
Abstract
Background:
Research examining at-risk substance use by disability status is limited, with little investigation into differences by disability type. We investigated binge drinking and prescription opioid misuse among adults with and without disabilities, and by type of disability, to inform need for assessment and intervention within these populations.
Methods:
Secondary analyses of adults who completed the disability, alcohol, and prescription opioid misuse items in the 2018 Ohio, Florida, or Nebraska Behavioral Risk Factor Surveillance System surveys (n = 28 341), the only states that included prescription opioid misuse in 2018. Self-reported disability status (yes/no) relied on 6 standardized questions assessing difficulties with: vision, hearing, mobility, cognition, self-care, and independent living (dichotomous, nonmutually exclusive, for each disability). Logistic regression models estimated the association of disability status and type with (1) past 30-day binge drinking and (2) past-year prescription opioid misuse. Additional models were restricted to separate subsamples of adults who: (a) currently drink, (b) received a past-year prescription opioid, and (c) did not receive a past-year prescription opioid.
Results:
One-third reported at least one disability, with mobility (19.5%), cognitive (11.5%), and hearing (10.2%) disability being the most common. Disability status was associated with lower odds of binge drinking (adjusted odds ratio [AOR] = 0.74, 95% confidence interval [CI] 0.68-0.80, P ≤ .01). However, among adults who currently drink, people with disabilities had higher odds of binge drinking (AOR = 1.11, 95% CI 1.01-1.22, P ≤ .05]. Disability was associated with higher odds of past-year prescription opioid misuse (AOR = 2.51, 95% CI 2.17-2.91, P ≤ .01).
Conclusions:
Adults with disabilities had higher odds of prescription opioid misuse, and among adults who currently drink, higher odds for binge drinking were observed. The magnitude of the association between disability status and prescription opioid misuse was particularly concerning. Providers should be trained to screen and treat for substance use problems for people with disabilities.
Highlights
Adults with disabilities had lower odds of binge drinking overall; yet among people who currently drink, they had 11% higher odds of binge drinking, compared to people without disabilities.
Adults with disabilities had 151% higher odds of prescription opioid misuse, compared to people without disabilities.
Adults with vision or cognitive disabilities had higher odds for both binge drinking (among people who currently drink) and prescription opioid misuse.
Substance use treatment settings should incorporate appropriate accommodations for people with disabilities.
Introduction
Although research to date has raised awareness of the complexity of the relationship between disability and at-risk substance use, a nuanced understanding is lacking.1,2 Several recent studies have shed some light on this area, including a nationally representative study of adults from the 2020 National Alcohol Survey, which found that current drinking was less likely among people with a disability compared to those without. 3 However, among people who currently drink, people with disabilities were significantly more likely to report high-intensity drinking days (ie, 8+ drinks/day). 3 Yet, disability status was no longer significant when adjusting for demographics, clinical characteristics, and chronic pain. In the same study, 3 people with disabilities were significantly more likely to have misused a prescription drug in the past year compared to people without disabilities after controlling for covariates. Their disability definition was limited to just 3 items included on the survey (ie, self-report of at least one of the following: serious difficulty with vision or hearing, receipt of Medicare if under age 65, or reporting being disabled on the employment item) and did not capture a broader range of functional disability. Self-reported chronic pain was associated with these substance use patterns, 3 which has been reported as a reason for opioid misuse among persons with disabilities.4-6 Another study using the 2017 National Survey on Drug Use and Health (NSDUH) found that college students with a disability had nearly twice the odds of misusing prescription pain medications compared to college students without disabilities. 7
There have been multiple and inconsistent reports of at-risk substance use and/or substance use disorder in subpopulations of people with specific disabilities. Studies of deaf and hard-of-hearing adults are inconclusive regarding an association between this type of disability and at-risk substance use.8-10 Greater alcohol use among people with intellectual and developmental disabilities may be present at younger ages but not later in life.11-13 Among people who have experienced traumatic brain injury (TBI), substance use routinely declines in the short term following injury, yet often increases over time. 14 People with spinal cord injury have a similar pattern. 15
However, these studies of single disability types have not allowed for a nuanced understanding about potential differences between disability subpopulations, which may inform the complex relationships of at-risk substance use and disability. A study using 2015 to 2017 NSDUH data compared prescription opioid misuse and disorder across 6 types of disability (ie, vision, hearing, mobility, cognition, self-care, or independent living). 4 Prescription opioid misuse ranged from 2.6% to 6.9%, and prescription opioid use disorder ranged from 1.0% to 3.0%; yet, due to limited sample size, this study did not examine the association between disability type with prescription opioid outcomes in multivariate models. Another study using 2015 to 2019 NSDUH data found that adults with disabilities had higher prevalence of marijuana use compared to adults without disabilities; and adults with vision disability only or cognitive disability only had higher odds of marijuana use compared to adults without disabilities. 16 These types of analyses are informative for screening and treatment efforts for people with disabilities.
In the current study, we sought to examine the association of 6 types of self-reported functional disability (vision, hearing, mobility, cognition, self-care, or independent living) with binge drinking and prescription opioid misuse, which have high potential for adverse consequences, including addiction, morbidity, and mortality. Specifically, we first investigated associations between having a disability (yes/no) with past 30-day binge drinking and past-year prescription opioid misuse. To address gaps in knowledge about potential differences between disability type and generate hypotheses to inform practice and future research, we then examined the associations of each disability type with the 2 at-risk substance use outcomes. Data were drawn from the Ohio, Florida, and Nebraska 2018 Behavioral Risk Factor Surveillance System (BRFSS) population-based surveys of noninstitutionalized adults. Findings should inform healthcare providers about the need to assess people with disabilities for problematic alcohol and prescription opioid misuse. Furthermore, this study is expected to provide evidence that there is need for assessment and interventions related to at-risk substance use that are accessible to and appropriate for people with disabilities, given that accommodations are often required to effectively support people with disabilities in healthcare and substance use treatment settings.
Methods
Sample
The BRFSS is an annual telephone-based (landline and mobile) household survey that is federally-funded and jointly-administered by the Centers for Disease Control and Prevention (CDC) and individual State Departments of Health. 17 BRFSS surveys include core questions used by all states, and optional modules that states may choose to include. The 2018 BRFSS was administered in each state to random samples of noninstitutionalized adults 18 years or older and contained demographic information and questions regarding alcohol use and disability status. The Ohio, Florida, and Nebraska surveys were selected for this study as they were the only 3 states in 2018 that included items in their state modules that corresponded to the definition of prescription opioid misuse used by the National Institute on Drug Abuse (NIDA). 18 A few other states had prescription opioid modules in 2018 but did not ask the same prescription opioid misuse items.
After combining data to create the 3-state sample, we excluded individuals with missing data for the disability items (n = 678) and sex (n = 9) as the binge drinking measure is sex-specific. We restricted our analytic sample to adults who completed all alcohol and prescription opioid use items needed to create our dependent variables. We excluded those with missing data for alcohol use (n = 1189; 759 of these adults also had missing prescription opioid items) and those with missing items for prescription opioid use (n = 5048), bringing the 3-state analytic sample to 28 341 (see Online Supplement Figure 1).
Measures
Dependent Variables
Past 30-day binge drinking (yes/no) was defined as self-report of having 5+ drinks on one occasion for men or 4+ for women, in the past 30 days, regardless of whether they reported currently using alcohol, consistent with the definition recommended by the National Institute on Alcohol Abuse and Alcoholism. 19 Additional analyses examined past 30-day binge drinking among a sample restricted to people who currently drink (ie, those who reported having at least one drink of any alcoholic beverage in the past 30 days; n = 13 688).
Past-year pain medication use (ie, prescription opioid use; yes/no) was constructed based on self-report of “using any pain medications prescribed to you by a healthcare provider in the past year.” Past year prescription opioid misuse (yes/no) was defined based on responses to the following items: (1) “The last time you filled a prescription for pain medication, did you use any of the pain medication more frequently or in higher doses than directed by a healthcare provider?” and (2) “In the past year, did you use prescription pain medication that was not prescribed to you?” Consistent with the NIDA definition and other research, 18 self-report of “yes” to at least one of these questions was categorized as prescription opioid misuse. 20 Additional analyses examined past-year prescription opioid misuse restricted to (a) those who reported past-year pain medication use, and (b) those who did not report past-year pain medication use.
Key Independent Variable
Disability status was based on responses to 6 standardized questions of serious difficulty or difficulty with:
vision (ie, are you blind or do you have serious difficulty seeing, even when wearing glasses);
hearing (ie, are you deaf or do you have serious difficulty hearing);
mobility (ie, do you have serious difficulty walking or climbing stairs);
cognition (ie, because of a physical, mental, or emotional condition, do you have serious difficulty concentrating, remembering, or making decisions);
self-care (ie, do you have serious difficulty dressing or bathing); and
independent living (ie, because of a physical, mental, or emotional condition, do you have difficulty doing errands alone such as visiting a doctor’s office or shopping), which measure functional disabilities resulting in part from societal barriers (eg, inaccessible environments).
These 6 questions were developed to be consistent with the World Health Organization’s International Classification of Functioning, Disability and Health and are recommended in the Department of Health and Human Services (DHHS) data collection standards for disability status.7,21,22 For our analyses, self-report determined the status for each disability type (yes/no for each of the 6 types), and having at least one disability type was classified as having a disability (yes/no). Positive responses to individual disability types were not mutually exclusive.
Covariates
Covariates included demographic variables: sex (female, male), age group (18-24, 25-34, 35-44, 45-54, 55-64, 65+), race and ethnicity (White/non-Hispanic; Black/non-Hispanic; and other [Hispanic, Asian, Native Hawaiian, Other Pacific Islander, American Indian, or Alaska Native]—collapsed to adhere to CDC suppression guidelines 23 for small sample sizes), and marital status (married, never married, or other [widowed, separated, a member of an unmarried couple]).
Because disability status correlates with increased disparities in income, education and employment opportunities, and mental health problems, and we wished to examine the full effect of having a disability on our outcomes, we did not include these as covariates in our main models.6,24 This methodology is informed by the Institute of Medicine Unequal Treatment definition of health disparities which separates needs-based disparities from true disparities,25-27 improving our ability to measure and understand health inequities.28-30 However, as sensitivity analyses, we replicated our logistic regression models, including 4 dichotomous variables that represent these domains (ie, annual income lower than $25 000 per year; completed a high school degree; employed; and reported 14+ days of mental health as not good in the past 30 days).
Statistical Analysis
BRFSS data include weights constructed by iterative proportional fitting to represent the noninstitutionalized adult population of each state. However, given our interest in the associations among disability status and the substance use outcomes, rather than epidemiological prevalence, we used unweighted data from the combined 3-state sample. There is no greater risk of bias in our use of unweighted data when reporting adjusted odds ratios (AORs) because the parameter being estimated would be the same for the weighted or unweighted data. 31 CDC cell suppression guidelines were followed, 23 where an estimate was suppressed when the relative standard error was greater than 30 or when the corresponding denominator was less than 50 respondents. Adhering to CDC suppression guidelines required us to collapse certain categories more broadly (eg, race and ethnicity).
We conducted bivariate chi-square tests to determine whether disability status, or each disability type, was significantly associated with the substance use variables. We conducted logistic regression models to estimate the association of disability status (yes/no) with the 2 dependent variables (ie, past 30-day binge drinking and past-year prescription opioid misuse), adjusted for the main covariates (ie, sex, age group, race and ethnicity, marital status). Additional logistic regression models estimated the association of disability status with binge drinking, restricted to those who reported any alcohol use in the past 30 days; and prescription opioid misuse, restricted to those who reported using a prescription opioid in the past year. Since respondents can also meet criteria for prescription opioid misuse by using someone else’s prescription opioid, we ran logistic regression models to estimate the association of past-year prescription opioid misuse, restricted to those who reported not using a past-year prescription opioid. This set of 5 models using overall disability status (yes/no) is referred to as Model 1 in the Results section and tables.
The set of 5 models was then repeated with separate dichotomous indicators for the 6 disability types (not mutually exclusive), replacing the indicator for overall disability status (referred to as Model 2). The results for each disability subgroup can be interpreted in comparison to adults without that type of disability (eg, adults with vision disability compared to adults without vision disability).
Sensitivity Analyses
For each of the 5 models for overall disability status, and by disability type, we replicated the analyses by also including the 4 dichotomous measures for income, education, employment, and poor mental health. This alternative specification allowed us to examine the residual association of disability status with the dependent variables when controlling for sociodemographic and mental health variables that are correlated with disability status.
We conducted additional analyses to examine the potential impact of our decision to limit the sample to respondents who completed both the alcohol and prescription opioid items. To do so, we first conducted bivariate analyses to assess whether adults excluded from the sample due to missing alcohol or prescription opioid data were significantly different from the adults included in the analysis based on study covariates. Following this, we conducted multinomial logistic models for the binge drinking and prescription opioid misuse outcomes on the full sample of adults (n = 34 578), with missing outcomes assigned to a separate category, rather than leading to deletion from the analyses.
We report the significance level and 95% confidence intervals (CIs) for the corresponding AORs. All analyses were completed in SAS version 9.4. SAS Institute Inc., Cary, NC, USA. The 3 datasets analyzed in this study were provided by the Ohio, Florida, and Nebraska Departments of Health with approved data use agreements. The Brandeis University Institutional Review Board determined that this study does not meet criteria for human subjects research as defined by the Common Rule (45 CFR46), because the data being analyzed are publicly available and de-identified. We obtained the 3 de-identified data sets directly from the states.
Results
Study Population
The sample was comprised mostly of females (56.7%) and people who self-identified as White/non-Hispanic (84.0%)—Table 1. Approximately 40% were age 65 or older. One-third (33.8%) reported a disability, with mobility (19.5%), cognitive (11.5%), and hearing (10.2%) disability being the most common. Just over half (51.7%) reported using alcohol in the past month and 13.2% reported past-month binge drinking. Over a quarter (27.6%) reported past-year prescription opioid use and 2.9% met criteria for past-year prescription opioid misuse. Compared to the analytic sample, adults who were excluded due to missing data for alcohol or prescription opioid items were significantly more likely to be male, Black/non-Hispanic, or other race or ethnicity, never married, and younger (ie, age 18-44; data not shown).
Characteristics, Disability Status, and Self-Reported Alcohol and Prescription Opioid Use Among Adults Within the 3-State Sample and by State, in 2018.
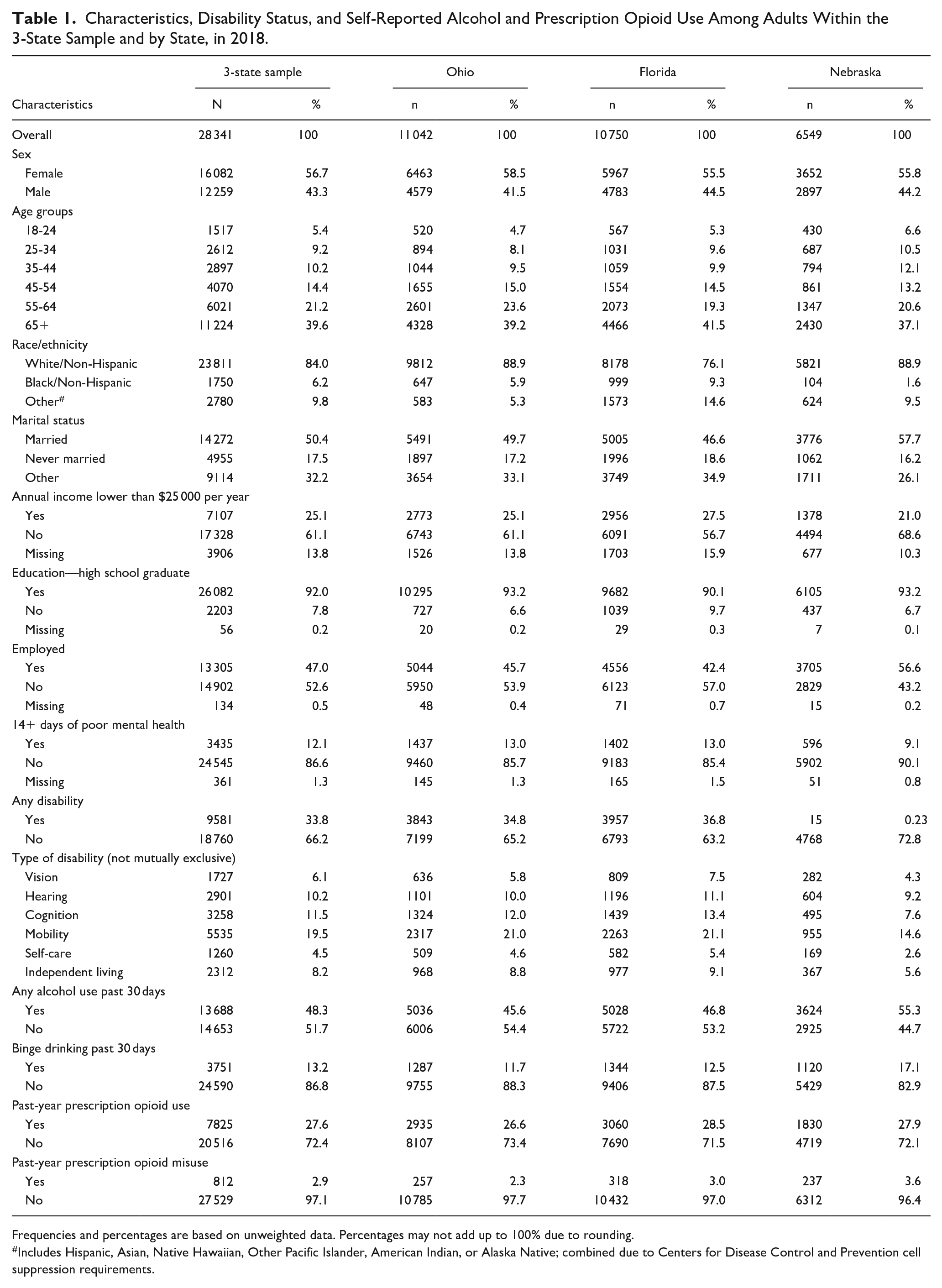
Frequencies and percentages are based on unweighted data. Percentages may not add up to 100% due to rounding.
Includes Hispanic, Asian, Native Hawaiian, Other Pacific Islander, American Indian, or Alaska Native; combined due to Centers for Disease Control and Prevention cell suppression requirements.
Bivariate Results
Adults with disabilities were significantly less likely to report past 30-day alcohol use (35.9% vs 54.6%, respectively) or binge drinking (9.1% vs 15.3%, respectively) compared to adults without disabilities—Table 2. Binge drinking varied by disability type, with adults with cognitive disabilities (11.9%) having the highest prevalence, and those with mobility disabilities (6.7%) having the lowest prevalence. People with disabilities were more likely to have an annual income less than $25 000 per year (39.4% vs 17.7%) and to report 14+ days of poor mental health in the past 30 days (23.7% vs 6.2%), and less likely to be employed (24.1% vs 58.6%) or have graduated from high school (87.3% vs 94.4%), compared to people without disabilities (see Online Appendix Table 2).
Bivariate Associations Between Disability Status (Any and by Type) With Alcohol Use and Prescription Opioid Use Behaviors Among Adults in the 3-State Sample in 2018 (n = 28 341).
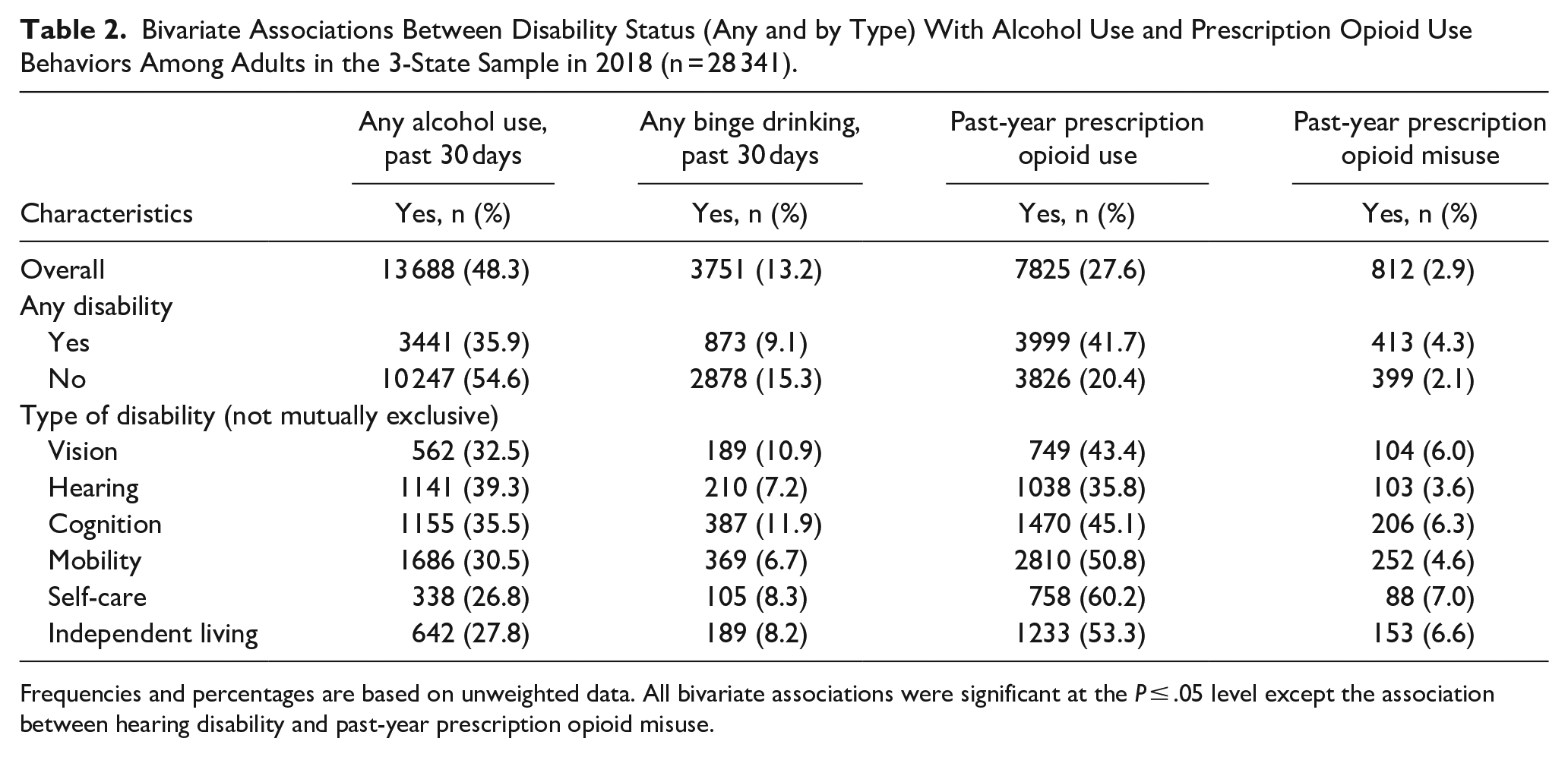
Frequencies and percentages are based on unweighted data. All bivariate associations were significant at the P ≤ .05 level except the association between hearing disability and past-year prescription opioid misuse.
Adults with disabilities were significantly more likely to report past-year prescription opioid use (41.7% vs 20.4%, respectively) or prescription opioid misuse (4.3% vs 2.1%, respectively) compared to adults without disabilities. Prescription opioid misuse varied by disability type, with adults with self-care, independent living, cognition, and vision disabilities having the highest prevalence (6%-7%).
Logistic Regression Results
Controlling for covariates, disability status was significantly associated with lower odds of past 30-day binge drinking (AOR = 0.74; 95% CI 0.68-0.80)—Table 3. Adults with hearing, mobility, or independent living disabilities each had significantly lower odds of binge drinking compared to adults without those types of disabilities. When the sample was restricted to people who currently drink, disability status was associated with significantly higher odds of past 30-day binge drinking (AOR = 1.11; 95% CI 1.01-1.22). This association varied by disability type. Compared to adults without the specific disability type, currently drinking adults with hearing disabilities (AOR = 0.77; 95% CI 0.65-0.91) continued to have significantly lower odds for past month binge drinking; while currently drinking adults with vision (AOR = 1.48; 95% CI 1.21-1.81) and cognitive (AOR = 1.20; 95% CI 1.03-1.39) disabilities had significantly higher odds for past 30-day binge drinking.
Characteristics Associated With Binge Drinking Among Adults in 3-State Sample, by Disability Status, AORs, and 95% CIs.
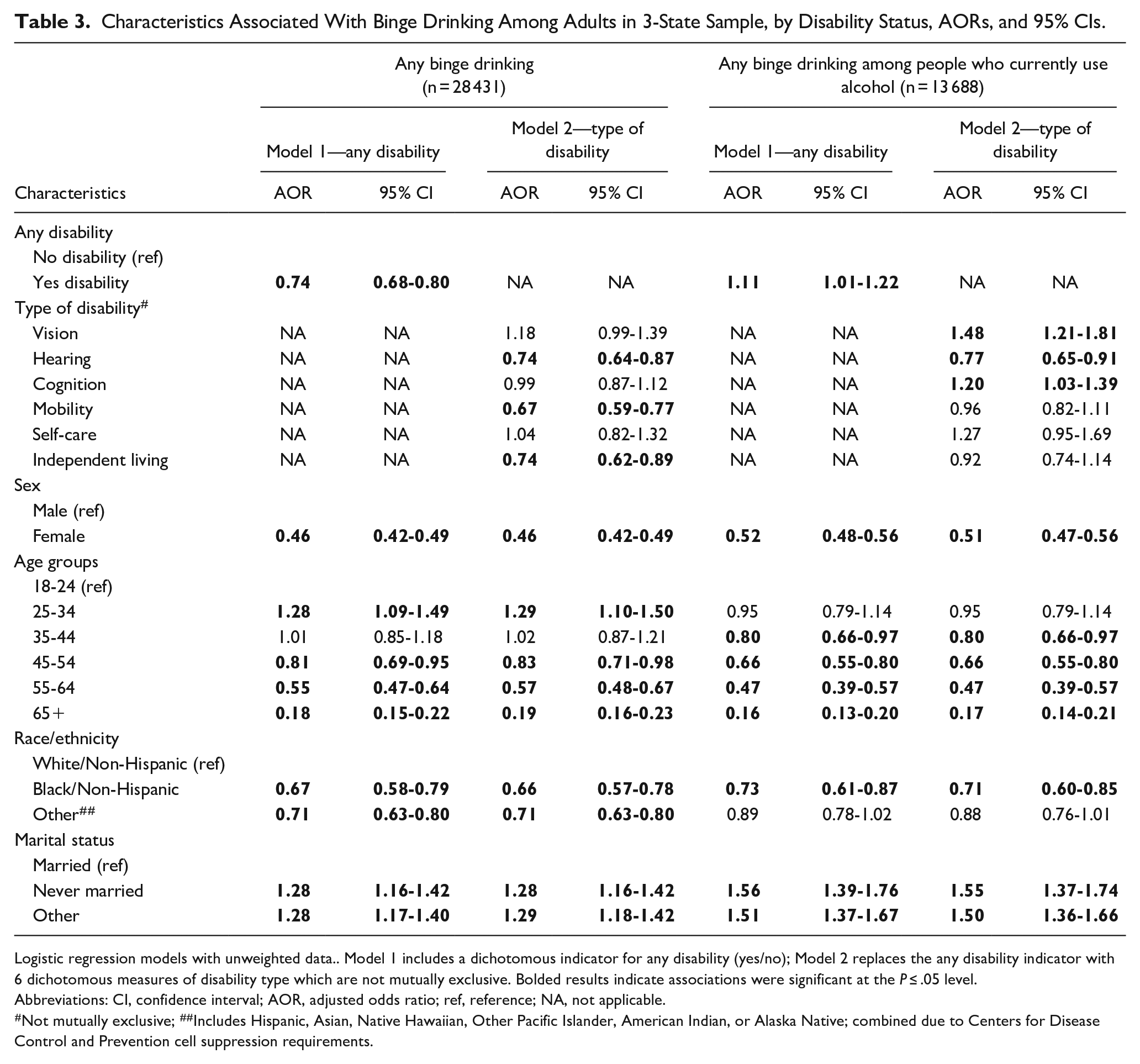
Logistic regression models with unweighted data.. Model 1 includes a dichotomous indicator for any disability (yes/no); Model 2 replaces the any disability indicator with 6 dichotomous measures of disability type which are not mutually exclusive. Bolded results indicate associations were significant at the P ≤ .05 level.
Abbreviations: CI, confidence interval; AOR, adjusted odds ratio; ref, reference; NA, not applicable.
Not mutually exclusive;
Includes Hispanic, Asian, Native Hawaiian, Other Pacific Islander, American Indian, or Alaska Native; combined due to Centers for Disease Control and Prevention cell suppression requirements.
Controlling for covariates, disability status was significantly associated with higher odds of past-year prescription opioid misuse (AOR = 2.51; 95% CI 2.17-2.91)—Table 4. Adults with mobility, cognition, vision, and independent living disability had significantly higher odds of prescription opioid misuse (AOR range 1.47-1.69). When the sample was restricted to those who reported any past-year prescription opioid use, the odds for disability status were attenuated, yet disability remained significantly associated with higher odds of opioid misuse (AOR = 1.69; 95% CI 1.38-2.08). When examining disability type in restricted models, only those with cognitive (AOR = 1.52; 95% CI 1.20-1.93) or vision (AOR = 1.36; 95% CI 1.02-1.83) disabilities had significantly higher odds for prescription opioid misuse.
Characteristics Associated With Past-Year Prescription Opioid Misuse Among Adults in 3-State Sample, by Disability Status, AORs, and 95% CIs.
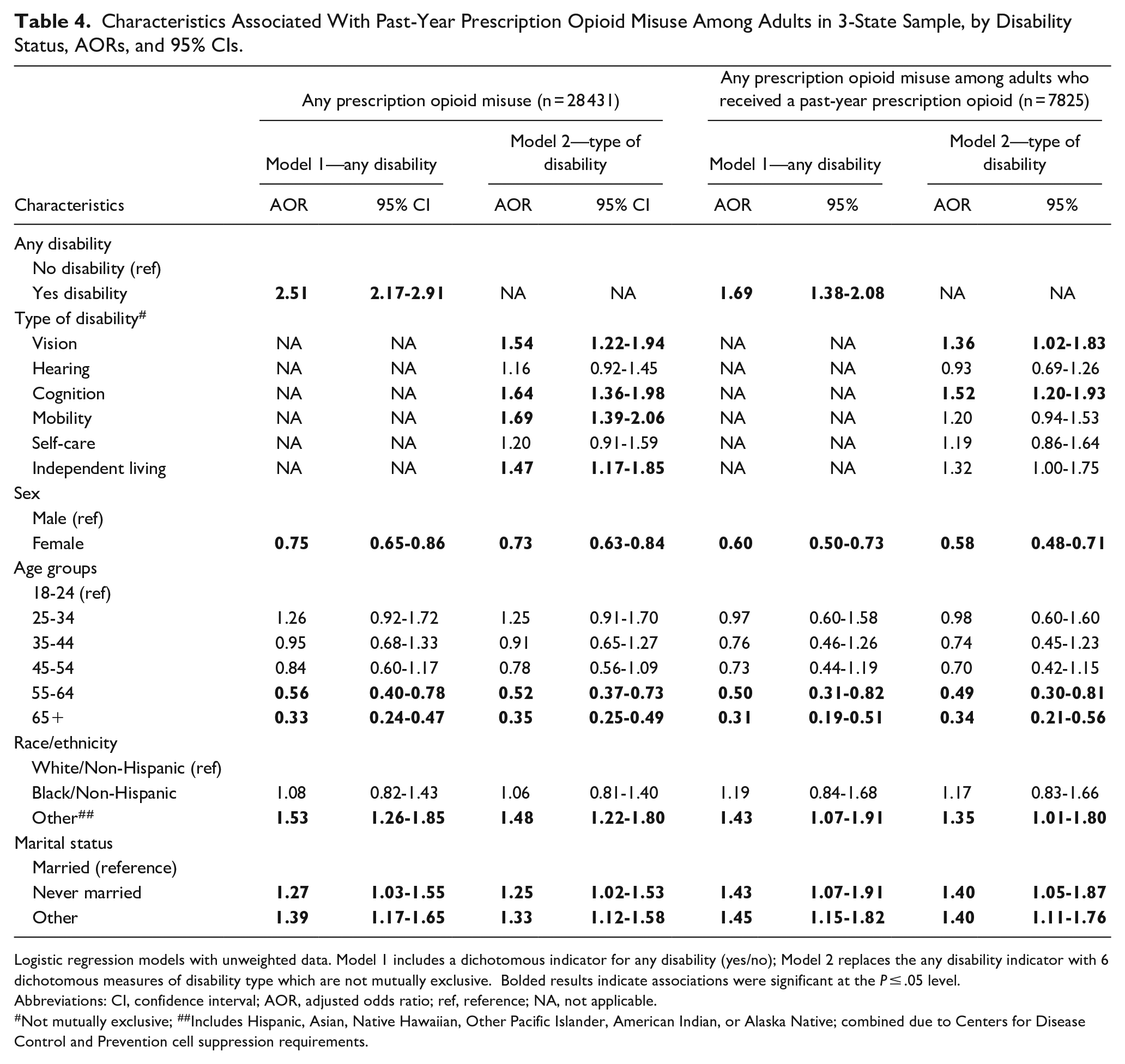
Logistic regression models with unweighted data. Model 1 includes a dichotomous indicator for any disability (yes/no); Model 2 replaces the any disability indicator with 6 dichotomous measures of disability type which are not mutually exclusive. Bolded results indicate associations were significant at the P ≤ .05 level.
Abbreviations: CI, confidence interval; AOR, adjusted odds ratio; ref, reference; NA, not applicable.
Not mutually exclusive;
Includes Hispanic, Asian, Native Hawaiian, Other Pacific Islander, American Indian, or Alaska Native; combined due to Centers for Disease Control and Prevention cell suppression requirements.
In the models restricted to adults who reported not receiving a prescription opioid in the past year (n = 20,516), (see Online Appendix Table 1), disability status remained significantly associated with higher odds of prescription opioid misuse (AOR = 2.26; 95% CI 1.81-2.82). Similarly, adults who reported not receiving a prescription opioid in the past year with vision, hearing, mobility, or cognitive disabilities had significantly higher odds of prescription opioid misuse compared to people without those types of disabilities.
Sensitivity Analyses
When we replicated our logistic regression models (yes/no) by including the 4 dichotomous measures for income, education, employment, and poor mental health, the AORs for the any disability variable were attenuated slightly, yet remained significant with the exception of the binge drinking model restricted to current alcohol users, where this variable became not significant (AOR = 1.05; 95% CI 0.94-1.17; see Online Appendix Table 3). In the corresponding disability type models, the AORs for each disability type were attenuated slightly but did not change in direction. For a few specific disability indicators, the AOR changed from significant to not significant or vice versa, particularly where the AOR in the main models was very close to 1.00, but these changes were minimal and rare (Online Appendix Table 4).
In our alternative multinomial logistic analyses, which expanded the sample to include all adults, with missing outcomes as separate categories, estimates of the association of disability status overall, and by type, did not change in significance or direction, with 1 exception. Using the full sample, the multinomial logistic model of any binge drinking found that the vision disability indicator became significant (AOR = 1.20, 95% CI 1.03-1.39; data not shown).
Discussion
Our study findings suggest that disability status should not be overlooked when considering risk for binge drinking, and in particular, for prescription opioid misuse. We examined the association between self-reported disability status, based on 6 self-reported functional limitations recommended for inclusion in US surveys, 24 with binge drinking and prescription opioid misuse behaviors among a 3-state sample of noninstitutionalized adults in 2018. We found that disability status, and in most cases each disability type, was associated with the substance use measures; however, the direction and magnitude of effect varied by substance use behavior and by type of disability.
When adjusting for select demographics, disability status was significantly associated with lower odds of past 30-day binge drinking. However, and most important, when analyses were restricted to people who currently drink, findings reversed directions; people with disability had 11% higher odds for binge drinking compared to adults without disability. The magnitude of effect for the association between disability status and prescription opioid misuse was more concerning. In adjusted models, people with disability had 151% higher odds for prescription opioid misuse. Disability status remained significantly associated with prescription opioid misuse in our conditional analyses which first restricted to adults prescribed a past-year prescription opioid, and then to adults who did not receive a past-year prescription opioid. The latter analysis captures adults who reported prescription opioid misuse by using someone else’s prescription opioid.
While slightly attenuated, results for any disability (yes/no) remained significant even when additionally controlling for variables generally associated with disability status (ie, income, education, employment, and poor mental health). The one exception was that disability status was not significant in the binge drinking model restricted to current alcohol users, which may have been in part related to the reduction in sample size due to missing data with the addition of the 4 covariates. Given the differences in these measures by disability status, the robust results with and without their inclusion adds confidence that these at-risk substance use behaviors are associated with disability status. These findings emphasize the need to better assess people with disabilities for risky alcohol use and prescription opioid misuse.
An innovation of our study was investigation into whether substance use behaviors varied by disability type. In general, the associations between each disability type with the at-risk substance use behaviors were in the same direction as the any disability models, yet usually somewhat attenuated, and varied by type. When we restricted the analyses to people who currently drink, adults with vision and cognitive disabilities were more likely to report binge drinking compared to adults without those types of disabilities. Similarly, a study 3 using the 2020 National Alcohol Survey found that when restricting analyses to people who currently drink, adults with vision, hearing, and mobility disabilities each had higher odds of high-intensity drinking (ie, drinking 8+ drinks in a day), compared to adults without these types of disabilities. While our study and theirs used slightly different assessments of disability (eg, cognitive disability was not included in their study) and high-risk drinking, these converging results suggest that, once drinking, there are subgroups of people with disabilities that may be more vulnerable for high-risk drinking. Adults with vision disabilities who use alcohol may be at high risk as this subgroup had significantly elevated risk in both studies. While previous research is limited, studies suggest that substance use disorders may be elevated among people with vision impairment, and have posited that alcohol may be used to self-medicate or cope.32-34 Previous research has also found that adults with TBI are at increased risk for binge drinking, 35 a population likely represented in the cognitive disabilities subgroup in our study. Additional understanding of what disability subgroups are particularly vulnerable to excessive drinking would improve our ability to engage in targeted assessment and intervention efforts.
We also found that adults with certain types of disabilities had increased odds for prescription opioid misuse (ie, those with mobility, cognition, vision, and independent living disabilities), ranging from 47% higher odds (independent living) to 69% higher odds (mobility) compared to adults without those disabilities. When stratifying the prescription opioid misuse models by past-year prescription opioid use status, adults with vision and cognitive disabilities had higher odds for prescription opioid misuse in both models. Adults with hearing and mobility disabilities were at elevated odds for prescription opioid misuse only in the sample that did not receive a past-year prescription opioid, suggesting that these subgroups may be more likely to use someone else’s prescription opioids. These results support findings from other studies which found that people with hearing disabilities were at higher risk for substance use disorders including prescription opioid use disorder 36 and opioid use disorder-related emergency department visits 5 ; and people with spinal cord injury (likely included in the mobility subgroup) had higher odds of substance use disorders including almost 8 times the odds of having opioid use disorder. 37 In addition, evidence has been mounting that persons with TBI are at increased risk for prescription opioid misuse.6,20,38,39
Our study did not account for mental health comorbidities or chronic pain (not captured on BRFSS), both of which may be disproportionately elevated among people with disability,3,4,6,38,40 and may also increase risk for binge drinking and prescription opioid use as a potential pathway to opioid misuse.1,3,4 Some studies have found that persons with disabilities are at increased risk for adverse opioid-related outcomes,3-5 yet once pain and/or mental health conditions were controlled for, these associations were no longer significant. However, even if the heightened odds for adverse alcohol and opioid-related consequences is in part due to increased risk for pain and mental health comorbidities among persons with disabilities, the pervasiveness of chronic pain and mood disorders among people with disabilities suggests that disability status is of critical importance to understand as we try to reduce substance use-related morbidity and mortality.
Study findings have implications for the need to assess people with disabilities for at-risk substance use and to ensure access to treatment when warranted. As demonstrated here, people with disabilities who use alcohol and prescription opioids are more likely to use in risky ways. While this alone is not an indicator of a substance use disorder requiring treatment, both binge drinking and prescription opioid misuse would lead to a positive screening result on the single alcohol and drug screening questions that are recommended for use by healthcare providers,41,42 which indicate the need for more in-depth screening and brief intervention and referral to treatment if needed. 43 Due to abelism, healthcare providers may incorrectly assume that people with disabilities do not use substances,2,44 and may not screen for substance use. Such misunderstanding can be detrimental to the well-being of people with disabilities, given our findings of increased at-risk use. Healthcare providers should take a universal approach to screening for risky alcohol use, and misuse of prescription opioid medications, which would help reduce assumptions about people with disabilities. When indicated, providers should also conduct brief interventions for people with disabilities, as they would for people without disabilities, and refer to specialty substance use treatment as needed.
When disability is visible (eg, mobility impairment), stigma regarding expectations and capabilities may affect treatment access and completion. When disability is less apparent (eg, cognitive difficulties), treatment may not be attuned to differences in how a person communicates, learns, or pays attention, which in turn can undermine the therapeutic alliance and lead to premature termination. 45 Attention to the need for accommodations is essential for quality of care for people with disabilities, and should be incorporated into universal design approaches that include multiple methods of communication. Health and healthcare disparities are commonly experienced by people with disabilities, 46 and this is true in substance use treatment as well.43,46 Accomodations are needed within the substance use treatment system to ensure that people with disabilities can be adequately treated, and to reduce stigma related to disability.2,46,47 These accommodations are likely to span standard approaches (eg, group therapy), expectations for participation, learning styles, materials used, and consequences for apparent lack of engagement. 2 With these efforts, people with disabilities should have greater likelihood of succeeding in substance use treatment when warranted.
Limitations and Strengths
As with all studies, ours has limitations. Disability status was based on self-report and was not confirmed with a clinical diagnosis. However, use of the standard 6 disability items captures the approach recommended in the Americans with Disability Act and by DHHS, although it has been criticized for not capturing all people with mental disorders or intellectual disabilities. 24 Binge drinking and prescription opioid misuse behaviors were captured via self-report and may have been vulnerable to social desirability bias. Yet, BRFSS assures confidentiality; furthermore, participants were not asked to self-identify as having “misused” opioids because the word misuse is not included in the screening items. 20 Because the data are cross-sectional, we do not know whether the disability preceded the substance use outcomes; at-risk substance use can be a risk factor for certain types of disability (eg, spinal cord injury, TBI).35,48 The sample included a high proportion of people aged 65 years or older, who are more likely to have functional disabilities and less likely to have at-risk substance use, 49 and are more likely to respond to household surveys. 50
Future research is warranted with larger and more diverse population-based US samples. Creating the “other” race and ethnicity category to adhere to CDC suppression guidelines for small sample sizes likely masked important differences between subpopulations. Selection bias may have been an issue due to missing data on the alcohol and prescription opioid variables, which disproportionately omitted adults who were male, Black/non-Hispanic, or other race or ethnicity, never married, and younger. However, our findings in the restricted sample held in multinomial models that included all participants. Our findings do not generalize to other populations at risk for both disability and excessive substance use that would not have been included in a household survey (eg, homeless individuals, incarcerated populations, some people with severe disabilities).
Because our study predated the COVID-19 pandemic, it will be important to replicate these analyses with data from the early years of the pandemic and following the expiration of the federal public health emergency for COVID-19 in May 2023. Studies from the early years of the pandemic have found that adults with disabilities were more likely to report new or increased substance use compared to adults without disabilities.51,52
Despite these limitations, this study brings several strengths. We were able to bring enhanced focus on at-risk use of alcohol and prescription opioids, which have significant potential for morbidity and mortality. Our analytic approach allowed a nuanced examination of how people were using the substances (eg, with their own prescription or another person’s prescription) and delineated the different vulnerability for binge drinking when limited to people who currently drink. Furthermore, our analytic approach was strengthened by our adoption of the Institute of Medicine’s definition for identifying health disparities distinct from needs-based differences. Examining types of disability allows an understanding of which populations may be of greater concern.
Conclusions
Recognition that disability is a source of health disparity, driven in part by social determinants of health,24,53,54 underscores the need to better understand at-risk substance use and substance use disorders in this population. Persons with disabilities had higher odds of prescription opioid misuse, and if they used alcohol, higher odds for binge drinking. The magnitude of effect for the association between disability status and prescription opioid use was particularly concerning. General statements about the prevalence of co-occurring disability and at-risk substance use should be offered with caution due to the complex interactions of subgroups of people with disabilities and the substances used. 1 Our findings emphasize the need for broad prevention, assessment, and intervention efforts that are accessible to people across disability types.
Supplemental Material
sj-docx-1-saj-10.1177_29767342241236027 – Supplemental material for Association of Disability Status and Type With Binge Drinking and Prescription Opioid Misuse Among Adults From a 3-State Sample
Supplemental material, sj-docx-1-saj-10.1177_29767342241236027 for Association of Disability Status and Type With Binge Drinking and Prescription Opioid Misuse Among Adults From a 3-State Sample by Rachel Sayko Adams, John D. Corrigan, Grant A. Ritter, Zoe A. Pringle, Galina Zolotusky, Rachel Blayney and Sharon Reif in Substance Use & Addiction Journal
Supplemental Material
sj-docx-2-saj-10.1177_29767342241236027 – Supplemental material for Association of Disability Status and Type With Binge Drinking and Prescription Opioid Misuse Among Adults From a 3-State Sample
Supplemental material, sj-docx-2-saj-10.1177_29767342241236027 for Association of Disability Status and Type With Binge Drinking and Prescription Opioid Misuse Among Adults From a 3-State Sample by Rachel Sayko Adams, John D. Corrigan, Grant A. Ritter, Zoe A. Pringle, Galina Zolotusky, Rachel Blayney and Sharon Reif in Substance Use & Addiction Journal
Supplemental Material
sj-docx-3-saj-10.1177_29767342241236027 – Supplemental material for Association of Disability Status and Type With Binge Drinking and Prescription Opioid Misuse Among Adults From a 3-State Sample
Supplemental material, sj-docx-3-saj-10.1177_29767342241236027 for Association of Disability Status and Type With Binge Drinking and Prescription Opioid Misuse Among Adults From a 3-State Sample by Rachel Sayko Adams, John D. Corrigan, Grant A. Ritter, Zoe A. Pringle, Galina Zolotusky, Rachel Blayney and Sharon Reif in Substance Use & Addiction Journal
Supplemental Material
sj-docx-4-saj-10.1177_29767342241236027 – Supplemental material for Association of Disability Status and Type With Binge Drinking and Prescription Opioid Misuse Among Adults From a 3-State Sample
Supplemental material, sj-docx-4-saj-10.1177_29767342241236027 for Association of Disability Status and Type With Binge Drinking and Prescription Opioid Misuse Among Adults From a 3-State Sample by Rachel Sayko Adams, John D. Corrigan, Grant A. Ritter, Zoe A. Pringle, Galina Zolotusky, Rachel Blayney and Sharon Reif in Substance Use & Addiction Journal
Supplemental Material
sj-docx-5-saj-10.1177_29767342241236027 – Supplemental material for Association of Disability Status and Type With Binge Drinking and Prescription Opioid Misuse Among Adults From a 3-State Sample
Supplemental material, sj-docx-5-saj-10.1177_29767342241236027 for Association of Disability Status and Type With Binge Drinking and Prescription Opioid Misuse Among Adults From a 3-State Sample by Rachel Sayko Adams, John D. Corrigan, Grant A. Ritter, Zoe A. Pringle, Galina Zolotusky, Rachel Blayney and Sharon Reif in Substance Use & Addiction Journal
Footnotes
Author Contributions
RSA and SR originated the project and obtained funding. RSA, JDC, ZAP, RB, and SR drafted the initial manuscript. RSA, SR, GZ, and GAR secured the data and conducted the analyses. All authors participated in interpreting the results, contributed to the writing of the manuscript, provided critical feedback to the manuscript, and approved the final manuscript draft for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant to Brandeis University from the US Department of Health and Human Services (HHS), Administration for Community Living’s (ACL) National Institute for Disability, Independent Living, and Rehabilitation Research (NIDILRR) 90DPGE0007. Rachel Blayney’s effort on this project was funded in part by the Centers for Disease Control and Prevention (CDC; NU17CE924989). Zoe Pringle’s effort was supported by her role as a Lurie Disability Undergrad Fellow at Brandeis University. The contents of this article do not necessarily represent the policy of NIDILRR, ACL, or HHS, and you should not assume endorsement by the Federal Government. NIDILRR and CDC had no role in the study design, collection, analysis, or interpretation of the data, writing the manuscript, or the decision to submit the article for publication. Ohio Behavioral Risk Factor Surveillance System (BRFSS) data used in these analyses were obtained from the Ohio Department of Health, supported by the CDC; Florida BRFSS data were collected by the Florida Department of Health; and Nebraska BRFSS data were collected by Nebraska Department of Health and Human Services. Use of these data and the views expressed in this article are solely of the authors and do not necessarily reflect those of the Ohio Department of Health, CDC, Florida Department of Health, or Nebraska Department of Health and Human Services. These institutions do not agree or disagree with the analyses, interpretations, or conclusions in this publication.
Compliance,Ethical Standards,and Ethical Approval
The 3 datasets analyzed in this study were provided by the Ohio, Florida, and Nebraska Departments of Health with approved data use agreements; they are de-identified and publicly available. Secondary analysis of these data is considered nonhuman subjects research by the Brandeis University Institutional Review Board.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.