
Abstract
Introduction:
Labor pain and childbirth-related anxiety are significant factors that influence women’s physiological and psychological well-being during delivery. Nonpharmacological interventions such as guided imagery and music have been increasingly been used to support comfort and positive birth experiences. This randomized controlled trial aimed to determine the effects of guided imagery combined with music on labor pain, anxiety, and birth experience among primiparous pregnant women.
Methods:
A total of 123 primiparous women were randomly assigned to three groups: guided imagery with music, music-only, and control. The intervention groups received their respective practices in addition to routine intrapartum care, whereas the control group received only usual care. Labor pain was measured using the Visual Analog Scale (VAS), anxiety using the State Anxiety Inventory, and birth experience using the Childbirth Expectations and Experiences Scale-II. Birth experience was considered a secondary outcome in this study. Data were analyzed using repeated-measures analysis of covariance (ANCOVA) and one-way ANCOVA. Baseline pain, baseline anxiety, and planned pregnancy status were included as covariates in the adjusted models. Statistical significance was set at p < 0.05.
Results:
A significant group × time interaction was observed for labor pain, indicating that the trajectory of pain differed across the three groups over time (p < 0.05). Post-test anxiety scores were significantly higher in the music-only group compared to the other groups (p < 0.05). Birth experience scores were significantly higher in the music-only group compared to the control group (p < 0.05), with a small effect size. No adverse events were reported in any group.
Conclusion:
Both guided imagery combined with music and music-only interventions were associated with reductions in labor pain, although the pattern of change differed across time. However, neither intervention improved anxiety levels, and the findings for birth experience were limited. These results suggest that while nonpharmacological interventions may support certain aspects of childbirth, additional strategies may be needed to effectively address perinatal anxiety.
Introduction
Pain, as defined by the International Association for the Study of Pain and the World Health Organization (WHO), is “an unpleasant sensory and emotional experience associated with or resembling actual or potential tissue damage.” 1 However, labor pain is unique as it combines both physical and psychological aspects, including uterine contractions, fear, and a sense of powerlessness. 2 Many women report labor pain as the most intense pain they have ever experienced, making it a highly individual and distressing experience. 3 Despite birth being a natural and instinctive process, vaginal birth rates in Turkey are declining. 4 The perception of labor pain is one factor influencing this decrease. 5 Both pharmacological and nonpharmacological methods are available for managing labor pain exist, 6 and both with WHO and the American College of Obstetricians and Gynecologists (ACOG) support the use of nonpharmacological approaches.7,8 Nonpharmacological methods are cost-effective, simple, and can improve the childbirth experience by reducing pain and shortening labor duration, though they are not routinely implemented in practice. 9
Guided imagery, a technique that connects the mind and body, has shown effectiveness in pain management by promoting relaxation and positive energy. 10 Studies have found that guided imagery reduces stress and anxiety in pregnant women, especially in primiparous women, and can be easily applied during labor.11,12 Music, another nonpharmacological method, has also been found to reduce labor pain, decrease anxiety, and even shorten labor duration. In particular, the Acemasiran mode of music has muscle relaxant properties and aids in managing labor pain.13,14 Studies show that music reduces pain and anxiety during labor, particularly in first-time mothers. 13 Prenatal music intervention also shortens the first labor stage and reduces anxiety in nulliparous women, 15 fostering a positive birth experience and satisfaction. 16
Although the literature includes research investigating guided imagery and music as separate interventions during childbirth, no study has examined their combined use, leaving an important gap regarding whether integrating these two complementary techniques could produce stronger or more comprehensive effects. Therefore, the present study aimed to examine the effects of guided imagery combined with music intervention on labor pain, anxiety, and birth experience among primiparous pregnant women.
Accordingly, it was hypothesized (H) that guided imagery combined with music would affect perceived labor pain (H1a), state anxiety (H1b), and birth experience (H1c). In addition, it was hypothesized that music alone would affect perceived labor pain (H1d), state anxiety (H1e), and birth experience (H1f).
Materials and Methods
Study design
This study was conducted in the maternity unit of a public hospital in western Türkiye between March 2023 and March 2024. The study was a nonblinded randomized clinical trial with a three-arm design (guided imagery and music intervention, music intervention, and control) during labor and delivery. The Consolidated Standards of Reporting (CONSORT) checklist (Fig. 1) was used as a reporting guide (Supplementary Appendix A1, CONSORT checklist). The study was registered at https://www.clinicaltrials.gov (ID: NCT06035172) prior to recruitment.
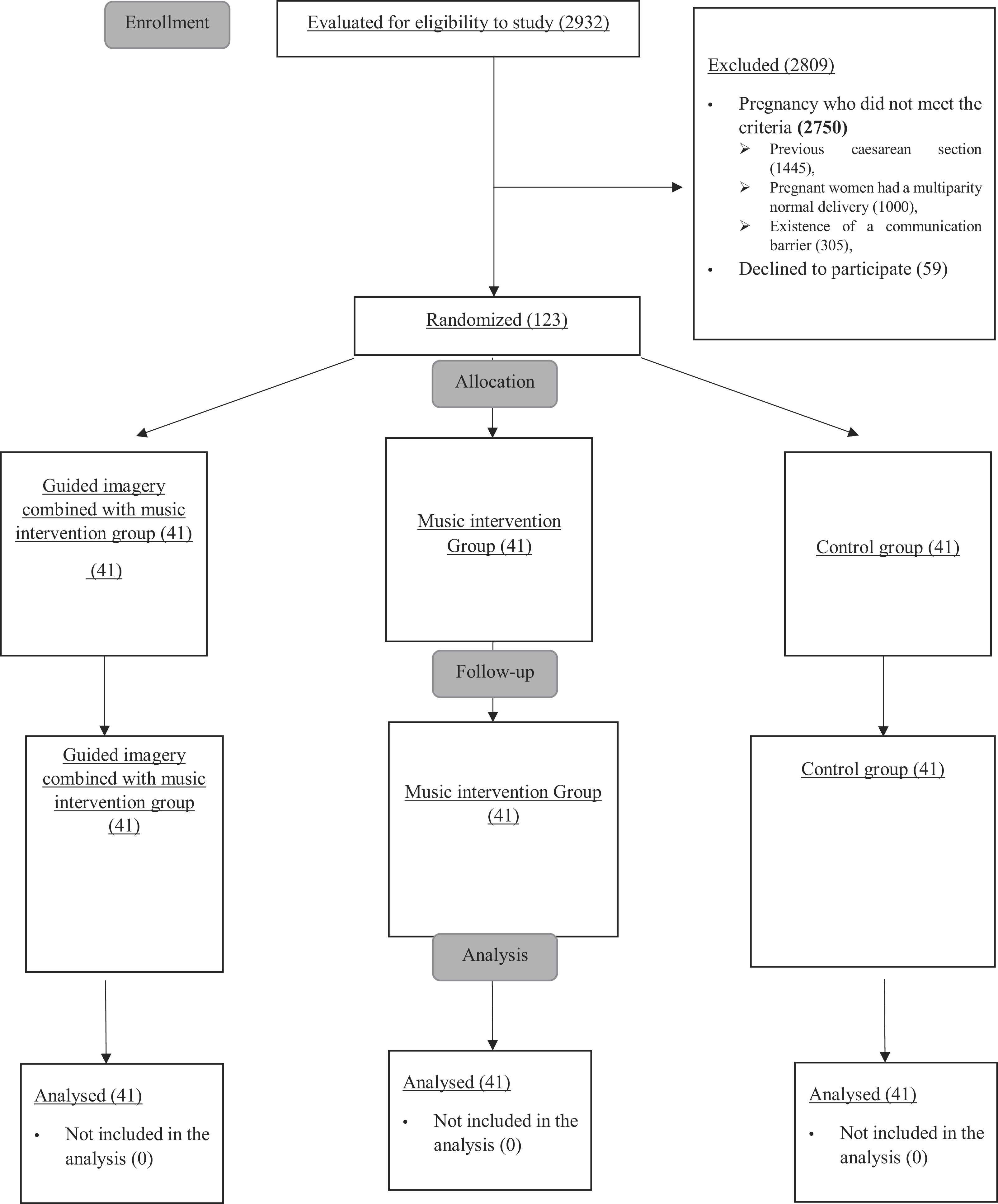
Consolidated standards of reporting trials 2018 flow diagram. G1, guided imagery group; G2, music recital group; G3, control group; VAS, Visual Analog Scale; STAI Form TX-1, State-Trait Anxiety Inventory; CEES-1, Childbirth Expectations and Experiences Scale-I; CEES-II, Childbirth Expectations and Experiences Scale-II; T1, cervical dilation 5–6 cm before intervention; T2, after the intervention when the cervical dilation was 5–6 cm; T3, after the intervention when the cervical dilation was 7–8 cm; T4, one hour after the placenta emerges at the end of labor; M1, guided imagery recital; M2, music recital; M3, no intervention.
Population and sample
The study population consisted of primiparous pregnant women with cervical dilation of 4 cm or more who were admitted to the maternity unit.
Study inclusion criteria
Women were eligible for inclusion if they met the following criteria: aged 18–35 years, primiparous, singleton cephalic pregnancy, term gestation, spontaneous onset of labor, cervical dilation ≥4 cm at admission, absence of high-risk pregnancy conditions (e.g., gestational diabetes mellitus or hypertension), no previous cesarean section, no use of pharmacological pain relief during labor prior to enrollment, literate, fluent in Turkish, and able to communicate effectively.
Study exclusion criteria
Women were excluded prior to randomization if they did not meet the inclusion criteria or had a communication barrier preventing informed consent or data collection.
Sample size and randomization
The sample size of the study was calculated using the G*Power 3.1.9.7 software program based on the Visual Analog Scale (VAS) used in the study by Gönenç and Dikmen. 17 Based on this reference study, the sample size for each group was calculated as 31, taking into account the effect size (f = 0.25), a 5% margin of error (α = 0.05), and 80% power in the analysis. Randomization in the study was performed by the researcher using a computer program. Pregnant women meeting the inclusion criteria were numbered from 1 to 123 according to the order of acceptance, and these numbers were assigned to the intervention and control groups using www.randomizer.org (Fig. 1). There were no losses after group assignments, and the study was completed with 41 participants in each group. The sample size was calculated based on the primary outcome of labor pain measured using the VAS. Although state anxiety was also defined as a primary outcome, no separate power calculation was performed for this variable. A post hoc power analysis was also conducted for the anxiety outcome (State Anxiety Inventory-TX [STAI-TX]).
Consent and ethics
Ethical approval for the study was obtained from the Clinical Research Ethics Committee of the relevant institution (Decision no.: 2022/362). Permission to conduct the research was also granted by the hospital administration. The study was carried out in accordance with the principles of the Declaration of Helsinki. Primiparous pregnant women admitted to the labor unit were informed about the purpose, procedures, and voluntary nature of the study. Written informed consent was obtained from all participants prior to enrollment. Participants were assured that refusal to participate would not affect their access to routine care and that they would continue to receive standard intrapartum services without any consequences.
Characteristics of the institution
At the institution where the study was conducted, maternity services are structured based on the Labor–Delivery–Postpartum (LDP) model and consist of 10 single-occupancy LDP rooms. Each room includes a functional birthing bed, a radiant warmer for the initial assessment of the newborn, a companion chair, and a dedicated toilet and bathroom area for the mother. The unit was managed by specialist physicians and midwives experienced in supporting physiological labor, and pregnant women receive personalized, evidence-based routine care. However, guided imagery and music interventions are not routinely included in the unit’s nonpharmacological methods. Furthermore, due to the new structure of the maternity unit, the integration of nonpharmacological methods for labor pain management into clinical practice has not yet become widespread.
Interventions
Development and implementation of the guided imagery and music interventions
In this study, two nonpharmacological interventions were developed and implemented in addition to routine maternity care: a guided imagery and music intervention (G1) and a music-only intervention (G2). All interventions were prepared before data collection and underwent content development, expert review, and pilot implementation to ensure their clinical suitability for the labor process. The recordings used for both interventions were professionally created, edited in accordance with expert opinions (two obstetricians, two midwives, and two mental health professionals), and pilot-tested on three pregnant women in active labor. Final recordings were uploaded to wireless headphones, which were disinfected after each use and provided with hygienic disposable covers, and sound levels were standardized in advance. All interventions were implemented in single-occupancy delivery rooms under appropriate environmental conditions that ensured quietness and privacy. At the hospital where the study was conducted, labor was monitored by midwives, and during the second stage of labor, the obstetrician and midwife jointly managed the birth. Participants were assessed for eligibility when they reached 4 cm cervical dilation. Baseline measurements (Pregnancy Diagnosis Form, VAS, STAI TX-I, Childbirth Expectations and Experiences Scale-I [CEES-I]) were obtained. After randomization, they were assigned to the appropriate groups. All women continued to receive standard intrapartum care throughout labor (Fig. 2).
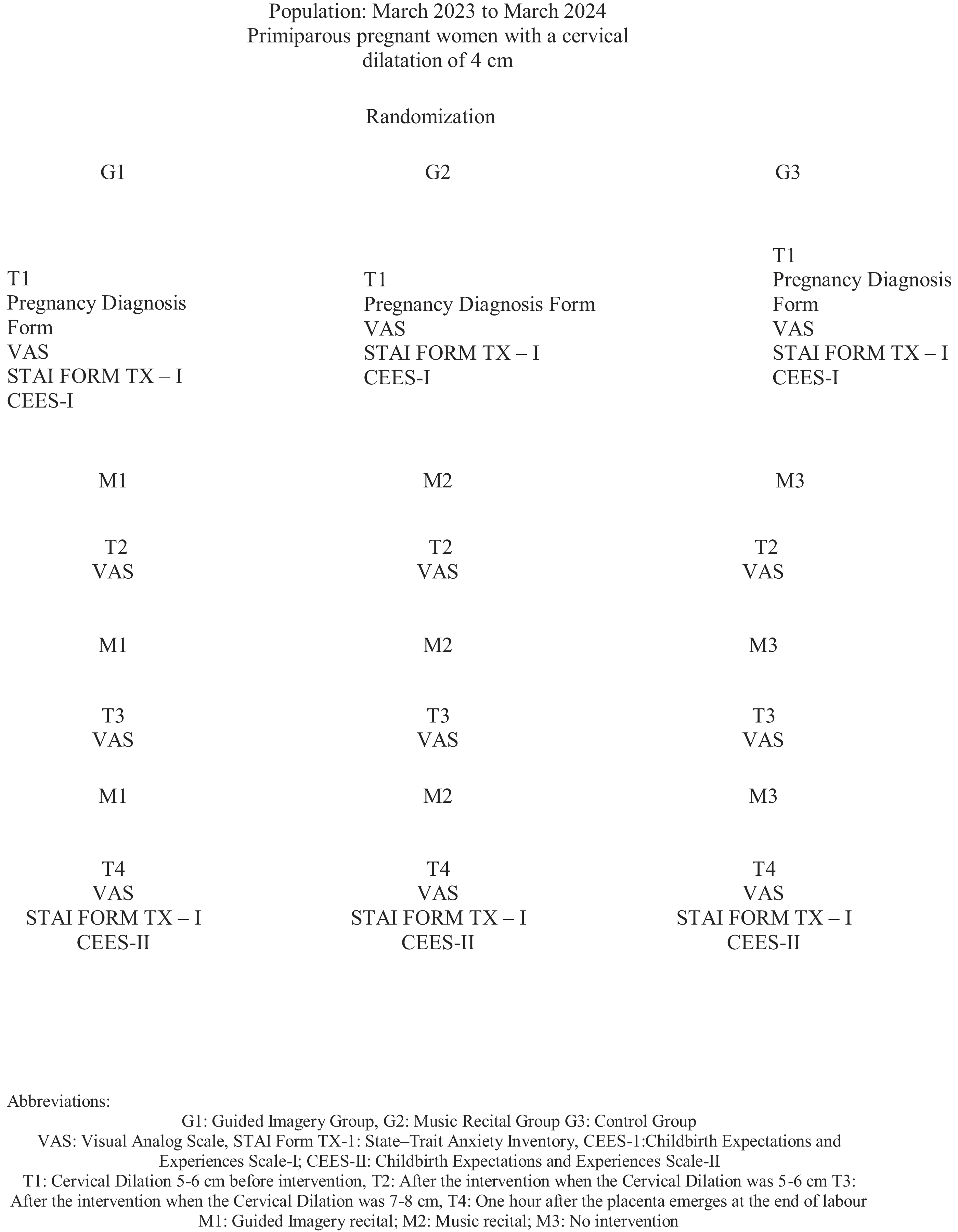
Research process.
Intervention groups
G1: Guided imagery + music intervention
The guided imagery script was developed based on Owen’s guided imagery framework 18 and supported by relevant literature on childbirth and imagery-based interventions. The intervention consisted of a 15-min professionally recorded audio script. The content included structured breathing exercises, progressive muscle relaxation cues, and guided visualization scenarios. Participants were instructed to imagine a calm natural environment (e.g., a peaceful garden) and to associate the progression of labor with a symbolic opening process (e.g., a blooming flower), synchronized with their breathing and uterine contractions. The script also incorporated positive affirmations emphasizing trust in the body, a sense of control, and anticipation of meeting the baby (Supplementary Appendix A2). All verbal content was accompanied by background music prepared in the Acemasiran makam. The recording was evaluated by experts for content quality, emotional relevance, and clinical safety. After the pilot test, minor adjustments were made to the tempo and musical balance. Participants listened to the recording in 15-min sessions during predefined stages of labor based on cervical dilation. They were encouraged to maintain a comfortable position throughout the session and follow the breathing and visualization prompts.
G2: Music intervention only
This intervention consists of a 15-min reed flute audio recording in the Acemasiran makam, prepared by an artist experienced in therapeutic music. The Acemasiran makam was selected based on its documented therapeutic properties and its established role in traditional Turkish music therapy, where specific makams are believed to influence emotional and physiological states, such as relaxation, autonomic regulation, and pain modulation. Previous studies have suggested that this musical mode may contribute to muscle relaxation, reduction of labor pain, and emotional balance.13,14,19 To ensure intervention consistency and internal validity, a standardized music recording was used for all participants in the music group. Allowing participants to select their own music could have introduced variability in tempo, rhythm, familiarity, and emotional associations, potentially confounding the effects of the intervention. Therefore, the use of a single controlled musical stimulus was considered methodologically appropriate for this randomized controlled trial. The recording was evaluated and pilot-tested by the same expert panel as G1. Participants listened to the music recording without guided imagery prompts during the same stages of labor. The duration, environmental conditions, and technical standards were kept consistent with those used in G1.
G3: Control group
Women in the control group received no structured nonpharmacological interventions and were provided only standard intrapartum care. Routine care included monitoring maternal vital signs, fetal heart rate assessment with Non-Stress Test (NST) or Doppler, uterine contraction monitoring, emotional support, and appropriate positioning aids. Oxytocin was administered to enhance labor when deemed necessary by the obstetrician. No additional music, relaxation techniques, or audio support tools were used outside of the research protocol. Measurements were taken at the same time points as in the intervention groups.
Blinding
Due to the nature of the interventions, it was not possible to blind the participants. However, the assessment of outcome measures was supported by clinic-based midwives who were unaware of the participants’ group allocation. These midwives were not involved in the delivery of the intervention and were responsible for administering the measurement tools. Furthermore, the data were coded prior to statistical analysis, and the statistician was kept unaware of the group allocation to ensure objectivity in data interpretation.
Data collection tools
The “Pregnancy Diagnosis Form,” “VAS,” “STAI Form TX-1,” CEES-I, and CEES-II were used to collect the research data. The data collection tools are presented below.
Pregnancy diagnosis form: This form, developed by the researchers based on literature,13,15 includes 13 questions about women’s sociodemographic (age, education, employment, income, and family type) and obstetric characteristics (pregnancy history, voluntary pregnancy).
Primary outcomes
The primary outcomes were labor pain and state anxiety. Labor pain was assessed using the VAS, and anxiety was measured using the STAI Form TX-1.
VAS: It was developed by Price et al. in 1983 to measure pain intensity and monitor pain. The VAS is 10 cm long, and its two ends are named differently. On the scale, “0”means no pain, and “10” means the most severe pain. The VAS is a measurement tool frequently and safely used to evaluate labor pain.20,21 The VAS measurement was used to test the first and fourth hypotheses, H1a and H1d.
STAI Form TX-1: The State Anxiety Inventory, developed by Spielberger et al. 22 and translated into Turkish by Oner and Le Compte, 23 includes 20 items assessing state anxiety. This study used the state anxiety inventory, with total scores ranging from 20 to 80. Higher scores indicate higher anxiety levels. The inventory is sensitive to emotional changes, with a Cronbach’s α of 0.83 in reliability analysis. In this study, Cronbach’s α was 0.91 at T1 and 0.97 at T4. State anxiety data were used to test the second and fifth hypotheses (H1b and H1e).
Secondary outcomes
The secondary outcome measure was the birth experience, assessed using the CEES-II.
CEES-I and CEES-II: The CEES scale, developed by Tanglakmankhong 24 and adapted into Turkish by Muslu and Yanıkkerem, 25 consists of two sections: CEES-I and CEES-II. CEES-I assesses birth expectations before labor, whereas CEES-II evaluates whether those expectations were met after birth. CEES-I includes 36 items with “Yes” or “No” responses, with evaluations categorized as “Met expectations,” “Unmet expectations,” “Unexpectedly met expectations,” and “Unexpectedly not met expectations.” Item 37 in CEES-II asks about overall birth satisfaction using a 4-point Likert scale. Cronbach’s α for CEES-II is 0.891, with this study reporting 0.63. CEES-II data were used to test the third and sixth hypotheses (H1c and H1f).
Data analysis and evaluation
The data obtained from the study were analyzed using the program SPSS for Windows (version 20.0, Statistical Package for Social Sciences). Continuous variables were presented as means and standard deviations (SDs), and categorical variables as frequencies and percentages. Prior to analysis, assumptions of normality, homogeneity of variances, and homogeneity of regression slopes were evaluated. Baseline characteristics were compared across groups using chi-square tests for categorical variables and one-way analysis of variance for continuous variables. Baseline pain, baseline anxiety, and planned pregnancy status were included as covariates based on both theoretical relevance and observed baseline differences. For the pain outcome (VAS), a repeated-measures analysis of covariance (ANCOVA) was conducted to examine the group (G1, G2, G3) × time (T2, T3, T4) interaction while controlling for baseline pain (VAS T1) and planned pregnancy status. The assumption of sphericity was assessed using Mauchly’s test and when violated, the Greenhouse–Geisser correction was applied. For the anxiety outcome (STAI-TX), a one-way ANCOVA model was conducted to examine group differences at post-test (T4), adjusting for baseline anxiety (STAI-TX T1) and planned pregnancy status. For birth experience, assessed using the CEES-II, a one-way ANCOVA was performed with planned pregnancy status included as a covariate. Adjusted group means were estimated using estimated marginal means (EMMs) derived from the fitted models. Pairwise comparisons were conducted using the Bonferroni correction. Effect sizes were reported as partial eta squared (ηp2) for overall tests and standardized mean differences (Cohen’s d) for pairwise comparisons. Statistical significance was set at p < 0.05.
Results
Table 1 presents the baseline characteristics of the participants. The groups were comparable in most descriptive characteristics; however, significant baseline differences were observed in pain, anxiety, and planned pregnancy status. Therefore, these variables were included as covariates in subsequent analyses. Table 2 summarizes the covariate-adjusted effects of the interventions on pain, anxiety, and birth experience. For pain, repeated-measures ANCOVA revealed significant main effects of group (F = 38.01, p < 0.001, ηp2 = 0.41) and time (F = 52.78, p < 0.001, ηp2 = 0.32), as well as a significant group × time interaction (F = 25.72, p < 0.001, ηp2 = 0.32). Baseline pain (F = 1.93, p = 0.055) and planned pregnancy status (F = 0.70, p = 0.403) were not significant covariates. As shown in Table 3, adjusted mean pain scores were significantly lower in both intervention groups compared with the control group at T2 and T3. Specifically, at T2, both G1 and G2 had significantly lower pain scores than G3 (p < 0.001 for both comparisons). At T3, these differences became more pronounced, with both intervention groups continuing to show significantly lower pain scores than G3 (p < 0.001). At T4, only the difference between G2 and G3 remained significant (MD = −1.29, p = 0.044). Within-group comparisons indicated that pain decreased from T3 to T4 in G1 (p = 0.009), from T2 and T3 to T4 in G2 (p = 0.019 and p = 0.003, respectively), and across all time points in G3 (p < 0.001). For anxiety, Table 2 shows a significant group effect on post-test STAI-TX scores (F = 39.40, p < 0.001, ηp2 = 0.53), with baseline anxiety also identified as a significant covariate (F = 26.18, p < 0.001, ηp2 = 0.18), whereas planned pregnancy status was not significant (F = 1.55, p = .216). As detailed in Table 3, post-test anxiety scores were significantly higher in G2 compared with both G1 (MD = −8.80, p < 0.001) and G3 (MD = 7.14, p < 0.001), whereas no significant difference was observed between G1 and G3. For birth experience, Table 2 indicates a significant group effect on CEES-II scores (F = 4.40, p = 0.014, ηp2 = 0.05), although the effect size was small. Planned pregnancy status was also a significant covariate (F = 5.17, p = 0.025, ηp2 = 0.04). As shown in Table 3, G2 had significantly higher CEES-II scores than G3 (MD = 0.15, p = 0.017), whereas other group comparisons were not statistically significant.
Comparison of the Descriptive Characteristics of the Experimental and Control Groups (N = 123)
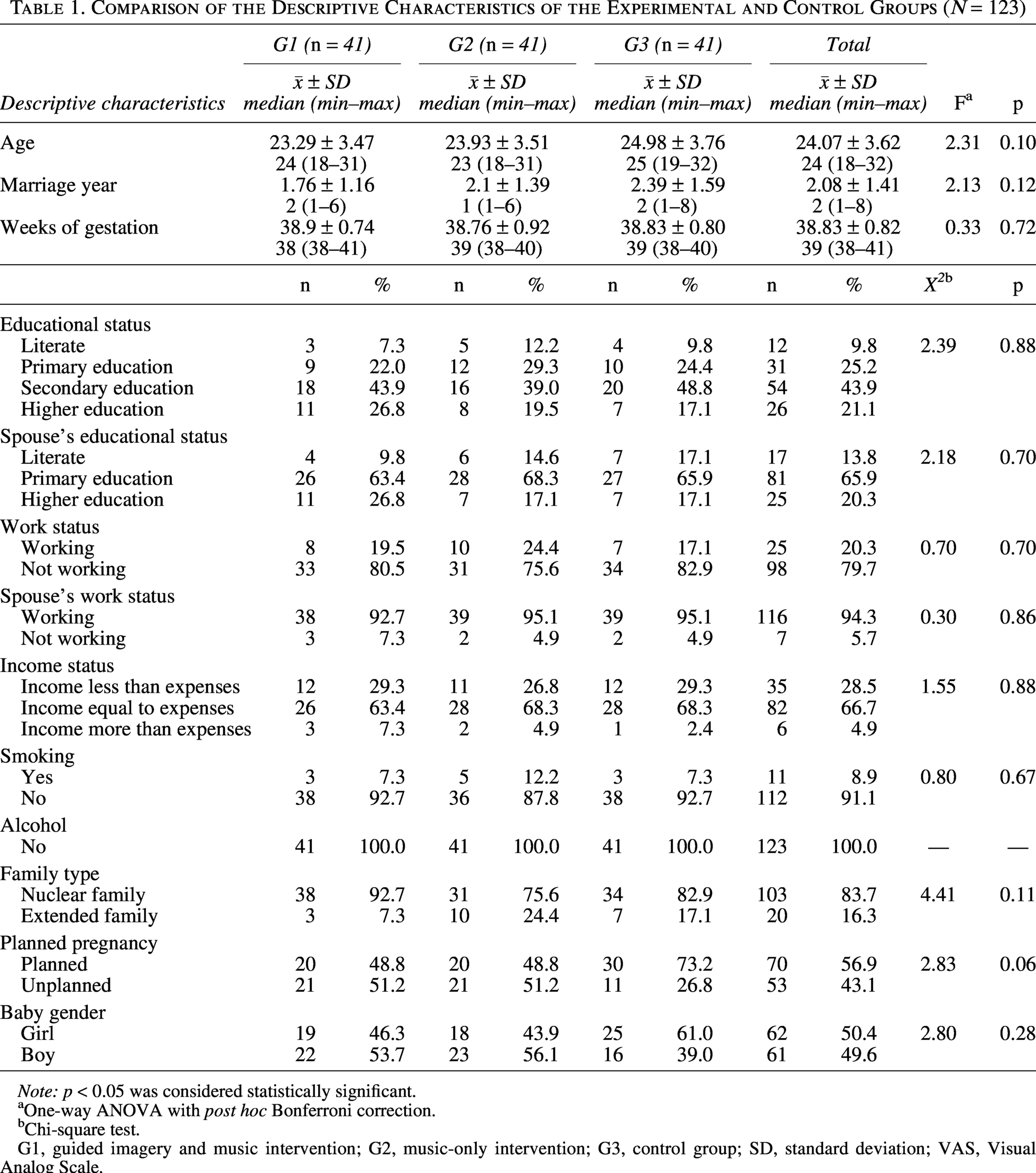
Note: p < 0.05 was considered statistically significant.
One-way ANOVA with post hoc Bonferroni correction.
Chi-square test.
G1, guided imagery and music intervention; G2, music-only intervention; G3, control group; SD, standard deviation; VAS, Visual Analog Scale.
Covariate-Adjusted Analysis of Covariance Results for Intervention Effects on Pain, Anxiety, and Birth Experience
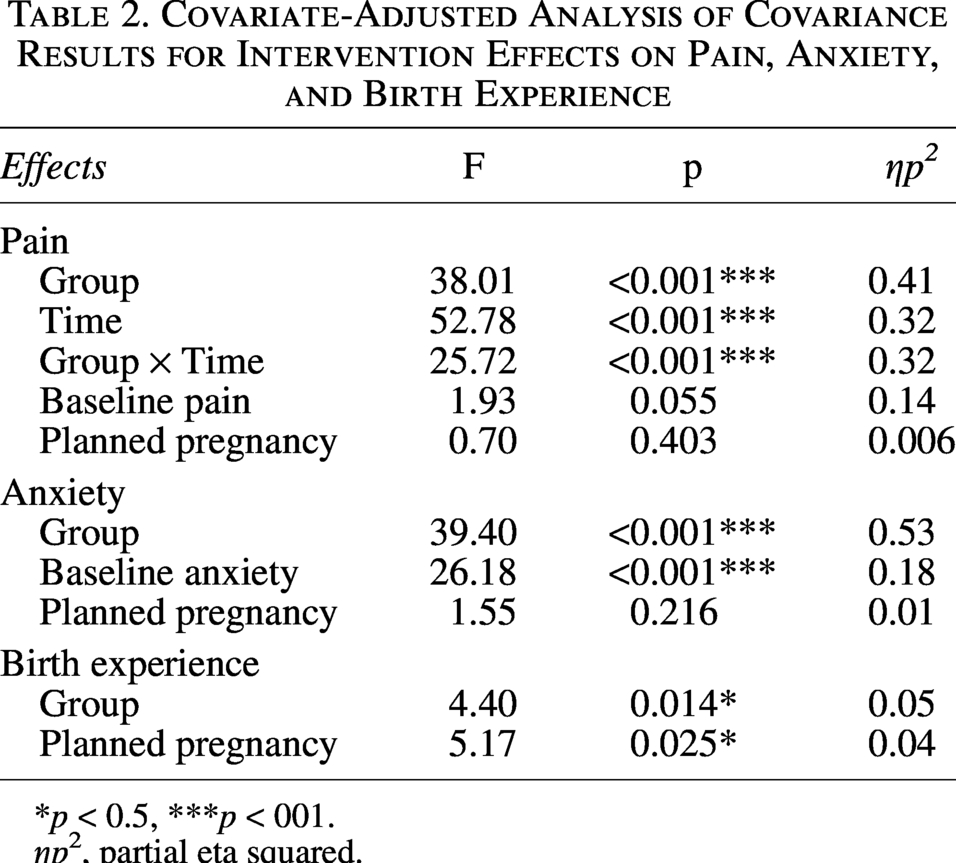
*p < 0.5, ***p < 001.
ηp², partial eta squared.
Adjusted Means and Pairwise Comparisons of Pain, Anxiety, and Birth Experience Across Intervention Groups
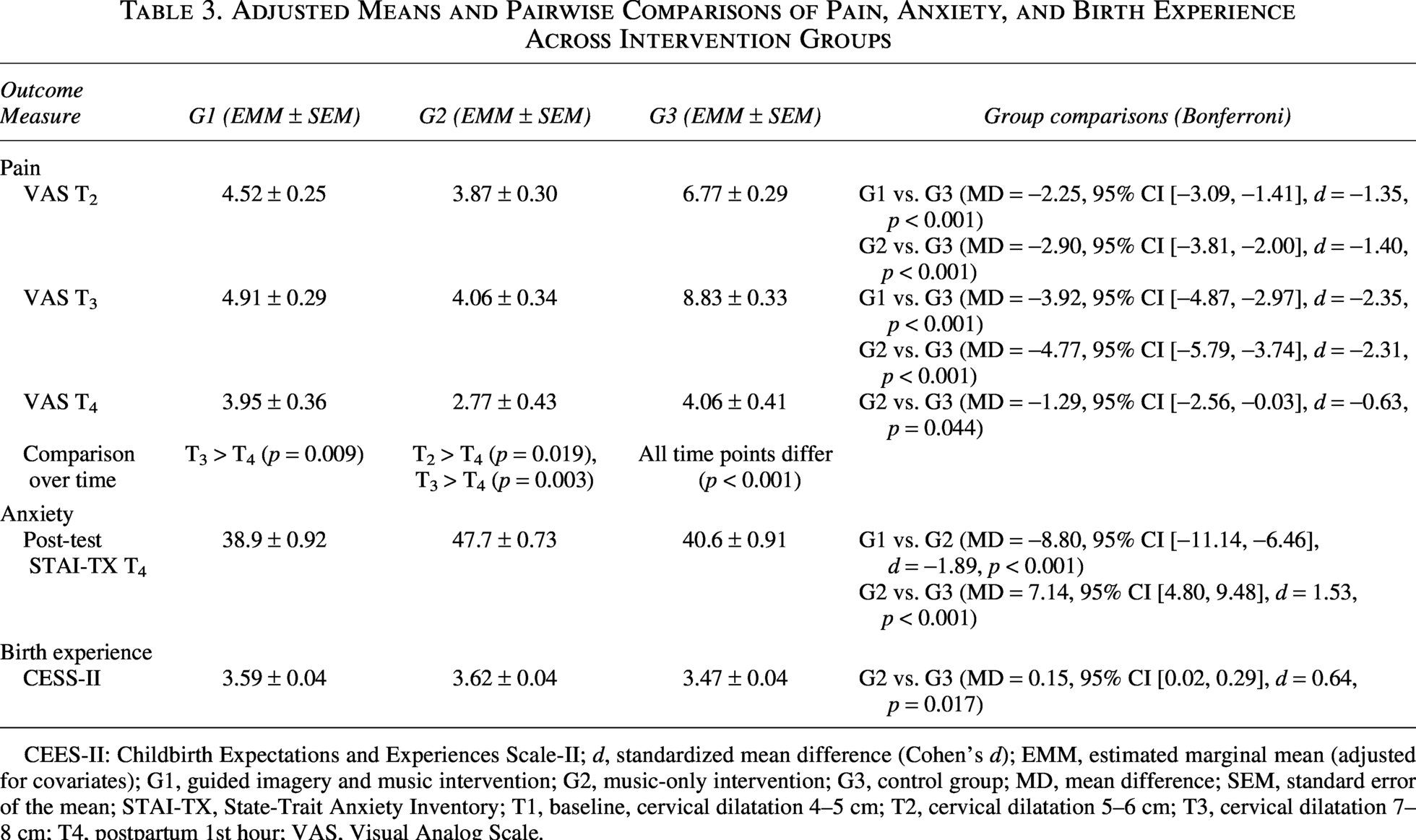
CEES-II: Childbirth Expectations and Experiences Scale-II; d, standardized mean difference (Cohen’s d); EMM, estimated marginal mean (adjusted for covariates); G1, guided imagery and music intervention; G2, music-only intervention; G3, control group; MD, mean difference; SEM, standard error of the mean; STAI-TX, State-Trait Anxiety Inventory; T1, baseline, cervical dilatation 4–5 cm; T2, cervical dilatation 5–6 cm; T3, cervical dilatation 7–8 cm; T4, postpartum 1st hour; VAS, Visual Analog Scale.
Adverse events
No adverse events, complications, or intervention-related discomfort were observed or reported in any of the study groups during the intervention, labor, or postpartum period.
Discussion
Pain is a significant human experience, and nonpharmacological methods such as music intervention and guided imagery are increasingly used for labor pain management due to their low cost and ease of application. This study explored the effects of these interventions on labor pain, anxiety, and birth experience in primiparous women. No negative outcomes were observed during or after the interventions, highlighting their potential benefits during childbirth.
The literature identifies several factors that may influence labor pain, anxiety, and birth experience, including age,2 marriage duration, 26 income status, 27 gestation week, 26 pregnancy planning, 26 education level, 28 employment, 28 family type, 29 and participation in pregnancy education. 2 Some baseline differences were observed in the present study; therefore, these variables were controlled for in the adjusted analyses.
The effect of guided imagery and music intervention on the management of labor pain
Relieving labor pain is crucial in medical care, with epidural analgesia being the most effective method. However, factors such as women’s preferences, contraindications, accessibility, and technical issues may limit its use. 30 Therefore, many women choose nonpharmacological methods for pain management. 31 Literature shows that guided imagery reduces pain and anxiety, although most studies focus on surgery rather than childbirth. 32 One study using guided imagery during childbirth found significant pain reduction when pregnant women watched a guided imagery video. 12 Similarly, this study observed a significant decrease in pain scores in the G1, aligning with previous research findings. However, given the study design, the observed effects should be interpreted as the outcome of the combined intervention rather than the isolated effect of guided imagery. Research on music as a nonpharmacological method for pain relief shows varying evidence quality; however, it is generally effective in reducing pain and increasing satisfaction. 6 A systematic review found that music interventions reduce pain and anxiety during childbirth. 33 Music significantly reduces pain and fear in the active labor phase, 17 with studies showing its benefits during birth and postpartum. 34 A study on ney music during labor found lower pain and anxiety levels in the music group. 35 Acemasiran mode music has previously been associated with reduced labor pain and anxiety. 19 In the present study, the use of Acemasiran music was associated with lower pain scores during labor, supporting previous findings. 36 While no pain reduction was observed in the control group, pain scores decreased in the fourth measurement, 1 h after birth. The literature shows various music genres used in audio recordings,35,37 highlighting the need for better understanding of music genre preferences. 38 The long-term effects of music interventions are unclear, and further research is needed to explore the impact of guided imagery with music intervention on labor pain. In the present study, pain scores in the music-only group decreased at the postpartum measurement. However, this finding should be interpreted with caution, as the reduction in pain after delivery may primarily reflect the natural cessation of uterine contractions rather than a specific effect of the intervention. Therefore, attributing this decrease solely to the music intervention may not be appropriate. These findings support the hypotheses that both guided imagery combined with music (H1a) and music alone (H1d) would influence perceived labor pain. Importantly, during the active phase of labor, both intervention groups demonstrated lower pain levels compared to the control group, suggesting that the interventions may have contributed to pain management during labor rather than in the postpartum period.
The effect of guided imagery and music intervention on the management of childbirth anxiety
Women with perinatal anxiety have reduced coping abilities during childbirth, which can affect labor progression and increase the likelihood of cesarean sections. Low anxiety levels are crucial for a positive perception of pregnancy and childbirth. 39 Nonpharmacological interventions, such as aromatherapy, are commonly used to reduce anxiety and pain during childbirth. 40 Even light touch can reduce cortisol and catecholamine levels, thereby lowering anxiety during labor. 41 Audiovisual therapy during childbirth has been shown to reduce pain and anxiety compared with standard care. 42 Although limited evidence exists on guided imagery in childbirth, it has been shown to reduce anxiety in other clinical populations. 43 Music interventions have also been associated with reduced stress and an improved sense of control during labor. 44 In contrast to expectations, the findings of the present study did not demonstrate a reduction in anxiety levels. Post-test anxiety scores were significantly higher in the music-only group compared to both the guided imagery with music group and the control group. These findings suggest that the interventions used in this study were not effective in reducing state anxiety during labor. This result is consistent with previous research on labor dance interventions, which reported reductions in pain and improvements in maternal satisfaction but no significant effects on anxiety. 36 However, the hypotheses that guided imagery combined with music (H1b) and music alone (H1e) would reduce anxiety were not supported by the findings of this study. The lack of effect on anxiety may be explained by the complex and multifactorial nature of childbirth-related anxiety, which may not be adequately addressed by single-modality or primarily sensory-based interventions. Therefore, while guided imagery and music may contribute to certain aspects of the childbirth experience, they may not be sufficient as standalone strategies for managing perinatal anxiety. Although post hoc analyses suggested adequate statistical power to detect the observed anxiety outcomes, smaller but potentially clinically meaningful effects may still have remained undetected. Therefore, further research using more comprehensive or multimodal interventions and larger sample sizes is needed to better evaluate strategies targeting anxiety during labor.
The effect of guided imagery and music intervention on birth experience
Childbirth is a significant event in women’s lives, and their experiences during labor can influence both maternal well-being and family dynamics. 45 Women who perceive labor pain as a natural part of childbirth may develop a more positive outlook on the process. 46 Previous research has shown that environmental factors such as safety, comfort, and a calm atmosphere contribute to a more positive birth experience. 47 Negative childbirth experiences, on the other hand, may lead to fear of future births and postpartum psychological distress.48,49 Supportive care and minimal intervention have been associated with improved maternal satisfaction and overall birth experience. 50 While evidence on guided imagery and birth experience during labor is limited, music-based interventions have been associated with improvements in maternal satisfaction. 37 In the present study, a significant difference in birth experience scores (CEES-II) was observed between groups; however, the effect size was small. Pairwise comparisons indicated that the music-only group reported higher birth experience scores compared to the control group. These findings suggest that music-based interventions may have a modest positive effect on birth experience. Although a statistically significant difference was observed, the small effect size indicates that the intervention had a limited impact on birth experience. Regarding birth experience, the hypothesis related to music-only intervention (H1f) was partially supported, whereas the hypothesis related to guided imagery combined with music (H1c) was not supported. Further research is needed to clarify the role of nonpharmacological interventions in shaping the childbirth experience.
Strengths and limitations of the study
This study has some strengths as well as limitations. One of its main strengths is the use of a random group assignment method, which minimizes selection bias and enhances the internal validity of the findings. The study also used valid and reliable measurement tools, such as VAS, STAI, and CEES, which are widely used to assess labor pain, anxiety, and the birth experience. Furthermore, the intervention content (guided imagery and music intervention recordings) was developed through expert consultation and pilot tested for clarity and feasibility, thereby enhancing the robustness of the intervention design. Another strength is the structured timing of measurements at different stages of cervical dilation, which allowed for a more precise assessment of changes throughout labor.
However, certain limitations should also be acknowledged. The study sample was drawn from a single hospital, which may limit the generalizability of the findings to other birth care settings. In addition, the data were obtained from self-reported measures, which may be subject to subjective interpretation. Furthermore, environmental factors such as single-room birth settings, routine care practices, and differences in staff-patient communication could not be fully standardized across participants.
Another limitation is that participants’ baseline anxiety and pain levels immediately prior to the first intervention could not be assessed beyond the standard tools used at predefined stages of dilation. Labor pain and anxiety are highly subjective and dynamic experiences that can fluctuate rapidly and potentially affect the effectiveness of interventions. Although routine clinical assessments of maternal health were performed and all women received standard intrapartum care, individual differences in emotional and physiological responses may have influenced the results. These factors should be considered when interpreting the study results. Although outcome assessors and the statistician were blinded, participants were not blinded to group allocation, which may have introduced performance bias. Although anxiety was defined as a primary outcome, the sample size calculation was not based on this variable. A post hoc power analysis for the anxiety outcome (STAI-TX) was conducted using the observed effect size (f = 1.06), α = 0.05, a total sample size of 123, three groups, and two repeated measurements. The achieved statistical power was 1.00. However, although the study demonstrated adequate power to detect the observed large effect, caution is still warranted when interpreting anxiety outcomes, as smaller but potentially clinically meaningful differences may not have been fully detected. An additional limitation of this study is the absence of a guided imagery-only group. Therefore, it is not possible to determine whether the observed effects were related to guided imagery, music, or the combined intervention. Accordingly, the findings should be interpreted cautiously, and no conclusions can be drawn regarding the independent effects of guided imagery or music. Future studies incorporating a guided imagery-only group and a four-arm design are recommended to better clarify the specific contributions of each intervention component.
Conclusion
This study suggests that guided imagery combined with music was associated with a reduction in labor pain among primiparous women. In contrast, the interventions did not lead to improvements in anxiety levels, and the effects on birth experience were limited. These findings suggest that while nonpharmacological interventions such as guided imagery and music may support certain aspects of the childbirth experience, their impact may not be consistent across all psychological outcomes. Therefore, additional or complementary strategies may be required to effectively address perinatal anxiety. Future research using more comprehensive designs, including separate intervention arms and larger sample sizes, is needed to better understand the independent and combined effects of these approaches.
Authors’ Contributions
B.U.: Conceptualization, methodology, software, supervision, original draft writing, review and editing writing, funding acquisition, and project management; T.Y.: Conceptualization, methodology, formal analysis, supervision, and review and editing writing; N.S.: Research, data collection, methodology, formal analysis support, and review and editing; and M.K.D.: Conceptualization, formal analysis, and review and editing.
Author Agreement
This article is the authors’ original work. It has not been previously published and is not under consideration for publication elsewhere. All authors have read and approved the final article and agree to be accountable for all aspects of the work.
Ethics Statement
The study protocol was reviewed and approved by the relevant institutional ethics committee (H.S.U. Istanbul Training and Research Hospital Clinical Research Ethics Committee and approval no. 362; approval date: 11.25.2022). Institutional permission was obtained prior to data collection to conduct the research in the study setting.
Consent
Written informed consent was obtained from all participants before they were included in the study.
Footnotes
Data Availability Statement
The datasets created and analyzed during the current study can be obtained from the corresponding author upon reasonable request. The data are not publicly available due to confidentiality and ethical restrictions that protect the privacy of participants.
Acknowledgment
The authors would like to thank the pregnant women who voluntarily agreed to participate in this study and the clinical staff who facilitated the data collection process in the delivery unit. We are also grateful to our colleagues and mentors who provided methodological and statistical guidance throughout the project.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the TÜBİTAK-2209 (acceptance number:
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.