
Abstract
Background:
In women who have had a cesarean section, symptoms such as pain, mood swings, and fatigue can negatively impact the postpartum recovery process and make newborn care more difficult. While practical interventions such as classical foot massage (CFM) and kinesio taping (KT) are clinically promising, evidence in the literature regarding the comparative effectiveness of these methods is limited.
Objectives:
To compare the effects of KT and CFM on pain (primary outcome), fatigue and mood (secondary outcome).
Methods:
This parallel-group randomized controlled trial was conducted at a university hospital in the Aegean region of Türkiye between December 2024 and April 2025. A total of 105 participants meeting the criteria were randomized into the study (n = 35 in each group); after losses during the follow-up period (KT: 3, CFM: 2, CG: 3), the study was completed and analyzed with 97 participants: KT (n = 32), CFM (n = 33), and CG (n = 32). KT was administered at the 8th hour postoperatively; CFM was administered at 8th and 33rd hours using a standard protocol.
Results:
Group differences at the 8th and 33rd hours, representing the pre-intervention period, were similar. At 9th hour, lower pain scores were found in the CFM compared to the KT and CG (Cohen’s f = 0.34; 95% confidence interval [CI]: [2.90–4.43]; p = 0.009). Similarly, at 34th hour, lower pain scores persisted in the CFM group (Cohen’s f = 0.31; 95% CI: [1.77–3.08]; p = 0.014). Regarding subscales, higher “energy” scores were observed in the CFM at 8th hour (Cohen’s f = 0.28; 95% CI: [5.08–6.47]; p = 0.026), whereas the KT group showed higher energy at 34th hour (Cohen’s f = 0.27; 95% CI:[5.50–6.77]; p = 0.034). In addition, the pleasant mood subscale was significantly higher in favor of CFM at 34th hour (Cohen’s f = 0.43; 95% CI: [19.23–23.86]; p = 0.014). No serious side effects were observed during the applications. Mild and transient discomfort was reported in a small number of participants in the CFM group.
Conclusion:
CFM demonstrated a more pronounced short-term effect in reducing postcesarean pain compared to KT and the CG. Time-varying differences were observed between the CFM and KT groups in terms of energy levels and mood. However, larger-scale studies are needed to confirm the place and effectiveness of these methods in routine clinical use.
Trial Registration:
ClinicalTrials.gov NCT06811285.
Introduction
Pain is one of the most common problems in the postcesarean period. Incision pain after cesarean delivery can lead to negative effects such as difficulty breastfeeding, decreased sleep quality, increased anxiety, prolonged recovery time, and longer hospital stays. 1 Various complementary therapy methods such as massage, kinesio taping (KT), relaxing music, relaxation exercises, mind–body techniques, reflexology, herbal treatments, hypnosis, and therapeutic touch are used to support pain management.2,3
KT, one of the complementary therapy methods used to relieve pain, is effective in superficial and deep tissues by continuously stimulating the receptors in the skin. 4 This mechanism is based on Melzack and Wall’s (1965) gate control theory of pain. 5 KT can help strengthen muscles, increase blood and lymph circulation, reduce pain, support joints, and improve balance and movement awareness. 6 KT can remain on the skin for 3 days with its breathable and water-resistant structure. 3 Postpartum women who received KT generally report a reduction in certain symptoms and an increase in comfort. The elastic structure of the band supports movement ability by adapting to the body. 7 Another complementary therapy method for pain relief is classical foot massage (CFM). This method provides relaxation and general well-being with rhythmic and systematic touches applied to the soft tissues of the body. This application increases the release of endorphins by stimulating nerve endings and thus contributes to the reduction of pain. 8 The fact that pain receptors are most densely located in the hands and feet suggests that CFM may be an effective method for relieving pain after cesarean section by providing neuronal stimulation. 9
There are a limited number of studies in the literature that separately examine the effects of KT and CFM on pain in women who have given birth by cesarean section. However, no study has been found that evaluates the effects of KT and CFM applied to mothers after cesarean section together and examines their effects on pain, fatigue, and mood. This study was conducted to determine the effects of KT and CFM applied to mothers after cesarean section on pain, fatigue, and mood.
Research hypotheses
Pain levels of women who received KT after cesarean section are lower than those who did not.
Fatigue levels of women who received KT after cesarean section are lower than those who did not.
Post-cesarean women who received KT had higher scores on the “pleasant mood” subscale compared to those who did not receive the application.
The pain levels of women who underwent CFM after cesarean delivery are lower than those who did not.
The fatigue levels of women who underwent CFM after cesarean delivery are lower than those who did not.
Post-cesarean women who received CFM had higher scores on the “pleasant mood” subscale compared to those who did not receive the application.
Materials and Methods
Study design
A parallel-group, single-blind randomized controlled clinical trial was conducted in two different obstetrics and gynecology departments in a Training and Research Hospital located in the Central Aegean Region of Türkiye between December 02, 2024, and April 18, 2025. The study was reported according to the Consolidated Standards of Reporting Trials (CONSORT) 2025 guideline. 10
Inclusion criteria
Inclusion criteria are as follows: being between 38 and 42 gestational weeks for the study, being between 18 and 45 years of age, having received general anesthesia, being able to speak Turkish, having a transverse incision cesarean section, having given birth to a live baby weighing 2500–4000 g, having a singleton pregnancy, not having a dermatological condition, and being willing to participate in the study. The patients were prepared for mobilization after 6 h. Before mobilization, nonsteroidal anti-inflammatory drugs (75 mg sodium diclofenac per ampoule) were administered. The participants did not use any other analgesic drugs during the analgesia process.
Exclusion criteria
Exclusion criteria are as follows: those diagnosed with allergic skin conditions, those with postpartum complications (bleeding, infection), those with a body mass index of 40 or above, those with hemoglobin levels lower than 9 g/dL or hematocrit levels lower than 30%, those with any psychiatric disorder, those using different types and doses of painkillers in the postoperative period, those whose babies are being treated in the neonatal intensive care unit, and participants with impaired consciousness or communication difficulties.
Data collection tools
Study data were assessed using an information form prepared for the study, the Visual Analog Scale for Fatigue (VAS-F), and the Brief Mood Introspection Scale (BMIS) for mood.
Information form
The information form includes 11 descriptive questions aiming to examine the participants’ introductory and obstetric characteristics, including age, education status, occupation, social security, chronic disease, number of cesarean sections, planned pregnancies, and smoking status.
Primary outcome
The primary outcome of the study was postoperative pain intensity. Pain was assessed using the Visual Analog Scale (VAS). VAS is commonly used to assess postpartum pain by translating subjective pain experiences into measurable values. It consists of a 100-mm line, which can be either horizontal or vertical, with endpoints labeled “no pain” (0) and “worst possible pain” (100). Participants are instructed to place a mark on the line corresponding to the intensity of their current pain. The distance from the “no pain” end to the mark is then measured in millimeters to provide a numerical representation of pain severity. 11 Prior to the assessment, participants received a detailed explanation of how to use the scale to ensure accurate reporting.
Secondary outcome
The secondary outcomes included fatigue and mood status.
Fatigue was evaluated using the VAS-F, which was developed by Lee et al. (1991) to assess individuals’ fatigue; its Turkish validity and reliability study was conducted by Yurtsever and Bedük (2003).12,13 VAS-F is an 18-item scale with 2 subdimensions, namely fatigue and energy. There are 10 cm lines on each statement of the scale. Participants were asked to mark on this line. In this scale, the Fatigue subdimension is scored as minimum: 0 and maximum: 130, and the Energy subdimension is scored as minimum: 0 and maximum: 50.12,13 For this study, the VAS-F Cronbach’s α values were found as 0.871 for the Fatigue subdimension and 0.832 for the Energy subdimension.
Mood status was measured using the BMIS. BMIS was developed by Mayer and Gaschke (1988); its Turkish validity–reliability study was conducted by Kavcıoğlu (2011). BMIS is a 16-item measurement tool with a 4-point Likert-type scale (1 = I definitely do not feel, 4 = I definitely feel) that evaluates individuals’ moods. The scale has two mood subdimensions: Pleasant and Unpleasant. The minimum score for each subdimension is 8, and the maximum score is 32.14,15 For this study, the BMIS Cronbach’s α values were found to be 0.830 for Positive Mood and 0.810 for Negative Mood.
Safety assesment
To assess the safety and patient tolerability of the procedures, all participants were meticulously monitored for potential adverse events during and after the procedure. Routine clinical conditions that arose in the postoperative period (mild nausea, incision pain, etc.) were managed with standard clinical care; however, specific to the procedures, skin irritation, erythema, or allergic reactions that might develop in the KT group, and discomfort, pain, or hypersensitivity during the procedure in the CFM group were monitored by the researchers.
Data collection
To ensure standardization and minimize data loss during the data collection process, participants were given detailed information by trained researchers on how to complete the scales (VAS-F and BMIS) prior to the application. Researchers were present at the data collection times to answer participants’ questions and address any potential ambiguities. All measurements were meticulously recorded according to a predetermined timeline: pain intensity at the 8th, 9th, 33rd, and 34th hours postoperatively, and fatigue and mood at the 8th and 34th hours.
Interventions
Two active interventions were evaluated in addition to routine postoperative care: kinesiology taping (KT) and CFM. Both protocols were standardized and delivered by trained professionals.
In accordance with Baby-Friendly Hospital protocols, breastfeeding practices were standardized among all participants. Mothers received regular breastfeeding support from trained midwives, including assistance with positioning and breastfeeding technique. Breastfeeding was initiated as early as clinically possible, and exclusive breastfeeding was encouraged. Infants were breastfed approximately every 2–3 h, with an average of 15–20 min of feeding from each breast. No mother experienced breastfeeding interruptions or clinically significant breastfeeding difficulties during the study period, and breastfeeding practices were comparable across all groups.
The primary outcome measure of the study was pain intensity, determined by the VAS. Pain intensity was assessed at four postoperative time periods: 8th, 9th, 33rd, and 34th hours. Participants’ fatigue and mood were evaluated as secondary outcome measures of the study. These secondary outcome measures were measured at the 8th and 34th postoperative hours.
Kinesiology taping protocol
A hypoallergenic cotton KT (brand, width 5 cm) was applied bilaterally over the rectus abdominis in parallel “I” strips with approximately 25% tension on clean, dry skin, while anchor zones were applied with 0% tension. All applications were performed by a KT-certified physiotherapist academician. Participants were instructed to keep the tape dry and report any pruritus or irritation (Fig. 1). At the 8th postoperative hour, KT was applied after a preoperative pain assessment with VAS and left in place until the 33rd hour. Pain levels were assessed using VAS at the 8th, 9th, 33rd, and 34th postoperative hours.

Kinesio Taping Protocol.
CFM protocol
Sessions were delivered by a trained midwife academician using a neutral lotion. The standardized massage sequence included effleurage (3 min)→petrissage (5 min)→friction/circular kneading (2 min) per foot, with a total duration of 20 min. Pressure was maintained at a moderate level (The patient was asked to rate the intensity of the pressure applied on a scale of 1–10. Foot massage was performed based on the patient’s perceived pressure level of 5–6) (Fig. 2). Before CFM applications, patients’ pain levels were assessed using a VAS at the 8th and 33rd postoperative hours. Following the applications, pain was assessed again using a VAS at the 9th and 34th postoperative hours to observe the effects of the CFM application.

Foot Massage Protocol.
Randomization
Participants who provided written informed consent and met the inclusion/exclusion criteria were numbered sequentially in order of registration, and these identification numbers were communicated to an independent statistician who was not involved in the recruitment, intervention, or outcome assessment processes. Participants were assigned to three groups (KT, CFM, and CG) using block randomization in a 1:1:1 ratio to ensure balanced distribution; the block size was set at six, and a randomization sequence was created using a random number table, with two participants per group in each block (Randomizer.org, https://www.randomizer.org). Blocks were applied according to sequential participant numbers, regardless of the recruitment time.
The random assignment list was securely stored by the independent statistician and had no access to it by any member of the research team. Group assignments were placed in sequentially numbered, sealed, and opaque envelopes and delivered to the principal investigator; the envelopes were opened sequentially by the principal investigator immediately before the intervention, and the group assignments were determined at this stage. Outcome evaluators were unaware of the group assignments and were not involved in the intervention process.
Bias and blinding
Due to the nature of the intervention, this study was conducted using an open-label design in which blinding of participants and implementers was not feasible. Therefore, blinding at the participant and practitioner level could not be applied. However, in order to minimize detection and interpretation biases, the data analysis process was planned to be blinded.
All collected data were coded to conceal group assignments and were analyzed by an independent biostatistician who was blinded to the intervention arms of the study. This approach aligns with item 11a (“Blinding”) of the CONSORT 2025 guidelines, which emphasize transparency and reliability in the reporting of randomized controlled trials. 10
By implementing this method, group information was not considered during statistical analysis, thereby enhancing the scientific credibility of the study.
Sample size
An a priori power analysis of the study was performed using the G*Power 3.1.9.4 program (Heinrich Heine Universität Düsseldorf, Germany) for one-way analysis of variance (ANOVA). In the calculation of the sample size, the effect size at the Cohen’s f = 0.25 level obtained in a randomized controlled trial examining the effect of kinesiology taping on pain in the postcesarean period 1 was taken as the basis. Accordingly, when the significance level (α) was determined as 0.05 and the statistical power was determined as 80%, it was determined that there should be 25 participants in each group. Considering the losses during the study, 30% more participants were added, and 35 participants were included in each group.
Statistical analysis
The data obtained in the study were analyzed using the Statistical Package for Social Sciences for Windows 25.0 program (IBM Corp., Armonk, NY, USA). Descriptive statistical methods (number, percentage, minimum–maximum values, mean, and standard deviation) were used while evaluating the data. Reliability analysis was performed to test the reliability of the scales. The conformity of the data to the normal distribution was tested with kurtosis and skewness values. In the comparison of quantitative data with normal distribution, one-way ANOVA, Bonferroni paired comparison test was used for the difference between more than two independent groups, and ANOVA test in repeated measures was used in the comparison of more than two dependent groups. Chi-square analysis was used to test the relationship between categorical variables.
One-way ANOVA was used for intergroup comparisons, and multiple comparisons were performed using the Bonferroni post hoc test when a significant difference was found. In accordance with the CONSORT statement, inferential statistical tests were not performed on baseline characteristics, which are considered a natural consequence of randomization; these variables were presented only with descriptive statistics. Similarly, in line with the main purpose of randomized controlled trials, within-group comparisons were not used as the basis for interpreting the results; analyses were structured to focus primarily on between-group differences.
In addition to statistical significance, effect sizes were also reported to strengthen clinical significance. Cohen’s f effect size coefficient was used for one-way ANOVA results. According to Cohen’s classification, f = 0.10 was considered small, f = 0.25 medium, and f ≥ 0.40 large effect. 16 To increase the reliability and clarity of interpretation of the results, 95% confidence intervals were also provided along with p-values. Thus, the study’s findings were evaluated holistically, not only in terms of statistical significance but also in terms of clinical effect size.
In the analysis of the data, a “per-protocol” analysis approach was adopted for managing missing data. No imputation method was used for participants who did not comply with the protocol or had missing data in their dataset; only participants with complete data at all measurement time points were included in the analyses.
Results
Participant flow
At the start of the study, a total of 105 participants meeting the eligibility criteria were randomized to participate (KT: 35, CFM: 35, CG: 35). During the follow-up period, eight participants were unable to complete the study for various reasons. These participants were identified as having failure to attend treatment and willingness to withdraw from the study in the KT group (n = 3), adaptation difficulty to intervention in the CFM group (n = 2), and willingness to withdraw from the study in the control group (n = 3). Per-protocol analyses were conducted on 97 participants who fully adhered to the protocol and completed all data collection stages (KT: 32, CFM: 33, CG: 32). Participant flow and reasons for exclusion are presented in detail in the CONSORT flowchart in Figure 3.
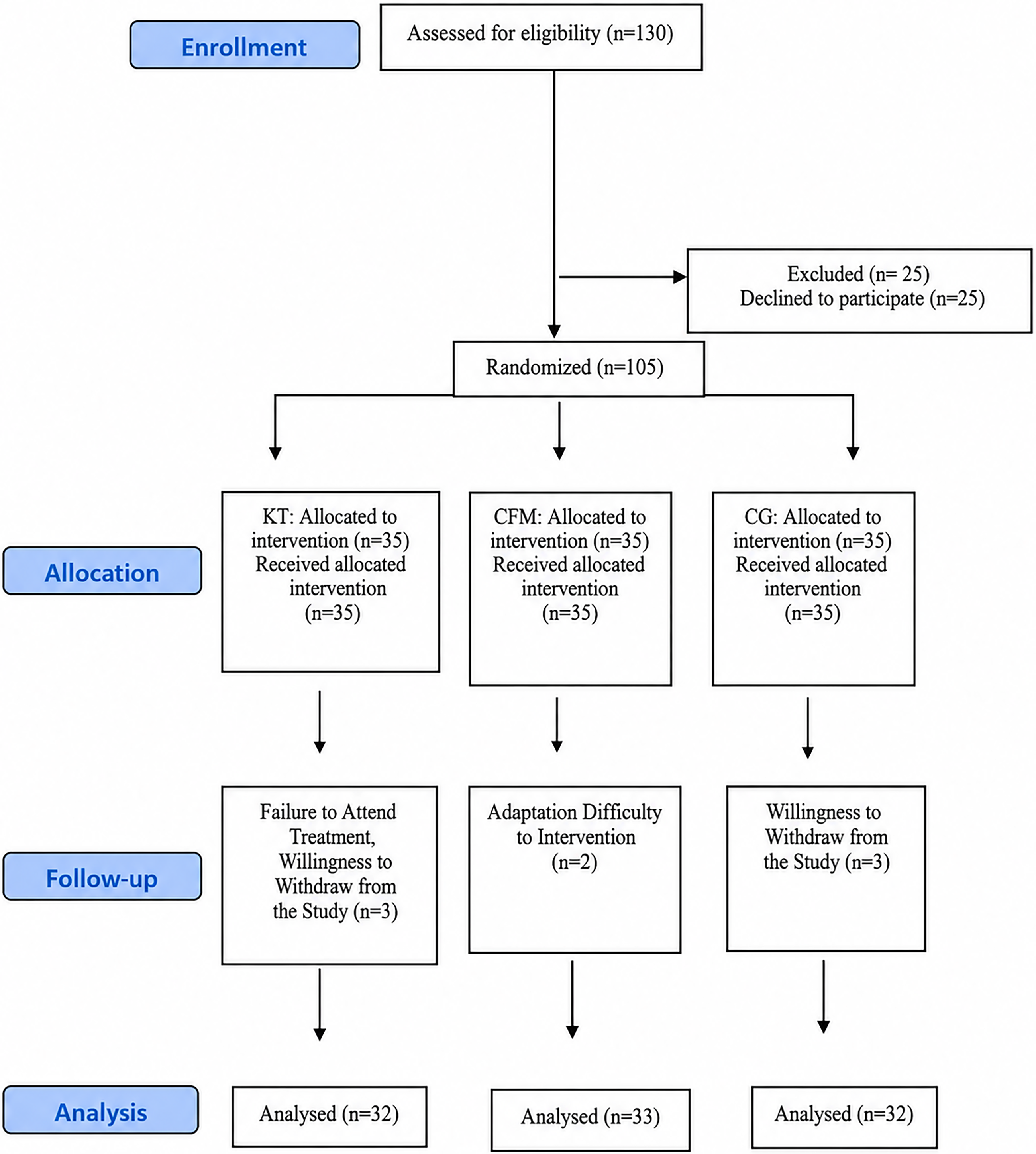
Participant flow diagram according to the CONSORT.
Participant introductory and clinical characteristics
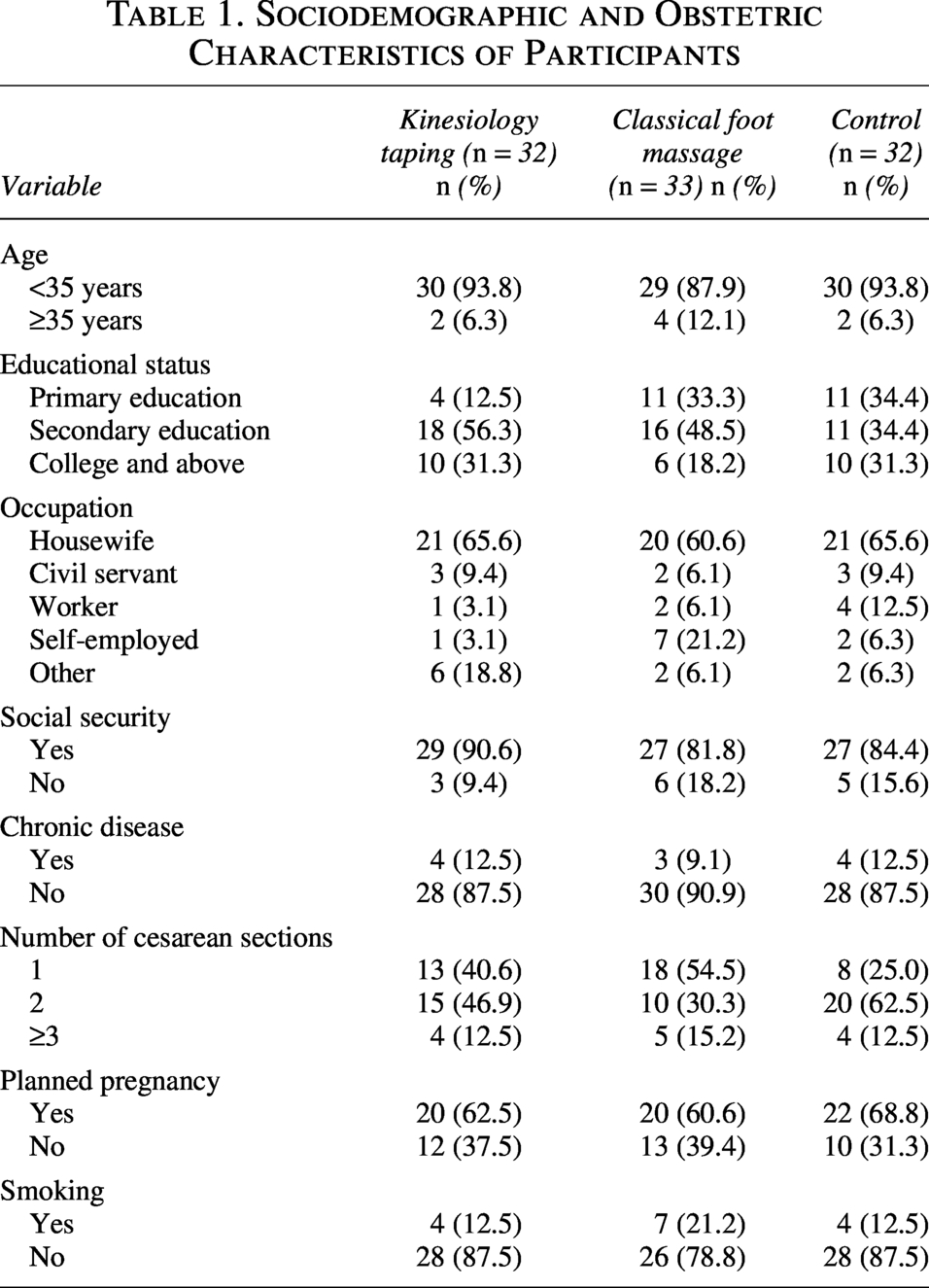
Participants’ age, education level, occupation, social security status, chronic disease status, number of cesarean sections, planned pregnancy, and smoking status were recorded (Table 1).
Sociodemographic and Obstetric Characteristics of Participants
Comparison of primary outcome among intervention groups and the control group
In the post hoc power analysis applied to 97 people to determine whether the sample size was sufficient, the effect size was found to be 0.64 at the α = 0.05 level according to the VAS results, and the power of the study was calculated as 0.92. According to the analysis, the power of the study was at an acceptable level, 16 and it was determined that the number of samples taken for each group was sufficient. 17
The analysis showed that there was no statistically significant difference in VAS scores among the groups at the postoperative 8th hour, prior to the intervention (p = 0.221), indicating that the participants had comparable baseline pain levels. However, following the intervention, significant differences emerged in the VAS scores measured at the postoperative 9th hour (p = 0.009). Between-group comparisons revealed a statistically significant difference in VAS scores at this time point (p < 0.05). Pairwise analyses indicated that the CFM group had significantly lower VAS scores compared to both the CG and KT groups, with this difference reflecting a medium effect size (Table 2).
Comparison of Visual Analog Scale Pain Scores Between Groups
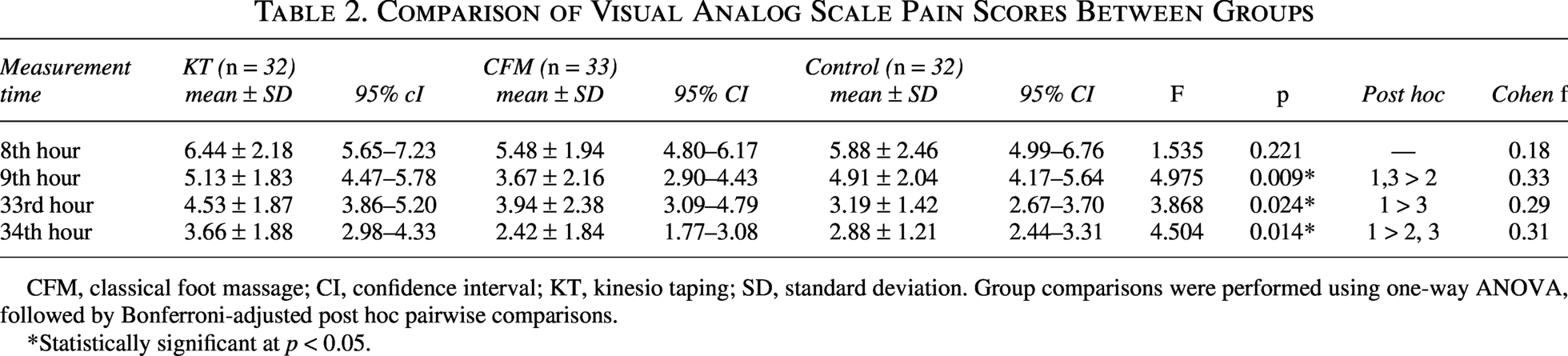
CFM, classical foot massage; CI, confidence interval; KT, kinesio taping; SD, standard deviation. Group comparisons were performed using one-way ANOVA, followed by Bonferroni-adjusted post hoc pairwise comparisons.
*Statistically significant at p < 0.05.
At 33rd (p = 0.024) and 34th hours (p = 0.014) postoperatively, VAS scores also differed significantly between groups (p < 0.05). Pairwise comparisons revealed that the KT group had significantly higher pain scores than both the CG and CFM groups at both time points. The effect size was moderate at both time points.
Comparison of secondary outcomes among intervention groups and the control group
Two subdimensions were defined for the VAS-F. First, a significant difference was detected between the groups in the pretest 8th-hour measurements of the Fatigue subdimension. This difference was found to be higher in the KT group (p = 0.001). However, no significant difference was detected between the groups in the 34th hour measurements (p = 0.332).
The second subdimension for VAS-F is the Energy subdimension. There was a significant difference between the groups in the pretest 8th and 34th hour measurements in the Energy subdimension (p < 0.05). While the CFM group had significantly higher scores than the control group at the 8th postoperative hour (p = 0.026), the KT group demonstrated significantly higher scores than the CG at the 34th postoperative hour (p = 0.034) (Table 3).
Comparison of Fatigue (Visual Analog Scale–Fatigue) and Mood (Brief Mood Introspection Scale) Scores Between Groups
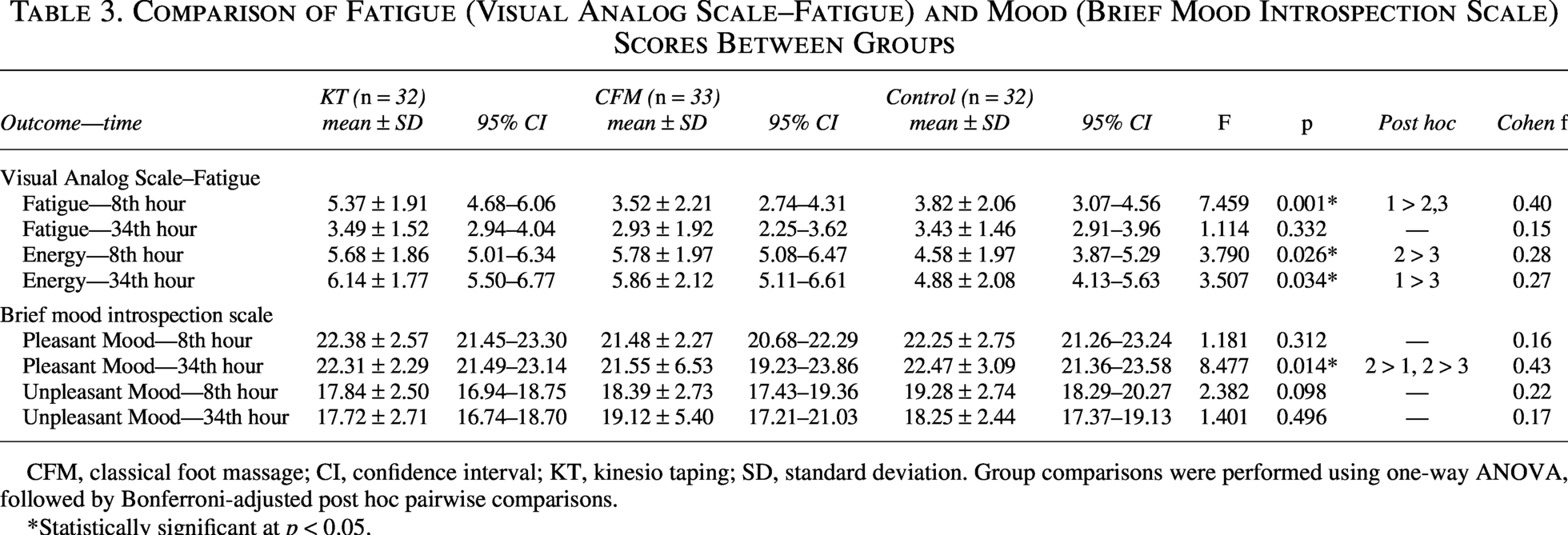
CFM, classical foot massage; CI, confidence interval; KT, kinesio taping; SD, standard deviation. Group comparisons were performed using one-way ANOVA, followed by Bonferroni-adjusted post hoc pairwise comparisons.
*Statistically significant at p < 0.05.
Two subdimensions were defined for the BMIS. The first of these dimensions is the “Pleasant subdimension.” No significant difference was found between the groups in the 8th-hour measurement of the Pleasant subdimension of the BMIS (p = 0.596). However, at the 34th hour, a statistically significant difference was detected between the groups (p = 0.031). The CFM group demonstrated significantly higher Pleasant subdimension compared with both the KT and CG groups.
The second subdimension of the BMIS is the “Unpleasant subdimension.” No statistically significant difference was found in the intergroup comparisons in the “Unpleasant subdimension” scores measured at postoperative 8th (p = 0.098) and 34th hours (p = 0.496).
Safety outcomes
The study remained free from any complications requiring termination or adverse postoperative clinical conditions. Regarding the specific methods used, in the KT group, no adverse events related to the KT application, such as skin irritation, erythema, or allergic reactions, were reported. In the CFM group, participants were evaluated for application tolerance; three participants reported a mild and transient tingling/tickling sensation at the beginning of the application. This resolved spontaneously without requiring any medical intervention and did not lead to termination of the procedure. In conclusion, both procedures were well tolerated by the participants; no clinically significant safety risks or serious adverse events related to the procedure were identified during the study period.
Discussion
Pain
The findings of this study show that among nonpharmacological interventions applied in the early and mid-postoperative period after cesarean section, CFM has a more significant advantage in pain management. When intergroup comparisons were examined, it was found that the CFM group had significantly lower pain scores compared to the KT and control groups, especially in the 9th, 33rd, and 34th hour VAS measurements. This result is consistent with the gate control theory, which states that massage application suppresses pain transmission by stimulating peripheral mechanoreceptors and reduces pain perception via the central nervous system. 5 Studies in the literature reporting that hand–foot massage and deep tissue massage applied in the postcesarean period significantly reduce pain also support these findings.2,9,18,19
KT has been reported to have positive effects on pain management in pregnancy and the postpartum period, and this is stated to be related to mechanisms such as proprioceptive feedback, reduction of facial tension, and regulation of muscle tone.1,20–22 However, in the current study, the KT group did not show a significant superiority compared to the CFM group and obtained values close to the control group at some measurement times. This suggests that despite the theoretical mechanisms of KT, its practical clinical effectiveness may not be as strong as CFM. Therefore, the results of the study indicate that CFM may be a more effective complementary approach to KT in postcesarean pain management.
Fatigue
This study compared the Fatigue and Energy subscales of the VAS-F scale to assess the physical well-being of mothers in the postcesarean period. The findings show a significant difference between the groups in terms of the Fatigue subscale at the 8th hour postsurgery, with the KT group having higher fatigue scores compared to the other groups. This result suggests that KT application does not provide a significant advantage in reducing fatigue in the early postoperative period. However, the disappearance of the difference between the groups at the 34th hour indicates that the interventions do not create a significant and lasting superiority in long-term fatigue levels. Postoperative fatigue is known to be associated with many factors, including postpartum bleeding, low hemoglobin levels, infection, sleep problems, stress, anxiety, pain at the incision site, breastfeeding problems, and depression. 23 Therefore, it is considered difficult for a single intervention to determine the entire fatigue experience.
When the energy subscale was examined, it was determined that the CFM group had a higher energy level than the control group at the 8th hour postsurgery, and at the 34th hour, the KT group reached higher energy scores than the CG. However, the limited differences between the groups at both time points and the similarity of the values in all groups indicate that the applied interventions did not have a strong and decisive superiority on the energy level. Nevertheless, it is consistent with studies in the literature reporting the positive effects of massage applications on physical well-being and relaxation2,9,18,19 that CFM application, in particular, can positively support energy perception by providing short-term physiological and psychological relief through tactile stimulation and relaxation.
Mood
It is noteworthy that the CFM group had higher scores in the Pleasant Mood subscale compared to other groups in the mood results. Massage is known to activate the parasympathetic nervous system through tactile stimulation, providing relaxation and emotional relief. The literature reports that hand and foot massage and deep tissue massage reduce anxiety and support emotional well-being in mothers.2,18,24 It is also stated that cesarean delivery may increase the risk of postpartum depression and that nonpharmacological supportive approaches may play an important role in reducing this risk. 25 In this context, it can be said that CFM can be considered as a complementary intervention that supports emotional well-being.
Limitations
The fact that the interventions are limited only to the hospital stay does not reveal the long-term effects of the interventions. Although the application has a randomized controlled experimental study design, pain perception, psychosocial status, and previous life experiences may affect the intervention results. Since the sample consisted of women who applied to a hospital for cesarean delivery, the results are limited to this sample group. Therefore, the results cannot be generalized. Although breastfeeding conditions are standardized, the potential analgesic effect of oxytocin released during breastfeeding has not been directly evaluated. Future studies evaluating the interaction between oxytocin-mediated responses and postpartum pain outcomes are recommended.
Conclusion
The findings of this randomized controlled trial, conducted in the early postoperative period after cesarean delivery, show that CFM is associated with lower scores in reducing pain intensity at specific time points compared to the KT and control groups. However, the observed effects are limited to short-term measurements and vary across time points. The effect of KT on pain management appears to be more limited compared to CFM.
Findings regarding secondary outcomes such as fatigue, energy level, and mood suggest that the effects of the interventions are time dependent and limited. Although higher energy and more positive mood scores were observed at some time points in the CFM and KT groups, these findings differed across all measurement time points.
While the fact that neither intervention evaluated in this study resulted in serious side effects supports the applicability of these approaches, caution should be exercised in directly generalizing these findings to clinical practice. The findings suggest that CFM has potential as a complementary approach to pain management in the early postcesarean period, but the magnitude and persistence of this effect need to be confirmed by larger samples and multicenter studies.
In conclusion, this study provides preliminary evidence on the potential role of nonpharmacological interventions in postcesarean symptom management, and stronger evidence is needed before making definitive recommendations for their integration into clinical practice.
Authors’ Contributions
All authors made substantial contributions to the conception of this article. K.G.: Conceptualization, methodology, investigation, data curation, formal analysis, writing—original draft, supervision, and project administration. Ş.C.: Methodology, investigation, data curation, writing—review and editing. All authors read and approved the final article.
Ethics Statement
Ethical permission was obtained for the study from the Non-Interventional Clinical Ethics Committee of a University in the province where the study was conducted. (Decision number: 477-477-24, Date: November 7, 2024). In addition, legal permissions were obtained for the study permit from the hospital where the study was conducted (Decision number: E-45786011-799-257839961, Date: October 25, 2024). The study was conducted in accordance with the Declaration of Helsinki. Participants signed an informed consent form before being included in the study. The clinical protocol of the study was registered with the ClinicalTrials.gov system with the registration number NCT06811285 on January 31, 2025.
Data Availability Statement
All data generated or analyzed during this study are available in this study. For more information, please contact the authors.
Footnotes
Acknowledgments
The authors would like to thank all the participants who carried out the participant recruitment process.
Author Disclosure Statement
There are no conflicts of interest among the authors of this study.
Funding Information
This research received no specific grant from any public, commercial, or not-for-profit funding agency.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.