
Abstract
Background:
Probiotics have been suggested as therapeutic agents for acute gastroenteritis (AG) in children. However, the optimal probiotic strains, doses, and durations of supplementation remain unclear.
Objective:
This umbrella meta-analysis was conducted to assess the clinical efficacy of different strains of probiotics on AG.
Methods:
To gather pertinent evidence, a search was conducted on PubMed and Scopus from their inception up to October 12, 2025. Standardized mean difference and relative risk with their 95% confidence interval were used as the metrics for assessing treatment effects on continuous and binary outcomes, respectively.
Results:
A total of 36 eligible meta-analyses (MAs), including 107,541 participants, were included. The analysis showed that probiotics may help prevent the incidence of AG and decrease the duration of diarrhea, vomiting, fever, length of hospital stays, as well as the frequency of stool and the presence of diarrhea on specific days post-treatment. However, the effects were found to be strain-specific and, for certain outcomes, were influenced by the dose (colony-forming units) and duration of treatment. Overall, the most effective probiotics in terms of efficacy on AG symptoms were Saccharomyces boulardii CNCM I-745, Lacticaseibacillus rhamnosus GG (formerly Lactobacillus rhamnosus GG; ATCC 53103), Limosilactobacillus reuteri DSM 17938 (formerly Lactobacillus reuteri), Lactiplantibacillus acidophilus, Bacillus clausii O/C, Bifidobacterium animalis subsp. lactis BB-12 (formerly Bifidobacterium lactis), and a combination of Lactobacillus acidophilus spp.+ Bifidobacterium spp. Probiotics were effective in both viral and bacterial acute AG in inpatient and outpatient settings. The effects of probiotics on certain outcomes were dose- and duration-dependent, although these effects varied across strains and clinical settings.
Conclusions:
This study indicates that probiotics have the potential to prevent AG and reduce associated symptoms in children.
Introduction
Acute gastroenteritis (AG) is a common diarrheal disease in children, characterized by inflammation of the gastrointestinal tract, often accompanied with symptoms such as vomiting, fever, nausea, and abdominal pain. 1 AG remains a major public health issue and is the fifth leading cause of mortality in children under five. 2 In addition, AG leads to high hospitalization rates and health care costs. 3 AG can cause dehydration and electrolyte imbalances in children, leading to serious issues such as stunted growth, malnutrition, and impaired cognitive development.4,5 AG in children is caused by various pathogens, including viruses (norovirus and rotavirus), protozoa, and bacteria. 6 While many countries have recently implemented rotavirus vaccination, this preventive measure has not significantly reduced the burden of AG. 7 Therefore, prioritizing effective management of AG remains crucial.
At present, the approach to managing childhood AG mainly emphasizes the use of oral rehydration salts (ORS) and ongoing nutritional support to prevent and treat dehydration. 8 However, ORS cannot alleviate diarrheal symptoms and address gut microbiota dysbiosis. 9 The disruption of intestinal microflora is a key characteristic of AG and its associated symptoms. 10 Recently, there has been increasing interest in the use of probiotics as a potential complementary treatment. 11 Probiotics could boost host immunity, restore balance to intestinal microflora, and improve gut barrier function. 12 The current research on probiotics for AG in children has made significant progress, yet several potential gaps remain that warrant further investigation. Discrepancies exist regarding the overall effectiveness of different probiotics strains and formulations on AG. While some meta-analyses (MAs) indicate that probiotics can effectively reduce the duration of diarrhea and stool frequency,13,14 several other MAs revealed minimal or no benefits. 15 A recent large randomized clinical trial (RCT) in the USA involving 971 children aged 3 months to 4 years found no differences in outcomes, including diarrhea duration and daycare absence, between those receiving Lacticaseibacillus rhamnosus GG (formerly Lactobacillus rhamnosus GG; ATCC 53103; hereafter LGG) and a placebo over 5 days. 16 Another RCT in Vietnam found that Lactobacillus acidophilus (e.g., ATCC 4356 or NCFM; hereafter L. acidophilus) administered at a dosage of 4 × 108 colony-forming units (CFU) twice daily had no significant effect on the duration of diarrhea and stool frequency during the first three days after enrollment. 17 In addition, the Cochrane Database of Systematic Reviews concluded that probiotics have minimal or no impact on the number of individuals experiencing diarrhea that lasts 48 h or more, and it remains unclear whether probiotics can shorten the duration of diarrhea. There were concerns about publication bias, significant heterogeneity in results, and potential biases in many studies included in the review. 15
The inconsistency highlights the need for a comprehensive evaluation of the existing literature to clarify the overall impact of various strains of probiotics on AG outcomes in children. The most effective probiotic for children with AG remains controversial. Besides, the effectiveness of multi-strain probiotics compared to single strains is yet to be evaluated. Moreover, there is considerable variability in the dosages and durations of probiotic administration across studies, which complicates comparisons and generalizations. An umbrella MA serves as a valuable tool for synthesizing findings from multiple MAs, providing a higher level of evidence regarding the effectiveness of interventions. This umbrella MA was conducted to thoroughly investigate the effects of a wide range of single-strain and multi-strain probiotics, considering different doses and treatment durations, on AG in children. The aim was to identify the most effective probiotics, as well as the optimal dosage and treatment duration for managing AG in this population.
Materials and Methods
Search strategy
This report adheres to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. 18 To gather pertinent evidence, a search was conducted on PubMed and Scopus from their inception up to October 12, 2025. The primary search terms and MESH headings utilized for the search strategy are presented in Supplementary Table S1. The search was restricted to publications written in English. In addition, the reference lists of the identified MA were examined to find any other relevant research.
Inclusion criteria
Following the PICO framework, all pertinent MAs of RCTs that met the following criteria were included: Participants: Patients were children under 18 years old diagnosed with AG; Intervention: Probiotics administered at any dose, regardless of the strain; Comparator: Placebo; Outcomes: The primary outcome was the duration of diarrhea, while secondary outcomes included the length of hospitalization, length of fever, duration of vomiting, prevention of AG, presence of diarrhea on days 1 to ≥7, the frequency of diarrhea at various time points (days 1 to ≥7). We excluded letters, qualitative reviews, protocols, MA with unrelated interventions, abstracts, and proceedings from scientific conferences. Eligibility was assessed by two independent investigators, with the senior investigator resolving any disagreements between them.
Data extraction and quality assessment
Two investigators independently evaluated quality evaluation and extracted data using a standardized data extraction form, with any discrepancies resolved by consulting a third author. The following information was collected: author, year of publication, sample size, number of studies included, risk of bias assessment, effect sizes for outcomes, country, mean age, type of intervention, and dose and duration of treatment. If additional information was needed, the authors of the MA were contacted for further data. The methodological quality of the MA was assessed using the AMSTAR 2 tool, which comprises 16 items—7 of which are considered critical for determining the overall quality of a review. AMSTAR 2 categorizes reviews as “high,” “moderate,” “low,” or “critically low” quality. 19
Calculating the overlap
Calculating overlap is essential in umbrella reviews since primary studies may appear in multiple MAs, which can bias results. Overlap was assessed visually through a citation matrix and quantified using three indices, including percentage of overlaps, covered area (CA), and corrected covered area (CCA) based on the following formulas:20,21
% Overlaps = number of primary RCTs included in more than one MA/r

N: Total number of primary RCTs including duplicates
r: Number of rows or total number of primary RCTs
c: Number of columns or MAs
The overlap status was interpreted using the CCA score: values between 0 and 5 indicate a mild overlap, 6–10 signify a moderate overlap, 11–15 reflect a high overlap, and scores above 15 represent a very high degree of overlap.
Statistical analysis
Our analysis was based on pooling summary effect estimates from published MAs, not individual primary studies. This approach is consistent with the methodology used in previous umbrella reviews,22–25 where the aim is to synthesize findings across multiple MAs rather than re-analyzing individual study data. Pooling effect sizes from MAs and pooling individual studies rely on the same fundamental statistical methods. Mean difference (MD) and 95% confidence interval (95% CI) were used as the metrics for assessing treatment effects on continuous outcomes. For binary outcomes, relative risk (RR) and 95% CI were employed. Data were combined using random-effects models suggested by DerSimonian and Laird. 26 The degree of heterogeneity among MA was evaluated using the I2 test, with I2 values exceeding 50% indicating a significant level of heterogeneity. When at least 10 effect sizes were available, publication bias was examined using Egger tests and funnel plots, where a p-value of less than 0.05 suggests the presence of publication bias. Sensitivity analysis was conducted by sequentially removing individual MAs to evaluate the impact of each study on the overall outcomes. Prespecified subgroup analyses were carried out based on quality of studies (low, moderate, and high), sample size (≥2000 vs. <2000 participants), etiology of disease (rotaviral, bacterial, nosocomial, and parasitic) type of probiotics, duration (≥6 vs. <6 days), dosage (≥1010 versus <1010 CFU), and symptom severity (inpatients vs. outpatients). In addition, meta-regression analysis was performed to determine whether the results were influenced by the number of included studies, sample size, and the proportion of primary studies with low risk of bias. Statistical analyses were conducted using STATA software (Version 15.1).
Results
Study selection
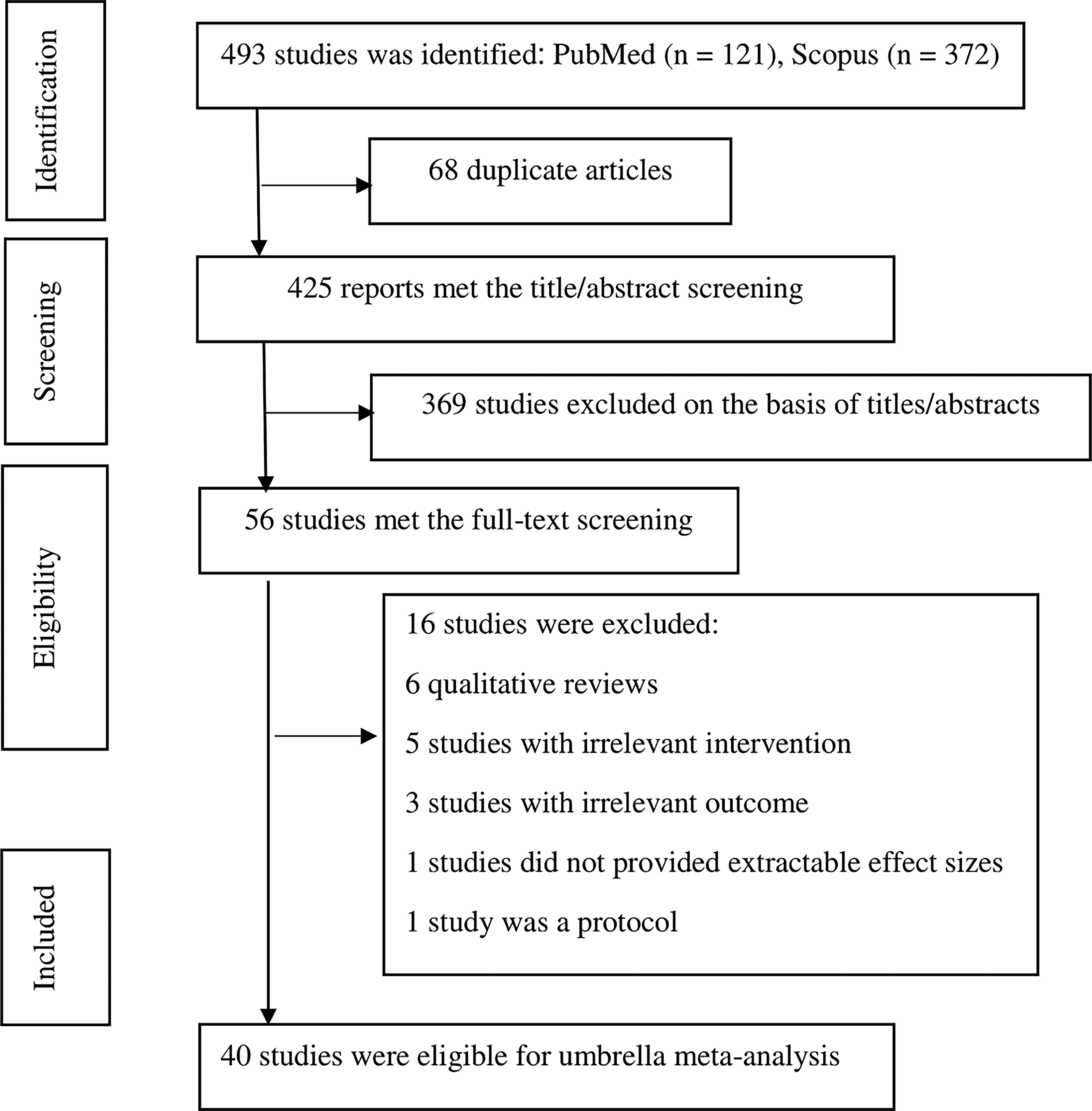
The literature search identified 491 citations, with 64 studies being duplicates. Following a thorough review of the titles and abstracts, 377 irrelevant citations were eliminated. A full-text evaluation of 50 potentially relevant studies led to the inclusion of 40 MAs in the analysis.13–15,22,27–62 The selection process is detailed in Figure 1. These 36 eligible MAs collectively provided 78 effect sizes associated with various probiotic interventions. The interventions examined included multi-strain probiotics in 15 MAs, Saccharomyces boulardii CNCM I-745 (S. boulardii) in 14 MAs, L. acidophilus in 8 MAs, LGG in 14 MAs, Lactobacillus spp. in 4 MAs, Bifidobacterium spp. in 2 MAs, a mixture of L. acidophilus spp.+ Bifidobacterium spp. in 3 MAs, Limosilactobacillus reuteri DSM 17938 (formerly Lactobacillus reuteri; hereafter L. reuteri) in 9 MAs, Bifidobacterium animalis subsp. lactis BB-12 (formerly Bifidobacterium lactis; hereafter B. lactis) in 2 MAs, Bacillus coagulans (formerly misclassified as Lactobacillus sporogenes) in 2 MAs, Bacillus clausii O/C (B. clausii) in 3 MAs, and Enterococcus faecium SF68 in 2 MAs (Table 1). The most commonly used probiotic strains were S. boulardii, L. acidophilus, LGG, and L. reuteri. The daily doses of probiotics varied from 0.02 × 1010 to 14.6 × 1010 CFU, with supplementation durations ranging from 3 to 105 days and a median follow-up period of 6 days. Sample sizes across the MA ranged from 304 to 13,443 participants, totaling 107,541 individuals. The number of primary studies included in each MA varied from 2 to 63, with a median of 18 studies. Bias in the primary studies was assessed using the Cochrane tool 63 or the Jadad scale, 64 , revealing significant variability in the proportion of high-quality studies, ranging from 0% to 85% in each MA. For the duration of diarrhea, data were reported in 38 MA (76 effect sizes).13–15,22,27–41,44–62 Prevention of AG was assessed in 3 MAs (5 effect sizes).42,43,53 Duration of hospitalization was reported in 20 MAs (32 effect sizes),13–15,28,31,33–38,40,41,44–47,52–58 and duration of vomiting in 7 MAs (12 effect sizes).13,37,38,41,45,49,58 Duration of fever was reported in 3 MAs (10 effect sizes).13,41,58 Presence of diarrhea on specific days after treatment initiation were reported as follows: day 1 after treatment initiation in 6 MAs (6 effect sizes),14,34,43,45,53,59 day 2 in 12 MAs (21 effect sizes),13–15,31,43–45,49–51,53,59 day 3 in 21 MAs (29 effect sizes),14,15,28,31–35,38,43–47,49–53,58,59 day 4 in 13 MAs (15 effect sizes),14,28,31,32,38,43–45,47,49,52,53,59 day 5 in 7 MAs (7 effect sizes),14,31,43–45,50,53 day 6 in 4 MAs (4 effect sizes),43,45,49,53 and day ≥7 in 7 MAs (7 effect sizes).31,44,45,49–51,53 Presence of stool frequency on specific days after treatment initiation were reported as follows: day 1 after treatment initiation in 9 MAs (11 effect sizes),14,29,31,36,38,40,41,45,49 day 2 in 11 MAs (22 effect sizes),13,14,28,29,31–33,38,45,54,59 day 3 in 11 MAs (13 effect sizes),14,28,29,31,32,34,38,40,45,49,58 day 4 in 6 MAs (6 effect sizes),14,29,31,40,45,49 day 5 in 3 MAs (3 effect sizes),29,40,45 day 6 in 3 MAs (3 effect sizes),31,45,49 and day ≥7 in 3 MAs (3 effect sizes).31,45,49 According to AMSTAR-2 criteria, the quality assessment classified 12 MAs as high quality, 18 as moderate quality, and 6 as low quality. Table 1 summarizes the characteristics of the included MAs.
Flow diagram of the study.
Characteristics of Eligible Studies
AG, acute gastroenteritis; CFU, colony-forming unit; NR, not reported.
Overlap calculation
In the citation matrix (Supplementary Data S1), 40 MAs were arranged in columns, while 221 primary RCTs were presented in rows. Using the provided formulas, overlap metrics were calculated as follows:
Total number of primary RCTs including duplicates (N) = 828
Total number of RCTs (rows (r)) = 221
Number of MAs (columns (c)) = 40.
% Overlap = number of RCTs included in more than one MA/total number of RCTs = 136/221 = 61%


The percentage overlap was 61%, the CA was 0.09, and the CCA was 0.07, reflecting a mild degree of overlap among primary studies across MAs. The CCA of 0.07 indicates that most primary studies were unique to individual MAs, ensuring that the results were not overly biased by duplicated data.
Quantitative synthesis
Incidence of AG
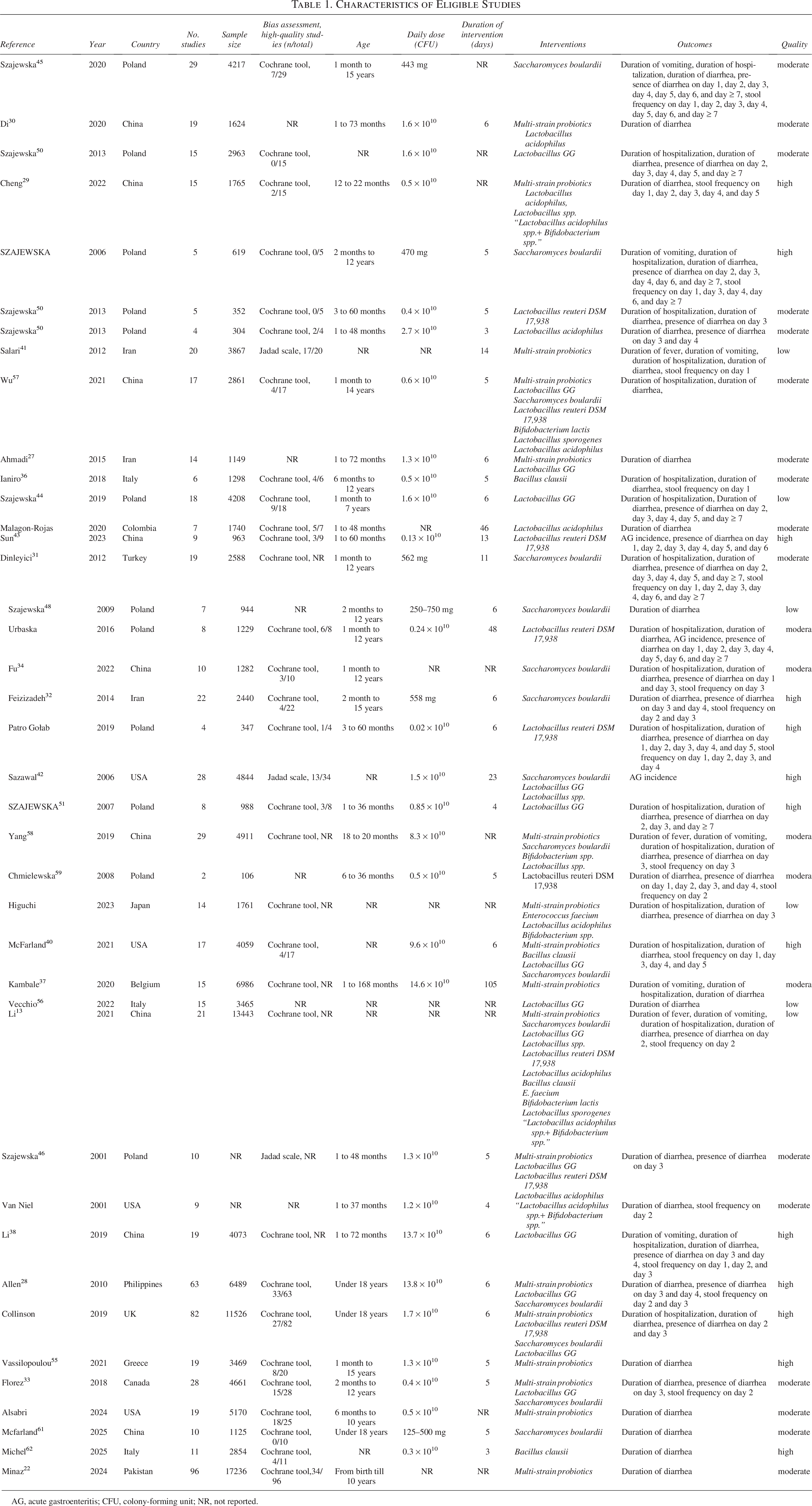
The results of the overall analysis and subgroup analysis based on the sample size, quality of MA, and dose and duration of treatment for all outcomes are presented in Table 2. A combined analysis of all the data indicated that probiotics did not significantly lower the risk of AG incidence. There was considerable heterogeneity among the MA (I2 = 67.9%, p = 0.01) (Fig. 2). In the subgroup analysis, the risk of AG was reduced at higher doses of probiotics (≥1010 CFU), in MA with larger sample sizes, and particularly when LGG (RR = −0.89, 95% CI: −1.04, −0.74) was administered. However, no significant effects were noted for other types of probiotics (Fig. 2, Table 2).
Pooled analysis for the effect of probiotics on the incidence of acute gastroenteritis.
Overall and Subgroup Analyses for the Effect of Probiotics on Acute Gastroenteritis in Children
95% CI, 95% confidence interval; CFU, colony-forming unit; NR, not reported; RR, relative risk; SMD, standardized mean difference.
Duration of diarrhea
When all effect sizes were pooled, probiotics significantly reduced the duration of diarrhea (Standardized mean difference [SMD] = −0.83 days, 95% CI: −0.98, −0.69), which was supported across subgroups based on sample size, quality of MA, as well as dose and duration of treatment. This effect was found for multi-strain probiotics (SMD = −0.91, 95% CI: −1.10, −0.72), S. boulardii (SMD = −1.01, 95% CI: −1.13, −0.90), LGG (SMD = −0.99, 95% CI: −1.20, −0.78), Lactobacillus spp (SMD = −0.35, 95% CI: −0.64, −0.06), L. reuteri (SMD = −1.12, 95% CI: −1.29, −0.95), B. lactis (SMD = −2.55, 95% CI: −3.30, −1.80), and B. clausii (SMD = −0.40, 95% CI: −0.71, −0.08), of which B. lactis and L. reuteri showed the highest efficacy, respectively (Fig. 3, Table 2).
Pooled analysis for the effect of probiotics on the duration of diarrhea (day).
Overall and subgroup analyses were conducted to evaluate which strains and doses are most effective for viral and bacterial AG. All probiotics reduced the duration of rotaviral AG, with S. boulardii and Lactobacillus GG showing the highest efficacy, particularly at doses ≥1010 CFU. For bacterial AG, only S. boulardii at doses ≥1010 CFU was effective. L. reuteri DSM 17,938 was effective in reducing the duration of nosocomial AG. S. boulardii was also effective in AG of unknown cause but was not effective against parasitic AG (Table 3). When subgroup analysis was conducted based on symptom severity, probiotics were effective in reducing the duration of AG in both inpatient and outpatient settings. S. boulardii, B. clausii, and L. reuteri DSM 17,938 were the most beneficial strains for reducing the duration of AG in inpatients. For outpatients, Lactobacillus GG was the most effective strain, followed by multi-strain probiotics and S. boulardii. Subgroup analyses were conducted according to the dose of probiotics within both the inpatient and outpatient populations. The results indicated that the effect of probiotics in both subgroups was not influenced by the administered dose (Table 3).
Overall and Subgroup Analyses for the Effect of Probiotics on Duration of Acute Gastroenteritis Based on Etiology and Symptom Severity
95% CI, 95% confidence interval; CFU, colony-forming unit; SMD, standardized mean difference.
Duration of hospitalization
The overall effect size for hospitalization when comparing probiotics to placebo across all included data was −0.82 days (SMD = −0.82 days, 95% CI: −0.92, −0.72), which was supported across all subgroups. This effect was identified for multi-strain probiotics (SMD = −0.84, 95% CI: −1.03, −0.65), S. boulardii (SMD = −0.89, 95% CI: −1.04, −0.74), LGG (SMD = −1.07, 95% CI: −1.50, −0.63), L. reuteri (SMD = −0.73, 95% CI: −1.15, −0.30), and B. clausii (SMD = −0.73, 95% CI: −1.28, −0.18), of which LGG demonstrated the highest efficacy (Fig. 4, Table 2).
Pooled analysis for the effect of probiotics on duration of hospitalization (day).
Presence of diarrhea on various days after treatment initiation
The forest plots illustrating the effect of different probiotics on the presence of diarrhea from day 1 to day ≥7 after treatment initiation are presented in Supplementary Figures S1, S2, S3, S4, S5, S6, and S7. In the overall analysis, probiotics reduced the risk of diarrhea compared to placebo on day 2 (RR = 0.52, 95% CI: 0.44, 0.61), day 3 (RR = 0.54, 95% CI: 0.48, 0.61), day 4 (RR = 0.63, 95% CI: 0.53, 0.75), and day ≥7 (RR = 0.35, 95% CI: 0.18, 0.70) (Table 2). However, in the stratified analysis, the risk of diarrhea on day 1 was reduced in MA with <2000 participants (Table 2), but no strain-specific effect was identified (Supplementary Fig. S1). The presence of diarrhea on day 2 was significantly reduced after receiving S. boulardii (RR = 0.54, 95% CI: 0.40, 0.73), LGG (RR = 0.52, 95% CI: 0.34, 0.80), L. reuteri (RR = 0.42, 95% CI: 0.28, 0.61), and a combination of L. acidophilus spp.+ Bifidobacterium spp. (RR = 0.20, 95% CI: 0.05, 0.78) (Supplementary Fig. S2), which was supported across all other subgroups (Table 2). The odds of diarrhea on day 3 after treatment initiation was significantly deceased for multi-strain probiotics (RR = 0.61, 95% CI: 0.54, 0.69), S. boulardii (RR = 0.45, 95% CI: 0.35, 0.59), LGG (RR = 0.56, 95% CI: 0.46, 0.68), and L. reuteri (RR = 0.43, 95% CI: 0.30, 0.61) (Supplementary Fig. S3), a finding that was consistent across all other subgroups (Table 2). On day 4, the odds of diarrhea were also significantly decreased for multi-strain probiotics (RR = 0.41, 95% CI: 0.32, 0.53), S. boulardii (RR = 0.50, 95% CI: 0.37, 0.69), LGG (RR = 0.64, 95% CI: 0.50, 0.82), and L. acidophilus (RR = 0.69, 95% CI: 0.57, 0.83), although no significant effect was observed for L. reuteri (Supplementary Fig. S4). This finding was consistent across all subgroups except for low-quality MA and when the dose was less than <1010 CFU. On day 5, diarrhea was significantly reduced after treatment with S. boulardii (RR = 0.29, 95% CI: 0.19, 0.43), but not when LGG or L. reuteri were administered (Supplementary Fig. S5). High-quality MA involving ≥2000 participants demonstrated a significant positive effect of S. boulardii (RR = 0.48, 95% CI: 0.30, 0.80) on the presence of diarrhea on day 6, while no effect was observed for L. reuteri (Supplementary Fig. S6). Also, high-quality MA with ≥2000 participants showed a significant positive impact of S. boulardii (RR = 0.32, 95% CI: 0.20, 0.52) and LGG (RR = 0.25, 95% CI: 0.12, 0.50) on reducing the risk of diarrhea lasting for ≥7 days after treatment initiation (Supplementary Fig. S7) particularly when administered at a higher dose (≥1010 CFU) for a short duration (<6 days) (Table 2), while no effect was found for L. reuteri (Supplementary Fig. S7).
Stool frequency on various days after treatment initiation
The forest plots for the effect of different probiotics on stool frequencies on day 1 to day ≥7 after treatment initiation are presented in Supplementary Figures S8, S9, S10, S11, S12, S13, and S14. In the overall analysis, compared with placebo, probiotics reduced stool frequency on day 2 after treatment initiation (SMD = −0.72, 95% CI: −0.85, −0.59), on day 3 (SMD = −0.90, 95% CI: −1.26, −0.54), on day 4 (SMD = −0.78, 95% CI: −1.24, −0.32) and on day ≥7 (all MA used S. boulardii; SMD = −0.84, 95% CI: −1.15, −0.52), but not on days 1, 5, and 6 (Table 2). In the stratified analysis, MA of moderate quality with sample sizes under 2000 participants, doses below 1010 CFU, and intervention durations of <6 days indicated a significant reduction in stool frequency on day 1, but no strain-specific effect was observed (Supplementary Fig. S8). On day 2, stool frequency significantly decreased following the administration of multi-strain probiotics (SMD = −0.83, 95% CI: −1.14, −0.51), S. boulardii (SMD = −0.68, 95% CI: −0.88, −0.48), LGG (SMD = −0.64, 95% CI: −0.95, −0.33), L. reuteri (SMD = −1.55, 95% CI: −2.15, −0.95), and L. acidophilus spp.+ Bifidobacterium spp. (SMD = −1.15, 95% CI: −1.94, −0.35) (Supplementary Fig. S9). This reduction was consistent regardless of the dose and duration of the intervention. On day 3, stool frequency also significantly decreased with multi-strain probiotics (SMD = −0.80, 95% CI: −1.20, −0.40), S. boulardii (SMD = −1.36, 95% CI: −1.62, −1.10), and L. acidophilus (SMD = −0.61, 95% CI: −1.00, −0.22) (Supplementary Fig. S10). Notably, this effect was significant only when lower doses of probiotics were used. On day 4, a significant reduction in stool frequency was observed specifically for the subgroup receiving S. boulardii (SMD = −1.08, 95% CI: −1.45, −0.71) (Supplementary Fig. S11), particularly at higher doses (≥1010 CFU). In addition, MA involving at least 2000 participants indicated that probiotics could reduce stool frequency on day 5, while high-quality MA showed a significant decrease in stool frequency on day 6 as well. Subgroup analyses further supported the beneficial impact of probiotics on stool frequency ≥day 7 after treatment initiation (Table 2).
Duration of vomiting
The overall effect size for vomiting when comparing probiotics to placebo was −0.16 day (SMD = −0.16, 95% CI: −0.26, −0.07). Subgroup analyses based on the type of probiotics did not support this effect (Supplementary Fig. S15), although it was supported by MA involving ≥2000 participants, as well as by low-quality MA (Table 2).
Duration of fever
The overall analysis for vomiting found that probiotics significantly decreased the duration of fever (SMD = −0.20, 95% CI: −0.33, −0.07). Subgroup analyses based on the type of probiotics showed a positive effect only when multi-strain probiotics (SMD = −0.18, 95% CI: −.04, −0.33) were used (Supplementary Fig. S15). Subgroup analysis by sample size, dose, duration of treatment, and quality of MA supported this finding (Table 2).
Sensitivity analysis and publication bias
There was a significant publication bias observed for diarrhea on days 2 and 3 after treatment initiation, as well as for stool frequency on day 1 after treatment initiation (Fig. 5). In contrast, other outcomes did not show any evidence of publication bias. In the sensitivity analysis, the pooled effect size for the incidence of AG was influenced by the study conducted by Sun et al. 43 The presence of diarrhea on day 1 was impacted by Szajewska et al., 45 while the presence of diarrhea on day 6 was affected by Urbanska. 53 In addition, stool frequency on day 1 was influenced by McFarland et al., 40 which diminished the reliability of the associated findings. When we excluded the MAs with the highest overlap (≥50% overlap) with other included MAs, the results remain consistent, showing the reliability of the findings.
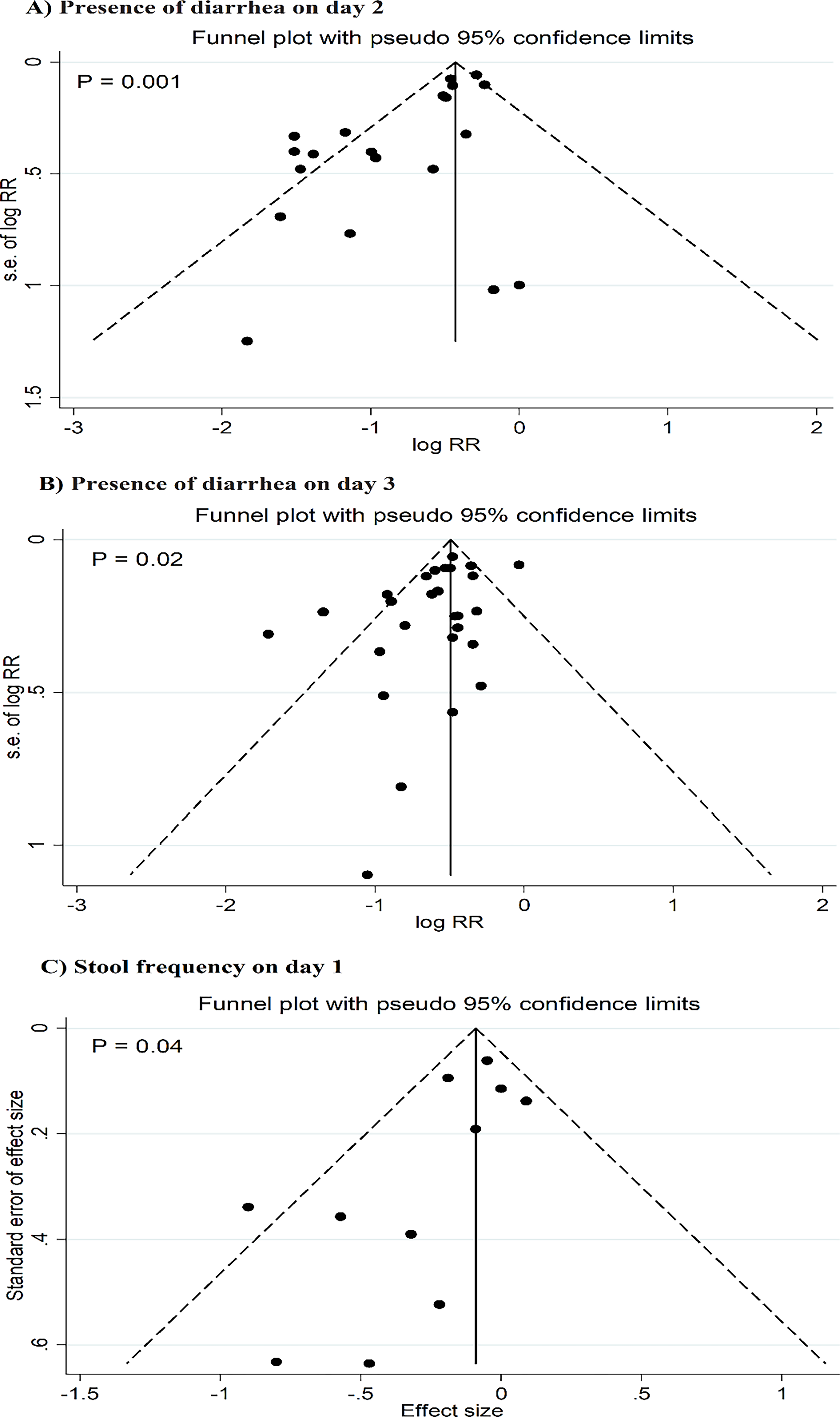
Publication bias for the presence of diarrhea on day 2
Meta-regression analysis
The effect of probiotics on the presence of diarrhea on day 4 was affected by sample size (B = −0.0001, SE = 0.0002, p = 0.01) and the dose of intervention (B = −0.004, SE = 0.0008, p = 0.001). For the presence of diarrhea on day ≥7, the pooled estimate was significantly affected by the duration of treatment (B = 0.02, SE = 0.005, p = 0.01) and the proportion of high-quality studies in each MA (B = 0.02, SE = 0.006, p = 0.02).
Safety and adverse effects
Generally, no adverse effects were reported in the probiotics and control groups.34,35,39,44,46,47,49,57 Urbanska et al. 53 reported that administration of Lactobacillus reuteri may result in a change in bowel habits, but Chmielewska et al. 59 showed that adverse effects associated with L. reuteri were not reported in any of the RCTs. Ianiro et al. 36 reported that vomiting was the most commonly reported adverse event after supplementation with B. clausii; however, no statistically significant difference in the number of patients experiencing adverse events was observed between the probiotic and placebo groups. In the MA by Schnadower et al., 16 some adverse events such as abdominal cramps, intestinal rumbling, nausea, weakness, bloating, constipation, loss of appetite, headache, and fever were reported in both the LGG and placebo groups, but no significant differences were observed between the trial groups in the rates of adverse events.
Discussion
This umbrella MA, which included 36 MA encompassing 78 probiotic interventions, suggested that probiotics may decrease the duration of diarrhea, the number of diarrheal episodes, presence of diarrhea, vomiting, fever, and the length of hospital stays in children. However, the effects were found to be strain-specific and, for certain outcomes, were influenced by the dose and duration of treatment. Moreover, there was weak evidence in subgroup analysis indicating that probiotics may help prevent the incidence of AG when LGG is prescribed at higher doses.
Several probiotics have been evaluated for their efficacy for preventing and treating AG, but have yielded inconsistent results. In this study, a higher dose of probiotics was effective in reducing the risk of diarrhea on day 4 and for diarrhea lasting ≥7 days when administered for a short duration of <6 days. Conversely, lower doses of probiotics were found to be more effective in decreasing stool frequency on days 1, 3, and 4. In addition, an intervention duration of less than <6 days was beneficial for reducing stool frequency on day 1, while longer intervention periods did not yield effective results. These findings suggest that both the dosage and duration of probiotic treatment play crucial roles in their effectiveness, indicating that tailored approaches may be necessary to optimize outcomes in different contexts.
For the duration of diarrhea, strains such as B. lactis and L. reuteri demonstrated the highest efficacy in reducing diarrhea duration, while multi-strain probiotics, S. boulardii, LGG, Lactobacillus spp, and B. clausii also showed positive effects. In terms of hospitalization duration, LGG was particularly effective, while multi-strain probiotics, S. boulardii, LGG, L. reuteri, and B. clausii also showed positive effects. Regarding the presence of diarrhea and the frequency of stools, generally, S. boulardii was the most beneficial intervention, indicating consistent positive effects through day 1 to ≥7 post-treatment. However, other strains such as LGG, L. reuteri, a combination of L. acidophilus spp.+ Bifidobacterium spp., L. acidophilus, and multi-strain probiotics also displayed positive impacts on specific days after the treatment. The strain-specific effects on AG symptoms are evident, with S. boulardii demonstrating superior efficacy over bacterial strains. This superiority likely arises from its yeast cell wall rich in β-1,3-glucans and mannoproteins, conferring exceptional gastric acid and bile tolerance compared to bacterial peptidoglycan walls, enabling direct binding to bacterial toxins (e.g., E. coli LT/ST) and competitive exclusion of pathogens in the inflamed gut.65–67 S. boulardii also exhibits distinct phenotypic and physiological attributes that drive its probiotic efficacy, including optimal growth at body temperature, gastric acid resistance, and viability in low-pH conditions. 68 L. reuteri was effective in reducing the risk of diarrhea up to 3 days after the initiation of the intervention, but not after a longer duration of follow-up. Overall, these findings highlight the importance of strain selection and dosage in utilizing probiotics for managing AG symptoms in children, emphasizing that specific strains can have varying degrees of effectiveness in alleviating symptoms and shortening recovery time.
Given the strain-specific effects observed, health care providers can tailor probiotic use based on specific strains known to be effective for particular outcomes, enhancing treatment efficacy. Overall, the most effective probiotics in terms of efficacy on AG symptoms were S. boulardii, LGG, L. reuteri, L. acidophilus, B. clausii, B. lactis, and a combination of L. acidophilus spp.+ Bifidobacterium spp, which is consistent with existing evidence.29,44,45,62
A MA found that B. clausii effectively reduced diarrhea, stool frequency, and hospital stay duration. 62 Another MA by Cheng et al. 29 showed that L. acidophilus shortened diarrhea duration, although this effect was not statistically significant when used as a single strain. However, it was effective when administered at doses ≥0.01 × 1010 CFU daily, notably reducing diarrhea frequency between days 2 and 5, with significance on day 3. Szajewska et al. 44 reported that Lactobacillus rhamnosus GG did not affect stool volume compared to placebo but was associated with decreased hospitalization length and diarrhea duration at doses ≥1010 CFU. Moreover, S. boulardii reduced diarrhea duration, hospitalization time, and the risk of diarrhea from days 2 to 7. 45 These findings support the results of the current umbrella MA.
Both single-strain and multi-strain probiotics have demonstrated efficacy in reducing the duration of AG, but the choice depends on the clinical scenario. Our MA showed that specific single strains such as S. boulardii and Lactobacillus GG have strong evidence of benefit, particularly for bacterial and viral AG. Multi-strain probiotics also significantly reduce diarrhea duration and may offer a broader spectrum of activity, which could be advantageous in viral or mixed infections. Dose and treatment duration are critical, with higher doses (≥1010 CFU) showing greater efficacy in both viral and bacterial AG. The superior efficacy observed at higher doses likely reflects a functional persistence threshold rather than permanent colonization. Preclinical studies and select human trials demonstrate dose-dependent fecal recovery and mucosal interaction, often in the range of 109–1010 CFU, which may be required to overcome gastrointestinal transit and dilution effects. 69 At these doses, probiotic exposure is sufficient to engage innate immune signaling pathways, including Toll-like receptor 2 (TLR2/MyD88)-mediated responses and anti-inflammatory cytokine production (e.g., IL-1070,71 Higher CFU levels may also enhance pathogen suppression through increased antimicrobial metabolite production and competitive niche exclusion, with several clinical trials reporting improved outcomes in AG.72,73 However, these effects are strain-specific and may exhibit dose plateaus rather than linear responses. Therefore, clinicians might prefer single strains with proven strain-specific benefits for targeted infections and consider multi-strain formulations for broader coverage, especially when the etiology is uncertain. Patient factors, availability, and safety profiles should also guide the decision. This evidence supports the integration of probiotics into clinical practice as a complementary approach alongside standard treatments like rehydration therapy, particularly for children at risk of severe dehydration and prolonged illness. However, clinicians should remain mindful of the variations in dose and duration that influence these outcomes, ensuring that probiotic administration is optimized for individual patient needs.
New insights of our study include dose-dependent effects and strain-specific impacts varying by viral or bacterial etiology. For example, S. boulardii was effective against bacterial AG and AG of unknown cause but not parasitic AG. These results support targeted probiotic use, aligning with previous findings while clarifying strain- and dose-specific responses that guide clinical application. This study further clarifies probiotic effects by subgroup analyses on symptom severity and health care settings, revealing distinct strain benefits in inpatient versus outpatient contexts. Such a nuanced evaluation extends prior research by linking probiotic effects to clinical variables, thus advancing practical understanding and optimizing therapeutic strategies in AG treatment. Overall, probiotics had no significant adverse effect compared to placebo, showing its safety in clinical practice. Altered bowel habits after L. reuteri use are typically transient and linked to microbiota shifts, such as enhanced short-chain fatty acid (SCFA) production. 74 However, in immunocompromised cases, rare bacteremia/fungemia risks (<0.01%) exist with S. boulardii, particularly in ICU settings with catheters.75,76
Mechanistically, probiotics suggest several pathways, including competitive exclusion of pathogens, enhancement of gut barrier function, modulation of immune responses, and restoration of healthy gut microbiota, through which these interventions exert their beneficial effects on children with AG. 77 Probiotics enhance gut health by adhering to the intestinal mucosa, which helps create a protective barrier against pathogenic bacteria through competitive exclusion. 78 This adherence also stimulates the growth of beneficial commensal bacteria while inhibiting the proliferation of harmful pathogens, thereby reducing inflammation and promoting a favorable gut environment. 79 Furthermore, probiotics modulate the immune response by interacting with intestinal epithelial cells and immune cells, leading to the production of immunoglobulin A (IgA) and various cytokines that bolster mucosal immunity, which helps control infections. 80 S. boulardii has been shown to decrease inflammation in the gut by producing a low-molecular-weight soluble factor that inhibits Nuclear factor kappa B (NF-κB) activation and ERK1/2 MAP kinase signaling. This leads to decreased expression of the interleukin-8 (IL-8) and tumor necrosis factor alpha (TNF-α) genes, along with increased levels of anti-inflammatory cytokines such as IL-10 and an elevated IL-10/IL-12 ratio in intestinal epithelial cells and monocytes, resulting in reduced secretion of proinflammatory cytokines, thereby helping to reduce inflammation in conditions like AG. 81 S. boulardii has been also demonstrated to attach to invading pathogens such as E. coli and Salmonella typhimurium through lectin receptors on its cell wall, which prevents these microbes from adhering to the intestinal brush border. This action helps trap the pathogens and facilitates their removal from the body during bowel movements. 82 The synthesis of antimicrobial compounds, such as bacteriocins, cathelicidins, defensins, and SCFAs, further contributes to pathogen inhibition and promotes gut integrity. 83 L. acidophilus produces lactic acid and other metabolites that inhibit pathogen growth, thereby reducing diarrhea incidence. 84 LGG enhances the intestinal barrier by reinforcing tight junctions between epithelial cells and increasing the production of intestinal mucins. It also protects against damage triggered by lipopolysaccharide (LPS) or TNF-α, counteracting the reduction of essential barrier proteins such as mucin 2 (MUC2) and zonula occludens-1 (ZO-1), thereby maintaining the overall integrity of the intestinal lining. 85 LGG and B. lactis modulate immune responses by reducing the production of inflammatory cytokines such as TNF-α.86,87 L. reuteri also enhances local immune responses and may reduce the severity and duration of diarrhea episodes by modulation of TLR4 and NF-κB signaling in the intestine. 88 The combination of L. acidophilus spp. + Bifidobacterium spp. leverages the strengths of both strains, enhancing overall efficacy in restoring gut microbiota balance and improving immune responses against pathogens. 89 As a spore-forming probiotic, B. clausii can survive harsh gastrointestinal conditions, allowing it to effectively colonize the gut and exert its beneficial effects. 90 It helps restore the balance of gut microbiota disrupted by infections or antibiotics, thus aiding recovery from diarrhea. 91 These mechanisms highlight the potential of probiotics not only to prevent AG but also to alleviate its associated symptoms effectively.
Although several outcomes reached statistical significance, statistical significance does not necessarily imply clinical relevance. Some of the observed effect sizes, particularly for outcomes such as duration of vomiting and fever, were relatively small and may translate into modest absolute reductions in symptom duration. Therefore, the clinical importance of these findings should be interpreted with caution. In contrast, reductions in the duration of diarrhea and length of hospitalization may have greater practical implications, especially in moderate to severe cases or in resource-limited settings. In addition, this umbrella MA did not formally assess cost-effectiveness. While probiotics appear to confer clinical benefits in specific contexts, their economic value should be evaluated in future studies that incorporate cost analyses alongside clinical outcomes. Consequently, treatment decisions should consider not only statistical significance but also clinical magnitude of effect, patient characteristics, disease severity, and health care costs.
This study is the first umbrella MA to investigate the effects of probiotics on AG in children. A significant strength of this analysis is its comprehensive subgroup analysis based on the type of probiotics, as well as the dosage and duration of treatments, which aids in identifying sources of heterogeneity. In addition, meta-regression analysis was performed to further explore these sources of heterogeneity, and the reliability of the findings was evaluated through sensitivity analyses. The large sample size of 107,541 participants provided ample statistical power to detect effects. However, some limitations should be considered when interpreting these results. Significant heterogeneity was observed in certain outcomes across the MA, with meta-regression and stratified analyses indicating that differences in treatment dosage, probiotic types, treatment duration, study quality, sample size, and the proportion of studies with low bias contributed to this heterogeneity. Moreover, we found that variations in the etiology and severity of AG contributed significantly to the observed heterogeneity for diarrhea duration. Regional differences in gut microbiota composition can also influence host responses and susceptibility, thereby contributing to observed heterogeneity across the studies. Consequently, we employed random-effects models in our MA to yield more reliable summary estimates. In addition, caution is warranted when interpreting pooled findings for specific outcomes, particularly those derived from subgroup analyses due to the limited number of MAs involved. Furthermore, significant publication bias was identified for diarrhea on days 2 and 3, as well as for stool frequency on day 1. The search strategy focused solely on English publications, which may have led to the omission of some relevant MAs. Publication bias in our study likely arises because studies with positive or significant results are more frequently published than those with negative or null outcomes. This selective publication can lead to an overestimation of treatment effects and may distort the overall conclusions drawn from the analysis. Thus, the findings should be interpreted with caution. As this field continues to evolve rapidly, future research could enhance understanding by integrating results based on intervention and outcome characteristics, potentially resolving some existing uncertainties. Lastly, the literature search was restricted to two electronic databases (PubMed and Scopus). Although these databases provide extensive coverage of biomedical and multidisciplinary peer-reviewed literature, the exclusion of other databases such as Embase, Web of Science, and the Cochrane Library may have resulted in the omission of some potentially eligible MAs.
Conclusion
This study indicates that probiotics have the potential to prevent AG and reduce associated symptoms in children. However, it is important to note that these effects are strain-specific and may vary based on the dosage and duration of treatment, highlighting the need for careful consideration in probiotic selection and administration.
Statement of Ethics
As this study was a review of published literature, no ethics approval by a Research Ethics Board was required to conduct our research.
Authors’ Contributions
S.F., X.M., and R.L.: Investigation. S.F., X.M., and R.L.: Methodology. X.M.: Resources. X.M. and R.L.: Data curation. R.L.: Software. S.F. and X.M.: Writing—original draft. R.L.: Writing—review and editing. R.L.: Supervision.
Statement of Artificial Intelligence (AI) Use
Generative AI tools were employed solely to improve the English language quality of the article, using the Perplexity platform (https://www.perplexity.ai) under strict human supervision and review to ensure accuracy and clarity.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
No sources of external funding were utilized for this project.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.