
Abstract
Introduction:
Breast biopsies often cause anxiety and pain that influence patients’ experience and procedure outcomes. Music interventions offer a practical alternative to pharmacological methods for reducing these effects.
Methods:
We conducted a PRISMA-compliant systematic review and meta-analysis to evaluate the efficacy of music during breast biopsies. We searched PubMed, Cochrane CENTRAL Library, EMBASE, and ClinicalTrials.gov up to May 2025. We included randomized controlled trials (RCTs) comparing music interventions with routine care without music intervention. The primary outcomes were anxiety and pain scores; secondary outcomes assessed changes in these scores before and after the procedure. We calculated standardized mean differences (SMDs) with 95% confidence intervals (CIs) using a random-effects model.
Results:
Seven RCTs with 606 participants met the inclusion criteria. The mean age of participants was 50.8 years. Anxiety scores were significantly lower in the music group compared with controls (SMD = –0.22, 95% CI: –0.38 to –0.06, p < 0.05, I2 = 0%). Anxiety reduction from pre- to postprocedure was also greater with music (SMD = 0.25, 95% CI: 0.07–0.44, p < 0.05, I2 = 0%). However, pain scores did not differ significantly (SMD = –0.33, 95% CI: –0.83 to 0.17, p > 0.05, I2 = 82%).
Conclusion:
Music interventions were associated with a small but statistically significant reduction in anxiety during breast biopsy procedures, but no significant reduction in pain. These findings support music as a safe, nonpharmacological option to improve patient experience, particularly with respect to procedural anxiety.
Introduction
Breast biopsy is an essential procedure for diagnosing breast lesions, to the extent that approximately 1.6 million breast biopsies have been performed in the United States alone. 1 Although such microsurgical practices do not cause significant harm, they often bring considerable pain and suffering to the patient. 2 Anxiety related to breast biopsy procedures is attributed to reasons like fear of cancer, fear of suffering, lack of knowledge about what to expect, and uncertainty regarding procedural outcomes. 3 This fear can translate to an increased pain experience level, a low compliance rate to procedures followed, and detrimental and prolonged mental repercussions. 4
The traditional ways of managing anxiety and pain when carrying out a breast biopsy procedure include the use of pharmacological drugs like a local anesthetic, an anxiolytic, and an analgesic. 5 Such pharmacological techniques, however, may be associated with side effects, contraindications, and cost-effective health spending. 6 Moreover, as the tendency toward a patient-centric, more holistic approach to health care is currently on the rise, all nonpharmaceutical alternatives that can be applied as supplements to more traditional medical practices have also gained popularity. 7
The practice of utilizing music therapy has proved to be a potential nonpharmacological treatment mechanism to curb anxiety and pain in several medical contexts.8,9 The neurophysiological, psychological, and social processes provide the theoretical basis for music’s multifaceted therapeutic effect. 10 Neurophysiologically, the parasympathetic nervous system is activated when an individual listens to music, resulting in a decline in blood pressure, heart rate, and cortisol levels. 11 Melzack’s theory postulates that the experience of pain can be altered through music, which can outcompete a nociceptive stimulus’s access to a neural pathway. 12 In addition, music brings cognitive complexity, allowing for less attention to be paid to anxiety-arousing stimuli and pain signals. 13
Individual studies have evaluated the effectiveness of music intervention during breast biopsy procedures with varied findings in relation to the effect on anxiety and pain.14–20 These studies used heterogeneous music-inclusive interventions, including patient-chosen music, researcher-chosen music, live music, recorded music, and, in some cases, music combined with meditation or hypnosis, which makes it challenging to draw conclusions about a single standardized music protocol. 21 In addition, the variation in types of outcome measures, study populations, and intervention protocols across studies requires a methodical integration of all available evidence.
Ashour et al. 22 proposed a meta-analysis on the effectiveness of music in alleviating biopsy procedure-related anxiety and pain. Despite the informative nature of this review, it is necessary to conduct a more detailed review due to the dynamic character of the studies on music therapy and the appearance of new publications. In addition, recent high-quality randomized controlled trials (RCTs) can be combined and present more confident evidence that will help in making informed decisions in clinical settings.
The current systematic review and meta-analysis will be a comprehensive study aiming to identify the efficacy of music as an anxiety and pain alleviating tool during breast biopsies. The synthesis of evidence from RCTs may help inform supportive care practices and guide future research on the role of music interventions during breast biopsy procedures. The findings may provide useful insights into current evidence gaps and highlight priorities for future research in this important area of supportive care.
Methodology
Study design
We report our study according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 23 The review protocol was registered with PROSPERO (CRD420261282836). In this meta-analysis, we determined the effectiveness of the music intervention in reducing the level of anxiety and pain among the women who underwent a biopsy of the breast by pooling the RCTs conducted. Complete PICO is mentioned in the Supplementary Data (Supplementary Table S2).
Search strategy
The study systematically searched the following databases: Cochrane CENTRAL Library, PubMed, EMBASE, and ClinicalTrials.gov, covering the period till May 2025. The strategy employed in the search consisted of free-text words and medical subject headings related to breast biopsy interventions and the use of music interventions. The keywords include the following concepts and their synonyms, namely, Breast Biopsy, Breast, Biopsy, Core needle biopsy, Pain, Anxiety, Music, Fine needle aspiration, Music therapy, Symphony, Rhythm, and Melody. The use of Boolean operators (AND/OR) allowed combining these search terms into detailed search strings, which were designed specifically for each database. Refer to the Supplementary Data for the complete search string (Supplementary Table S1).
Moreover, the included papers were searched thoroughly, including their references, to identify possible eligible studies. We further conducted searches of conference proceedings to identify unpublished research or trials underway.
Eligibility criteria
Inclusion criteria
Women of any clinical background who were scheduled for breast biopsy procedures were considered eligible for inclusion. The intervention arm comprised various forms of music exposure delivered during the biopsy, which could involve live performances, prerecorded tracks, or selections chosen either by the patient or the investigators. Comparator groups consisted of participants who received routine clinical care without music, whether in the form of standard practice or no additional intervention. Primary outcomes included anxiety and/or pain measurements. Study design was an RCT. Sufficient data were available for meta-analysis.
Exclusion criteria
Publications that were not published in English. Nonrandomized clinical trials. Editorials, commentaries, reviews, or opinion pieces. Animal studies. Case reports or case series. Conference abstracts without full-text availability. Studies that did not report sufficient data for outcome extraction. Studies involving participants aged less than 18 years.
Outcomes
Primary outcomes included:
Secondary outcomes included:
Postprocedure anxiety scores and change-in-anxiety scores were treated as distinct outcomes and were not pooled within the same meta-analytic model.
Study selection and data extraction
Article selection was done by two independent reviewers (initials blinded during review). The studies were then searched after removing the duplicates based on the titles and abstracts. The complete text of potentially eligible studies was then obtained and screened against inclusion. In case of a conflict between the reviewers, it was solved by mutual discussion and negotiation. If disagreement persisted, a third reviewer was consulted.
Extraction of the data was performed using Microsoft Excel by three reviewers independently. Data extracted from each of the included studies consisted of the following: first author, publication year, study design, country of origin, sample size, and the characteristics of participants (age, race, education, and marital status). They also extracted the type of breast biopsy procedure used, specific information about the music intervention (type, duration, method of delivery), control group description, outcome measures, and any numerical data needed for meta-analysis.
Quality assessment
To assess methodological rigor, we employed the Cochrane risk-of-bias framework for RCTs, examining domains such as randomization, allocation concealment, and blinding. 24 The evaluation covered the assessment of the production of a random sequence, the allocation concealment, participant and staff masking, outcome blinding, incomplete outcome data, choosing what to report, and other biases.
Each domain was rated as low risk, high risk, or some concerns, as appropriate. Two independent reviewers performed the quality assessment. If there was any discrepancy between them, they resolved it via discussion.
Publication bias
Publication bias was planned to be assessed using funnel plots and Egger’s test. However, because fewer than 10 studies were included, no formal publication bias assessment was performed, consistent with methodological guidance. According to Egger et al., 25 publication bias alone cannot be used in analyzing meta-analyses with fewer than 10 studies, as the results may be biased and misleading.
Certainty of evidence assessment
The certainty of evidence for each pooled outcome was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach. Because all included studies were RCTs, the initial certainty of evidence was considered high and was downgraded when concerns were identified in the domains of risk of bias, inconsistency, indirectness, imprecision, and publication bias. Risk of bias was judged in relation to the Cochrane risk-of-bias assessment, with particular attention to lack of blinding because the main outcomes were subjective patient-reported measures. Inconsistency was assessed using the direction of effect, overlap of confidence intervals (CIs), and I2 statistic. Imprecision was considered when CIs were wide, crossed the line of no effect, or when the total sample size was limited. Indirectness was assessed according to differences in intervention delivery, comparator conditions, biopsy setting, and outcome measurement tools. Publication bias was not formally assessed because fewer than 10 studies were available for each pooled outcome. Two reviewers independently assessed certainty, and disagreements were resolved by discussion.
Statistical analysis
Quantitative synthesis was conducted with Review Manager (RevMan, version 5.3; Cochrane Collaboration, Copenhagen, Denmark), and procedures were aligned with methodological standards outlined in the Cochrane Handbook. 26 We present standardized mean differences (SMDs) with 95% CIs by using the inverted variance technique and random-effects model, when the data are continuous. The reason that SMD was included was that the studies in the review used varied measurement tools to measure similar consequences (i.e., various anxiety scales, such as SAS, STAI, and VAS).
Statistical heterogeneity was examined using both the chi-squared test (Cochrane Q test) and the I2 statistic, with thresholds of p < 0.05 or I2 above 50% interpreted as evidence of meaningful variability between studies. Where a large heterogeneity was observed, the random-effects model with the DerSimonian-Laird estimator was applied since it was assumed that the true effect sizes were a distribution and not a fixed value. For studies reporting baseline and postprocedure anxiety values, change scores were analyzed separately from postprocedure scores. Specifically, preintervention means were subtracted from postintervention means before standardization. This approach reflects a change-score analysis rather than a true ANCOVA adjustment, because individual participant-level baseline adjustment and baseline–follow-up correlation terms were not available. Postprocedure anxiety scores and change-in-anxiety scores were therefore meta-analyzed in separate models and were not combined.
The robustness of pooled estimates was further examined using a leave-one-out sensitivity analysis, whereby each study was sequentially omitted to assess its influence on the overall results.
The statistical level of significance in all analyses was p = 0.05. We have used the effect size guidelines of Cohen: small effect (SMD = 0.2), medium effect (SMD = 0.5), and large effect (SMD = 0.8). 27
Results
Study selection
Two hundred and 30 potentially relevant studies were produced based on the initial search. There were 52 duplicated studies, which were removed, leaving 178 studies to be screened by title and abstract. Based on the title and abstract review, 161 studies were excluded after the primary screening. A full-text review was conducted for 17 articles. Of these, 10 were excluded due to insufficient outcome data (n = 4), lack of randomization (n = 3), different intervention (n = 2), or different population (n = 1). The remaining seven studies met the inclusion criteria and were included in the systematic review and meta-analysis. The whole selection process can be seen in the PRISMA Flow Diagram (Fig. 1).
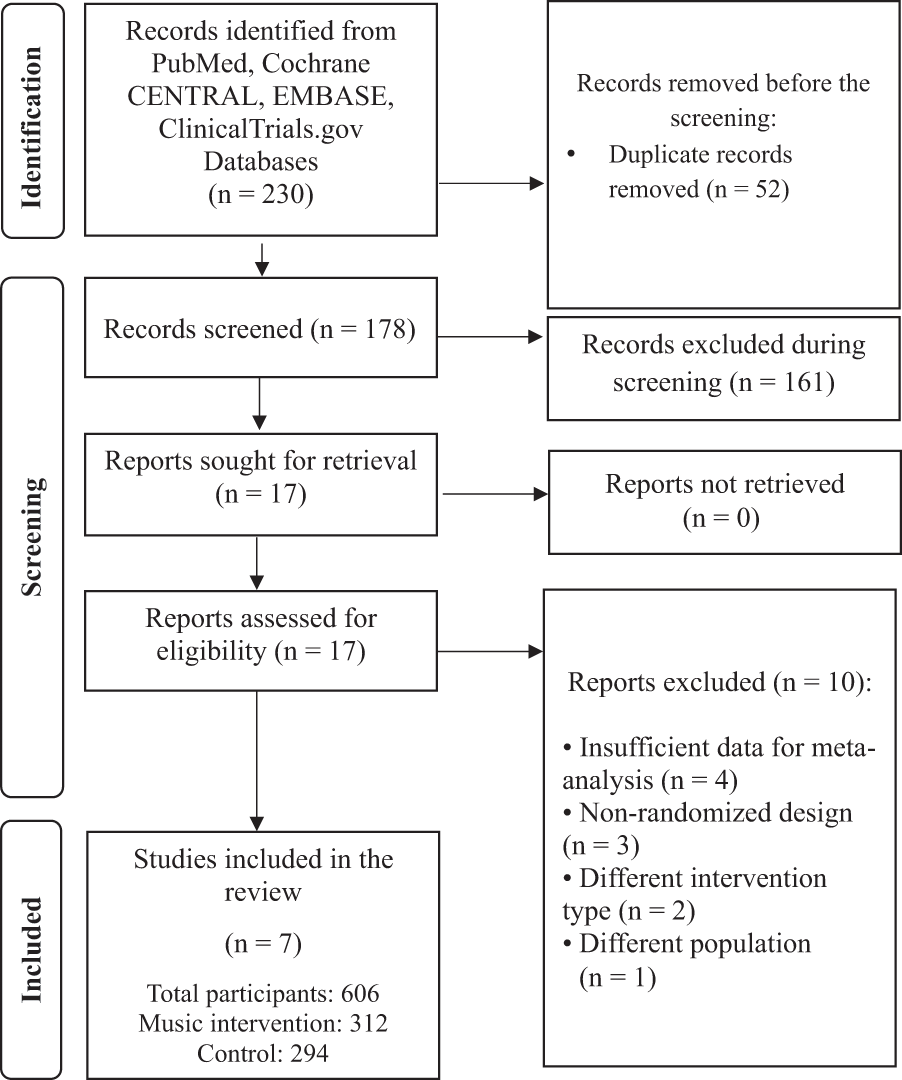
PRISMA flow diagram of the article selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
The included studies were published between 2005 and 2023. Reportedly, Turkey and the United States were the countries where all of these trials were conducted. The overall sample consisted of 606 participants, with a mean age of approximately 50.8 years. The music group had 312 participants, while the control group consisted of 294. The procedures used were core needle biopsy, ultrasound-guided biopsy, and fine needle aspiration. Table 1 shows the traits of the selected studies.
Characteristics of the Included Studies

SAS, Zung Self-Rating Anxiety Scale; STAI, State-Trait Anxiety Inventory; VAS, Visual Analog Scale.
Meta-analysis results
Anxiety scores
All seven studies (n = 606) measured anxiety levels following breast biopsy procedures. The pooled analysis demonstrated a statistically significant reduction in anxiety scores favoring the music intervention group (SMD = −0.22, 95% CI: −0.38 to −0.06, p = 0.008). The heterogeneity among studies was low and nonsignificant (I2 = 0%, p = 0.44), indicating consistency across studies (Fig. 3). The effect size was small according to Cohen’s criteria but statistically significant.
Decrease in anxiety
Five studies (n = 430) reported changes in anxiety scores from pre- to postprocedure. The pooled estimate showed a significantly greater decrease in anxiety in the music intervention group when compared to controls (SMD = 0.25, 95% CI: 0.07–0.44, p = 0.006). No heterogeneity was detected between pooled studies (I2 = 0%, p = 0.85), supporting the consistency of findings across different study populations and settings (Fig. 2).
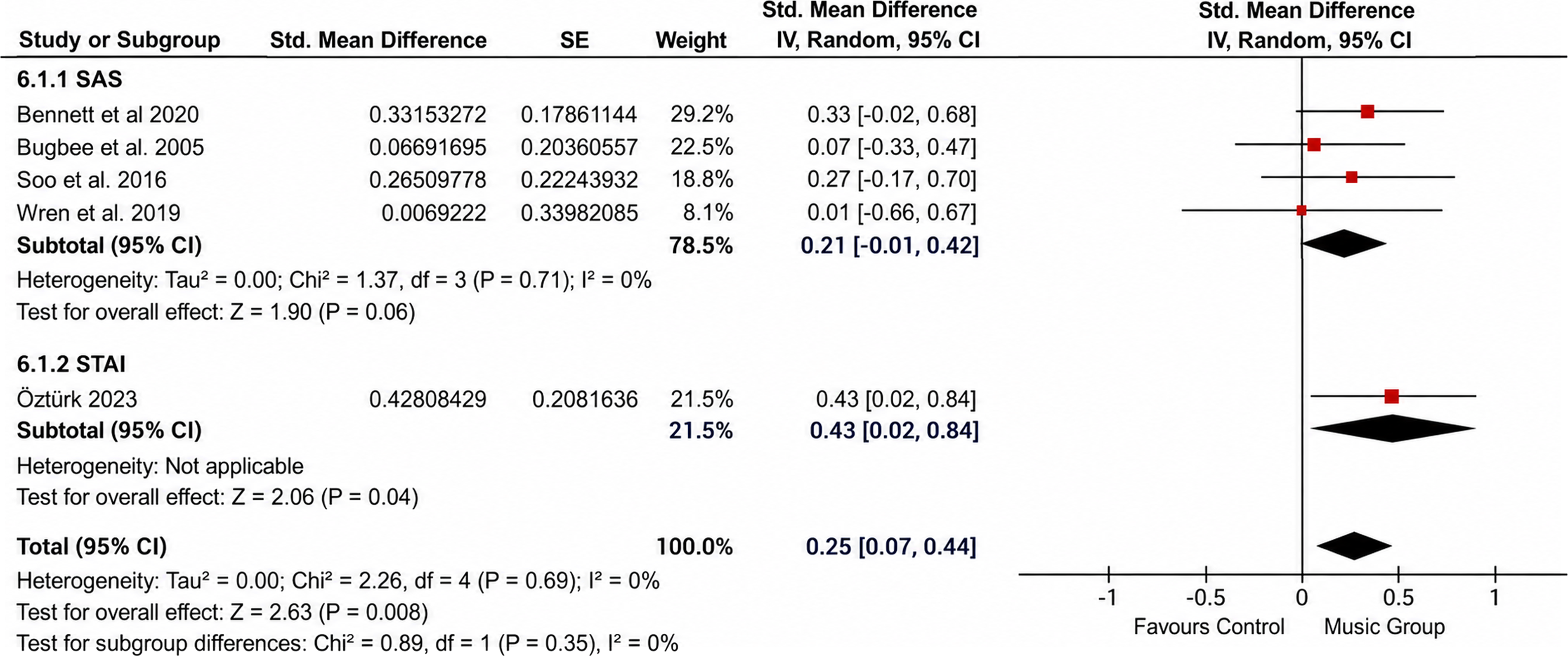
Decrease in anxiety.
Pain scores
Five studies (n = 382) included a VAS score for the level of pain. No statistically significant difference was found between the music intervention and control (SMD = −0.33, 95% CI: −0.83 to 0.17, p = 0.20). Heterogeneity was high (I2 = 82%, p = 0.0001), indicating significant differences among studies in terms of pain outcomes (Fig. 4a).
To investigate the origin of heterogeneity, leave-one-out sensitivity analysis was employed. Excluding the Öztürk 2023 study also lowered the heterogeneity levels to a moderate level (I2 = 50%, p = 0.11), but the overall effect was nonsignificantly changed (SMD = −0.19, 95% CI:−0.48 to 0.09, p = 0.18) (Fig. 4b). The results are summarized in Table 2.
Summary of Meta-Analysis Results
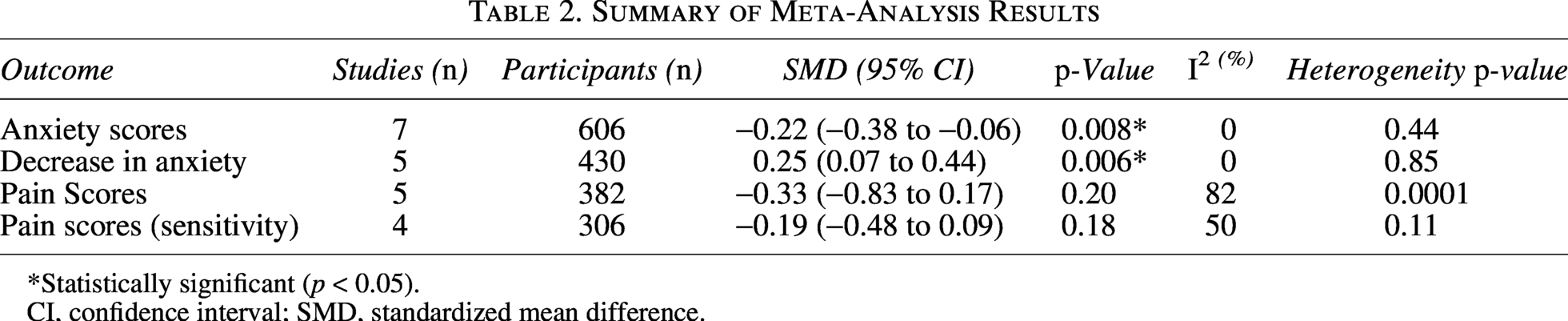
*Statistically significant (p < 0.05).
CI, confidence interval; SMD, standardized mean difference.
Quality assessment
The methodological quality assessment revealed generally acceptable quality across included studies, with some limitations typical of behavioral interventions. All studies demonstrated adequate random sequence generation, with most employing computer-generated randomization. Allocation concealment was adequately maintained in most studies, although some concerns were noted in three studies due to unclear descriptions of concealment procedures. A summary of the quality analysis is shown in Table 3.
Quality Assessment Summary
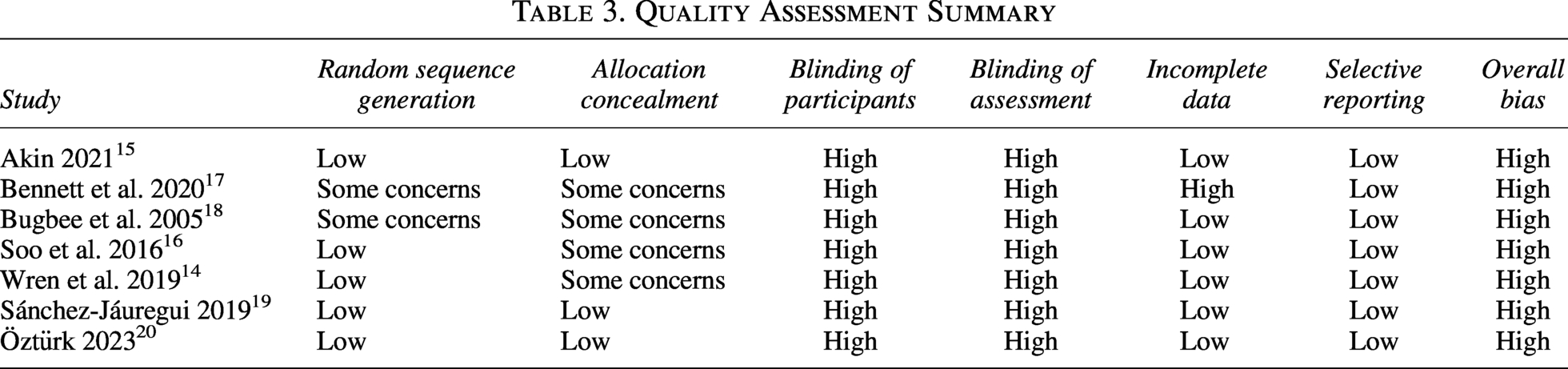
Masking of participants and care staff was rated as high risk in all studies, which is inherent to music intervention studies where participants are aware of receiving music. Similarly, outcome blinding was problematic in most studies, particularly for subjective outcomes like anxiety and pain. However, because anxiety and pain are subjective outcomes, the lack of blinding may have influenced participant-reported effects and should be considered when interpreting the findings.
Incomplete outcome data were adequately addressed in most studies, with appropriate handling of missing data and those participants who chose to drop out. Moreover, the risk of bias was low for selective reporting, with studies reporting all prespecified outcomes. Other potential sources of bias, including baseline imbalances and cointerventions, were adequately controlled in most studies.
Certainty of evidence
Using the GRADE approach, the certainty of evidence was judged as low for anxiety outcomes and very low for pain outcomes. Anxiety outcomes were downgraded primarily for serious risk of bias because the included trials were open-label or nonblinded and relied on subjective self-reported measures such as STAI, SAS, and VAS. For pain outcomes, the certainty was downgraded further because substantial heterogeneity was present in the primary pooled analysis (I2 = 82%), and the pooled CIs crossed the line of no effect. Additional concerns regarding indirectness arose from variability in intervention delivery and trial structure across studies, including differences in whether music was fixed or self-selected and in biopsy settings and outcome assessment methods. Formal assessment of publication bias was not performed because fewer than 10 studies were available per outcome Table 4.
Grading of Recommendations Assessment, Development, and Evaluation Assessment of the Included Outcomes

Forest plots
The forest plot of the mean difference in means between pre- and postprocedure shows the SMD of the change in anxiety scores across five studies.14,16,18–20 In the forest plot, each trial’s effect size is shown as a square, with the square’s area corresponding to its relative weight in the analysis, and horizontal bars denoting the 95% CIs. The overall pooled effect is visualized as a diamond-shaped marker at the bottom of the plot. All the studies report positive results in favor of music intervention, with effect sizes ranging between 0.15 and 0.35. A vertical reference line at zero indicates the point of no effect; CIs positioned to the left or right of this line suggest a potential benefit or lack thereof for the intervention. No heterogeneity was found (I2 = 0%, p = 0.85) (Fig. 2).
The anxiety score forest plot presents the SMDs for postprocedure anxiety scores across all seven included studies. The plot displays individual study results as squares with 95% CIs. Six of the seven studies show effect estimates favoring music intervention (negative values), while one study 18 shows a small positive effect. The effect sizes range from −0.45 to +0.10, with most studies clustering around −0.20 to −0.30. The pooled diamond shows the overall effect (SMD = −0.22, 95% CI: −0.38 to −0.06), indicating a statistically significant reduction in anxiety scores. The consistency in direction across most included studies, together with CIs that do not diverge widely, lends credibility to the stability of the observed effect with wide confidence (I2 = 0%, p = 0.44) (Fig. 3).
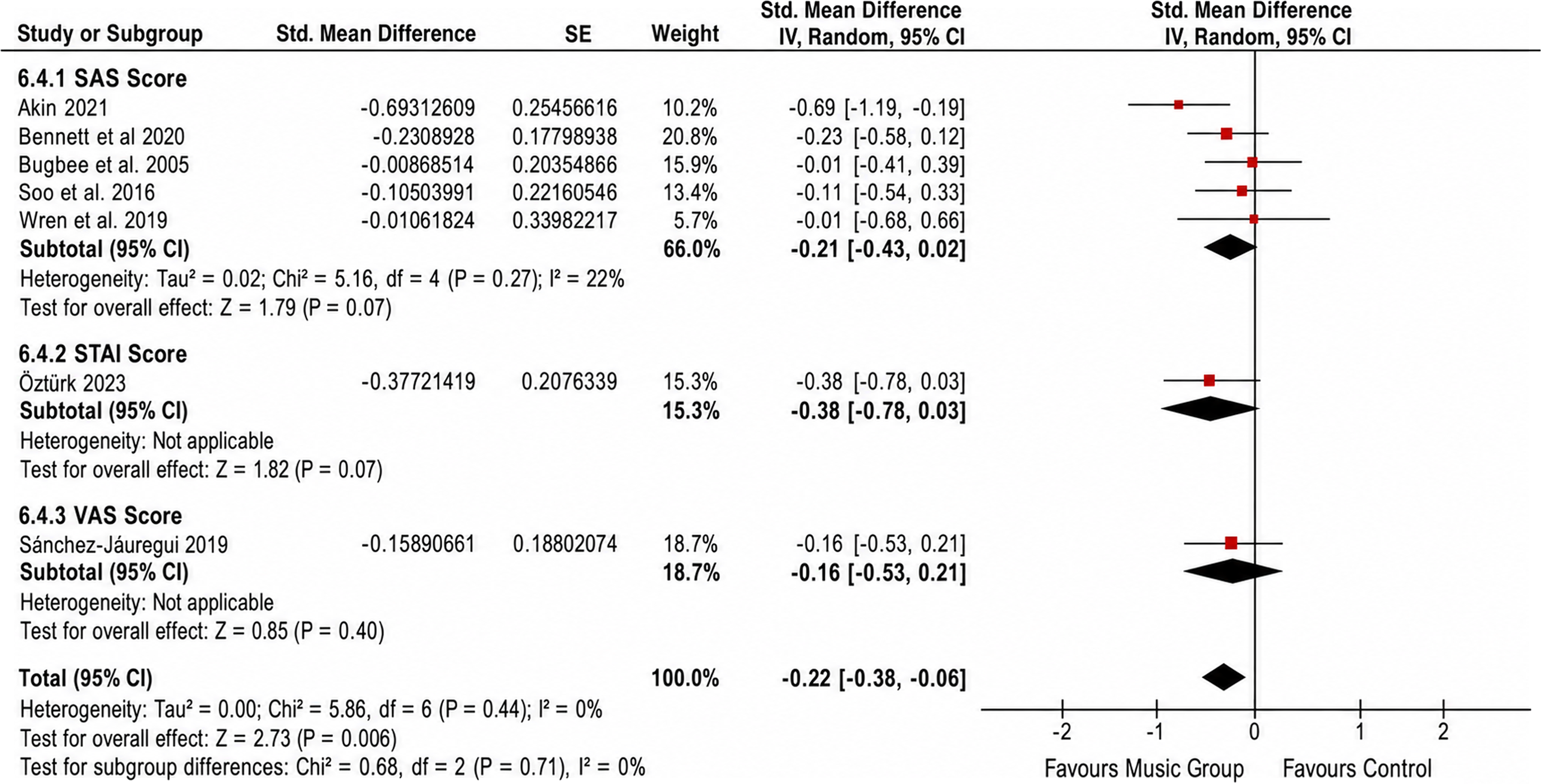
Anxiety scores.
This forest plot illustrates the SMDs for pain scores across five studies.14–16,19,20 The plot reveals considerable variability in effect sizes, ranging from −0.70 to +0.15. Three studies show beneficial effects of music intervention (negative values), while two studies show small harmful effects or no effect. The Öztürk 2023 study appears as a notable outlier with a large beneficial effect (−0.70), while other studies show more modest effects. The pooled diamond crosses the line of no effect (SMD = −0.33, 95% CI: −0.83 to 0.17), indicating no statistically significant difference between groups. The presence of a broad CI in the pooled pain analysis highlights the considerable variability between trials (I2 = 82%, p < 0.001) (Fig. 4a).
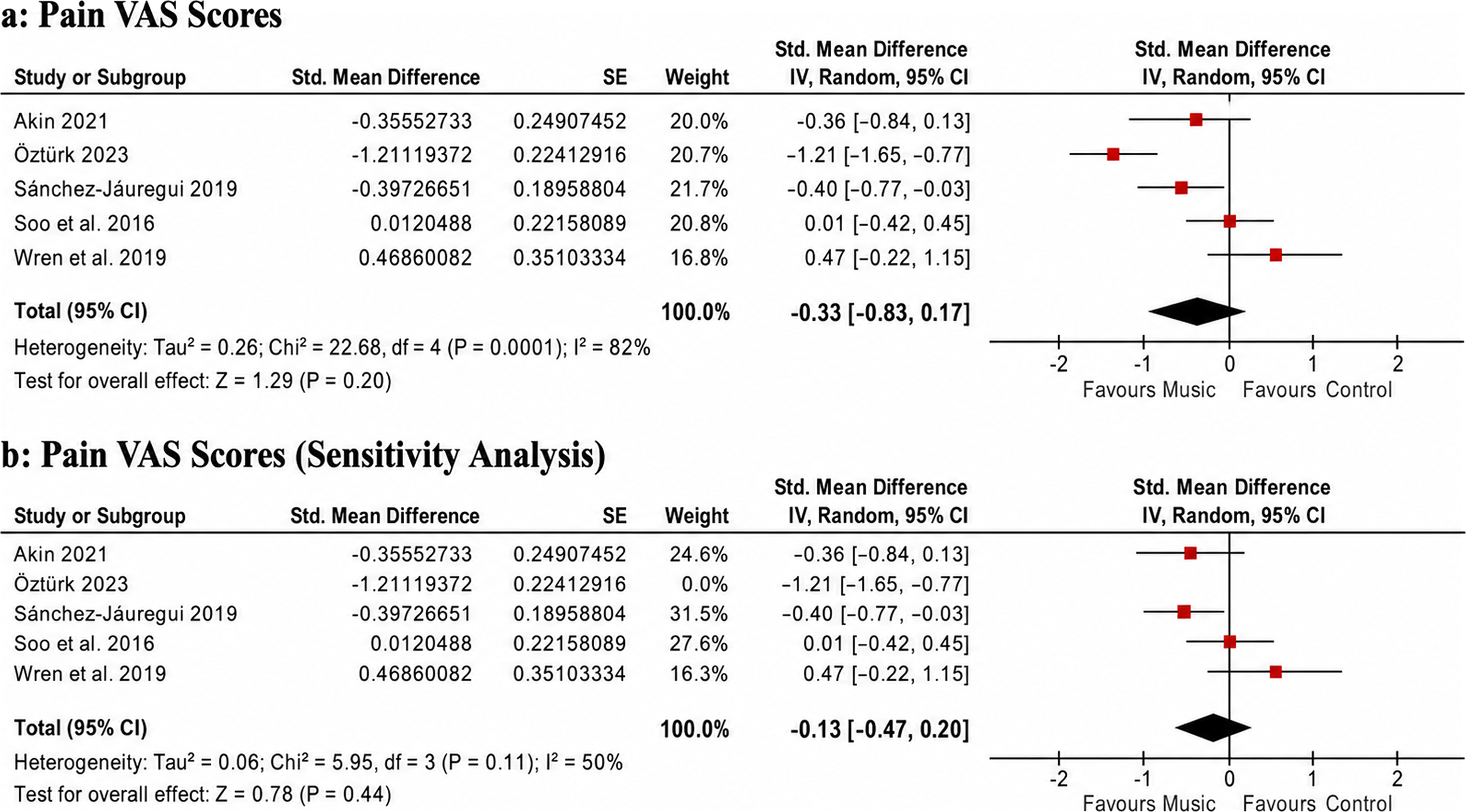
This forest plot shows the results after excluding the Öztürk 2023 study to address the high heterogeneity. The remaining four studies display more consistent effect sizes, ranging from −0.35 to +0.15. After excluding the identified outlier study, the between-study heterogeneity decreased to a moderate level (I2 = 50%, p = 0.11), although some variation persisted across the remaining data. The pooled effect estimate shifted closer to null (SMD = −0.19, 95% CI: −0.48 to 0.09) but remained nonsignificant. The sensitivity analysis confirms that the heterogeneity was largely driven by the Öztürk study, but the overall conclusion regarding pain outcomes remains unchanged, with no statistically significant benefit of music intervention for pain reduction (Fig. 4b).
Subgroup analysis
Given the limited number of studies, formal subgroup analyses were not feasible. However, descriptive analysis revealed that studies using patient-selected music15,20 showed consistent anxiety reduction effects, while studies combining music with other interventions (meditation, hypnosis) also demonstrated positive outcomes. The heterogeneity in pain outcomes appeared to be related to differences in biopsy procedures, pain assessment timing, and baseline pain levels across studies.
Discussion
Our study summarizes and synthesizes the available high-quality evidence depicting the effect of musical interventions on pain and anxiety scores during breast biopsy procedures. Compared with standard care, music-inclusive interventions were associated with a small but statistically significant reduction in postprocedure anxiety and a greater reduction in pre- to postprocedure anxiety change scores. In contrast, no significant benefit was observed for pain outcomes, and pain findings showed substantial heterogeneity across studies. These findings should be interpreted in light of the open-label nature of the included trials. Because participants and personnel could not be blinded to music exposure, and because anxiety and pain were self-reported outcomes, the pooled estimates may be influenced by performance bias, expectancy effects, or detection bias. This concern does not invalidate the observed anxiety reduction, but it lowers confidence in the magnitude of the effect.
The small but statistically significant reduction in postprocedure anxiety (SMD = −0.22) and the greater reduction in change-in-anxiety scores (SMD = 0.25) support a modest anxiolytic effect of music during breast biopsy procedures. These results are in agreement with those of past studies that show that music has anxiety-reduction effects in most health care environments.28,29 The dynamics of these effects are complex, as they involve both psychological and physiological aspects.
From a psychological standpoint, musical engagement can divert cognitive resources, thereby reducing the patient’s focus on procedure-related fears or discomfort. This redirection of attention diminishes the salience of anxiety-inducing cues. 30 The cognitive load theory suggests that music occupies cognitive resources that would otherwise be available for processing anxiety-related information. 31 In addition, music can evoke positive emotions and memories, counteracting the negative emotional state associated with medical procedures. 32 From a psychiatric perspective, procedural anxiety during breast biopsy can be understood as an acute stress response characterized by anticipatory fear, heightened arousal, and affective dysregulation. In this context, music may exert its benefits through emotion regulation, attentional redirection, and modulation of affective processing networks, thereby reducing the psychological burden of the procedure even when its effect on pain is less consistent.
On a biological level, exposure to music activates parasympathetic pathways, which are associated with relaxation responses such as lower circulating cortisol, reduced cardiac activity, and stabilization of blood pressure. 33 Collectively, these physiological shifts counteract the heightened arousal typical of the stress response, helping to create a more stable internal state during invasive procedures. In addition, experimental findings further suggest that music modulates neurochemical processes, enhancing dopamine release, supporting serotonin balance, and dampening sympathetic mediators like norepinephrine and epinephrine. 34
The consistency of anxiety reduction across studies (I2 = 0%) supports a reproducible direction of effect, although confidence in the magnitude of benefit remains limited by lack of blinding and reliance on subjective outcomes. This low heterogeneity suggests that the benefits of music interventions are robust and generalizable across different demographic groups and clinical contexts. Although the effect size was small according to Cohen’s criteria, its clinical meaning should be interpreted cautiously. The use of SMD not only allowed pooling across different anxiety instruments, but it also reduced direct clinical interpretability because the pooled estimate is not expressed in the original units of any single scale. In addition, a minimal clinically important difference was not consistently available across the included anxiety measures. Therefore, the anxiety findings should be interpreted as evidence of a small average reduction in patient-reported anxiety rather than definitive evidence of a clinically meaningful improvement. However, given the low cost, safety, and feasibility of music interventions, even a small effect may still be useful as an adjunctive supportive measure for selected patients, particularly those with high preprocedural anxiety.
The nonsignificant effect of music on pain with substantial heterogeneity (I2 = 82%) presents a more complex picture. This finding contrasts with some individual studies that have reported pain-reducing effects of music in various medical procedures.35,36 Several factors may explain this discrepancy.
First, the timing of pain assessment may be crucial. Pain during breast biopsy procedures is typically brief and procedure-specific. This makes it complex and challenging to identify the full impact of music interventions. Some studies assessed pain immediately after the procedure, while others measured it during specific procedural steps, leading to inconsistent findings. 37
Second, the heterogeneity in pain outcomes may reflect differences in procedural and contextual factors across studies. These may include the type and dose of local anesthesia used, timing of pain assessment, whether music was patient-selected or researcher-selected, and broader cultural differences in pain reporting across study populations, particularly between studies from the United States and Turkey. Such factors may have contributed to the substantial variability observed in the pooled pain analysis. Within the framework of Melzack’s gate control theory, the soothing effect of music is thought to arise from its ability to compete with nociceptive signals, thereby reducing the extent to which painful stimuli gain access to higher-order processing. 38
Third, breast biopsy procedures include types and levels of pain that are not necessarily well-suited to music interventions. Although music has proven effective in alleviating chronic or procedure-related pain in other settings, it is conceivable that localized, acute pain, such as biopsy pain, requires a more targeted approach. 39
The sensitivity analysis excluding the study by Öztürk 20 lowered heterogeneity without altering the absence of a significant effect, indicating that differences in methods, rather than a single study, cause the inconsistency in pain findings. This highlights the need for more standardized methods in pain assessments and intervention delivery in future studies.
The results of this meta-analysis may have practical implications for health care providers and health care systems. First, the consistent reduction in anxiety suggests that music may be considered as an optional supportive adjunct during breast biopsy procedures. Music interventions are low-cost, low-risk, and relatively simple to implement. With no negative outcomes, they have become a significant addition that can enhance the overall patient experience.
Music interventions may be considered as part of supportive preparation before medical procedures, particularly for patients with high procedural anxiety. 40 Music interventions are flexible and can be customized to suit individual preferences or needs; thus, patients can choose the music of their preference or a genre that best aligns with their personal tastes and cultural background.
In terms of a health care system, music intervention may result in improved patient satisfaction scores, reduced use of anxiolytic drugs, and higher overall quality of care. 41 The low cost of music interventions, combined with their positive impact on patient experience, is also a reason why such interventions can be attractive to health care organizations eager to enhance their patient-centered care.
The low levels of pain reduction, however, point to the fact that music interventions cannot be seen as alternatives to conventional pain treatments. It is recommended that the reduction of anxiety through the employment of local anesthesia and other methods of pain management be practiced by health care professionals, but at the same time, it must be used in combination with the employment of music in reducing anxiety.
Several methodological considerations emerge from this analysis that have implications for future research and clinical implementation. The inherent difficulty in masking the participants and staff in music intervention represents a fundamental limitation that cannot be entirely overcome. However, this limitation remains important, particularly because the main outcomes in this review were subjective and may therefore be more susceptible to performance and detection bias.
The diversity of interventions across studies, including music alone as well as music combined with meditation or hypnosis, reflects the complexity of this field and should be acknowledged as an important limitation. Accordingly, the pooled findings may best be interpreted as the average effect of music-inclusive interventions rather than a single standardized music protocol. While this diversity may contribute to heterogeneity, it also demonstrates the flexibility and adaptability of music interventions to different clinical contexts and patient populations. Accordingly, the present findings should be interpreted as reflecting music-inclusive interventions rather than a single standardized music therapy protocol.
The use of different anxiety and pain assessment tools across studies, while necessitating the use of SMDs, may have introduced additional variability in outcomes. Future research would benefit from greater standardization of outcome measures to improve comparability across studies. Although the use of SMDs allowed pooling across different instruments, this approach may reduce direct clinical interpretability compared with absolute mean differences.
Our study had some inherent limitations, which are as follows: First, only seven studies could be included, and the total number of study participants was 606 people, which can lead to a lack of generalizability. Further studies are required, specifically focusing on larger cohorts, to strengthen the evidence bank. Second, the variability of music intervention types, mode of delivery, and time means that it is hard to identify the most suitable form of music therapy during breast biopsy. In future studies, the emphasis should be placed on standardizing the intervention protocol to make it more comparable and applicable in clinical practice. Third, although major biomedical databases and ClinicalTrials.gov were searched, we did not search all regional databases, dissertation repositories, non-English databases, or broader gray-literature sources. In addition, non-English full-text articles were excluded. Therefore, relevant unpublished, regional, or non-English trials may have been missed, and some degree of language or publication bias cannot be excluded. Fourth, the failure to account for publication bias due to insufficient studies is a weakness. Although we attempted to include unpublished studies in multiple ways, we cannot completely eliminate the possibility of publication bias. Fifth, the narrowed target group of women undergoing breast biopsy procedures cannot elicit universality of research results to different patient groups or situations. However, at the same time, this kind of specificity enhances the clinical applicability of the findings for a specific population of interest. Finally, although the protocol was registered with PROSPERO, registration was retrospective; therefore, the possibility of protocol-stage deviations before registration cannot be fully excluded.
Future research shall look into the following areas: Larger RCT studies with uniform guidelines of the intervention are required to give more conclusive evidence. They are to design their studies such that the same outcome measurement and assessment timings are used to enhance comparisons. Second, existing research should be utilized to establish the ideal music intervention properties, such as music type, duration, administration mode, and timing. Comparative effectiveness studies of alternative music methods can provide evidence-based guidelines for clinical practice. Third, research into the influence of personal factors, such as music preference, anxiety levels at baseline, or cultural background, on the effectiveness of music interventions could potentially help determine which patients will benefit most from such interventions. Fourth, assessing the cost-effectiveness of music intervention in the breast biopsy setting would be very useful. This information will help health administrators decide whether to adopt the intervention. Lastly, studies on the long-term consequences of the music intervention on patient satisfaction, procedural compliance, and psychological well-being may yield insight into the general effects of these interventions beyond the immediate outcomes related to anxiety and pain.
Conclusion
The findings of this meta-analysis support further evaluation of patient-centered supportive approaches that address psychological as well as procedural aspects of care. Music interventions may improve patient experience during breast biopsy procedures, although further high-quality studies are needed before broader conclusions can be made.
This systematic review and meta-analysis suggest that music-inclusive interventions may produce a small reduction in anxiety during breast biopsy procedures. However, the certainty of evidence for anxiety outcomes was low, mainly because the included trials were open-label and relied on subjective patient-reported measures. Therefore, the findings should be interpreted as supportive but not definitive evidence of benefit. Similarly, evidence for pain reduction was weaker, statistically insignificant, had substantial heterogeneity, and showed very low certainty of evidence. Music interventions should therefore not be considered a replacement for standard analgesic or procedural pain-management strategies. Given their low cost, safety, and feasibility, music interventions may be considered as optional adjunctive supportive measures, particularly for patients with elevated preprocedural anxiety. Larger, well-designed randomized trials using standardized intervention protocols, consistent outcome measures, and clearer blinding or bias-reduction strategies are needed before stronger clinical conclusions can be made.
Data Availability
Data from the studies included are publicly available on the above-mentioned databases.
Authors’ Contributions
Y.C. and H.Y. conceived and designed the study. H.Q.U.A., I.J., A.H.B.G., and M.U. contributed to the literature search, study screening, eligibility assessment, and data extraction. H.Q.U.A., I.J., A.H.B.G., and D.K. contributed to data verification, quality assessment, and risk-of-bias evaluation. Y.C., H.Y., and D.K. contributed to statistical analysis, interpretation of findings, and preparation of tables and figures. Y.C. drafted the initial manuscript. H.Q.U.A., I.J., A.H.B.G., M.U., H.Y., and D.K. critically reviewed and revised the manuscript for important intellectual content. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-cpm-10.1177_27683605261461167 — Supplemental material for Music Intervention for Anxiety and Pain During Breast Biopsy Procedures: A Comprehensive Systematic Review and Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-cpm-10.1177_27683605261461167 for Music Intervention for Anxiety and Pain During Breast Biopsy Procedures: A Comprehensive Systematic Review and Meta-Analysis of Randomized Controlled Trials by Yao Chen, Hafiza Qurat Ul Ain, Inshal Jawed, Abu Huraira Bin Gulzar, Muhammad Umair, Hermann Yokolo, and Danaish Kumar
Footnotes
Author Disclosure Statement
There was no conflict of interest among the authors.
Funding Information
The study did not receive any kind of funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.