
Abstract
Background:
Acute sleep deprivation impairs cognitive, psychomotor, and mood outcomes, in part by reducing cerebral adenosine triphosphate (ATP) availability. Creatine supplementation may counter these effects by increasing phosphocreatine stores.
Methods:
Six databases were systematically searched (January 2006–May 2025) for studies investigating creatine’s effects on cognitive, psychomotor, and mood outcomes during acute sleep deprivation.
Results:
Results were synthesized narratively. Of 160 records, five studies met the inclusion criteria. Early investigations indicate a positive trend for creatine supplementation as an intervention for acute sleep deprivation, though effects may vary by cognitive domain.
Conclusion:
Despite favorable early results, research is sparse, and future high-quality trials are needed.
Introduction
Roughly one-third of Americans report insufficient sleep, which is linked to adverse health effects.1,2 Acute sleep deprivation (ASD), defined as less than 48 h of wakefulness, is associated with adverse psychological and cognitive effects (e.g., decreased vigilance and short-term memory, slower reaction times, and impaired sustained attention).3,4 Psychomotor performance may also be disrupted, but the effects are less clearly defined. 5 Considering the prevalence and adverse effects of ASD, identifying practical interventions is a growing priority.
Creatine, a potential intervention for ASD, is an endogenously produced compound that supports rapid ATP resynthesis through the phosphocreatine (PCr) system.6–8 During ASD, the PCr/inorganic phosphate ratio decreases, indicating reduced cerebral energy reserves. 6 By replenishing PCr stores, creatine may help maintain ATP availability and mitigate negative ASD-related effects.6,7 This report evaluates the existing literature on the role of creatine supplementation in cognitive, affective, and psychomotor domains during ASD.
Materials and Methods
This review was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines. A literature search was performed across PubMed, Scopus, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and PsycInfo using a combination of subject headings, Medical Subject Headings (MeSH) terms, and keyword phrases related to creatine and sleep deprivation. A detailed description of search strategies is provided in Supplementary Appendix A. Results were limited to publications from January 1, 2006, to May 30, 2025. Prior to 2006, no studies were conducted investigating creatine supplementation as an intervention for sleep deprivation. After duplicate removal, two independent reviewers (N.W., R.H.) screened titles, abstracts, and full texts for eligibility with disagreements resolved by consensus.
Inclusion criteria
Healthy human participants, ≥18 years Experimental studies involving ASD (≤48h) Studies that meet the predefined population, intervention, comparison, outcomes (PICO) (Table 1) Published in peer-reviewed journals
PICO Elements for Inclusion Criteria
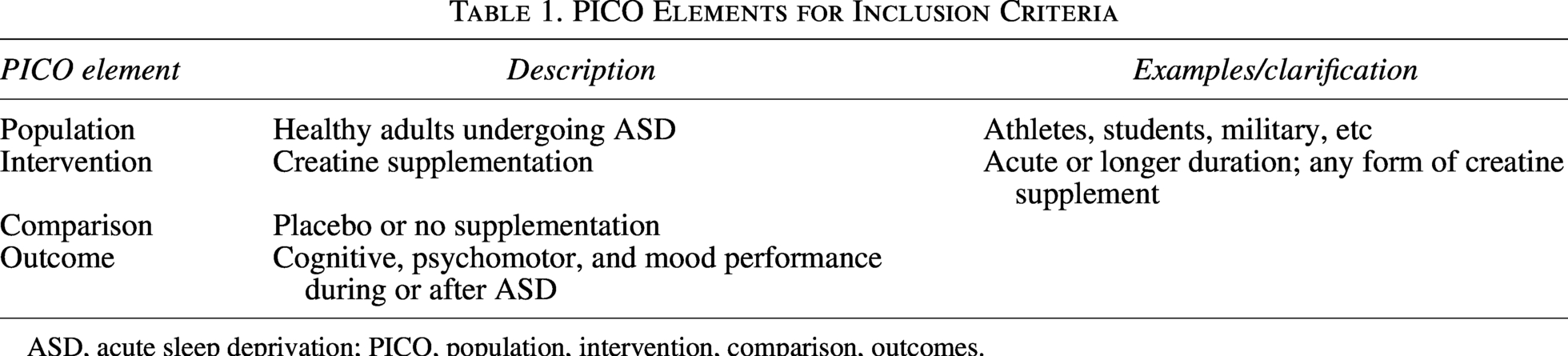
ASD, acute sleep deprivation; PICO, population, intervention, comparison, outcomes.
Exclusion criteria
Studies involving chronic sleep deprivation or insomnia Reviews or commentaries Studies not meeting the relevant PICO
The extracted data included study characteristics, creatine dosing regimen, cognitive, psychomotor, and mood outcomes. All results compatible within each domain were included. Effect direction, magnitude, and experimental conditions were recorded when available. Due to the small number of eligible studies and heterogeneity in study designs, a meta-analysis was not conducted. Findings were tabulated, and all included studies were considered as a single group for synthesis. Risk of bias was assessed using the Cochrane Risk of Bias 2.0 tool by two independent reviewers (N.W. and R.H.). Certainty of evidence and publication bias were not formally assessed (few studies; no pooling).
Results
The search generated 120 publications. After removing duplicates (n = 55), 66 articles remained; 61 were excluded based on title/abstract or full-text review. Five studies met all inclusion criteria and were retained for analysis. No eligible studies were excluded (Fig. 1).
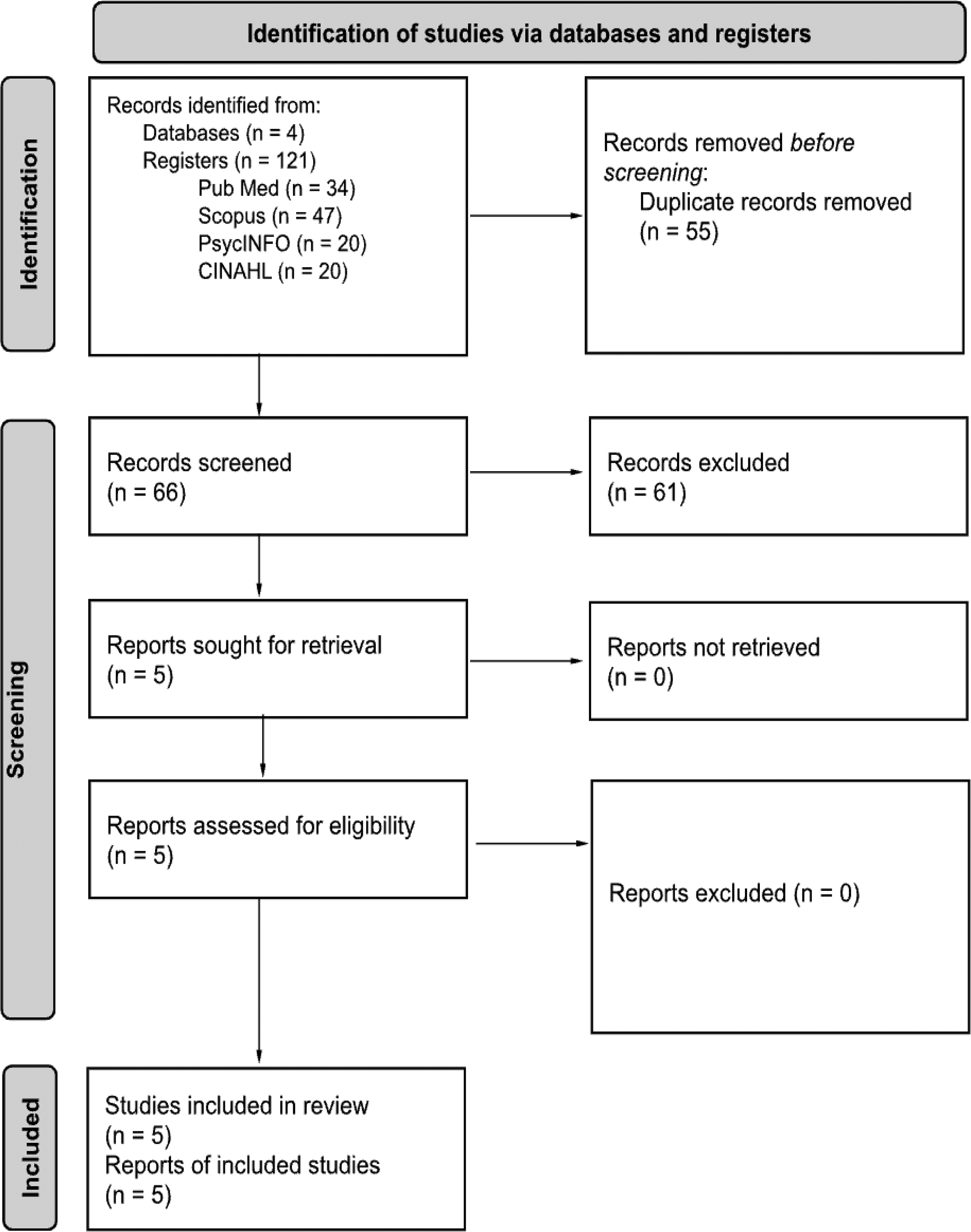
PRISMA flow diagram of the study selection through the systematic review process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The five studies varied in design, creatine dosing regimen, and sleep-deprivation paradigm, limiting direct comparability (Table 2). All populations consisted of healthy participants in their 20 sec undergoing total or partial ASD. Creatine monohydrate was administered either as a single acute dose or as a short loading regimen in each study. The outcomes are organized by functional domain to demonstrate the range of cognitive, psychomotor, and mood measures assessed across studies, as summarized below.
Characteristics and Outcomes of Studies Evaluating Creatine Supplementation During Acute Sleep Deprivation
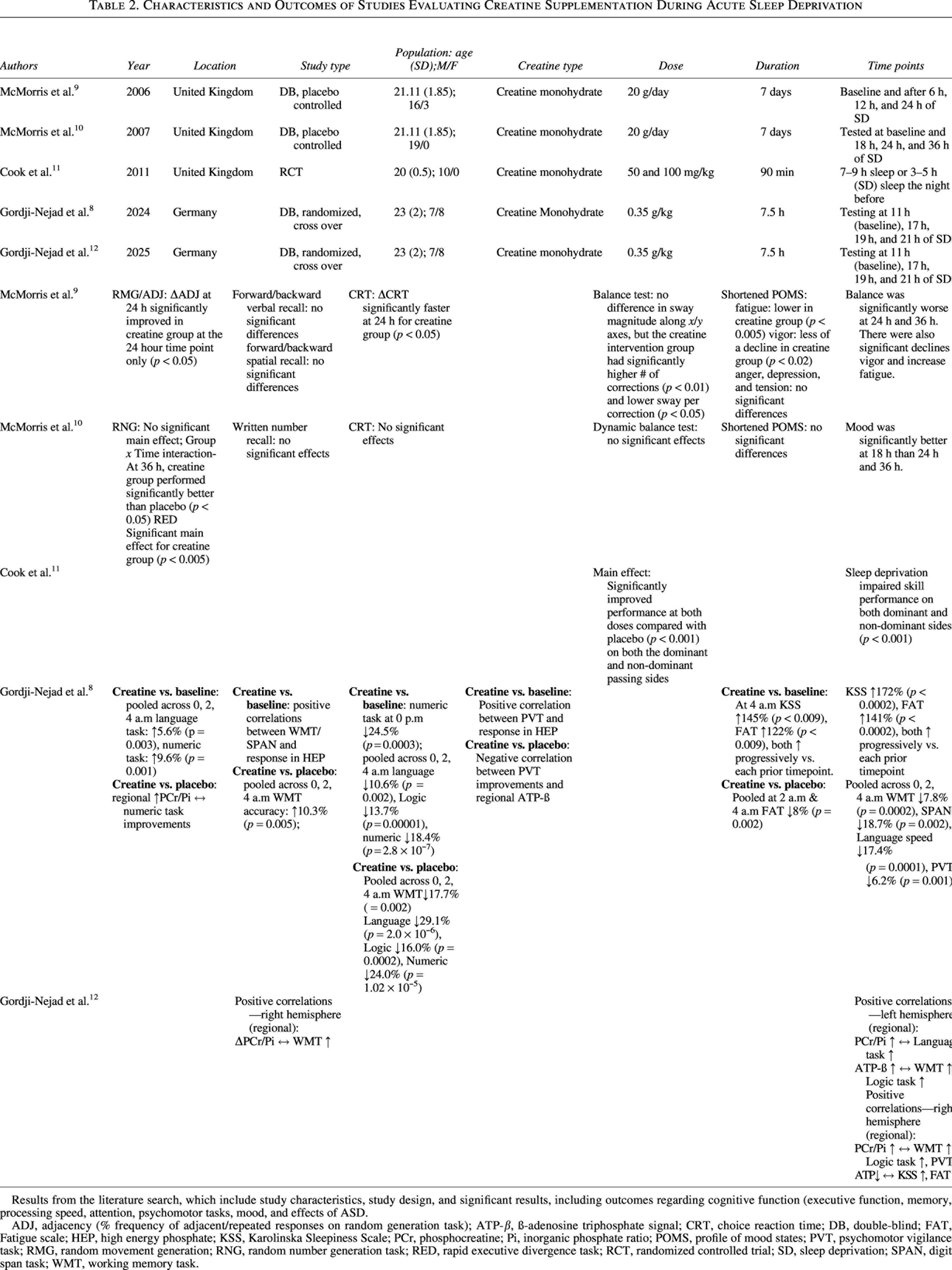
Results from the literature search, which include study characteristics, study design, and significant results, including outcomes regarding cognitive function (executive function, memory, processing speed, attention, psychomotor tasks, mood, and effects of ASD.
ADJ, adjacency (% frequency of adjacent/repeated responses on random generation task); ATP-β, ß-adenosine triphosphate signal; CRT, choice reaction time; DB, double-blind; FAT, Fatigue scale; HEP, high energy phosphate; KSS, Karolinska Sleepiness Scale; PCr, phosphocreatine; Pi, inorganic phosphate ratio; POMS, profile of mood states; PVT, psychomotor vigilance task; RMG, random movement generation; RNG, random number generation task; RED, rapid executive divergence task; RCT, randomized controlled trial; SD, sleep deprivation; SPAN, digit span task; WMT, working memory task.
The studies assessed creatine’s role regarding cognitive and psychomotor function, mood, and biochemical markers during ASD (Table 2).
Risk of bias results are tabulated in Supplementary Table S1 and Supplementary Figure S1.
Discussion
In this review, the effects of creatine supplementation are evaluated across cognitive, psychomotor, and mood domains under conditions of ASD. Creatine appeared to mitigate some of the adverse effects of ASD; however, evidence remains limited.
Effects of acute sleep deprivation
ASD has been linked with multiple adverse effects on cognition, psychomotor performance, and mood.3–5 Notably, among cognitive outcomes, the broader literature indicates that simpler tasks are more sensitive to the effects of sleep loss compared with complex tasks. 3 In the included studies, executive function and recall were preserved, yet other cognitive domains including memory, processing speed, and attention demonstrated declines.11,13,14 Psychomotor effects of ASD may also be task-specific. Previous work suggests that simple gross motor performance may be less affected, whereas performance decrements are more apparent for psychomotor tasks with higher cognitive demands. 9 In this review, Cook et al. found that rugby players’ passing accuracy declined during later repetitions of a repeated passing task (repetitions 10–20 versus 1–10), suggesting increasing mental fatigue. 11 Furthermore, consistent with previous literature, ASD resulted in worsened mood and increased perceived fatigue.4,11,13,14
The variability in impact of ASD on cognition and psychomotor function is likely due to the heterogeneity of the sleep deprivation period, task demands, circadian timing, and motor complexity; however, the negative trend combined with measured mood impairment supports the need for an effective intervention.
Effects of creatine supplementation
Metabolic response
Creatine supplementation increases brain PCr, but regional effects have not been thoroughly investigated.6–8 In this review, Gordji-Nejad et al. reported greater decreases in ATP in the right hemisphere compared with the left during ASD; yet, following creatine supplementation, there was significantly greater ATP consumption in the left hemisphere compared with the right.10,13 Greater creatine uptake was also observed in gray matter than white matter. 10 The authors suggest these high-energy demand regions may be particularly responsive to creatine supplementation.10,13 This observation may be supported by McMorris et al. who reported improved cognitive performance following creatine supplementation on tasks that had not declined during sleep deprivation. 11 Taken together, these results support the hypothesis that creatine increases the brain’s capacity to engage with metabolically demanding tasks during acute stress by enhancing local energy availability.
Cognitive function
Previous research on creatine’s cognitive benefits ranges from having no effect to moderate benefits. 8 Potential explanations for these discrepancies include dose-dependent effects of creatine, sensitivity to acute stress states, differences in metabolic task demands, and variation in participant age. In this review, multiple studies reported improvements in cognition during sleep-deprived conditions following creatine supplementation, such as increased accuracy in language and numeric tasks as well as RMG/ADJ as compared with placebo.13,14 Significant improvements were also seen in processing speed in CRT and number, logic, and language tasks both when compared with baseline and with placebo.11,13,14 Other areas of cognition such as memory and attention did not improve significantly or had mixed results.11,13,14 These task-specific effects may reflect that creatine is most beneficial when metabolic demand is high, such that tasks placing greater energy demand on the brain show larger performance benefits. Collectively, these findings suggest a favorable trend in creatine supplementation and that it may attenuate some of the negative consequences of ASD on cognition.
Psychomotor performance
Current research on creatine supplementation effects on psychomotor performance remains limited, largely confined to sport-specific contexts, and presents mixed findings. For instance, one study assessing soccer players reported improved dribbling but no change in kicking accuracy. 15 In our review, psychomotor benefits of creatine primarily emerged during ASD rather than under rested conditions. McMorris et al. reported improved static balance only at 24 h of sleep deprivation, not at 6 or 12 h, and found no effect on dynamic stability.11,14 Cook et al. found no effect on passing accuracy in rested rugby players; however, creatine supplementation preserved performance during ASD compared with placebo. 12 Overall, the available studies suggest that creatine might mitigate ASD-related decrements in psychomotor tasks, but the narrow range of tasks and small sample sizes limit the strength of these interpretations.
Mood
Prior work suggests that creatine can improve mood-related outcomes, including decreased fatigue and increased perceived energy, especially in individuals under stress.7,8 In the context of ASD, significantly blunted increases in fatigue and sleepiness were reported, along with elevated feelings of vigor.11,13,14 These findings support the broader literature on creatine’s mood-enhancing potential; however, further research is needed to confirm its efficacy.
Limitations
This review’s primary limitation is the small number of studies examining creatine supplementation during ASD. Although no study was judged to have high risk of bias, three of the five studies had some concerns related to randomization and deviations from intended interventions, which limits confidence in the findings. In addition, heterogeneity existed across studies in design, dosing, sleep-deprivation paradigms, and outcome measures, which precluded direct comparison and statistical analysis. Study populations were limited to healthy, young adults (primarily males), restricting generalizability and strength of conclusions. These limitations highlight the need to standardize dosing protocols and investigate other populations in future research.
Conclusion
Based on a small number of studies, creatine supplementation shows a possible benefit on cognition, psychomotor function, and mood during ASD. However, differences in study design and small sample sizes preclude firm conclusions. Given the prevalence of sleep deprivation, future trials in more diverse populations with standardized dosing protocols and real-world performance outcomes are needed to determine if creatine may serve as a low-risk, accessible intervention to support brain function during ASD.
Authors’ Contributions
N.W.: Conceptualization, methodology, database search, screening and study selection, data extraction, and writing. R.H.: Methodology, database search, screening and study selection, data extraction, and writing. M.C.: Supervision, methodology guidance, validation, writing—review and editing, and resources.
Availability of Data
All data analyzed during this study are included in this published article or are available from the corresponding author upon request.
Footnotes
Author Disclosure Statement
This review was not registered nor was a protocol prepared On behalf of all authors, the corresponding author states that there is no conflict of interest.
Funding Information
No funding was received to support the preparation of this article.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.