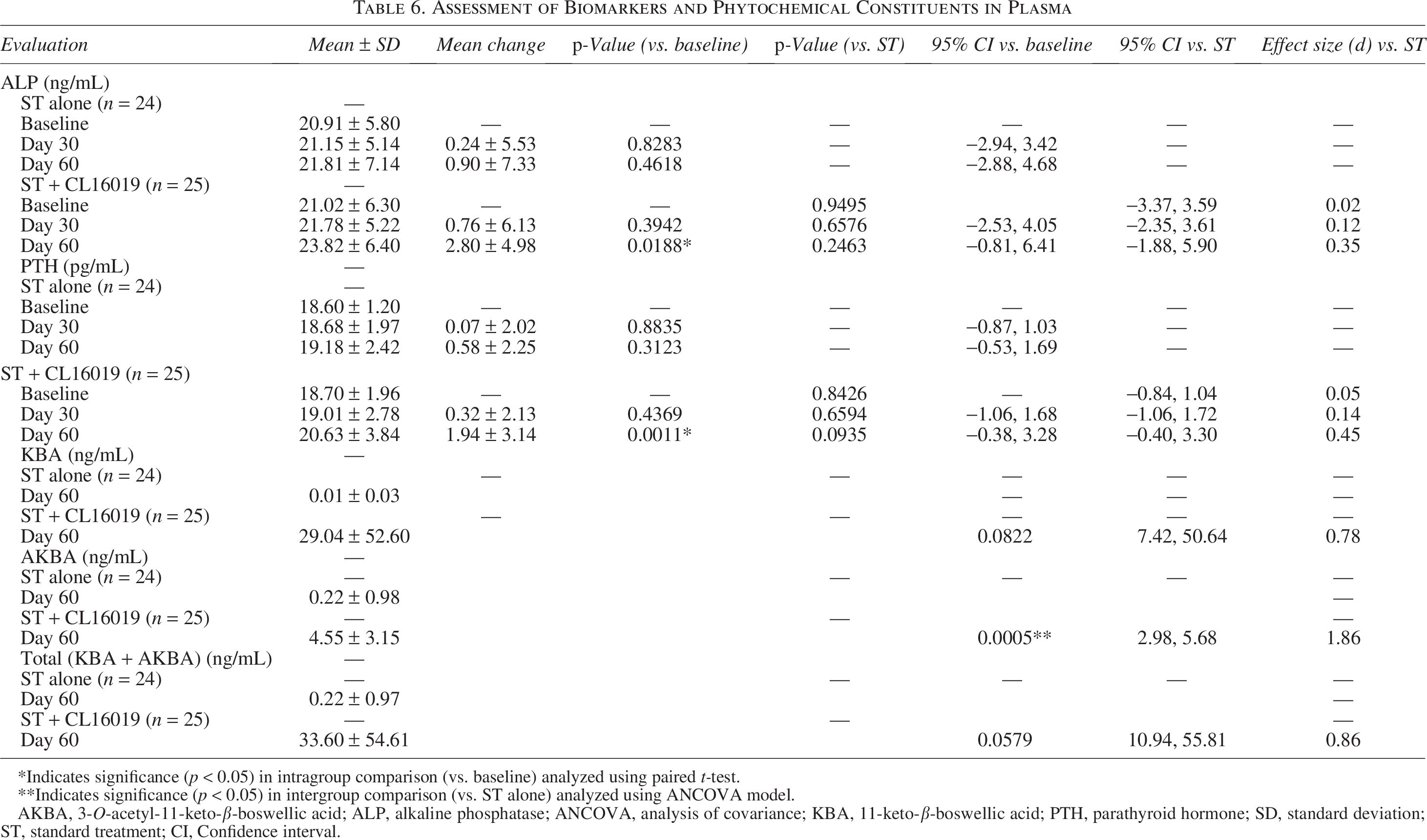
*Indicates significance (p < 0.05) in intragroup comparison (vs. baseline) analyzed using paired t-test.
**Indicates significance (p < 0.05) in intergroup comparison (vs. ST alone) analyzed using ANCOVA model.
AKBA, 3-O-acetyl-11-keto-β-boswellic acid; ALP, alkaline phosphatase; ANCOVA, analysis of covariance; KBA, 11-keto-β-boswellic acid; PTH, parathyroid hormone; SD, standard deviation; ST, standard treatment; CI, Confidence interval.
High-performance liquid chromatography analysis revealed that plasma levels of KBA and AKBA were considerably higher in the ST + CL16019 group than the ST group, with p-values of 0.0822 and 0.0005, respectively (Fig. 4; Table 6).
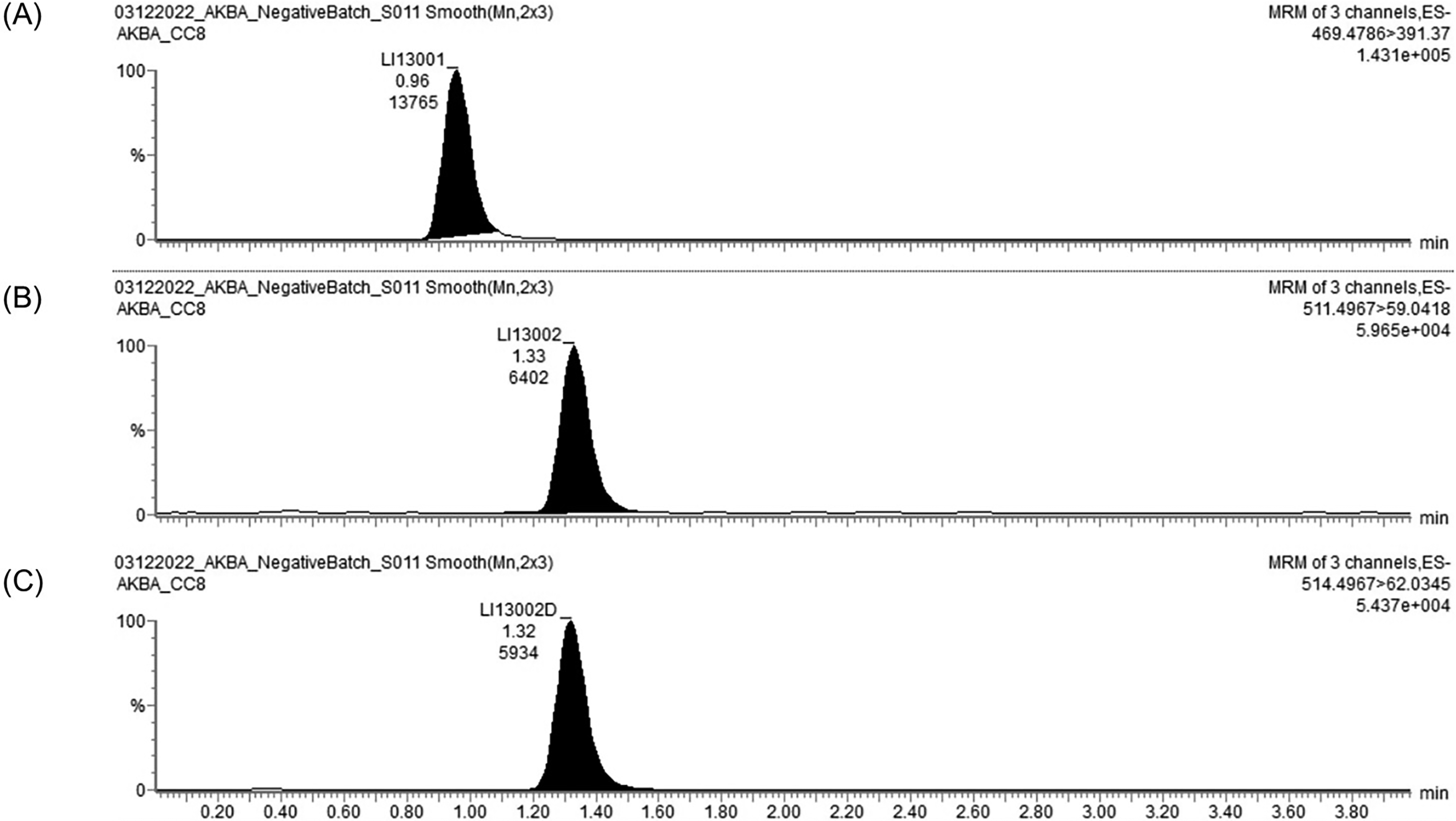
Liquid chromatography–mass spectrometry (LC–MS) chromatogram of
Two volunteers reported a “runny nose, classified as a mild AE” (Supplementary Table S2). None of the participants reported any serious AEs. Descriptive statistics of hematology, serum biochemistry, and lipid profile are summarized in Supplementary Table S3. During the trial duration, all these variables’ mean (or median) levels fell within typical reference ranges.
Discussion
Traditional herbal therapies have been proven to exhibit potent curative effects on functional disability of wrist joints after DRFs. 37 Currently, there is a growing interest in investigating the benefits of phytonutrients in healing bone fractures, reducing associated complications, and relieving pain in DRF subjects.38,39
Extracts of BS and CQ have demonstrated beneficial outcomes against bone health concerns in several in vitro, in vivo, and clinical trials.16,17,29–32 Our unpublished in vitro and in vivo research findings showed that CL16019 is safe. CQ and BS extracts promoted osteoblast differentiation, or the production of bone cells, and increased the BAP activity in vitro. In addition, they augmented the levels of osteoprotegerin in human osteoblast cell lines in a dose-dependent way.
In addition, oral supplementation of CL16019 at a daily dose of 300 mg/kg for 64 days showed better relative femur bone weight in the ovariectomized rat model of osteoporosis, indicating facilitation of bone formation by CL16019. Rats treated with CL16019 were protected from mild to moderate loss of trabecular architecture, thinning of trabeculae, widening of bone marrow/intertrabecular space, adipose tissue infiltration, and erosion of endosteal surface in the epiphysis of femur bones compared with disease control. CL16019 significantly lowered serum calcium levels, indicating reduced osteoclastic activity and improved osteoblastic activity. These findings suggest that CL16019 is safe and effective in ameliorating effects against ovariectomy-induced osteoporotic changes in Sprague Dawley rats (unpublished data).
However, the potential of CL16019 in healing bone fractures has not been investigated. In this context, the present clinical study, for the first time, evaluated the efficacy and tolerability of CL16019 when administered concurrently with ST in promoting fracture healing in human volunteers with DRF.
The radiological assessment for improvement in fracture healing using the RUSS results suggests that CL16019 was more effective than the ST alone arm in callus formation and cortical bridging in volunteers with DRFs. This indicated faster fracture healing with the CL16019 arm. CQ, a component of CL16019, is reported to build up the necessary components, including phosphorus, calcium, collagen, and mucopolysaccharides, for the healing of fractured bone. Swift utilization of these components accelerates fracture healing. In addition to the greater accumulation of mucopolysaccharides, CQ also facilitates the early disappearance of mucopolysaccharides from the fractured area, associated with the earlier calcification and firm callus formation. 40 AKBA, a principal phytochemical of BS, enhances the osteogenic differentiation potential of bone marrow mesenchymal stem cells in vitro. 40
Clinical presentation of DRFs includes distal radius pain, swelling, and tenderness of the affected area of the limb. These factors limit the mobility of the volunteers. CL16019 showed significantly greater improvements in all three clinical features, viz., pain, swelling, and tenderness, than the ST alone-treated arm. Earlier reports also showed a reduction in pain, swelling, and tenderness by CQ in participants with Colle’s fractures. 41 Nutraceutical formulations containing boswellic acids are known for reducing pain and improving mobility through their anti-inflammatory mechanisms. 42
Open fixation, immobilization, pain, swelling, and tenderness limit the wrist function to perform usual and specific activities in DRF volunteers. CL16019 cotreatment showed better improvements in all three domains of the PRWEQ compared with the ST alone group. CL16019-treated volunteers have less pain while performing repeated wrist movements or lifting objects. Furthermore, they also reported better wrist function during specific activities (turning on the doorknob, fastening buttons, pushing with the affected hand, carrying any object, handling a bath towel, etc.) and usual activities (personal care, household work, and recreational activities). An increase in the levels of BAP is an indicator of fracture healing. 43
In addition, CL16019 cotreatment led to elevated levels of serum PTH. By promoting bone regeneration, PTH plays a key role in fracture healing. 44 This may speed up the healing process. Greater scores of PGA and SGA scores in CL16019 groups support better recovery in volunteers. Volunteers cotreated with CL16019 showed higher levels of BAP in serum on days 30 and 60. Higher plasma concentrations of phytochemicals such as KBA and AKBA in the CL16019 group substantiate our claim of supporting fracture healing and restoring wrist function in DRFs.
However, this study is associated with some limitations. This study did not assess the plasma concentrations of the phytochemicals in CQ extract and the impact of treatment on various stages of bone healing and dynamics of blood flow, that is, the resistive index through the affected area. There were no safety issues with CL16019 cotreatment throughout this investigation. Only a few hematological and biochemistry markers showed differences across groups that were not clinically significant (Supplementary Table S3).
Conclusions
Cotreatment of CL16019 (Ostibind™) with ST supported the healing of DRFs by promoting callus formation and bridging of cortices. Moreover, CL16019 reduced the pain, swelling, and tenderness and significantly improved wrist function without any AEs in subjects with DRFs. Although this study has certain limitations, such as the shorter duration of supplementation and the lack of assessment of bone healing stages, the positive outcomes observed should not be understated. Together, the findings of the present study suggest that CL16019 might be a beneficial adjunct to the ST for faster healing of DRFs.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Authors’ Contributions
A.V.V.P.M.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, validation, visualization, writing—original draft, and writing—reviewing and editing. N.R.S.: Data curation, formal analysis, investigation, methodology, validation, writing—original draft, and writing—reviewing and editing. C.K.M.: Data curation, formal analysis, investigation, methodology, validation, writing—original draft, and writing—reviewing and editing. V.P.S.: Data curation, formal analysis, investigation, methodology, validation, and writing—reviewing and editing.
Footnotes
Acknowledgments
The authors are thankful to the subjects, study monitors, and the medical team for their meticulous support.
Data Availability Statement
The data presented in this study including statistical analysis plan are available on request from the corresponding author. The data are not publicly available due to confidentiality and ethical reasons.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Chemiloids Life Sciences Pvt. Ltd. (Grant number
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.