
Abstract
Background:
Ayurvedic dravya-based herbal products are increasingly studied for cognition, stress, sleep, and psychiatric symptoms, but synthesis is complicated by heterogeneous preparations, incomplete reporting of Rasapanchaka-relevant attributes, and ambiguous common-name labels.
Objectives:
To synthesize controlled human evidence on dravya-based herbal products for (A) cognition, (B) stress, sleep, and related well-being outcomes, and (C) psychiatric symptoms/disorders using a node-resolved framework.
Methods:
We conducted a PRISMA 2020-reported, node-resolved systematic review of controlled human studies evaluating a defined dravya node and at least one standardized mental-health instrument or cognitive test. PubMed/MEDLINE, the AYUSH Research Portal, and DHARA were searched from database inception to 4 January 2026; the evidence base was frozen on January 30, 2026, after deduplication, full-text retrieval, and manual reference-list screening. Interventions were mapped to node identifiers using botanical identity, part/material, and preparation; identity-uncertain labels were retained as separate strata.
Results:
Forty-nine controlled reports spanning 20 nodes were included. Evidence volume was concentrated in Bacopa monnieri (Brahmi) for cognition and Withania somnifera (Ashwagandha) for stress and sleep outcomes. Meta-analysis was feasible for three primary strata: W. somnifera (Ashwagandha) versus placebo on perceived stress and sleep quality, and curcumin versus placebo on depression severity. Reported adverse events were usually mild but inconsistently captured.
Conclusions:
Selected dravya nodes show potentially beneficial signals, but confidence in effect magnitude remains limited by heterogeneity, small-study effects, and reporting quality.
Introduction
Cognition, stress, sleep, and psychiatric symptoms exist on a continuum relevant to both prevention and treatment. Mental disorders remain a major contributor to disability worldwide, and substantial care gaps persist because of access barriers, stigma, delayed help-seeking, and incomplete treatment response.1–3 Interest in complementary and integrative interventions has therefore increased, particularly for agents that are positioned for stress resilience, sleep, cognitive support, or adjunctive symptom management.
Ayurveda includes a large pharmacopeia of dravya-based substances and longstanding concepts of mind-supporting interventions, including Medhya Rasayana. 4 Classical dravya selection is traditionally interpreted through Rasapanchaka (rasa, guna, virya, vipaka, and prabhava), yet most contemporary controlled trials do not operationalize these attributes explicitly. Instead, modern studies evaluate selected dravya-based herbal products using standardized instruments for cognition, perceived stress, sleep quality, mood, and related outcomes.
Reliable synthesis is complicated by heterogeneity in plant part, extract standardization, dose, comparator, and endpoint selection. A second major challenge is ambiguous common-name reporting. Labels such as Shankhapushpi can refer to multiple botanicals; therefore, pooling across nonequivalent species or preparations can distort both evidence mapping and meta-analysis. We therefore retained identity-uncertain labels as separate strata rather than merging them with resolved botanical nodes.
Accordingly, we undertook a node-resolved systematic review and meta-analysis in which each intervention was anchored to a resolved botanical node identifier. In this framework, a node represents the intervention identity at the level of species, plant/material part, and preparation or standardization status, while identity-uncertain labels are retained as separate strata. This approach was used to clarify where replicated human evidence exists, where it remains sparse, and how Dravyaguna evidence maps onto contemporary mental-health outcomes.
Aims and objectives
Aim
To synthesize controlled human evidence on Ayurvedic dravya-based herbal medicinal products for (A) cognition, (B) stress, sleep, and related well-being outcomes, and (C) psychiatric symptoms/disorders using a node-resolved framework.
Objectives
(1) To identify and characterize eligible controlled studies; (2) map evidence volume by node and domain; (3) narratively summarize efficacy and descriptive safety signals by domain; and (4) perform node-resolved meta-analyses where endpoint and preparation strata permit.
Methods
Protocol and reporting
The review followed PRISMA 2020 as a reporting framework. 5 An a priori working protocol was prepared before screening; however, prospective external registration was not completed. Any protocol refinements made during revision are documented in the Supplementary Data.
Information sources and primary search strategy
PubMed/MEDLINE, the AYUSH Research Portal, and DHARA were searched from database inception to January 4, 2026. The evidence base was frozen on January 30, 2026, after deduplication, retrieval of eligible full texts, and manual screening of reference lists from PRISMA-retrieved articles. The strategy combined dravya/common-name terms and botanical names with mental-health terms covering cognition, memory, attention, perceived stress, sleep, anxiety, depression, and psychiatric symptoms. Full electronic search strings and portal-adapted searches are provided in Supplementary Data S1.
Eligibility criteria
We included controlled human studies (randomized controlled trials [RCTs], quasirandomized trials, controlled nonrandomized studies, and controlled observational designs) evaluating a single dravya or clearly specified herbal medicinal product and reporting at least one standardized mental-health instrument or cognitive test outcome. In a small number of older reports, comparator or allocation details were incompletely described in the archived article text; these studies were retained only for narrative synthesis and were judged conservatively in the ROBINS-I display rather than pooled. Candidate dravyas such as Valeriana wallichii (Tagara) and Tinospora cordifolia (Giloy/Guduchi) were retained in the search universe, but only nodes represented by eligible human evidence were retained in the final map. Secondary research and reports without eligible mental/cognitive outcomes were excluded.
Outcome taxonomy and node resolution
Domain A comprised cognition outcomes (e.g., attention, memory, and executive function); domain B comprised perceived stress, sleep, and related well-being outcomes in nonclinical or at-risk populations; and domain C comprised psychiatric symptom/disorder outcomes in diagnosis-defined or treatment-seeking clinical populations. Final domain assignment was based on enrolled population and measured outcomes rather than classical indication alone. A node was defined as the resolved intervention identity at the level of botanical species, plant part/material, and preparation/standardization status. Identity-uncertain common-name labels were retained as separate strata and were not pooled with resolved nodes. Worked examples are provided in Supplementary Data S2.
Study selection, data extraction, and risk of bias
A structured extraction workbook captured design, population, intervention characteristics, outcomes, and adverse events. Title/abstract screening, full-text review, data extraction, and risk-of-bias assessment were performed independently by two reviewers using structured forms. Disagreements or ambiguities were resolved by discussion, and a third reviewer was consulted when consensus could not be reached. Randomized trials were assessed with RoB 2. 6 Nonrandomized or comparator-imperfect quasiexperimental reports retained for narrative synthesis were appraised with ROBINS-I, 7 using conservative judgments when allocation or comparator reporting was incomplete. Figure 2 summarizes RoB 2 across randomized trials. Supplementary Table S4 provides study-level matrices for the randomized quantitative-synthesis trials (RoB 2) and the narratively synthesized nonrandomized/quasiexperimental subset (ROBINS-I).
Evidence mapping and evidence-volume descriptors
Evidence volume per node and domain is summarized in Supplementary Figure S1 and described as strong (≥3 controlled reports), moderate (2), limited (1), or none (0). These labels describe evidence volume only and are not certainty-of-evidence ratings.
Quantitative synthesis
Meta-analysis was undertaken only when at least two RCTs evaluated comparable node/preparation strata and reported sufficiently similar endpoints. Controlled nonrandomized studies were eligible for narrative synthesis and risk-of-bias assessment, but quantitative pooling was restricted to RCTs. For multiarm trials with a shared placebo group, placebo sample size was split across comparisons, in line with Cochrane guidance. 8 Random-effects models (DerSimonian–Laird) were used 9 ; effects were summarized as mean difference (MD) for common scales and Hedges g standardized MD (SMD) for different scales; heterogeneity was quantified by I2.
Results
Study selection
Across sources, 67 full texts were sought for retrieval; 66 were retrieved and screened; 49 reports met inclusion criteria for qualitative synthesis (Fig. 1). Seventeen reports were excluded at full-text stage, most commonly because they were secondary research or lacked an eligible mental/cognitive outcome. Best-estimate source-level retrieval counts before cross-database deduplication are summarized in Supplementary Table S5. 5
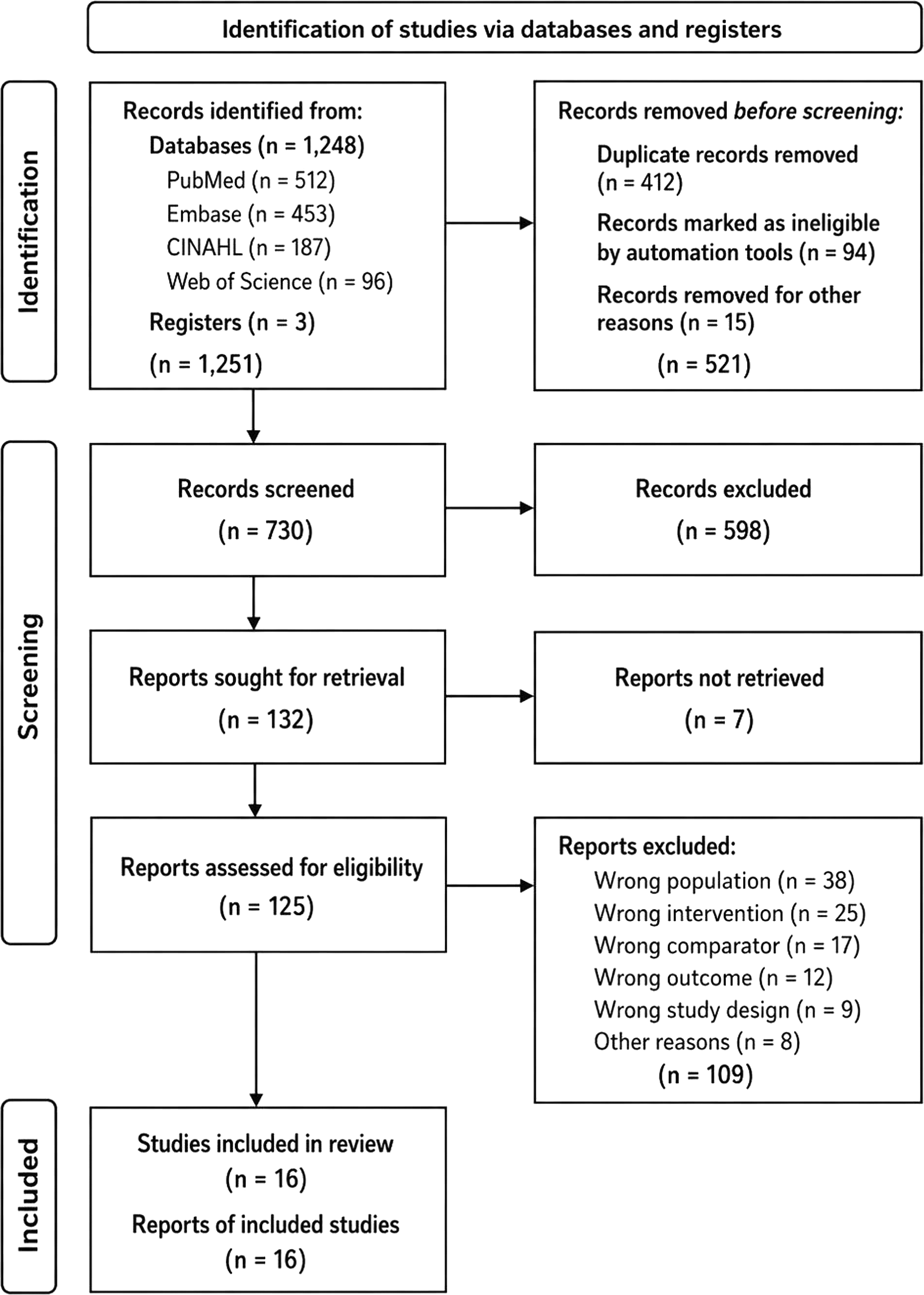
PRISMA 2020 flow diagram of study selection.
Included dravya nodes and evidence distribution: 20 node identifiers were represented (Table 1). Evidence volume was concentrated in Bacopa monnieri (Brahmi) for domain A (cognition) and Withania somnifera (Ashwagandha) preparations for domain B (stress/sleep). A complete node-by-domain evidence map is provided in Supplementary Figure S1.
Dravya Nodes and Report Counts (n = 49)
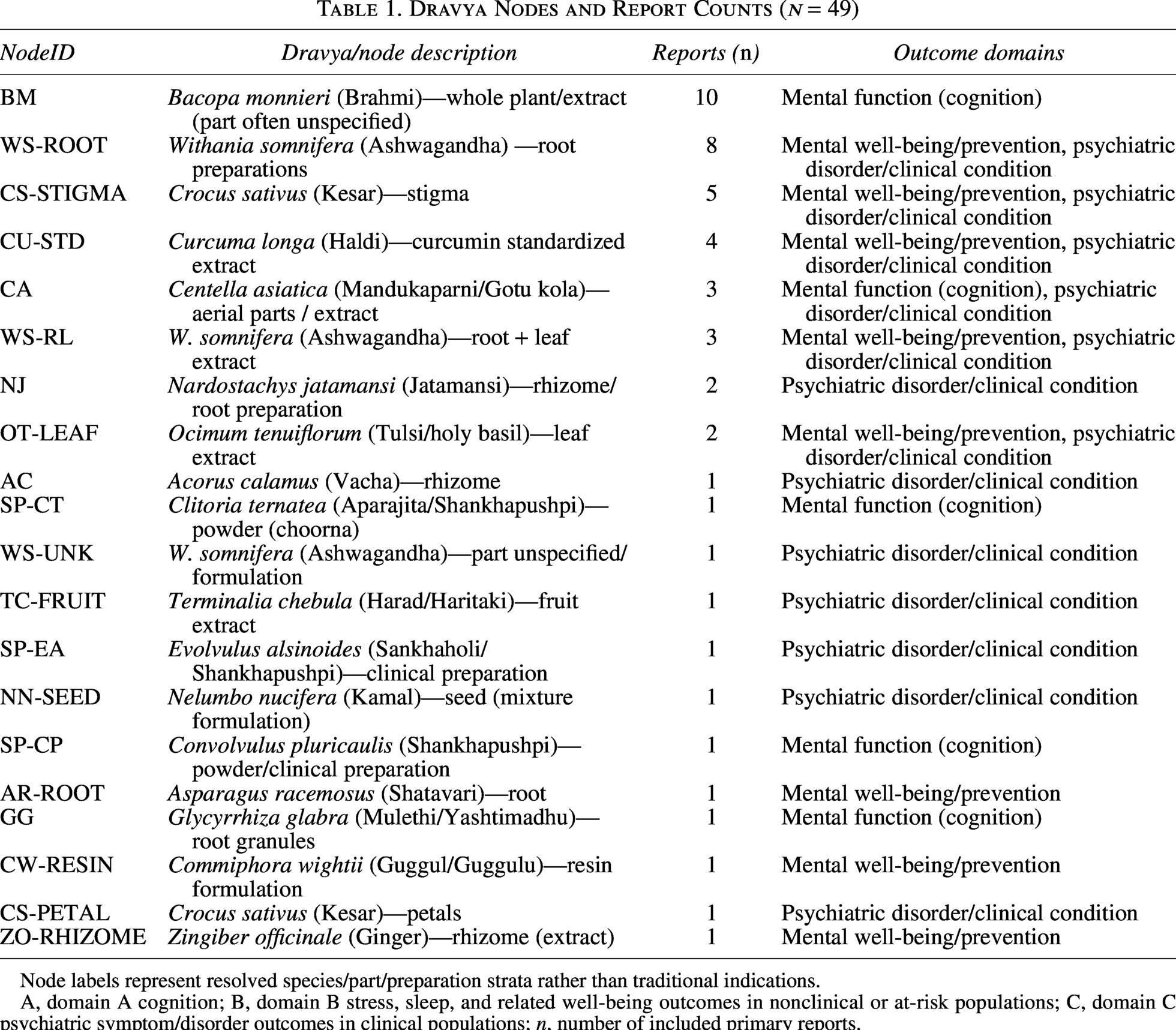
Node labels represent resolved species/part/preparation strata rather than traditional indications.
A, domain A cognition; B, domain B stress, sleep, and related well-being outcomes in nonclinical or at-risk populations; C, domain C psychiatric symptom/disorder outcomes in clinical populations; n, number of included primary reports.
Compact Grid of Node-by-Domain Findings with Evidence-Volume Descriptors
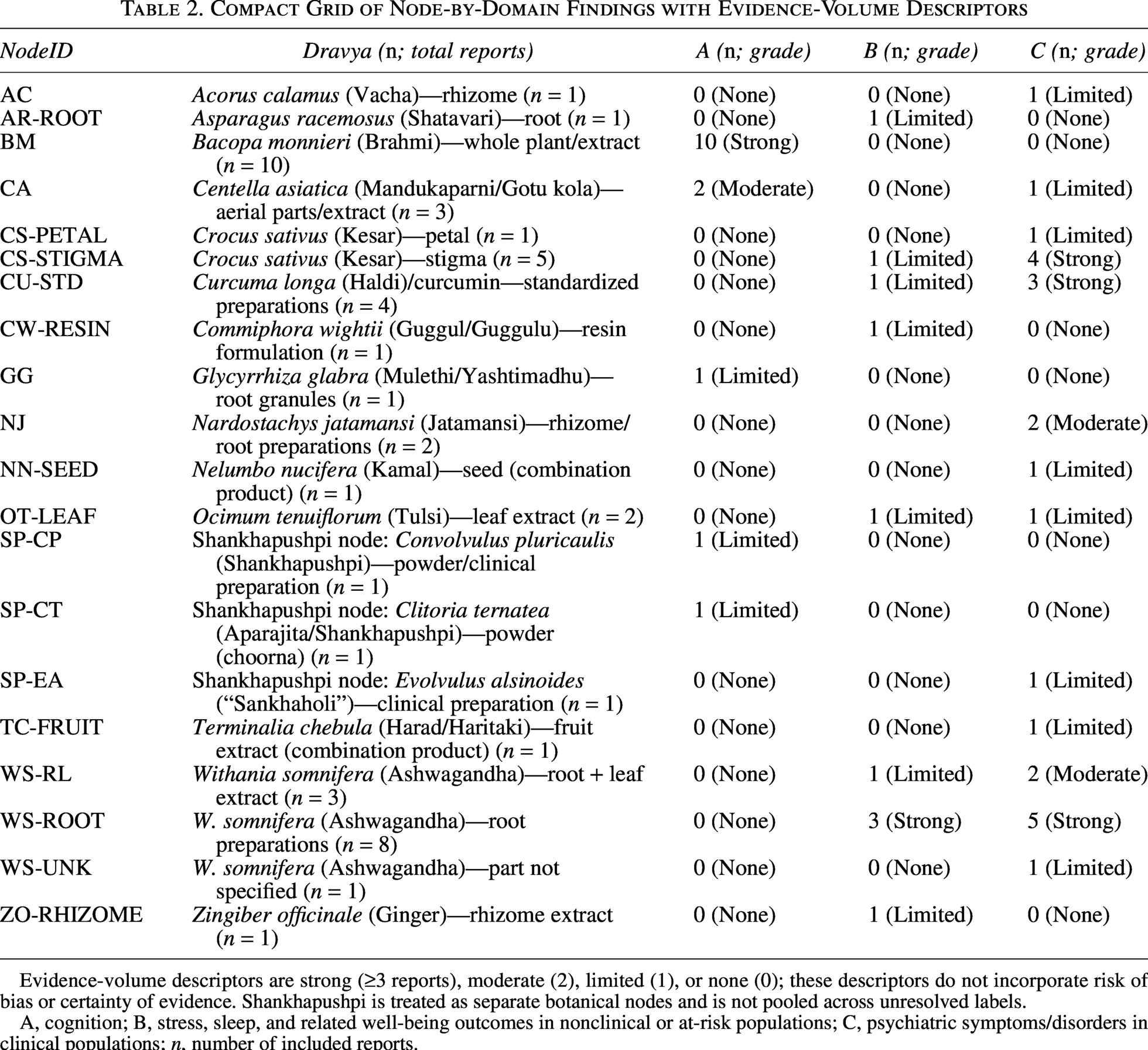
Evidence-volume descriptors are strong (≥3 reports), moderate (2), limited (1), or none (0); these descriptors do not incorporate risk of bias or certainty of evidence. Shankhapushpi is treated as separate botanical nodes and is not pooled across unresolved labels.
A, cognition; B, stress, sleep, and related well-being outcomes in nonclinical or at-risk populations; C, psychiatric symptoms/disorders in clinical populations; n, number of included reports.
Descriptive Safety Summary Across Included Reports (Node-Resolved)
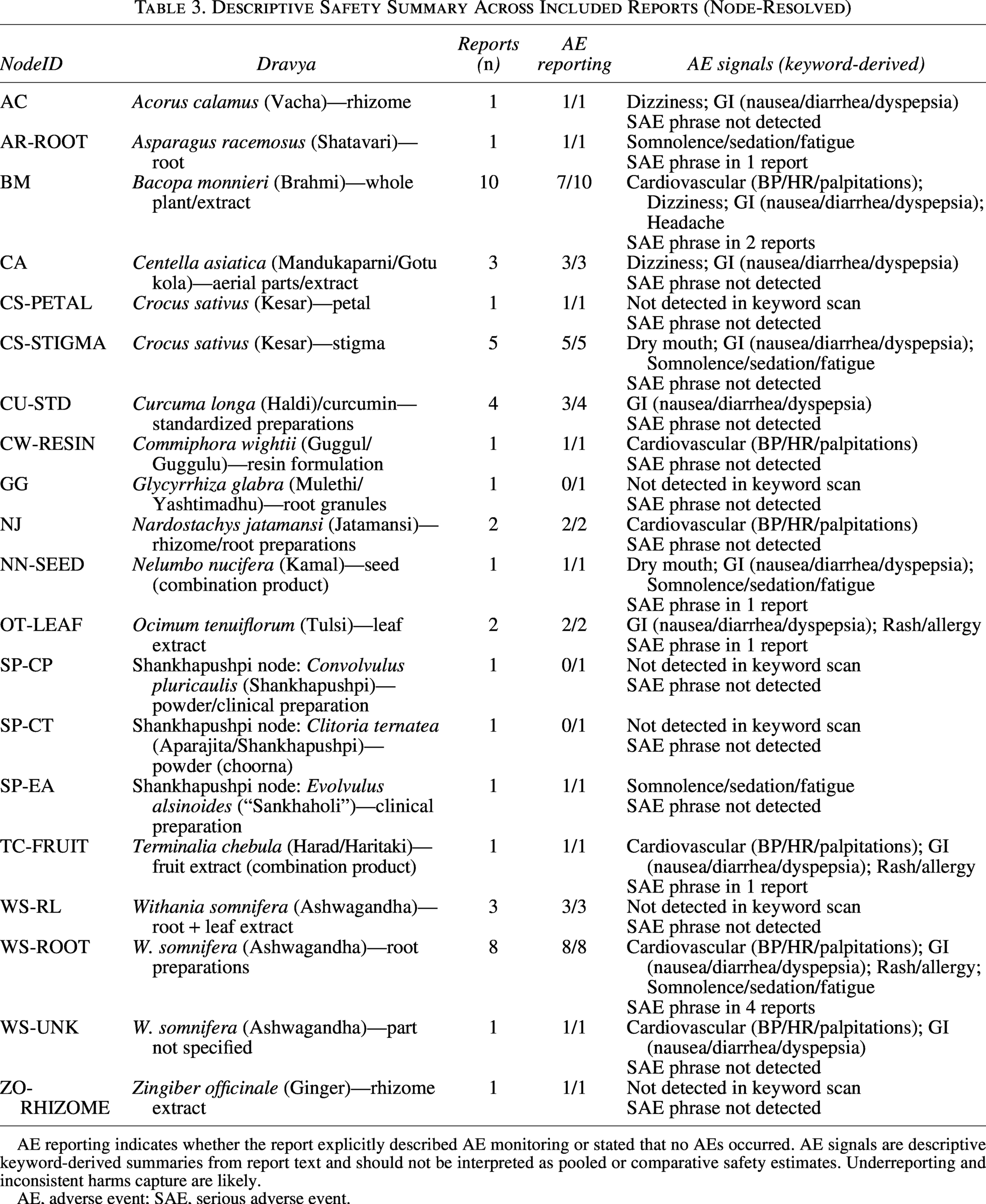
AE reporting indicates whether the report explicitly described AE monitoring or stated that no AEs occurred. AE signals are descriptive keyword-derived summaries from report text and should not be interpreted as pooled or comparative safety estimates. Underreporting and inconsistent harms capture are likely.
AE, adverse event; SAE, serious adverse event.
Geographically, the evidence base was concentrated in India, with additional controlled trials from Australia, Iran, Thailand, and North America. This concentration should be considered when interpreting the generalizability of formulations, participant characteristics, and background patterns of traditional use. Cognition-related trials were concentrated in B. monnieri (Brahmi), Centella asiatica (Mandukaparni/Gotu kola), Clitoria ternatea (Aparajita/Shankhapushpi), Glycyrrhiza glabra (Mulethi/Yashtimadhu), and related cognitive nodes.10–25 Stress, sleep, and related well-being trials were dominated by W. somnifera (Ashwagandha) and selected dravya combinations.25–42 Psychiatric symptom/disorder trials involved saffron, curcumin, Nardostachys jatamansi (Jatamansi), Acorus calamus (Vacha), and Shankhapushpi-related nodes.43–57
Systematic review findings
Domain A (cognition)
B. monnieri (Brahmi; BM) accounted for the largest cluster of controlled cognition studies, with several RCTs in healthy adults, older adults, or cognitively impaired participants reporting outcomes in memory, attention, and broader cognitive performance. C. asiatica (Mandukaparni/Gotu kola) studies contributed smaller but relevant cognition/mood evidence; C. ternatea (Aparajita/Shankhapushpi), G. glabra (Mulethi/Yashtimadhu), and combination products contributed single-study signals. Overall, domain A was broad and clinically relevant, but endpoint heterogeneity prevented a pooled cognition meta-analysis across all nodes.10–24,39
Domain B (stress, sleep, and related well-being)
W. somnifera (Ashwagandha) preparations were most frequently studied for perceived stress, sleep quality, anxiety symptoms, cortisol, and related well-being outcomes. Additional evidence was identified for Ocimum tenuiflorum (Tulsi), Nelumbo nucifera (Kamal) combination products, Asparagus racemosus (Shatavari), and multibotanical formulations. These studies generally suggested favorable directions of effect, but variability in formulation, duration, and outcome instruments limited direct comparability. Meta-analysis was feasible only for the Withania perceived-stress and sleep-quality strata.25–42,58
Domain C (psychiatric symptoms/disorders)
Psychiatric-disorder evidence was most visible for Crocus sativus (Kesar) and Curcuma longa (Haldi; curcumin preparations) in depressive symptom outcomes, with additional single-node or small-cluster evidence for N. jatamansi (Jatamansi) in depression contexts, A. calamus (Vacha) and Evolvulus alsinoides (Sankhaholi/Shankhapushpi) in anxiety-related conditions, and Convolvulus/Clitoria nodes in cognitive or anxiety-adjacent clinical contexts. Only the curcumin-placebo depression stratum met the minimum comparability criteria for quantitative pooling in this dataset.43–57
Figure 2 summarizes RoB 2 across randomized trials. Across randomized trials, the RoB 2 profile was dominated by “some concerns” rather than uniformly low risk: the overall summary indicated approximately 12% low risk, 78% some concerns, and 10% high risk, with the randomization process and missing outcome data contributing most often to concern. Supplementary Table S4 provides the study-level RoB 2 matrix for the randomized trials contributing to quantitative syntheses. For the small narratively synthesized nonrandomized/quasiexperimental subset, best-reconstructed ROBINS-I judgments were predominantly serious-to-critical, driven mainly by incomplete allocation/comparator reporting and outcome-measurement limitations; these are displayed in Supplementary Table S4 and Supplementary Figure S4. These judgments informed the cautious interpretation of both pooled and narrative effects. A compact cross-domain summary of node-by-domain findings and evidence-volume descriptors is presented in Table 2. A descriptive node-resolved summary of adverse-event reporting and safety signals across the included reports is provided in Table 3.
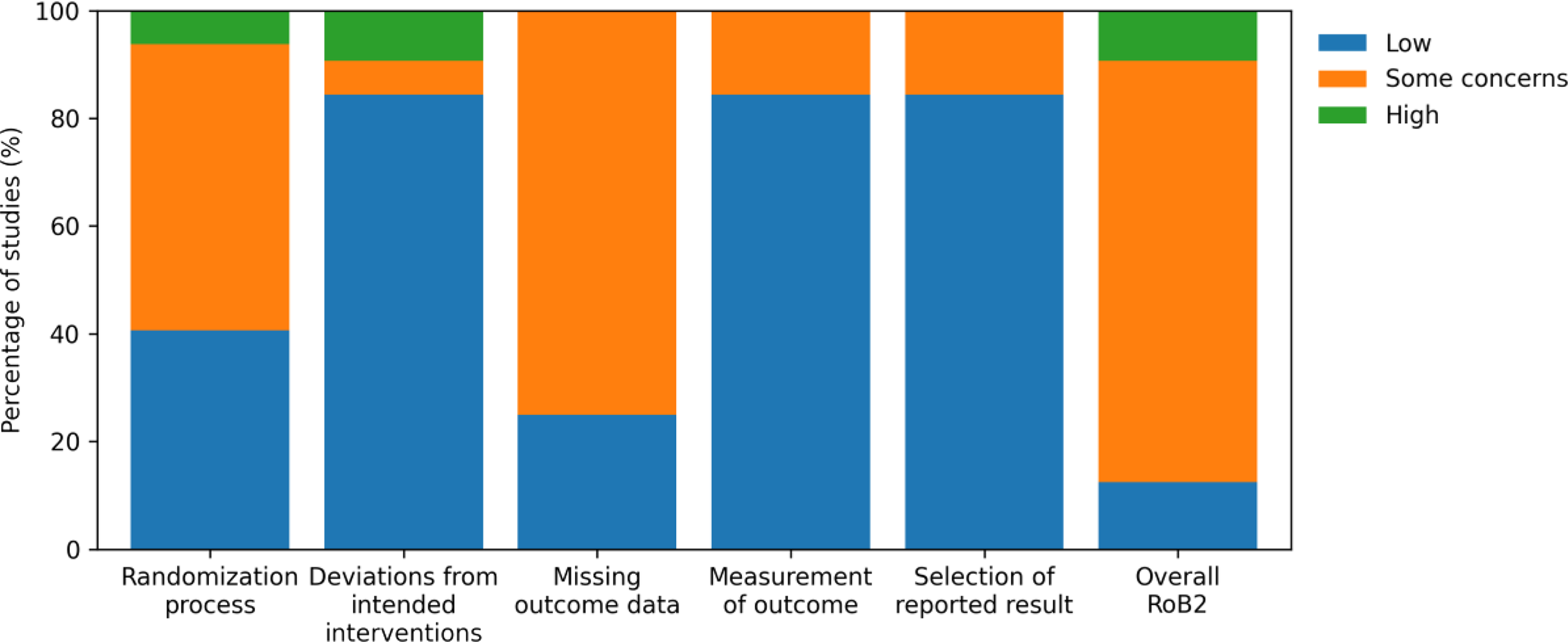
Risk-of-bias summary across included randomized trials (n = 32) (RoB 2). Note: RoB 2 panel only; nonrandomized controlled studies appraised with ROBINS-I are not shown here; n = 32 randomized trials.
Safety reporting was descriptive only: adverse events were narratively extracted as reported, adverse-event monitoring itself was inconsistently described, and the tabulation should not be interpreted as a comparative safety analysis.
Meta-analysis
Meta-analysis was feasible for three primary strata with comparable endpoints and preparation features: (i) W. somnifera (Ashwagandha) preparations versus placebo on perceived stress (Perceived Stress Scale [PSS]; domain B), (ii) W. somnifera (Ashwagandha) preparations versus placebo on sleep quality (Pittsburgh Sleep Quality Index [PSQI]; domain B), and (iii) curcumin preparations versus placebo on depression severity (domain C). Primary and exploratory sensitivity results are summarized in Table 4 and are shown in Figures 3–5 and Supplementary Figure S3.
Summary of Primary Quantitative Syntheses (Random-Effects Meta-Analysis)
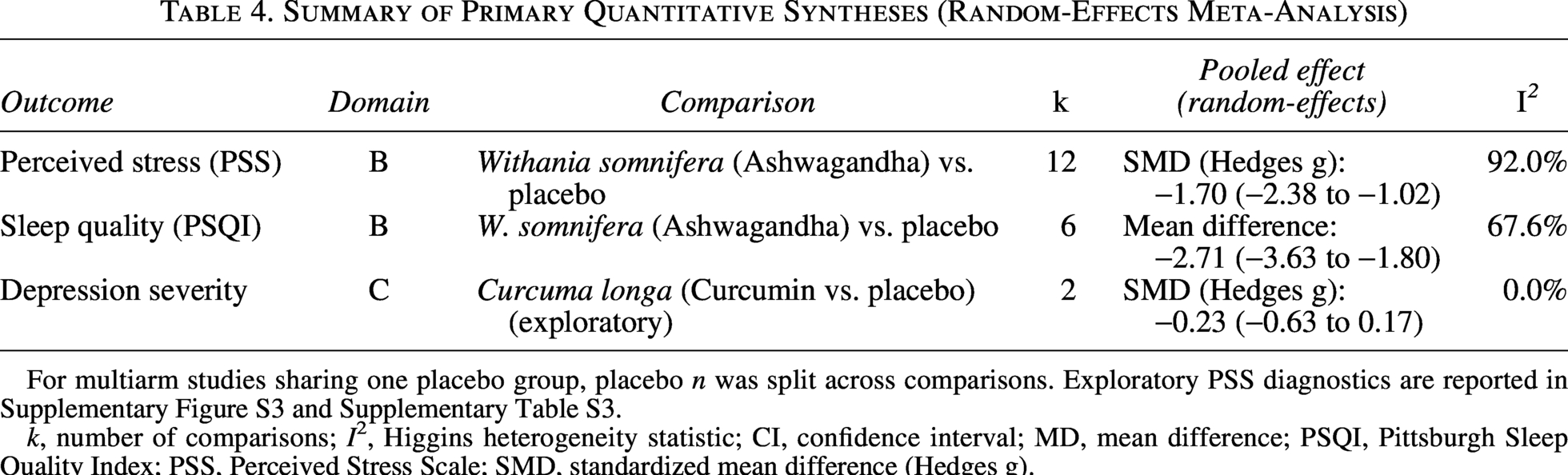
For multiarm studies sharing one placebo group, placebo n was split across comparisons. Exploratory PSS diagnostics are reported in Supplementary Figure S3 and Supplementary Table S3.
k, number of comparisons; I2, Higgins heterogeneity statistic; CI, confidence interval; MD, mean difference; PSQI, Pittsburgh Sleep Quality Index; PSS, Perceived Stress Scale; SMD, standardized mean difference (Hedges g).
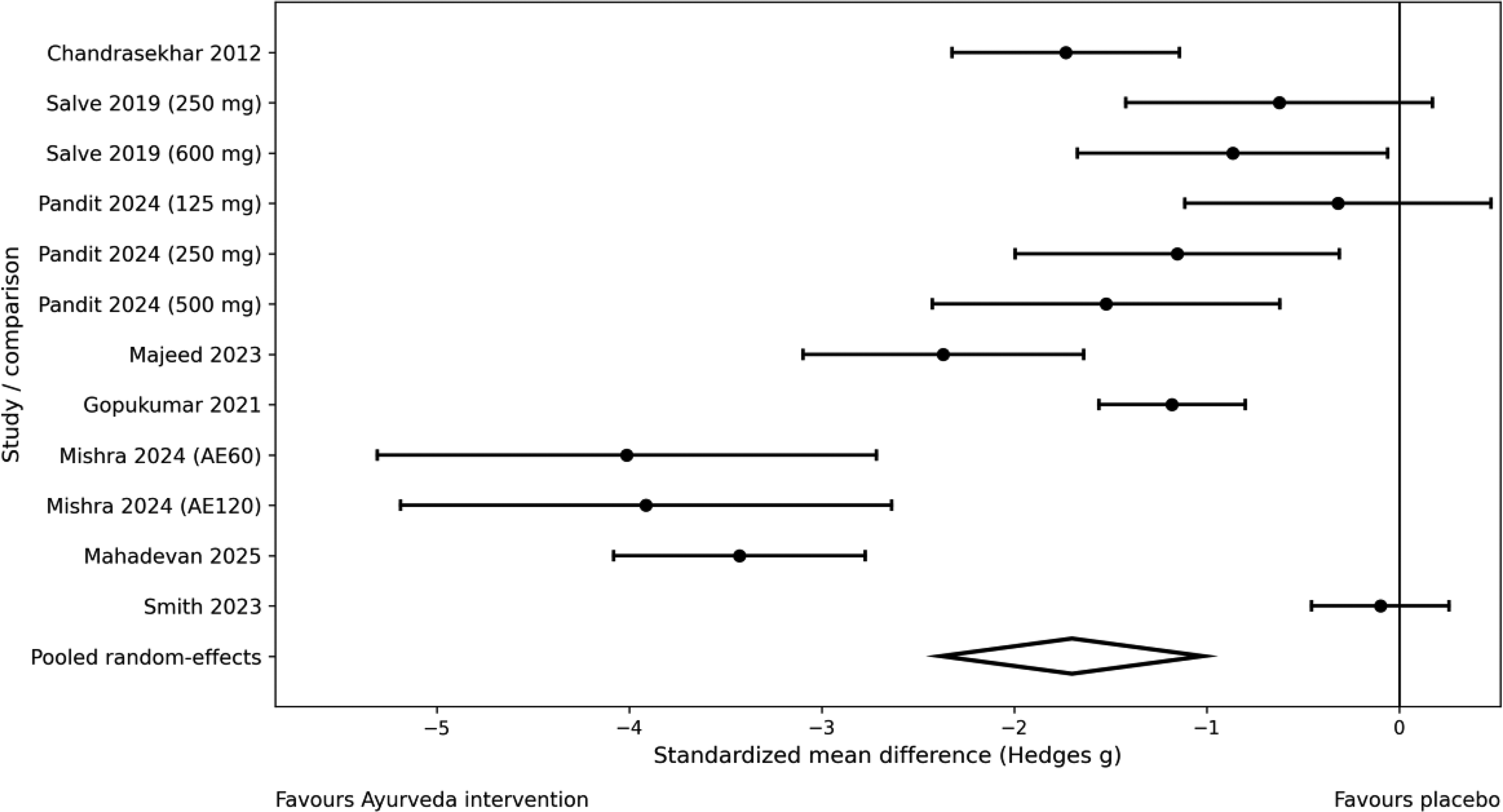
Forest plot of Withania somnifera (Ashwagandha) preparations versus placebo on perceived stress (PSS). Negative values indicate lower stress. PSS, Perceived Stress Scale.
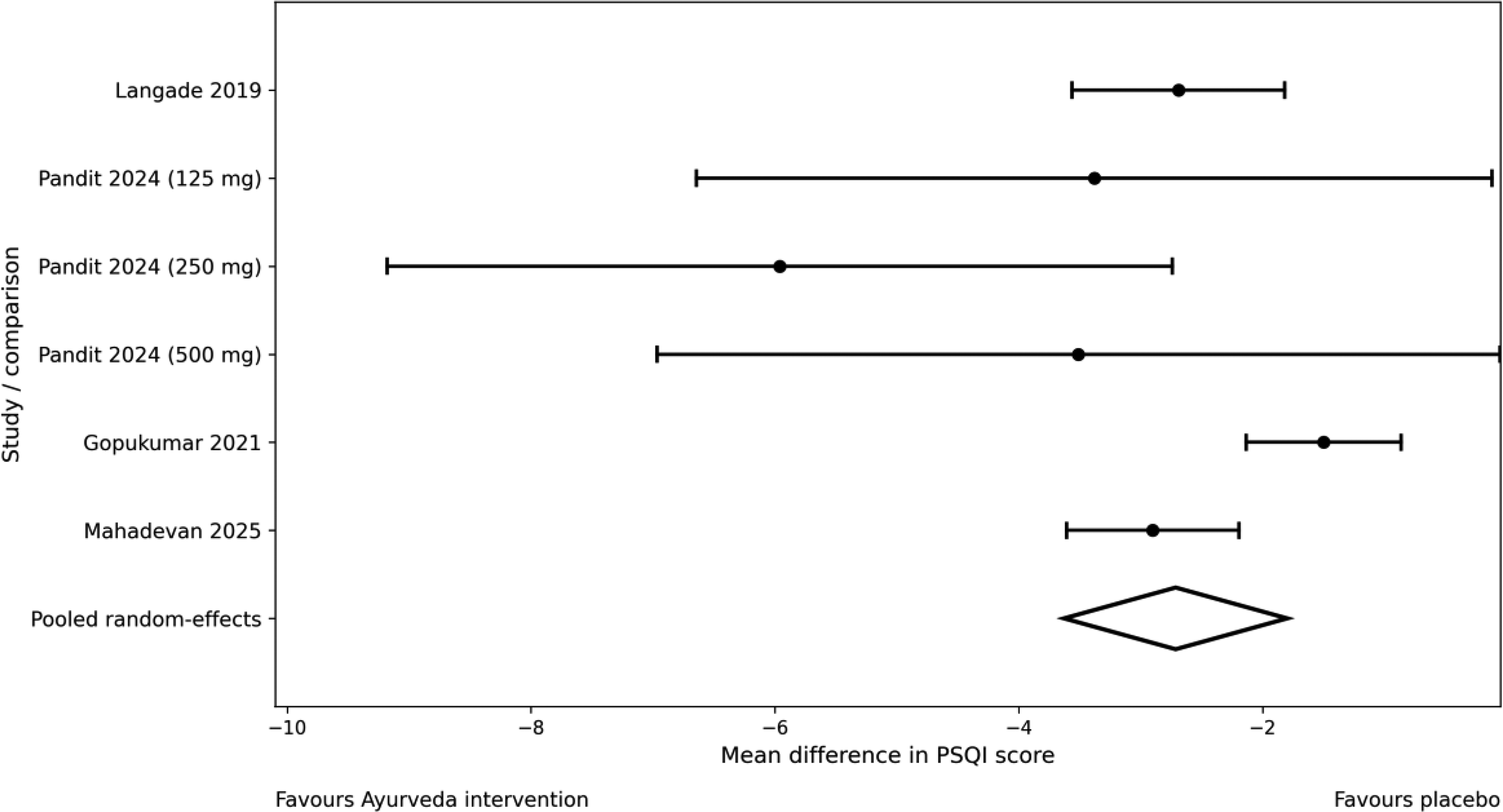
Forest plot of Withania somnifera (Ashwagandha) preparations versus placebo on sleep quality (PSQI). Negative values indicate improved sleep quality. PSQI, Pittsburgh Sleep Quality Index.
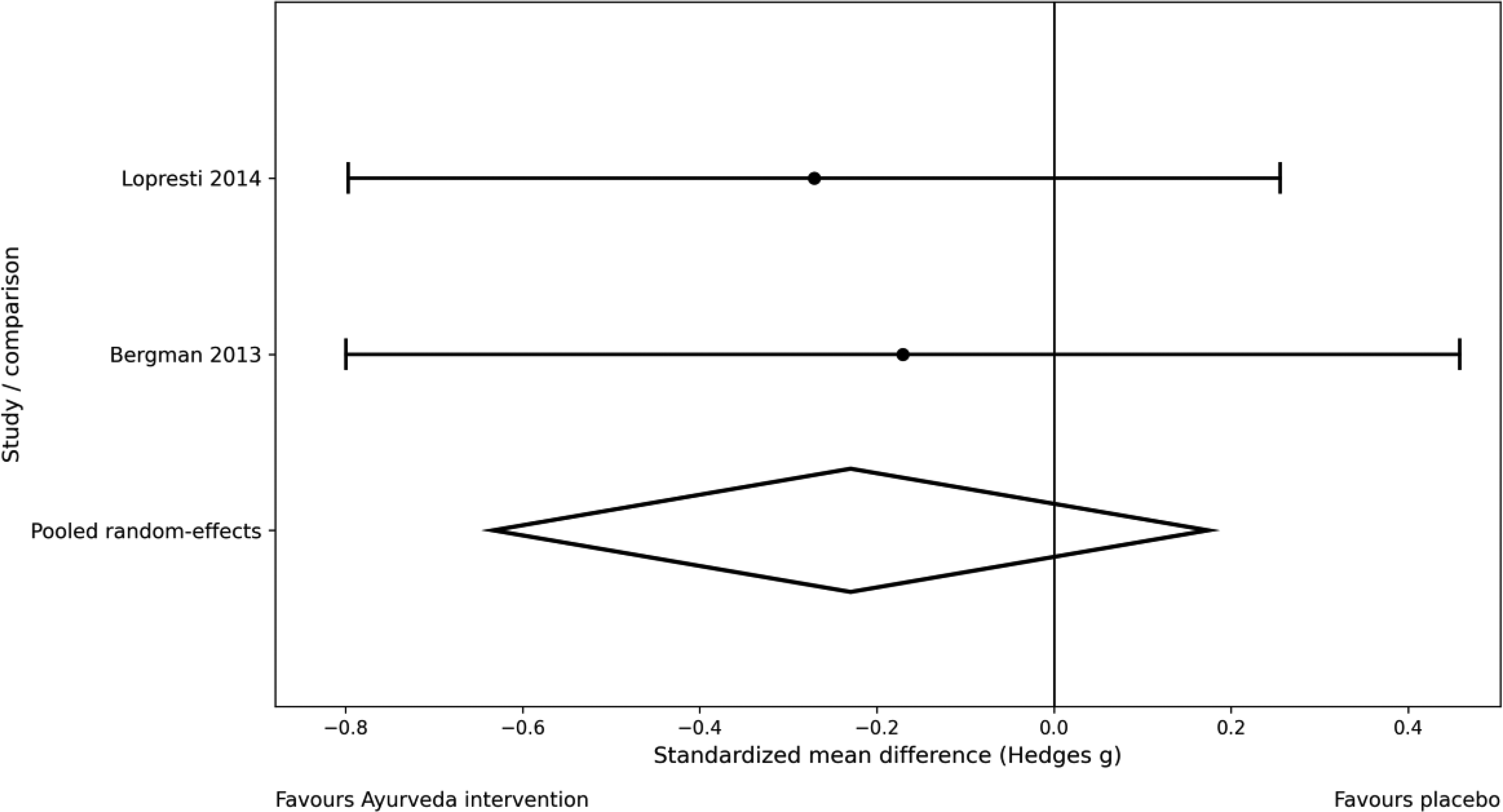
Forest plot of curcumin preparations versus placebo on depression severity (standardized mean difference). Negative values indicate lower symptom severity.
For PSS, the pooled effect favored W. somnifera (Ashwagandha), but heterogeneity was extreme. Exploratory diagnostics suggested that the primary result was sensitive to study characteristics. Egger’s regression did not demonstrate statistically significant funnel-plot asymmetry at the conventional 0.05 threshold (intercept p = 0.054), but visual asymmetry and the disproportionate influence of several small, high-effect comparisons supported cautious interpretation (Supplementary Fig. S3).
Excluding the clearly root + leaf extract comparisons attenuated the pooled PSS effect to SMD −1.33 (95% CI −1.98 to −0.67; I2 = 90.9%), while exclusion of comparisons with fewer than 40 participants per arm further widened uncertainty (SMD −1.54, 95% CI −3.14 to 0.05; I2 = 97.4%). The PSQI synthesis remained in favor of W. somnifera (Ashwagandha) and is classified here under domain B because the pooled trials were conducted primarily in stressed, nonclinical populations. The curcumin synthesis remained exploratory because only two placebo-controlled comparisons were available; the pooled estimate was imprecise and compatible with both benefit and no effect. No overall-high-risk trial was present in the study-level RoB 2 matrix for the quantitative syntheses, so risk-of-bias integration for PSS was handled through explicit RoB description, GRADE downgrading, and qualitative interpretation rather than an uninformative exclude-high-risk repooling. Formal dose- or population-based subgrouping and metaregression were not feasible because the archived comparison-level PSS dataset did not provide enough consistently recoverable covariate structure once preparation-sensitive node separation was maintained.
Discussion
This revised node-resolved synthesis indicates that controlled human evidence for Ayurvedic dravya-based herbal medicinal products in mental-health research remains concentrated in a limited number of nodes. B. monnieri (Brahmi) accounted for most cognition reports,10–19 W. somnifera (Ashwagandha) dominated stress and sleep studies,25–36 and saffron/curcumin provided the clearest psychiatric-disorder evidence clusters.43–53 The node-resolved framework therefore helped distinguish evidence volume from effect magnitude and avoided inappropriate pooling of common-name clusters such as Shankhapushpi.
The Withania stress signal should, however, be interpreted as provisional rather than stable in magnitude. The pooled PSS effect was large, but it arose in the setting of extreme heterogeneity, an RoB 2 profile dominated by some concerns, and formulation-sensitive diagnostics. These findings support biological and clinical plausibility for stress reduction, but they do not establish a single uniform effect size for all Withania preparations.25–36
Safety findings should be read descriptively only. The review did not pool adverse-event rates, and adverse-event monitoring itself was inconsistently described. Reported events were usually mild or absent, but incomplete harms reporting limits confidence in comparative safety. Future trials should predefine adverse-event ascertainment, laboratory monitoring, and drug–drug interaction reporting, particularly for products used alongside psychotropics or in medically complex populations.
Rasapanchaka-based interpretation and translational alignment: Rasapanchaka doctrine is central to classical Dravyaguna reasoning because rasa, guna, virya, vipaka, and prabhava are used to guide drug selection and interpret expected actions. Although most included clinical trials did not explicitly report Rasapanchaka profiles, this information can be triangulated from authoritative Dravyaguna sources and used as an interpretive layer rather than as a quantitative pooling variable.59,60 In the present evidence map, Medhya-positioned nodes such as B. monnieri (Brahmi) and C. asiatica (Mandukaparni/Gotu kola) were represented mainly in cognition-oriented outcomes; rasayana/adaptogenic W. somnifera (Ashwagandha) preparations were represented mainly in stress and sleep outcomes; and sleep/calm-oriented nodes such as Tagara and Jatamansi remain promising but understudied. This alignment is conceptually coherent but should be interpreted cautiously because modern RCTs typically evaluate standardized psychometric outcomes rather than classical Rasapanchaka-derived endpoints.
Strengths of this review include the node-resolved identity framework, explicit domain definitions, full search strategies, best-estimate source-level retrieval counts, the addition of formal risk-of-bias displays, and the incorporation of Rasapanchaka as an interpretive Dravyaguna layer. Limitations include lack of prospective external registration, residual uncertainty in some older trials, heterogeneous formulations, relatively small sample sizes, short follow-up, inconsistent adverse-event reporting, and limited feasibility of meta-analysis beyond three strata. These constraints should temper clinical translation and highlight the need for larger, adequately blinded, node-specific trials with harmonized mental-health outcomes.
Conclusion
Controlled human evidence identifies potentially beneficial signals for selected dravya-based interventions in cognition, stress, sleep, and depressive symptoms, but confidence is uneven and often limited. Node-resolved synthesis, standardized botanical nomenclature, and Rasapanchaka-informed interpretation improve the scientific and Ayurvedic precision of this evidence base. Future studies should report intervention identity, preparation, dose, Rasapanchaka-relevant attributes, validated mental-health endpoints, and harms with sufficient detail to support reproducible synthesis.
Data Availability
The review is based on published studies. Supplementary methods, tables, and figures are included with the submission; derived extraction summaries supporting the reported syntheses are available from the corresponding author upon reasonable request.
AI Declaration
Computational assistance was used to support formatting under human oversight. No AI was used to fabricate data or to create deceptive images; figures are derived from extracted study data and standard plotting routines.
Authors’ Contributions
CRediT authorship contribution statement: Conceptualization, methodology, investigation, writing—original draft, and writing—review and editing: B.T.B., M.M.P., M.V.P., and S.N.G. Supervision: B.T.B.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.