
Abstract
Objectives:
To assess the feasibility of conducting a randomized controlled trial and to explore preliminary effects of individualized homoeopathic medicines (IHMs) compared with placebo in patients with temporomandibular joint dysfunction (TMJD).
Trial Design:
A double-blind, randomized, parallel-arm, placebo-controlled pilot feasibility trial with equal allocation to IHMs or placebo.
Methods:
Adults with clinically and radiologically confirmed TMJD were randomized to receive IHMs or matched placebo for 3 months. Participants, investigators, outcome assessors, and statisticians were blinded to allocation. The primary clinical outcome was the Graded Chronic Pain Scale (GCPS), which was assessed monthly. Secondary outcomes included the Jaw Functional Limitation Scale-20 (JFLS-20), Patient Health Questionnaire-4 (PHQ-4), and qualitative assessment of pre–post cone beam computed tomography (CBCT) findings. Feasibility outcomes included recruitment, retention, adherence, blinding, and safety. Repeated-measures analysis of covariance was used for exploratory analysis.
Results:
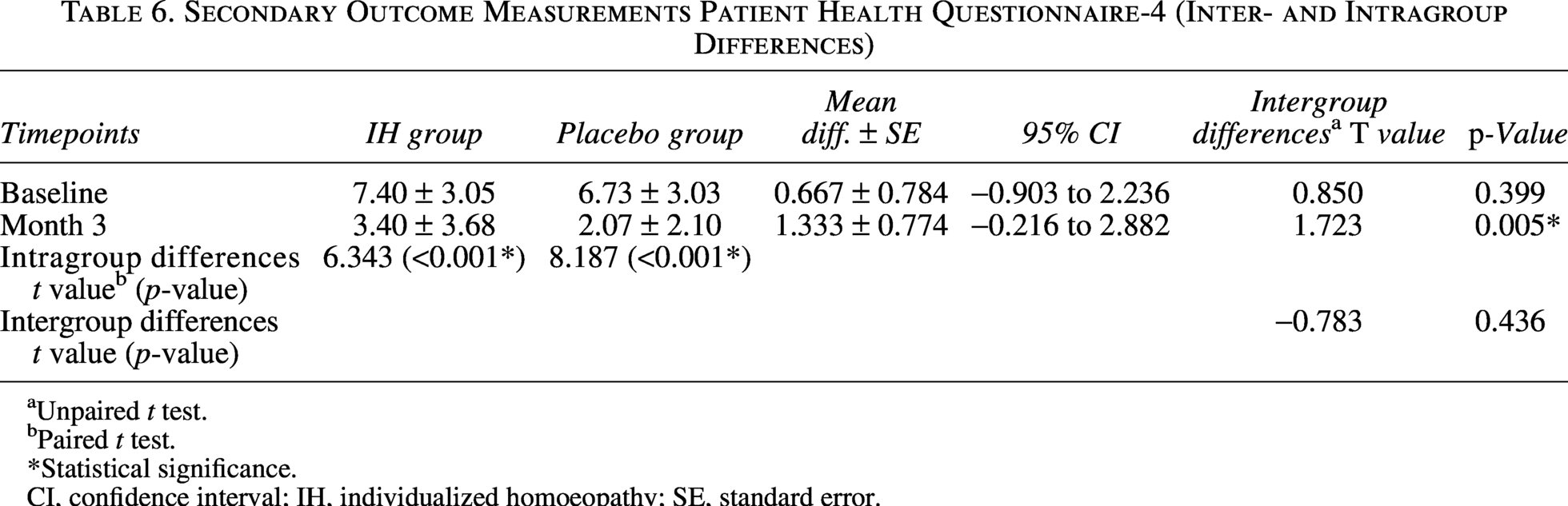
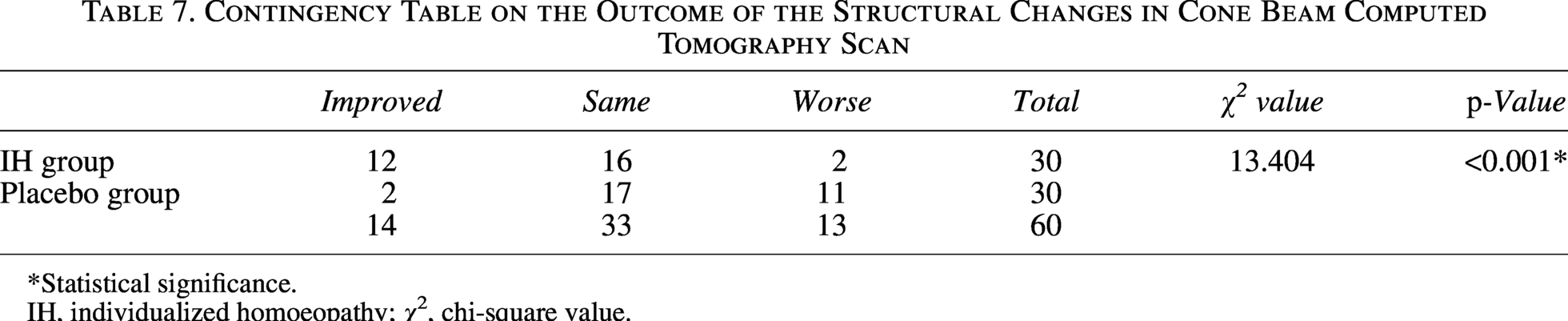
Sixty participants were randomized, with a retention rate of 91.7% and high intervention adherence (>80% in 91.7% of participants). No statistically significant intergroup difference was observed for overall GCPS scores (F = 2.151, p = 0.126). JFLS-20 scores showed a statistically significant group-by-time interaction (F = 3.642, p = 0.033). No significant differences were observed for PHQ-4 scores. Qualitative CBCT assessments demonstrated a statistically significant difference between groups (χ2 = 13.404, p = 0.001); these findings are exploratory and should be interpreted with caution.
Conclusion:
This pilot study demonstrates that the study is feasible; however, methodological challenges and potential confounding factors require careful consideration and additional safeguards before undertaking future definitive trials.
Trial Identifier:
Clinical Trials Registry of India, CTRI/2023/05/052919, registered on May 19, 2023.
Introduction
Temporomandibular joint dysfunction (TMJD) is a spectrum of orofacial disorders characterized by maxillofacial pain, most commonly from nondental causes. The condition is a broad term comprising of several complex conditions with symptoms of varying intensity. 1 The prevalence of the condition is ∼31% among adults and 11% among children. 2 The symptoms of the disease are experienced by almost 60%–70% of individuals, although only one-fourth of the cases are actually reported or treated. 3 It is the second most common cause of musculoskeletal pain following chronic back pain causing pain and disability. 4 The available treatment ranges from pharmacotherapy like nonsteroidal anti-inflammatory drugs and corticosteroids for pain management, psychological and multimodal therapy, physical therapy, acupuncture, dry needling, and substance injection within the intra-articular space. In severe cases, surgical procedures such as arthrocentesis, arthroscopy, and discectomy are also performed on the patients. 5 A major challenge in the treatment of the condition is the varied etiology associated with the disease, and the efficacy of any single therapy cannot be associated with the condition.
Homoeopathy, a prominent method of alternative medicine, has been successfully used in the treatment of a variety of musculoskeletal disorders. Considering the available literature in the form of materia medica and clinical experiences, the therapy shows a promising role in the treatment of the condition. Only a few previous studies have addressed the associated pain management, sleep disorders, and sleep bruxism through the use of specific homoeopathic remedies.6–8 Limited existing research does not provide insights into the role of homeopathic medicines in the management of TMJD. This study is the first of its kind—a double-blind, randomized controlled pilot feasibility trial—evaluating the role of individualized homeopathy in TMJD and exploring the feasibility of conducting a sufficiently powered definitive trial in the future.
Methods
Trial design
The study was conducted as a double-blind, randomized (1:1), parallel-arm, placebo-controlled pilot feasibility trial. The primary objective was to assess the feasibility of conducting a definitive randomized controlled trial of individualized homoeopathic medicines (IHMs) in patients with TMJD. The secondary objective was to explore preliminary trends in clinical outcomes. The focus of the study included recruitment, retention, adherence, acceptability, blinding, and safety rather than formal hypothesis testing for efficacy. The trial was conducted between February and December 2024 at the Clinical Research Outpatient Department of the Regional Research Institute for Homoeopathy, Siliguri, West Bengal, India, under the Central Council for Research in Homoeopathy, Ministry of AYUSH, Government of India.
Participants
Participants aged 18–75 years of either sex with clinically and radiologically confirmed TMJD were eligible. Clinical diagnosis was established by a consultant oro-maxillofacial surgeon using the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD). 4 Radiological confirmation was obtained using cone beam computed tomography (CBCT), and only cases confirmed by a radiologist were enrolled. Eligible participants were required to be free from serious systemic illnesses and capable of providing written informed consent. Exclusion criteria included uncontrolled metabolic disorders, severe psychiatric illness, malignancy, immunocompromised states, prior TMJ surgery, pregnancy, and lactation. Participants with habitual betel nut or tobacco chewing were not excluded in order to reflect real-world feasibility; however, this was prospectively recognized as a potential confounding factor and is addressed in the limitations.
Interventions
Experimental arm
Participants allocated to the experimental arm received IHMs prescribed according to classical homoeopathic principles following a comprehensive assessment of physical, mental, general, and system-specific symptoms. Remedy selection was performed using a consensus approach by two qualified homoeopathic physicians holding postgraduate degrees (MD [Homoeopathy]) and registered with the State Council, to ensure appropriate selection of the indicated similimum.
Each dose consisted of five to six cane sugar globules (size no. 30) medicated with the indicated homoeopathic preparation (dilution). All medicines were procured from a Good Manufacturing Practice–certified manufacturer and prepared in accordance with the Homoeopathic Pharmacopoeia of India. Doses were administered orally on an empty stomach in a clean mouth. Participants were advised to avoid handling the globules with bare hands and to refrain from eating, drinking, or smoking for at least 30 min before and after administration.
Participants were reviewed every 15 days over a 3-month period. Potency selection and repetition schedules were individualized. Modification of the prescribed remedy was permitted during follow-up based on evolving symptomatology. In cases of sustained clinical improvement, the same remedy was repeated at the end of the second month using the same dose and repetition schedule as at baseline
Control group
Participants allocated to the control arm received a placebo intervention identical in appearance, taste, size, and method of administration to the experimental treatment. The placebo consisted of unmedicated cane sugar globules (size no. 30) prepared using the same dispensing procedures as the active intervention, without impregnation with any homoeopathic medicine. The globules were moistened like homoeopathic medicines with 90% v/v ethanol to mimic the taste and smell of medicines.
Placebo globules were sourced and dispensed by the study pharmacy using standardized procedures to ensure blinding. Administration instructions were identical to those provided to the experimental group, including oral intake on an empty stomach in a clean mouth and avoidance of eating, drinking, smoking, or handling the globules with bare hands for at least 30 min before and after dosing.
Participants in the control arm were reviewed every 15 days for 3 months, following the same follow-up schedule as the experimental group. At each visit, symptom assessment and documentation were performed in an identical manner to maintain procedural consistency. No active homoeopathic remedies were administered at any point during the study period. Rescue medication, when required, was permitted according to the predefined protocol and recorded for both groups.
Concomitant care
All participants in both the experimental and control arms received standardized concomitant care throughout the study period to ensure ethical management and to minimize confounding. This included general advice on jaw rest, avoidance of excessive mouth opening, and limitation of parafunctional habits such as clenching or chewing hard substances. Participants were also counseled regarding oral hygiene and lifestyle modifications relevant to temporomandibular joint health.
Rescue medication in the form of nonsteroidal anti-inflammatory drugs was permitted for acute pain relief when required and was provided under the guidance of the consultant surgeon. The use, frequency, and duration of rescue medication were documented at each follow-up visit. No other concurrent therapies for TMJD, including physiotherapy, occlusal splints, or additional pharmacological treatments, were permitted during the study period.
Participants were instructed to continue their routine medical care for unrelated conditions but were advised not to initiate any new interventions specifically targeting temporomandibular joint symptoms during the trial.
Outcomes
The primary clinical outcome was the Graded Chronic Pain Scale (GCPS),9,10 a validated multidimensional instrument assessing pain intensity and pain-related disability in chronic pain conditions, including TMJD. The GCPS employs a standardized five-grade classification system (Grades 0–4), ranging from no pain to high-intensity, high-disability pain, allowing clear clinical benchmarking and interpretability. The scale demonstrates good internal consistency, construct validity, sensitivity to change, and versatility across different chronic pain conditions.11–13 GCPS assessments were conducted at baseline and at monthly intervals for 3 months.
Secondary clinical outcomes included the Jaw Functional Limitation Scale-20 (JFLS-20), 14 a condition-specific patient-reported outcome measure with established reliability and validity for assessing functional limitations related to mastication, jaw mobility, and verbal/emotional expression in TMJD. 15 Its domain-based structure supports clinically meaningful interpretation and longitudinal assessment of jaw function; JFLS-20 was assessed monthly during follow-up.
Psychological distress was evaluated using the Patient Health Questionnaire-4 (PHQ-4), 16 an ultra-brief screening tool for anxiety and depression with demonstrated internal consistency and convergent validity across medical populations 17 ; PHQ-4 assessments were performed at baseline and at the end of the third month.
Structural changes in the temporomandibular joint were explored using qualitative pre–post CBCT assessments, categorized as improved, unchanged, or worsened by a blinded assessor. CBCT is a low-dose imaging modality with high diagnostic sensitivity for osseous changes of the TMJ, particularly degenerative alterations such as condylar erosion, osteophyte formation, subchondral sclerosis, and flattening. CBCT is considered superior to conventional radiography and more sensitive than MRI for assessing cortical bone integrity, whereas Magnetic Resonance Imaging (MRI) remains the preferred modality for soft tissue evaluation.18–20 These imaging outcomes were considered exploratory and were interpreted with caution in the context of this pilot feasibility trial.
Feasibility outcomes, in accordance with CONSORT recommendations for pilot and feasibility trials 21 , included screening and recruitment rates, consent rate, retention, adherence to the intervention, success of blinding, and safety and were used to inform the design of a future definitive randomized controlled trial rather than to test hypotheses of efficacy.
Sample size
This study was designed as a pilot randomized controlled trial, and therefore, the sample size was not determined by formal power calculations for efficacy outcomes. Instead, a pragmatic sample size was chosen to permit preliminary assessment of recruitment feasibility, retention, protocol adherence, blinding procedures, and variability of outcome measures to inform the design of a future definitive trial. 22 A total of 60 participants were planned for enrollment, with 30 participants allocated to the experimental group and 30 to the control group. This allocation was considered feasible within the recruitment time frame and available resources and adequate for estimating key parameters relevant to pilot testing. No inferential claims regarding clinical effectiveness were intended based on this sample.
Randomization sequence generation
The random allocation sequence was generated using PASS 2024 statistical software. A permuted block randomization method was employed to ensure balanced group allocation throughout the enrollment period. Blocks of fixed size were used, with an equal allocation ratio maintained within each block, resulting in a 1:1 allocation of participants to the individualized homoeopathy (IHM) and placebo groups.
Allocation concealment
Allocation concealment was ensured using a pharmacy-controlled method. The randomization sequence was prepared in advance and sealed in sequentially numbered, triple-layered opaque envelopes, which were provided to the study pharmacist. Following participant enrollment and clinical consultation, investigators prescribed treatment without knowledge of group allocation. The pharmacist opened the corresponding envelope based on the participant’s enrollment number in the presence of an independent physician not otherwise involved in the trial and dispensed either the prescribed IHM or the placebo accordingly. The participant’s name, enrollment number, and date of envelope opening were recorded on the allocation slip. Opened envelopes and the dispensing register were signed and stored securely in a locked cabinet under the custody of the independent physician.
A double-blind design was adopted. Participants, investigators, outcome assessors, consultants, data entry personnel, and the statistical analyst remained blinded to treatment allocation throughout the study. At the end of the trial, the success of blinding was explored by asking participants and investigators to guess the allocated intervention based on perceived clinical response.
Statistical methods
Statistical analyses were performed primarily for descriptive and exploratory purposes, consistent with the objectives of a pilot randomized controlled trial. No formal hypothesis testing for clinical efficacy was prespecified. Baseline characteristics were summarized using descriptive statistics. Continuous outcomes are presented as means with standard deviations (SDs) or standard errors (SEs), and categorical variables as frequencies and percentages.
Changes in outcome measures over time were explored using repeated-measures analysis of variance or analysis of covariance (ANCOVA), with baseline values entered as covariates where appropriate, to examine patterns of change and estimate variability rather than to confirm treatment effects. Overall model effects were interpreted cautiously. Post hoc between-group comparisons were not interpreted in the absence of a statistically significant overall effect, and any exploratory comparisons are reported without inferential claims.
Effect estimates are presented with 95% confidence intervals (CIs) to aid interpretation of the magnitude and direction of observed differences. All p-values, where reported, were rounded to three decimal places and interpreted descriptively. The nominal level of statistical significance was set at α = 0.05.
Qualitative CBCT outcomes were summarized descriptively and compared between groups using contingency tables without inferential claims. Feasibility outcomes, including recruitment, retention, adherence, and blinding success, were analyzed descriptively. All analyses were conducted using standard statistical software.
Reporting guidelines
The study was reported in accordance with the CONSORT extension for randomized pilot and feasibility trials 23 and the Reporting Data on Homoeopathic Treatments (RedHot) guidelines, 21 which supplement the CONSORT statement. Adherence to reporting standards was ensured using the CONSORT pilot trial checklist.
Results
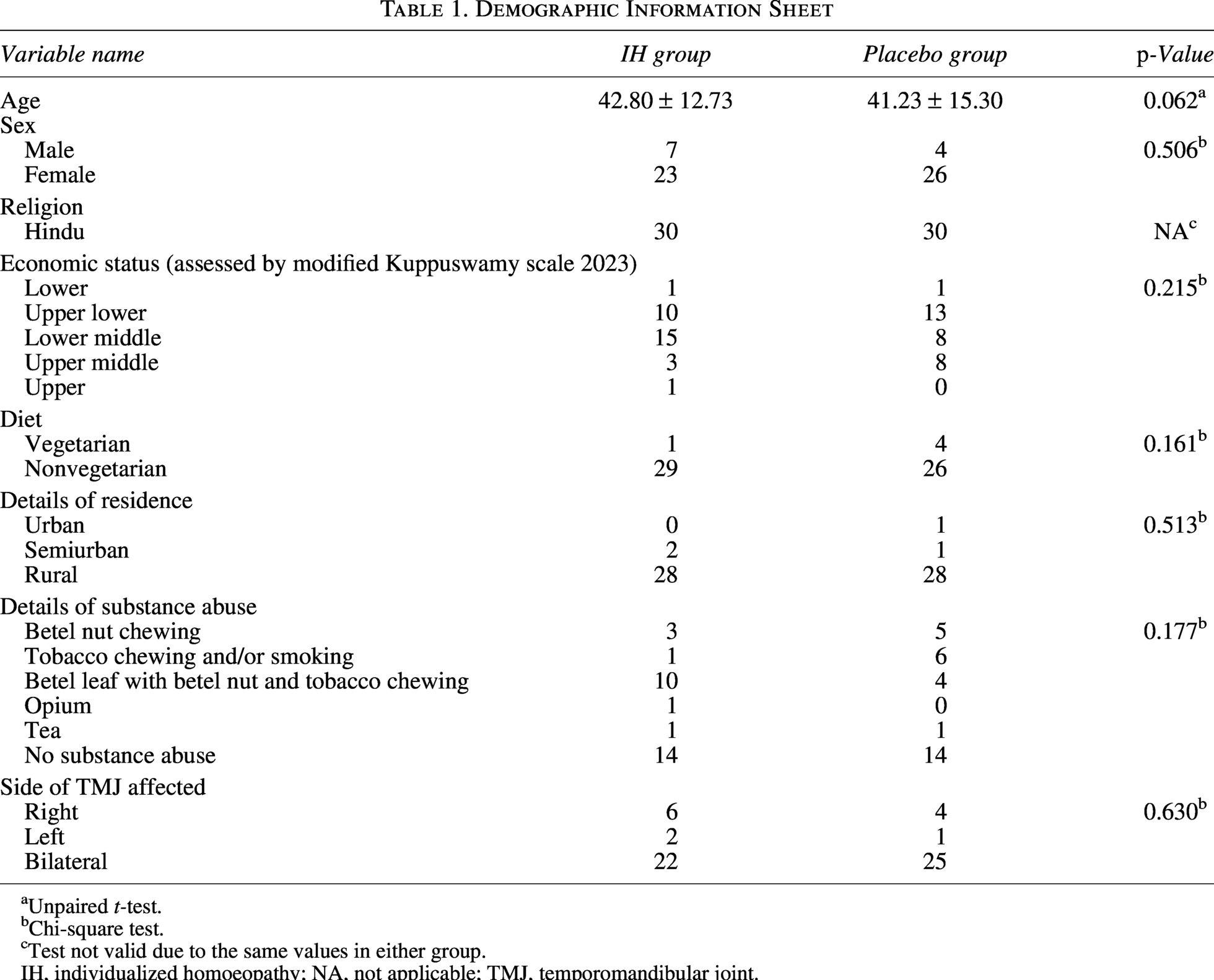
Participant enrollment was conducted between February 2024 and September 2024, and follow-up of the final enrolled participant was completed in December 2024. A total of 166 patients were screened at the General Outpatient Department of the Institute, of whom 106 were excluded based on predefined eligibility criteria. Sixty participants were enrolled and randomized to the experimental and control arms. During the study period, five participants were lost to follow-up. The flow of participants through the trial is presented in Figure 1. Baseline sociodemographic and clinical characteristics were comparable between the two groups (Table 1).
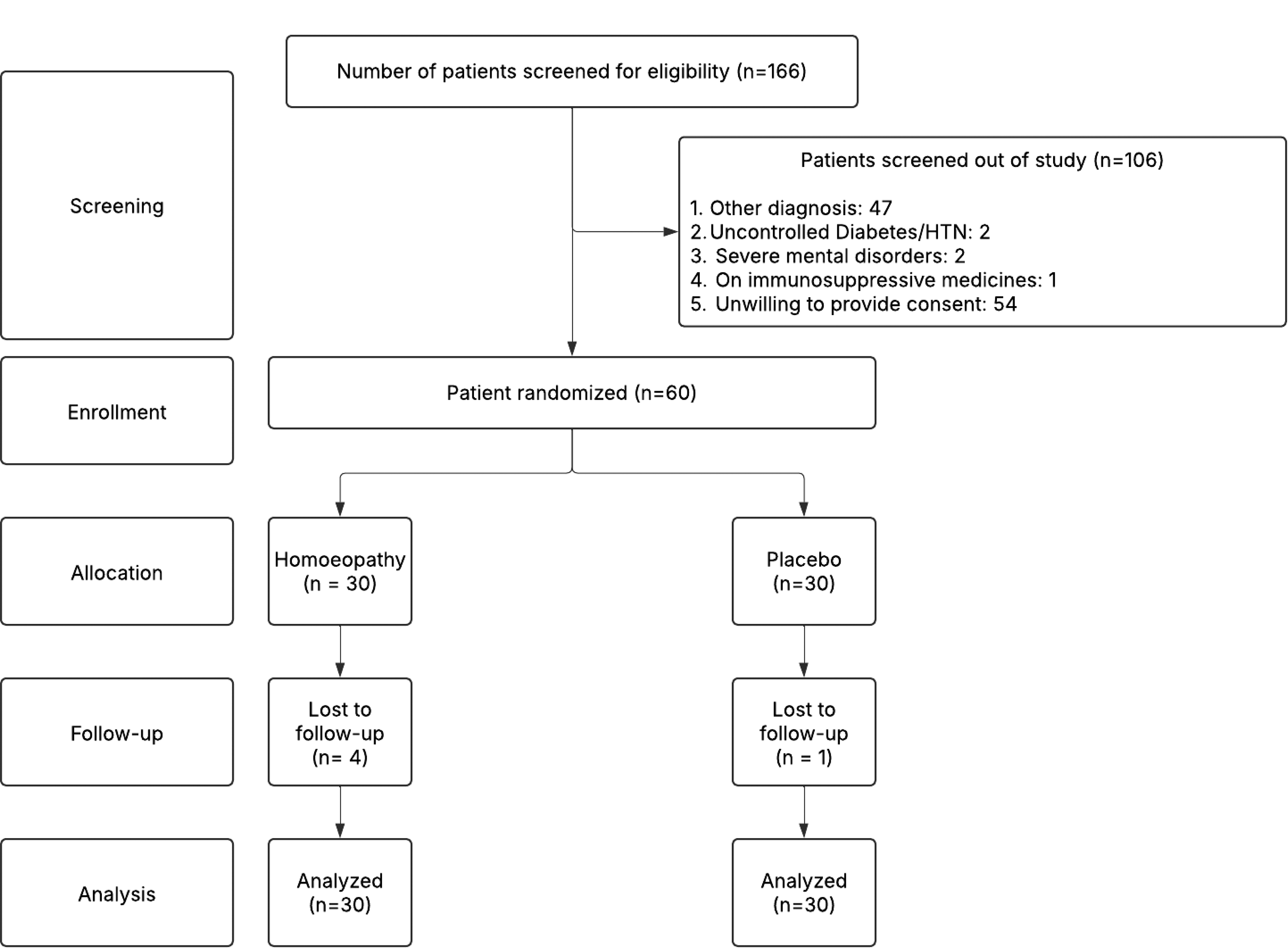
Study flow diagram. HTN (hypertension).
Demographic Information Sheet
Unpaired t-test.
Chi-square test.
Test not valid due to the same values in either group.
IH, individualized homoeopathy; NA, not applicable; TMJ, temporomandibular joint.
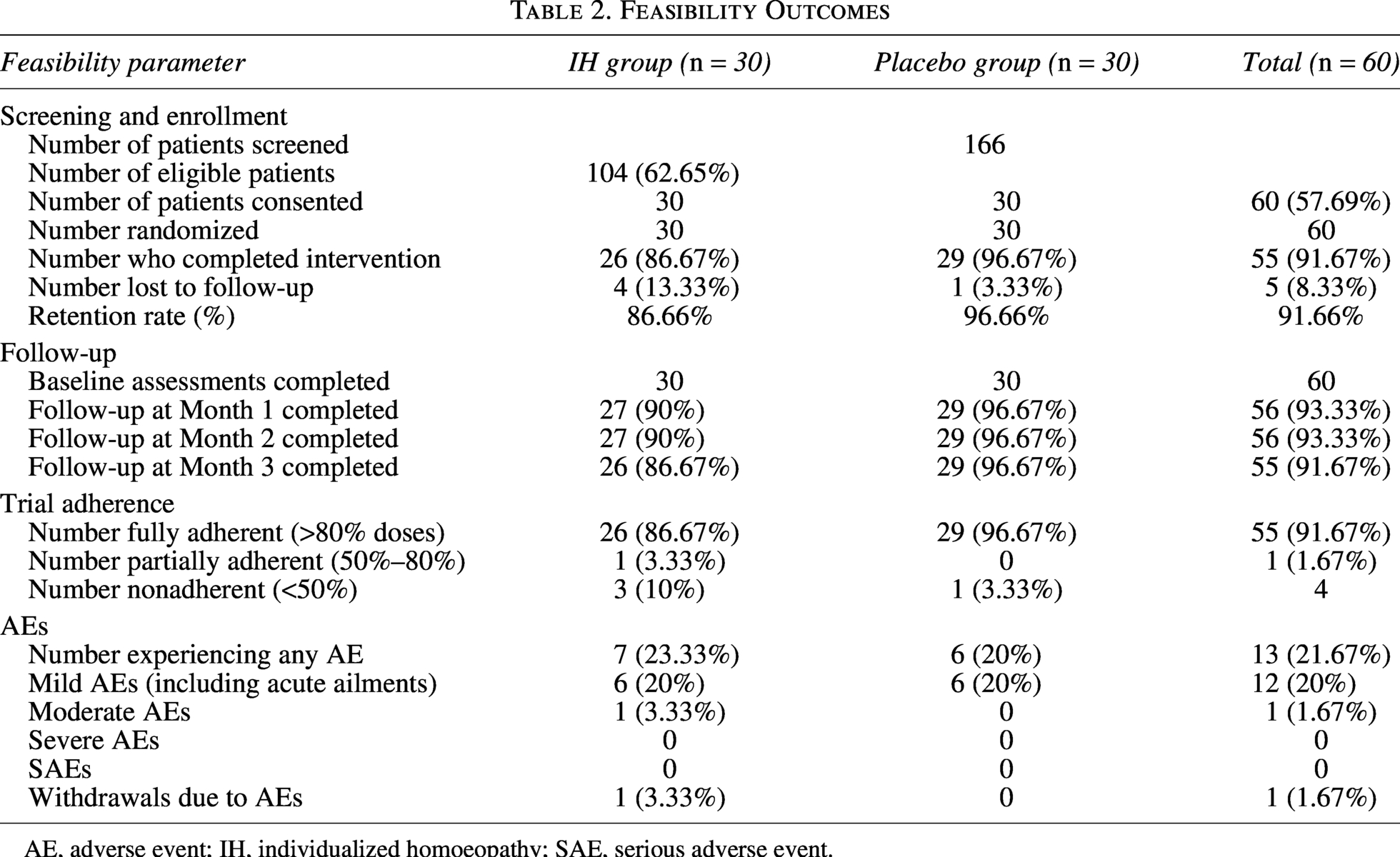
Feasibility outcomes
A total of 166 participants were screened, of whom 104 met the eligibility criteria, and 60 consented to participate and were randomized, yielding a recruitment rate of 57.69% among eligible individuals and an average recruitment rate of ∼10 participants per month (Table 2). While recruitment was achievable within the planned time frame, cultural practices prevalent in the study population, particularly betel nut and tobacco chewing, posed challenges to sustained behavioral adherence.
Feasibility Outcomes
AE, adverse event; IH, individualized homoeopathy; SAE, serious adverse event.
Of the 60 randomized participants, an overall retention rate of 91.67% was achieved, with retention rates of 86.67% in the IHM group and 96.67% in the placebo group. Although follow-up completion was high, adherence to lifestyle recommendations was moderate to poor in a subset of participants, with several resuming betel nut or tobacco chewing once symptom severity decreased. Adherence to the allocated intervention itself was high, with 91.67% of participants consuming more than 80% of the prescribed doses.
Adverse events were reported by 21.67% of participants during the study period and were predominantly mild and self-limiting, consisting mainly of acute ailments such as common cold, diarrhea, and upper respiratory symptoms. No serious adverse events were observed. Overall, the feasibility outcomes highlight that while recruitment, retention, and medication adherence were acceptable, behavioral factors and expectation-related biases represent important feasibility constraints that must be addressed in future definitive trials through stricter eligibility criteria, enhanced behavioral monitoring, and reinforced adherence strategies.
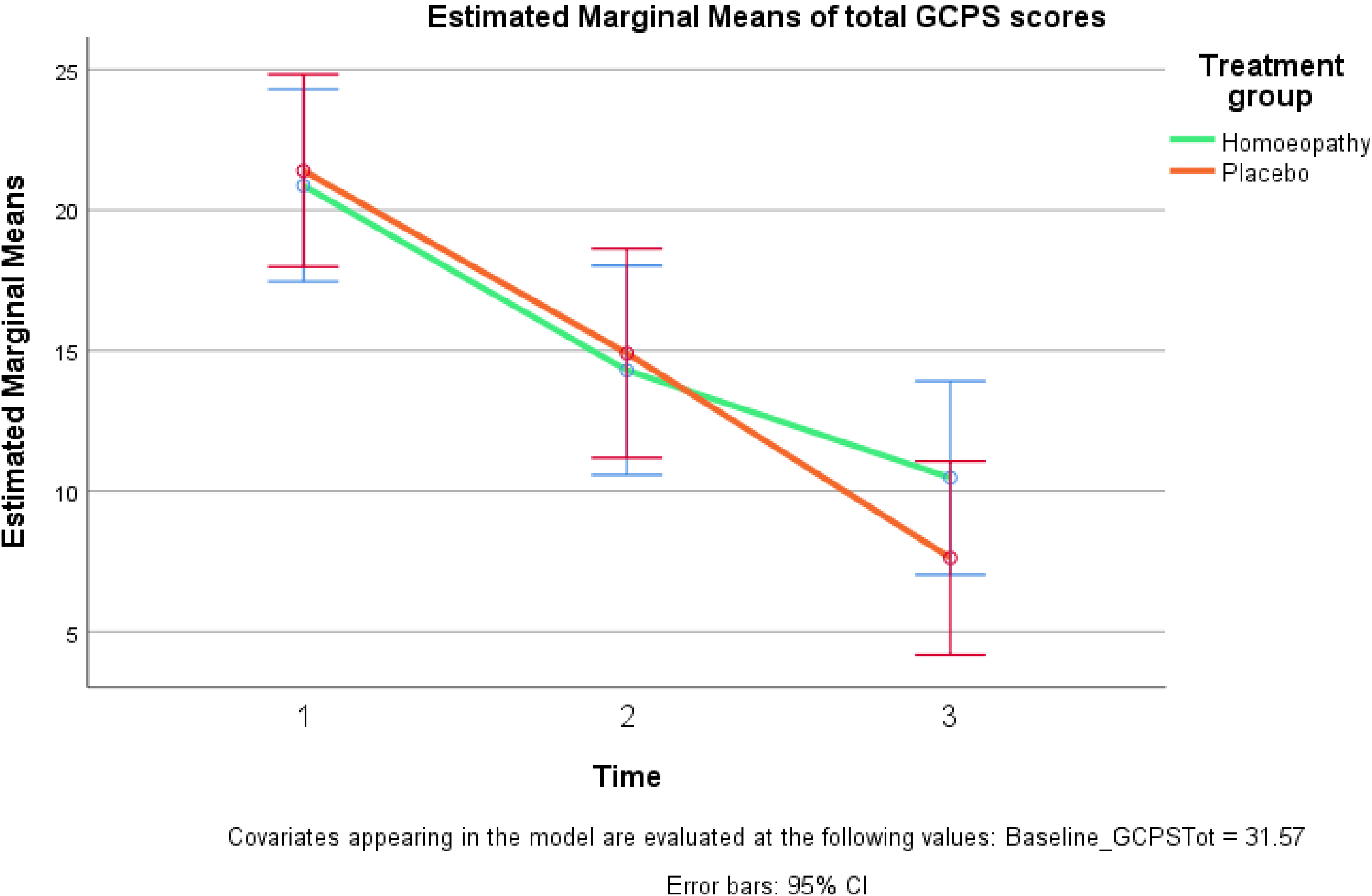
Line diagram of the estimated marginal means of total GCPS score with corrected baseline data. (CI, confidence interval; GCPS, Graded Chronic Pain Scale.)
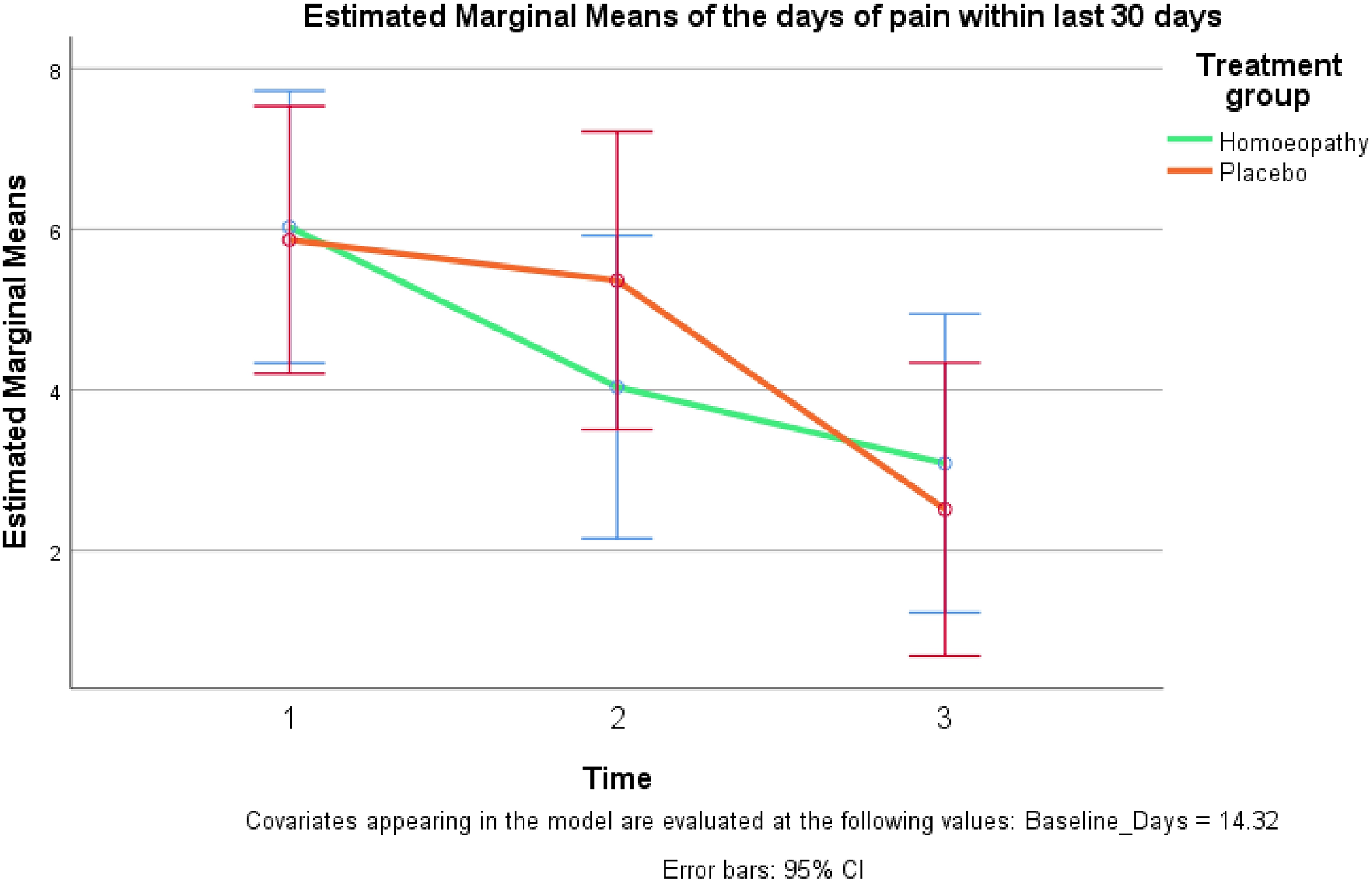
Line diagram of the estimated marginal means of mean days of pain within 30 days with corrected baseline data.
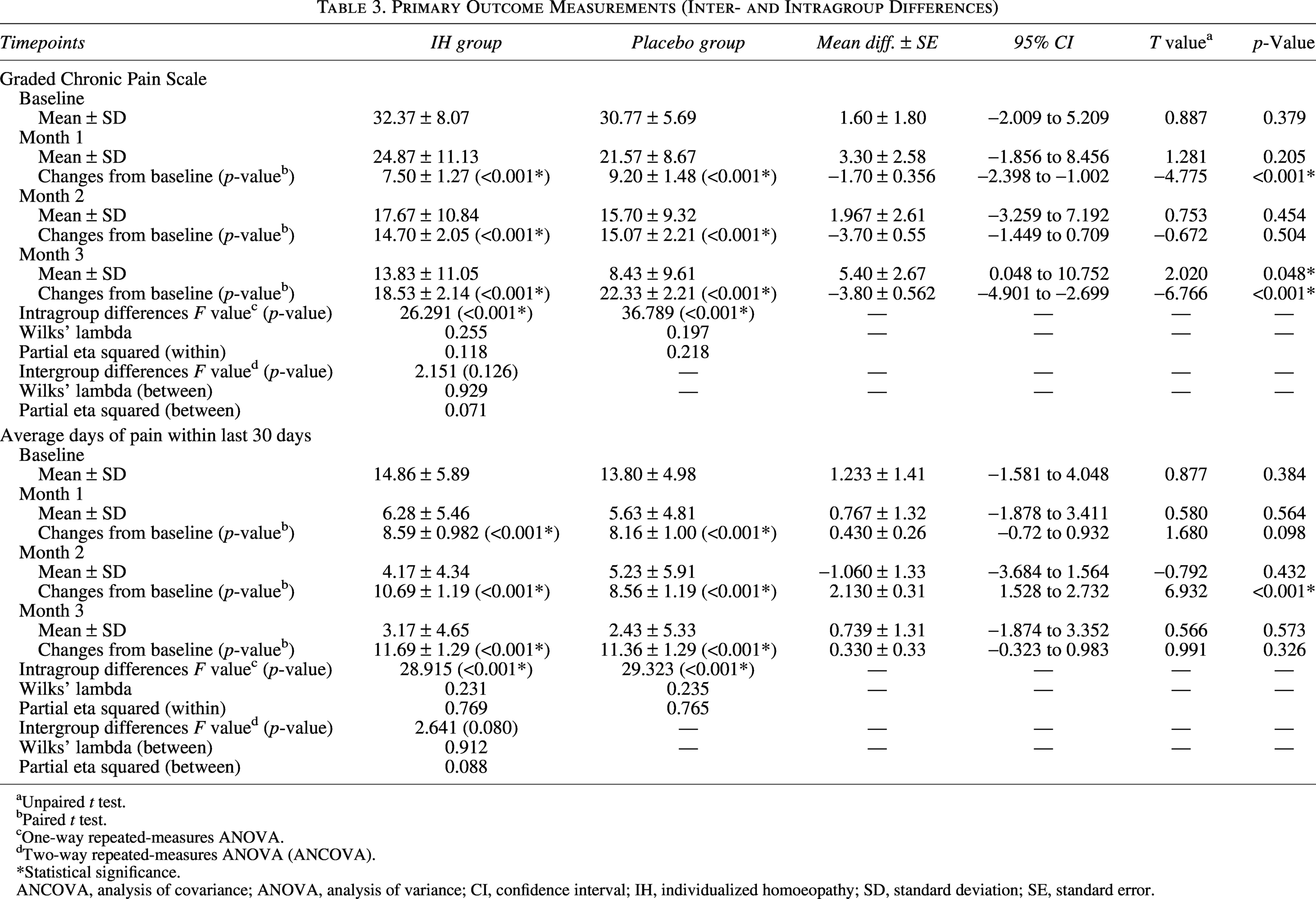
Primary Outcome Measurements (Inter- and Intragroup Differences)
Unpaired t test.
Paired t test.
One-way repeated-measures ANOVA.
Two-way repeated-measures ANOVA (ANCOVA).
Statistical significance.
ANCOVA, analysis of covariance; ANOVA, analysis of variance; CI, confidence interval; IH, individualized homoeopathy; SD, standard deviation; SE, standard error.
Outcomes
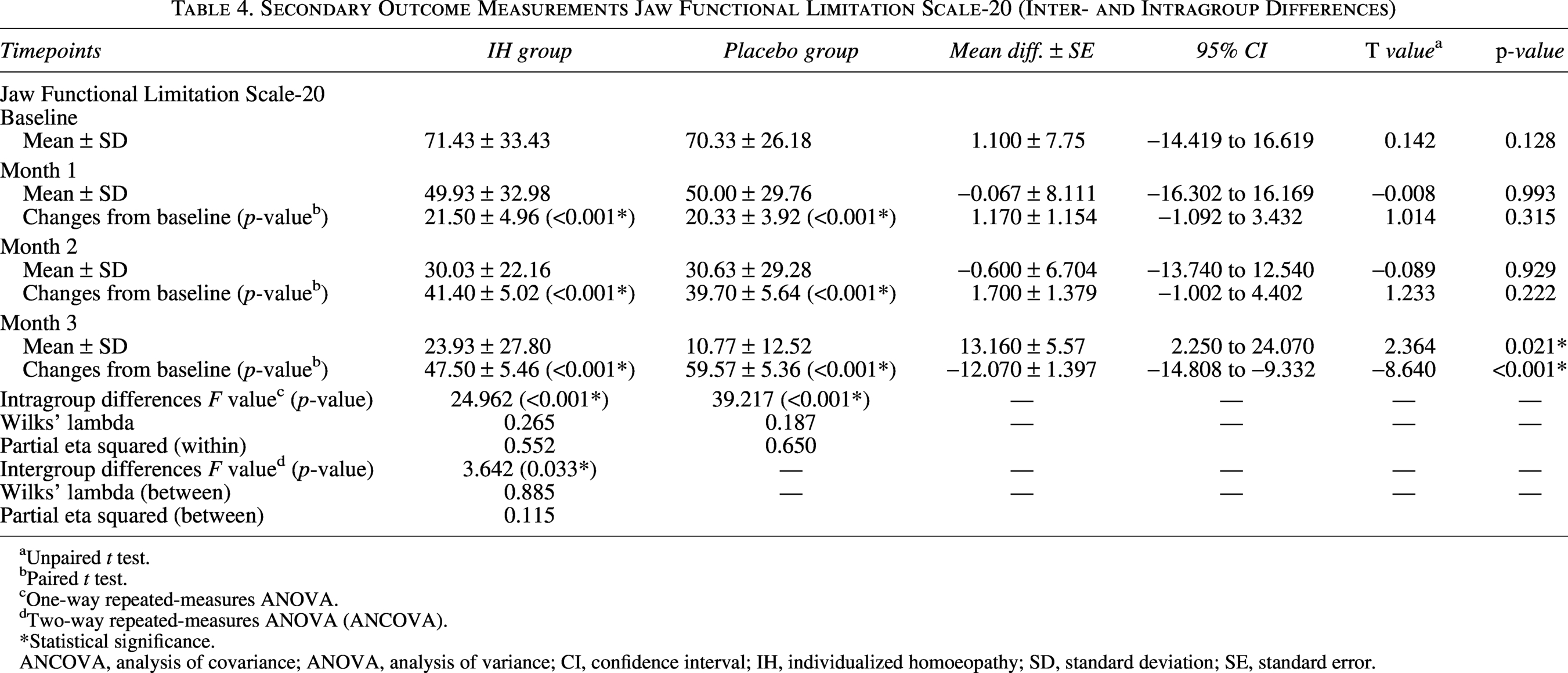
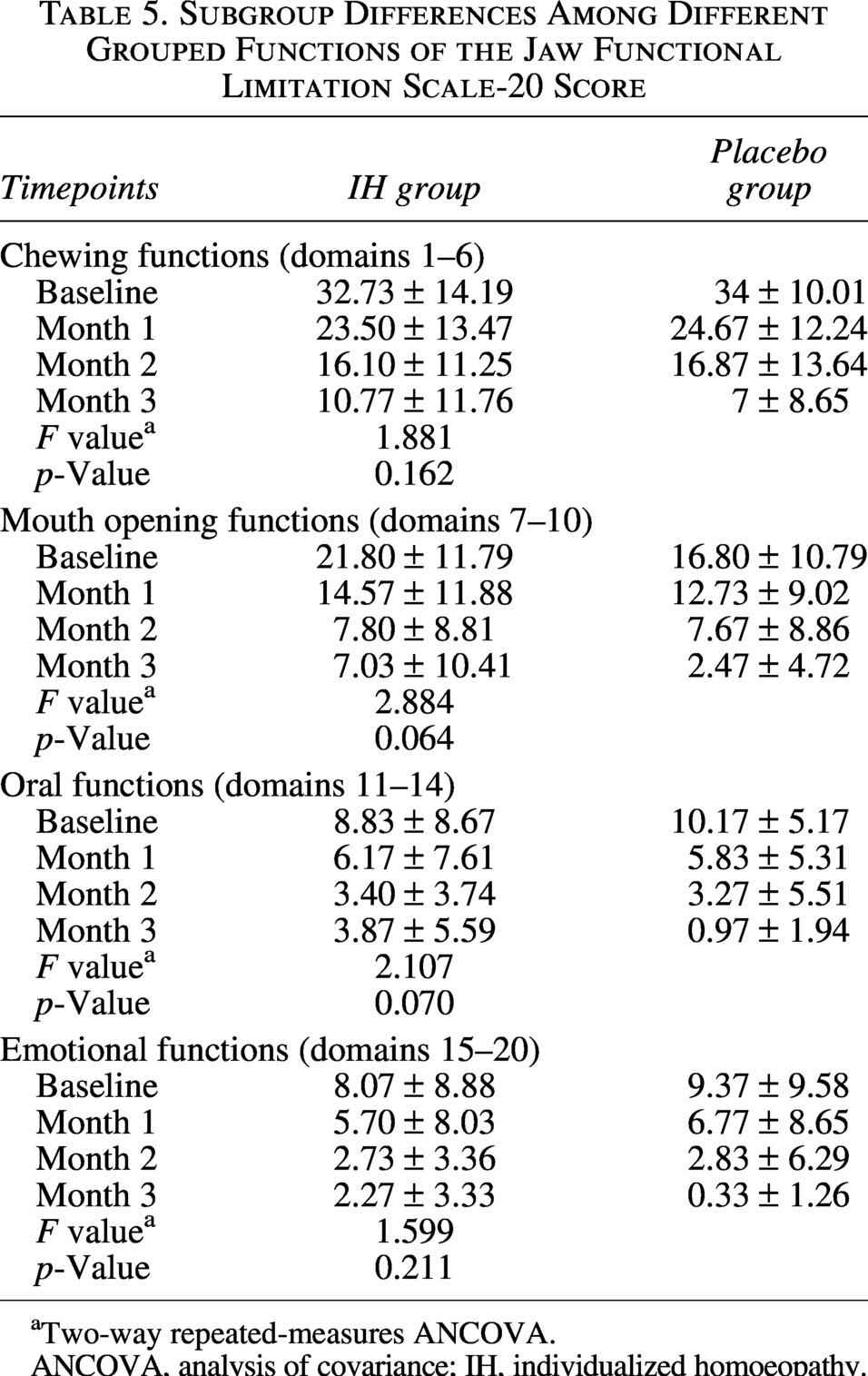
Exploratory intergroup comparisons at individual timepoints showed higher GCPS scores in the IHM group at Month 3 compared with the placebo group, indicating less favorable pain-related outcomes in the IHM group (mean difference ± SE: 5.40 ± 2.67; 95% CI: 0.048–10.752; p = 0.048; Table 3). As the overall group-by-time interaction was not statistically significant, these findings are reported descriptively and are not interpreted inferentially, in accordance with guidance for pilot trials. For the GCPS domain assessing the average number of pain days in the preceding 30 days, both groups showed significant within-group reductions from baseline at all follow-up points (all within-group p < 0.001). The overall intergroup difference over time did not reach statistical significance (two-way repeated-measures ANCOVA: F = 2.641, p = 0.080; Wilks’ lambda = 0.088), although temporal variation between groups was observed, particularly at Month 2, as shown in Figure 3 and Table 3. These findings are presented to illustrate trends and variability and should not be interpreted as evidence of the superiority of either intervention. Exploratory two-way repeated-measures ANCOVA identified a statistically significant group-by-time interaction for total JFLS scores (F = 3.642, p = 0.030; partial eta squared = 0.115). However, inspection of group-wise means showed that although both groups improved, the placebo group demonstrated a larger reduction in JFLS scores by Month 3 (mean ± SD: 10.77 ± 12.52) compared with the IHM group (23.93 ± 27.80), reflecting better jaw-related functional outcomes in the placebo group at the end of follow-up. Subdomain analyses indicated that changes in chewing function and mouth opening accounted for most of the observed temporal variation, while oral function and emotional domains showed smaller and overlapping changes between groups (Table 5). Given the pilot nature of the study and the presence of nonspecific improvements in both groups, these findings are reported to describe patterns, direction, and variability of change and should not be interpreted as evidence of clinical superiority of either intervention. Exploratory imaging changes classified as improved were primarily noted in osseous components of the temporomandibular joint, including the articular eminence and mandibular condyle, with qualitative reductions in features such as condylar flattening and osteophyte formation. Changes in joint space morphology were also observed in some participants classified as improved. Disc displacement showed qualitative improvement in two participants in the IHM group. Given the short duration of follow-up and the qualitative nature of assessment, these CBCT findings are considered exploratory and are reported to describe observed patterns rather than to infer structural modification attributable to the intervention.
Secondary Outcome Measurements Jaw Functional Limitation Scale-20 (Inter- and Intragroup Differences)
Unpaired t test.
Paired t test.
One-way repeated-measures ANOVA.
Two-way repeated-measures ANOVA (ANCOVA).
Statistical significance.
ANCOVA, analysis of covariance; ANOVA, analysis of variance; CI, confidence interval; IH, individualized homoeopathy; SD, standard deviation; SE, standard error.
Subgroup Differences Among Different Grouped Functions of the Jaw Functional Limitation Scale-20 Score
aTwo-way repeated-measures ANCOVA.
ANCOVA, analysis of covariance; IH, individualized homoeopathy.
Secondary Outcome Measurements Patient Health Questionnaire-4 (Inter- and Intragroup Differences)
Unpaired t test.
Paired t test.
Statistical significance.
CI, confidence interval; IH, individualized homoeopathy; SE, standard error.
Contingency Table on the Outcome of the Structural Changes in Cone Beam Computed Tomography Scan
Statistical significance.
IH, individualized homoeopathy; χ2, chi-square value.
Discussion
This randomized, double-blind, placebo-controlled pilot trial was designed primarily to assess the feasibility of conducting a controlled study of IHM in patients with TMJD, while secondarily exploring preliminary trends across clinical, functional, psychological, and imaging outcomes. In accordance with CONSORT recommendations for pilot trials, the findings are interpreted cautiously, with emphasis placed on feasibility metrics, sources of bias, and design implications for future definitive trials rather than on claims of clinical efficacy.
With respect to pain-related outcomes, both the IHM and placebo groups demonstrated statistically significant within-group reductions in GCPS scores over the follow-up period. As higher GCPS scores denote worse pain-related prognosis, these reductions indicate improvement over time irrespective of allocation. However, no statistically significant overall between-group difference or group-by-time interaction was observed for the primary pain outcome. Exploratory differences at individual timepoints, including higher GCPS scores in the IHM group at Month 3, were not supported by a significant interaction effect and are therefore reported descriptively. These findings suggest that nonspecific factors—such as natural fluctuation of symptoms, regression to the mean, concomitant care, and repeated clinical engagement—likely contributed substantially to observed pain improvement, underscoring the importance of avoiding inferential interpretation in an underpowered pilot study.
Jaw-related functional outcomes assessed using the JFLS-20 showed a statistically significant group-by-time interaction; however, interpretation of this finding requires careful consideration of score directionality. Although both groups demonstrated marked and clinically meaningful within-group reductions in JFLS scores over time (reflecting improved jaw function), inspection of mean values revealed that the placebo group exhibited greater functional improvement by Month 3 than the IHM group. Thus, despite a statistically significant interaction, the direction of effect does not support superior functional outcomes with IHM. These findings highlight the complexity of interpreting interaction effects in small pilot samples and suggest that functional measures may be sensitive to contextual and expectancy-related influences. Accordingly, JFLS findings should be viewed as exploratory and informative for outcome selection rather than as evidence of treatment benefit.
Psychological outcomes assessed using the PHQ-4 did not differ meaningfully between groups. Both groups showed similar, modest reductions in psychological distress over time, indicating that short-term individualized homoeopathic treatment did not confer measurable benefits for anxiety or depressive symptoms beyond those observed with placebo.
Qualitative CBCT imaging outcomes showed a statistically significant difference in distribution between groups, with more participants classified as “improved” in the IHM arm and more “worsened” classifications in the placebo arm. However, these findings must be interpreted with particular caution. Structural remodeling of degenerative osseous changes within a 3-month period is biologically implausible, and the qualitative, categorical nature of imaging assessment limits causal inference. Interobserver subjectivity, regression to the mean, and contextual interpretation may have influenced these findings. Consequently, the CBCT results are best regarded as hypothesis-generating observations highlighting variability in imaging interpretation rather than as evidence of intervention-related structural modification.
A major methodological limitation of the study was the high prevalence of betel nut and tobacco chewing among participants. These culturally ingrained habits are independently associated with increased mechanical loading, dental attrition, and progression of temporomandibular joint degeneration. Despite counseling, adherence to abstinence recommendations was inconsistent, with several participants resuming chewing once symptom severity decreased. This behavioral variability likely influenced pain trajectories, functional loading of the joint, and imaging outcomes, thereby confounding attribution of observed effects to the study intervention. Given the cumulative and progressive nature of this exposure, its confounding impact would be expected to increase in longer trials unless addressed through stricter eligibility criteria, stratification, or targeted behavioral interventions.
Feasibility outcomes demonstrated that recruitment, retention, and medication adherence were acceptable within the planned time frame. Nevertheless, marked expectancy effects were evident. The majority of participants—irrespective of actual allocation—believed they were receiving the active intervention, and investigators showed limited accuracy in guessing allocation for placebo recipients. These findings indicate challenges in maintaining blinding integrity and highlight the presence of expectancy bias in complementary medicine trials, which may have contributed to nonspecific improvements across multiple outcomes independent of the assigned intervention.
Additional limitations include the modest sample size inherent to pilot studies, short duration of follow-up, reliance on qualitative imaging assessments, and limited control over behavioral confounders. Although adverse events were mild and infrequent, the occurrence of unrelated acute illnesses and participant withdrawal further emphasizes the need for robust monitoring and clear attribution strategies in future research.
In summary, this pilot trial demonstrates that a randomized, double-blind study of individualized homoeopathic treatment for TMJD is feasible but methodologically challenging. The findings do not support definitive conclusions regarding clinical efficacy. Instead, they provide critical insights into outcome behavior, confounding influences, expectancy effects, and design constraints that should inform the planning of future adequately powered trials with longer follow-up, improved behavioral control, quantitative imaging endpoints, and enhanced strategies to mitigate bias.
Implications for Future Trials
This pilot study provides several important methodological lessons for the design of future definitive trials evaluating individualized homoeopathic interventions in TMJD. First, future studies should clearly distinguish feasibility objectives from efficacy testing at the protocol stage and be adequately powered, with sample size estimates informed by variability observed in functional outcomes rather than pain intensity measures alone. While this pilot offers preliminary parameters, formal sample size calculations should incorporate conservative assumptions, external evidence, and anticipated inflation for attrition, behavioral nonadherence, and expectancy effects. Second, major behavioral confounders—particularly betel nut and tobacco chewing—must be addressed through stricter eligibility criteria, stratification, or structured behavioral modification strategies, given their independent association with TMJ degeneration and their observed impact on outcomes. Third, functional outcome measures such as the JFLS-20 appear more responsive to short-term change and may be prioritized as primary endpoints. Fourth, future trials should strengthen blinding procedures and formally assess expectations to mitigate expectancy bias. Last, radiological outcomes should employ standardized, quantitative imaging protocols with longer follow-up durations to improve the interpretability of structural changes. Collectively, these refinements will enhance internal validity, reduce bias, and improve the interpretability of future trials in this domain.
Availability of Data and Material
The data of the study are presented as tables and figures within the article. Any further data required shall be provided upon request.
Trial Registration
The trial was prospectively registered at the Clinical Trial Registry of India (CTRI) vide CTRI/2023/05/052919 (https://ctri.nic.in/Clinicaltrials/regtrial.php?modid=1&compid=19&EncHid=36750.15025).
Ethical Considerations
The study was examined on ethical grounds, and clearance was obtained from the Institutional Ethics Committee of Regional Research Institute for Homoeopathy, Siliguri, vide Ref. No. 60/2022-23/RRI(H)/Siliguri/IEC/53 dated April 19, 2023 (UIN: TMJD/RCT/2023/08). Written informed consent was obtained from every participant before enrollment in the trial. The adverse events of the study were closely monitored, and any instance of such an event was to be reported directly or over the phone to the investigator. A Data Safety and Monitoring Board (DSMB) was constituted by the sponsor vide Ref. No. 50-5/2023-24/CCRH/Tech/Nodal Officer/TMJD/1836 dated July 31, 2024, to assess the safety of the study participants. An interim analysis was conducted and presented at the DSMB meeting on August 05, 2024. The Board was satisfied with the safety of the study, and the data were not unblinded.
Authors’ Contributions
B.B.: Conceptualization, methodology, formal analysis, investigation, resources, data curation, writing—original draft, writing—review and editing, visualization, supervision, project administration, and funding acquisition. S.G. and A.G.: Conceptualization, methodology, formal analysis, investigation, resources, data curation, writing—original draft, and writing—review and editing. N.B.: Conceptualization, methodology, investigation, resources, writing—original draft, and writing—review and editing. R.V.: Conceptualization, methodology, formal analysis, resources, data curation, writing—original draft, writing—review and editing, visualization, supervision, project administration, and funding acquisition. S.R. and S.K.: Conceptualization, methodology, formal analysis, writing—original draft, writing—review and editing, project administration, and funding acquisition.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of the following persons who had a significant role in the conduct of the submitted study. Mr. Richard Lepcha, Office Assistant, and Mrs. Sunita Barman, Pharmacist, were involved in the data entry, management, dispensing of medicines, and other essential activities associated with the study. Dr. Tanya Agarwal, Research Officer (Homoeopathy)/Scientist-1, was responsible for opening the allocation sequence and maintaining the adequate blinding in the study. Dr. Ranjit Sonny, Officer In-Charge, Regional Research Institute for Homoeopathy, Siliguri, was responsible for supervision of all the administrative and financial matters associated with the study. In addition, the authors would also recognize the efforts of Dr. Gurudev Choubey, Research Officer (Homoeopathy)/Scientist-4, and Dr. Ekta Gupta, SRF(H) who also contributed to the coordination of the trial. Dr. Lalchhuansanga Pachuau and Dr. Lalmuanpuia would also be acknowledged for their contribution during the protocol development phase of the trial. Mr. Anurag Bajpai, Statistician, Central Council for Research in Homoeopathy, is acknowledged for his contribution in the statistical analysis of the study data. The authors would also like to acknowledge Mr. Bhaja Debnath, Dr. Sharmistha Bhattacherjee, Dr. Souvik Sarkar, Dr. Patranu Parui, Dr. Ayan Midya, Dr. Madhumita Nath, Dr. Soumya Bhattacharyya, and Mr. Naresh Kumar for their valuable inputs and support in different phases of the study.
Author Disclosure Statement
The authors have no competing interests to declare.
Funding Information
The trial has been funded by the Central Council for Research in Homoeopathy, an autonomous body under the Ministry of Ayush, Govt. of India vide order no. F.No. 50-5/2023-24/CCRH/Tech/CRUSLG/Nodal Officer/Part File/TMJD/539 dated May 02, 2023 and F.No. 50-5/2023-24/CCRH/Tech/CRUSLG/Nodal Officer/Part File/TMJD/2800 dated September 12, 2023.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.