
Abstract
High-intensity interval training (HIIT) is a time-efficient strategy to improve fitness and performance. Whereas the multiple and negative effects of high intake of alcohol have been widely studied, the effect of moderate alcohol doses after exercise is not clear, and it is currently under debate. For that, a total of 80 young healthy adults are studied and allocated into 5 groups, each including 16 participants. Four groups follow a HIIT program, while the fifth group is a control non-training group. The training groups will be randomized according to the characteristics of the ingested beverage (alcohol beer, beer 0.0%, sparkling water, or ethanol). The effects of HIIT on several aspects of physical performance and mental health in young healthy adults are evaluated, also the concomitant effect of daily and moderate alcohol consumption. The novelty of this study lies in the continuous measurement of the psychological parameters associated with carrying out a highly demanding training program in conjunction with alcohol consumption in moderate quantities, reflecting real-life conditions.
Highlights
Responding to the social question: “Can consuming alcohol affect the benefits of a rigorous workout program?”
Multidisciplinary intervention to understand whether consuming beer or alcoholic beverages while being involved in a highly demanding training program affects exercise benefits in real-life conditions.
Understanding the role that alcohol may play in subjective perceptions, mood state, and psychosocial variables while undergoing an intensive training program.
Introduction
Physical exercise is a powerful tool to preserve health, enhance well-being, and improve physical and mental performance.1,2 For that, the most effective physical exercises lead to improvements in physical fitness and, consequently, are part of a structured training program. 3 High-intensity interval training (HIIT) is particularly effective and efficient since it achieves results with less time investment,4-6 representing an important physical and mental overload for the organism due to the pressure of performing multiple high-intensity exercises in short intervals.7-9 HIIT elicits improvements in physiological parameters, such as body composition,10-12 cardiorespiratory fitness,13-15 and muscular strength.13,16 There is also evidence that physical exercise enhances cognitive function, including better processing speed, attention, and memory, and shows positive associations with self-perceptions, self-esteem, and mental well-being in young adults.6,17-20 However, although some studies have shown HIIT’s potential to improve enjoyment and adherence in healthy individuals, 21 as well as its possible effectiveness in reducing depression or anxiety,15,22,23 little is known about the psychological effects of HIIT to translate into public health recommendations. Furthermore, no studies examined the affective responses to a long-term period (>2 weeks) of a HIIT intervention.
Adequate recovery is essential for physical and mental improvements. 24 This requires sufficient rest, proper nourishment, hydration, and the absence of hindering factors 25 ; thus, an adequate rehydration after exercise is crucial to facilitate the removal, regeneration, repair, and protection of damaged or worn structures.26,27 In this line, the intake of beer during recovery, or consumed as part of the lifestyle, has been questioned due to its alcohol content (approximately range 3.5%-7%).28-30 Generally, beer intake for thirst-quenching, accompanying meals, or after exercise is a common practice for many physically active people and is characteristic of many sports. 31 The fact that beer is one of the most consumed beverages in the world is undeniable, 32 and it is the first one to contain alcohol. 28 The current literature has been unable to establish a significant cause-effect relationship between alcohol and performance due to the small sample, which may have underpowered studies, the doses of alcohol often used, and the auto-reported method.33-36 There are reasons to believe that acute alcohol consumption may negatively affect metabolic, cardiovascular, or neurological functions, as well as cognitive function. 37 However, despite its alcohol content, beer is composed of water (90%), carbohydrates, amino acids, lupulins, vitamins, minerals, and other compounds, such as polyphenols, which may play a role in the recovery process (physical and mental) or even may have benefits on health.32,38
The present study has been designed to shed light on the existing controversy about moderate beer and alcohol consumption in relation to exercise or, more particularly, while training in healthy individuals.28,30,35,36 The study’s overall and primary aims are to evaluate the combined effects of a HIIT program and moderate alcohol/beer consumption on physical performance (ie, cardiorespiratory fitness, body composition, and cardiovascular adaptations), cognitive performance, and psychosocial parameters. We hypothesize that our 10-week HIIT intervention would positively affect physical fitness parameters, cognitive performance, and psychosocial measurements, but those positive effects may be influenced by the regular consumption of beer or its alcohol content in moderate amounts.
Participants and Methods
The BEER-HIIT project is a registered controlled trial (ClinicalTrials.gov ID: NCT03660579). The Ethics Committee on Human Research at the University of Granada (321/CEIH/1617) has provided advice and approved the study design, protocols, and informed consent procedure described here. The baseline and follow-up assessment are performed at the same setting (Instituto Mixto Universitario Deporte y Salud at the University of Granada). The study strictly follows the last revised ethical guidelines of the Declaration of Helsinki.
Participants and Selection Criteria
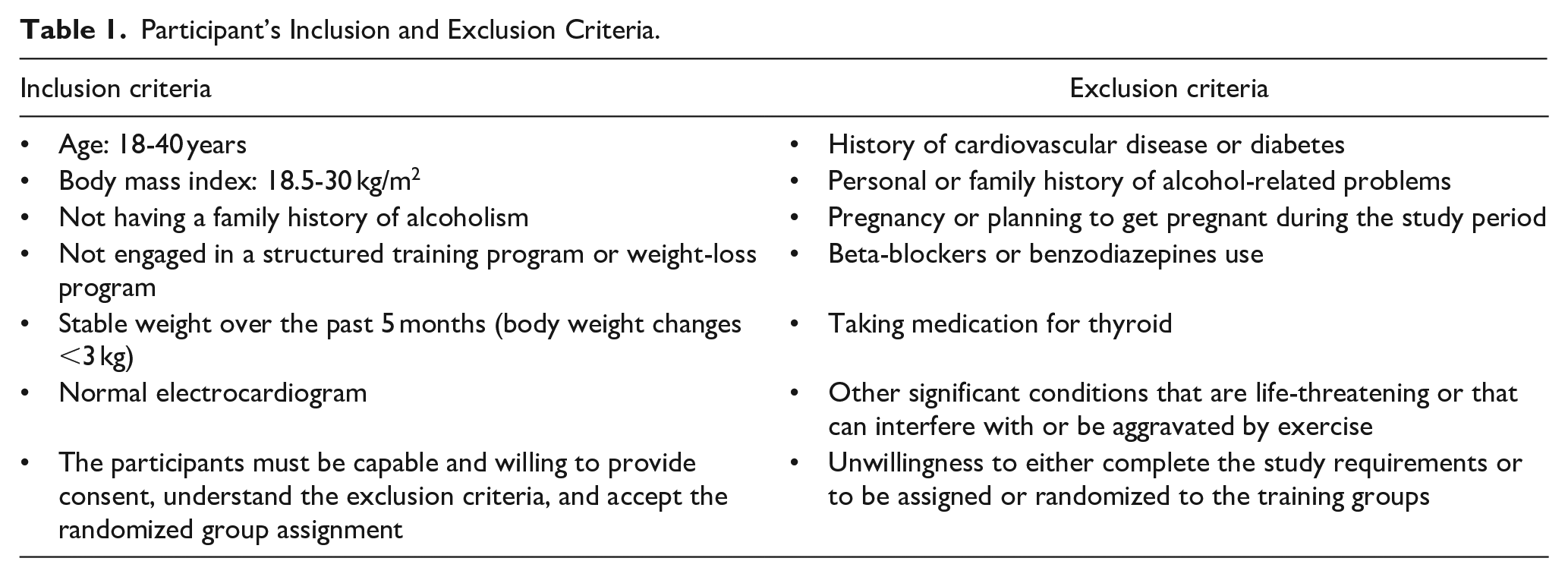
The participants are healthy Caucasian adults, aged between 18 and 40 years old, living in Granada (Spain). The inclusion and exclusion criteria are listed in Table 1. All participants have a health history and a medical examination done before the intervention program to minimize risks by ruling out contraindications to the testing and training protocols. If any participant suffers any injury or medical problem, a medical evaluation is performed and excluded from the study if necessary. In addition, adverse events related to our intervention (exercise or moderate alcohol consumption) are monitored and tracked daily by our staff members.
Participant’s Inclusion and Exclusion Criteria.
The study is announced on social networks, local media, and posters at different points in Granada. The people interested contact the research team by email and/or phone. They are invited to our laboratory to receive a thorough explanation of the study aims, the design of the study, group allocations, tests to be performed, the inclusion and exclusion criteria, and the types of intervention. What participants can expect from the study is clarified, and any questions will be answered. They are clearly informed about the risks of alcohol intake, the problems associated with excessive consumption, and the need for commitment to maintaining a healthy and stable lifestyle during the duration of the study. The potentially interested participants volunteering to participate and meeting the inclusion criteria are invited to a second orientation session in which they receive detailed written information about the study methodology, and a written informed consent is signed.
To reduce dropout cases and maintain adherence to the training program, several strategies are implemented. All sessions are accompanied by personalized music and held in an airy, well-lighted, well-equipped gym. Qualified and certified trainers carefully supervise every training session and work with groups of no more than 8 people to ensure that the participants perform the exercises correctly at the predetermined intensity. The trainers and the other study staff constantly support and supervise the participants weekly.
Prior to the evaluations, the participants are asked to avoid moderate exercise (24 hours), and strenuous exercise (48 hours); to avoid the consumption of alcohol, drug, or medication during the previous 48 hours; to avoid the consumption of stimulants such as coffee or caffeine-containing beverages the previous 12 hours; to avoid the consumption of food 2 hours before the evaluation and to have a standardized breakfast the evaluation day. In addition, all the participants are asked to report their usual frequency of alcohol intake in 7 possible response categories using the Beverage Intake Questionnaire (BEVQ) 39 before and after the 10-week intervention. This questionnaire was developed to estimate the mean daily water intake, sugar-sweetened beverages, and alcoholic beverages. To score the BEVQ, frequency (“How often”) is converted to the unit of times per day and then multiplied by the amount consumed (“How much each time”) to provide average daily and weekly intake beverage consumption. Total alcohol consumption was quantified through the sum of beverage categories containing alcohol (ie, beer, wine, spirits, and cocktails). In addition, the physical activity levels are registered before and after the intervention program by self-report.
Groups and Distribution of Participants
After completing the baseline measurements, the participants choose whether they prefer to be included in a training (T) or non-training group. Training consists of 2 HIIT sessions per week for 10 consecutive weeks (see below). Those going for training then choose whether they prefer to be included in a group that ingests from Monday to Friday, during those 10 weeks, an ethanol-containing beverage (5.4% alcohol content) or an alcohol-free beverage. Men ingest 330 ml of that beverage with lunch and 330 ml with dinner. Women ingest 330 ml with dinner. Training (T) participants choosing ethanol are randomly allocated either to beer (T-Beer) or to sparkling water with added vodka ethanol (T-Ethanol). Those choosing nonalcohol are randomly allocated to alcohol-free beer (T-0.0 Beer) or sparkling water (T-Water). Each group is composed of 8 men and 8 women. This nonrandom (based on individual preference) and random allocation of the participants is done following ethical considerations and advice made by the ethical committee (321-CEIH-2017) since drinking alcohol or participating in a highly demanding training program should be a personal choice.
Non-Training Group
A total of 2 informative meetings presided by Sport Sciences and Human Nutrition and Dietetics graduates are organized, in which general advice to the non-training group about the importance of health and well-being in having an active lifestyle is provided. We also explain the current physical activity recommendations from the World Health Organization. 40 These meetings take place prior to the beginning of the project. The participants included in this group are encouraged to keep an active lifestyle and, if desired, participate in sports activities, but they are strictly requested not to engage in any structured training program during the period of the study.
Training Groups: Exercise Program Rationale
HIIT refers to repeated bouts of a short-to-moderate duration of vigorous and intense exercise, interspersed with passive or active recovery periods. 9 There are many HIIT protocols, and the specific physiological adaptations induced by this training modality are related to exercise stimulus (ie, intensity, duration, or number of intervals performed, among others), as well as the duration and activity patterns during recovery. 41 Similar to other studies, our project will add a small intervention effect for psychological well-being in the intervention HIIT protocol: each session will be designed to meet participants’ psychological needs, such as choice of music, provision of challenging and progressive workouts, working in groups, and support to professional trainers. 23
Volume
Participants start with a dose of 40 minutes/week at an intensity of 8 to 9 Rating of Perceived Exertion (0-10 RPE scale),42,43 which will progressively increase to 50 minutes/week at 10 RPE intensity (Phase I) and then to 65 minutes/week at 10 RPE intensity (Phase II). This gradual progression will ensure better control of the exercise dose and avoid injuries and dropouts.
Intensity
The HIIT intensity is based on scientific evidence.9,44,45 The participants perform different sessions of HIIT with short rest intervals, with an intensity >8 RPE, 43 which has a positive linear relationship with heart rate (HR) and VO2max (maximal oxygen uptake).42,46
Frequency
Traditionally, HIIT has been recommended 3 times/week.47,48 However, considering the participants’ training level (untrained individuals) and based on our previous experience,41,49,50 we have decided to reduce the training frequency (twice per week) to ensure a correct training recovery after the HIIT session. 47
Type of Exercise
The participants perform 8 self-loading exercises in circuit form (ie, frontal plank, high knees up, TRX horizontal row, battle rope, squat, dead lift, push-up, and burpees) with a passive rest between exercises, and twice per set with an active rest (an intensity of 6 RPE, which corresponds with 60% VO2max42,51), following the periodization described in Table 2.
HIIT Program Periodization.
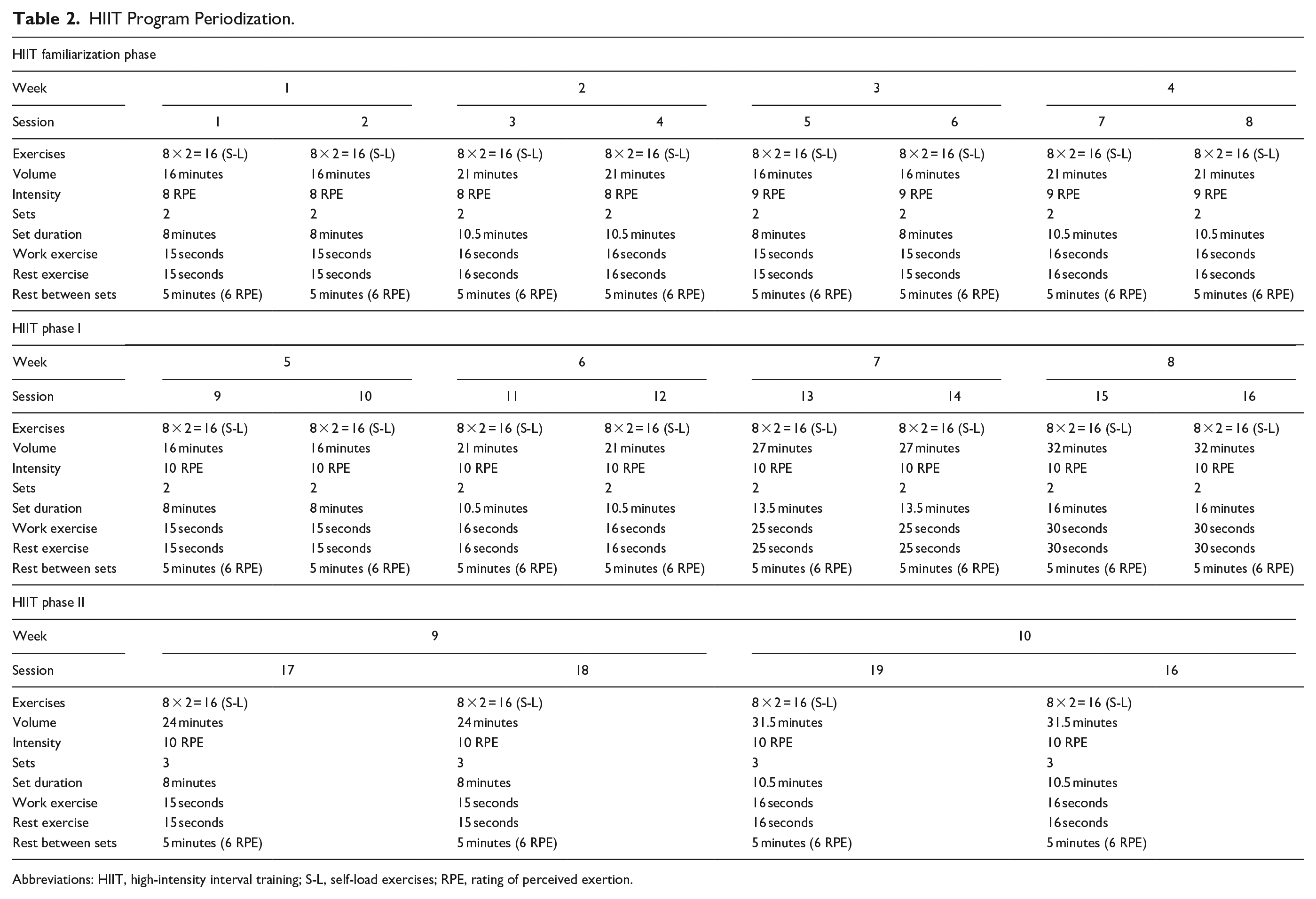
Abbreviations: HIIT, high-intensity interval training; S-L, self-load exercises; RPE, rating of perceived exertion.
Training Periodization
Table 2 shows the program’s training periodization. It is divided into 2 different phases, starting with a familiarization phase to learn the main movement patterns, as previously suggested.40,41,50
Training Sessions
The training sessions are performed in the late afternoon or early evening from Monday to Friday, allowing at least 2 days rest between consecutive sessions. The participants start with a dynamic standardized warm-up, including several muscle activations exercises (ie, child’s pose breathing, pelvis bridge, pelvic anteversion-retroversion, upper back rotation, front and side plank, toe walks, high knee walks, walking and side lunges, monster and sumo walk, and anti-rotational stability press). In addition, the training sessions end with a cooling-down protocol (active global stretching), including 7 anterior or posterior chain exercises (ie, pigeon pose, lying twist, figure 4 stretch, lunging hip flexor stretch, biceps stretch, and trapezius neck stretch).
Beverage Intake Protocol
The beverages are ingested daily from Monday to Friday. The volumes of fluid ingested are the same in all groups (660 ml for men and 330 ml for women); men ingest 330 ml with lunch and 330 ml with dinner, and women ingest 330 ml with dinner: (1) T-Beer group ingest regular Lager Beer (5.4% alcohol; Alhambra Especial); (2) T-0.0 Beer group ingest alcohol-free beer (0.0% alcohol; Cruzcampo®); (3) T-Water group ingest sparkling water (Eliqua 2®); (4) T-Ethanol group ingest sparkling water with exactly the same amount of distilled alcohol added. The distilled alcoholic beverage used in our study is branded vodka because of the purity of its composition (37.5% ethanol and 62.5% water). Table 3 shows the characteristics of the drinks. We are based on scientific evidence to select the amount of alcohol ingested by the participants, which define a moderate amount as 2 or 3 drinks/day or 24 to 36 g of ethanol/day for men and 1 to 2 drinks/day or 12 to 24 g of ethanol/day for women.38,52 The only alcohol consumption allowed from Monday to Friday is that supplied by the investigators. Specifically, the beverages are coded in a bottle with a predetermined quantity and provided by a staff member of our research laboratory at the beginning of each week. Empty bottles from the prior week were collected to monitor accurate consumption tracking. The investigators who do the evaluations are not aware of the group assignment of the participants. During the weekend, those participants included in alcohol groups are requested to drink no more than a moderate amount of alcohol on Saturday and Sunday (ie, 660 ml/day for men and 330 ml/day for women). Those included in nonalcohol groups are requested to refrain from alcohol also during the weekend. In addition, the alcohol intakes are registered before and after the intervention using a validated questionnaire.
Nutritional Characteristics of Drinks.
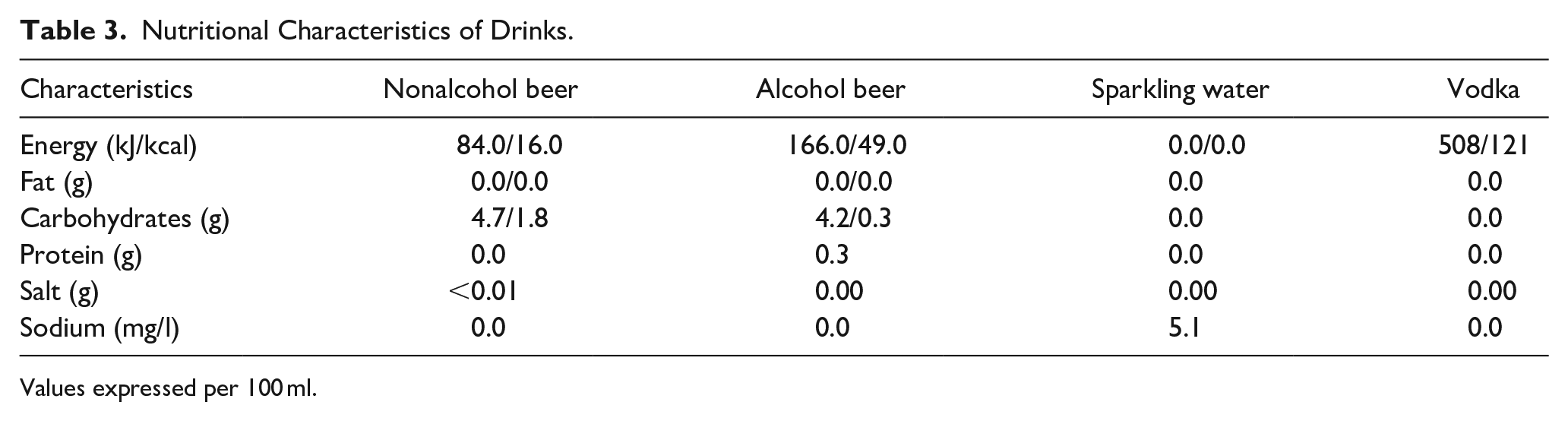
Values expressed per 100 ml.
Outcome Variables
The primary and secondary outcomes of our study are measured on 1 day, including physical fitness components, body composition and anthropometric measurements, heart rate variability (HRV), psychomotor and cognitive variables, health-related quality of life, psychological profile, dietary and exercise habits, quality of sleep, and sexual function. In addition, each participant completes a battery test of questionnaires at home (Table 4). The details of the outcome variables can be found in the Supplemental Material.
Time Frames of Questionnaire Battery.
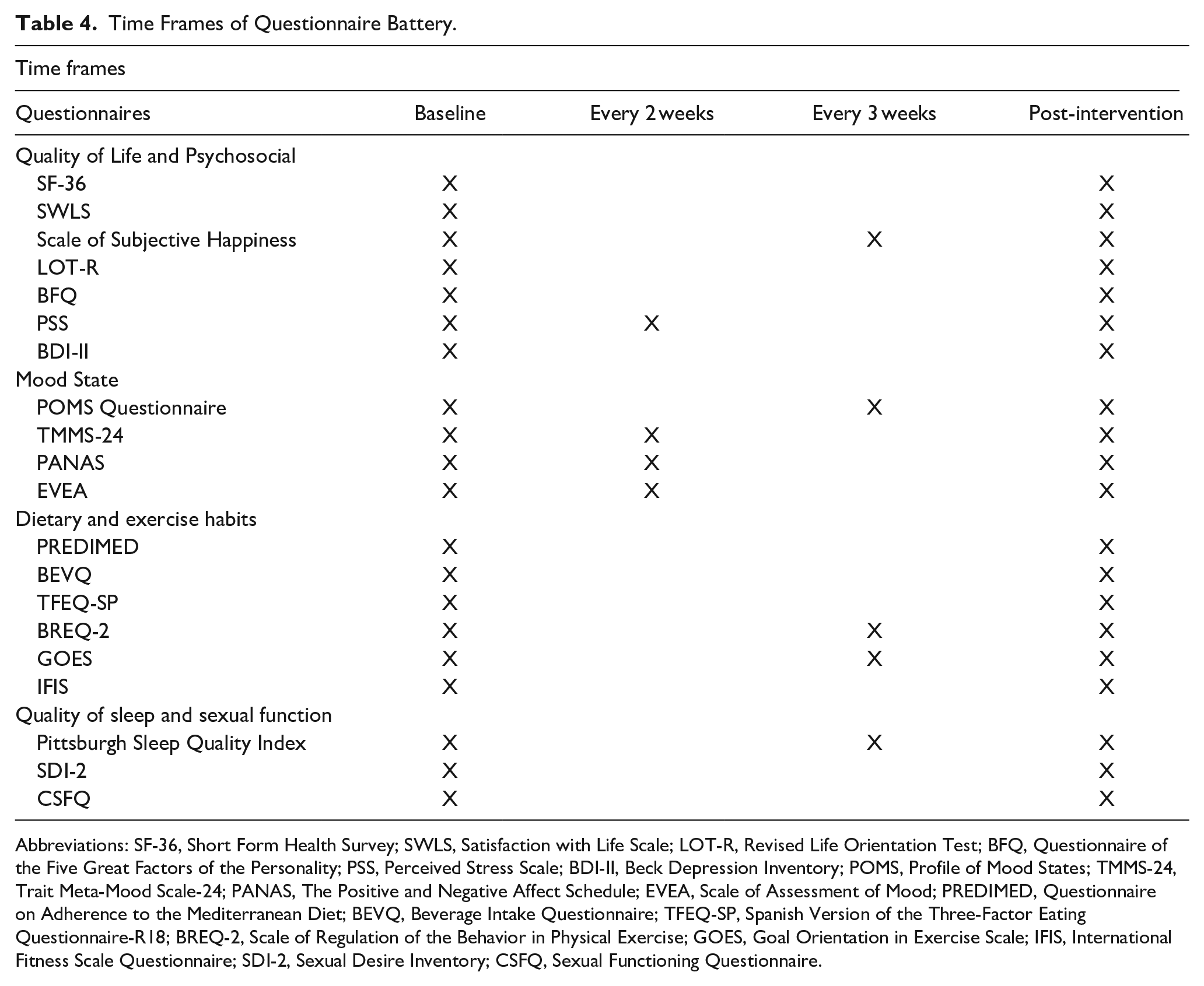
Abbreviations: SF-36, Short Form Health Survey; SWLS, Satisfaction with Life Scale; LOT-R, Revised Life Orientation Test; BFQ, Questionnaire of the Five Great Factors of the Personality; PSS, Perceived Stress Scale; BDI-II, Beck Depression Inventory; POMS, Profile of Mood States; TMMS-24, Trait Meta-Mood Scale-24; PANAS, The Positive and Negative Affect Schedule; EVEA, Scale of Assessment of Mood; PREDIMED, Questionnaire on Adherence to the Mediterranean Diet; BEVQ, Beverage Intake Questionnaire; TFEQ-SP, Spanish Version of the Three-Factor Eating Questionnaire-R18; BREQ-2, Scale of Regulation of the Behavior in Physical Exercise; GOES, Goal Orientation in Exercise Scale; IFIS, International Fitness Scale Questionnaire; SDI-2, Sexual Desire Inventory; CSFQ, Sexual Functioning Questionnaire.
Physical Health Measurements
Cardiorespiratory Fitness
Cardiorespiratory fitness is measured through a maximum treadmill test (H/P/Cosmos Pulsar treadmill; H/P/Cosmos Sport & Medical GMBH, Germany) applying the modified Balke protocol, 53 which has been widely used and validated.41,50,54 We measure O2 uptake and CO2 production with a breath-by-breath gas analyzer (CPX Ultima CardioO2; Medical Graphics Corp) calibrated with known gas mixtures and environmental air immediately before the test. During each trial, the participants are strongly encouraged to invest maximum effort. The criteria for achieving VO2max are a respiratory exchange ratio ≥1.1, a plateau in VO2/change of <100 ml/minute in the past 3 consecutive 10 seconds stage), a heart rate within 10 beats/minute of the age predicted maximal heart rate (168 − 0.7 × age),55,56 and if these criteria were not met, the peak oxygen uptake value during the exercise test was considered. 56 The exercise electrocardiogram is continuously monitored during the test. We also control the blood pressure before the test, 1 minute after the beginning of the test, and every 5 minutes during the treadmill test.
Muscular Strength
We measure muscular strength by the handgrip strength. The handgrip strength is measured using a digital dynamometer (TKK 5101 Grip-D; Takey). This measurement has been suggested as a valid test to predict muscular strength and endurance with simpler equipment and minimizing effort from subjects. Also, it has been associated with whole-body and upper-body strength. 57 The grip span is determined following the procedures previously described. 58
Muscular Power
The evaluation of power of the extensor muscles of the lower limbs is evaluated through the “Ergo Jump Bosco System®” (Globus). This device has a digital timer (±0.001 seconds) connected by a cable to a resistive (or capacitive) platform. The timer is triggered by the feet of the subject at the moment of release from the platform and stopped at the moment of touchdown. Thus, the flight time of the subject during the jump is recorded. 59 The test consists of a series of strictly standardized maximum vertical jumps. It offers a simple and intuitive method for evaluating the anaerobic (mechanical) power and trunk during the test. To familiarize the subjects with the test, the participants perform some practice trials before the assessment. 60
Body Composition and Anthropometric Measurements
Body weight, height, hip circumference, and waist circumference are determined following the recommended standardization procedures from the International Society for the Advancement of Kinanthropometry. 61 The fat mass, fat-free mass, lean body mass, visceral adipose tissue, and bone mineral density are evaluated by conducting a full-body dual-energy X-ray absorptiometry scan following the manufacturer’s instructions (Discovery Wi; Hologic, Inc).
Heart Rate Variability
The assessment of HRV is carried out in a supine position for 15 minutes. The Polar RS800CX (Polar Electro) is used to evaluate this parameter (R-R series active). The participants will be informed that their heart activity is recorded for 15 minutes, and they are instructed not to talk or move excessively and to relax as much as possible. The participants remain in a supine position for 5 minutes before the start of the recording. We use the Kubios HRV software (University of Eastern Finland,) to process the HRV. 62
Mental Health and Lifestyle Measurements
Psychological Profile and Lifestyle
A set of questionnaires are used to assess mental health and psychosocial parameters. To control the evolution of the variables measured during the intervention process, the time frames are at baseline and after 10-week intervention (pre- and post-intervention), every 2 weeks, and every 3 weeks (see Table 4).
Quality of Life and Psychosocial Measurements
Health Questionnaire, 63 Satisfaction with Life Scale 64 ; Subjective Happiness Scale, 65 Life Orientation Test Questionnaire, 66 Questionnaire of the Five Great Factors of the Personality, 67 Perceived Stress Scale, 68 and Beck Depression Inventory.69,70
Mood State
Profile of Mood States Questionnaire,71-73 Trait Meta-Mood Scale-24, 74 The Positive and Negative Affect Schedule Questionnaire, 75 and Scale of Assessment of Mood.76,77
Dietary
Questionnaire on Adherence to the Mediterranean Diet consists of 12 questions on food consumption frequency and 2 questions on food intake habits considered characteristic of the Spanish Mediterranean diet. 78 BEVQ estimates the mean daily intake of water, sugar-sweet beverages, alcoholic beverages, and total beverages across 19 categories79,80; Spanish Version of the Three-Factor Eating Questionnaire-R18, an 18-item questionnaire that measures 3 different aspects of eating behavior: (1) restrained eating, (2) uncontrolled eating, and (3) emotional eating.81,82
Exercise Habits
Scale of Regulation of the Behavior in Physical Exercise83,84; the Goal Orientation in Exercise Scale (GOES)85,86; and the International Fitness Scale Questionnaire.87,88
Quality of Sleep and Sexual Function
Pittsburgh Sleep Quality Index 89 ; the Sexual Desire Inventory 90 ; and the Sexual Functioning Questionnaire. 91
Cognitive Performance
Psychomotor Function Assessment
The analysis of the psychomotor function is measured using the determination test Turkish form (S16, DT) with the Vienna Test System (Schuhfried GmbH). This test measures reactive stress tolerance, attention, and reaction speed in situations requiring continuous, swift, and varying responses to rapidly changing visual and acoustic stimuli.92-94
Verbal Memory
We use the Spanish-Complutense Verbal Learning Test to evaluate episodic verbal memory 95 , as well as its codification processes, data storage, and retrieval.
Attention
We use the standard version of the D2 test to measure the different aspects of selective attention 96 .
Verbal Fluency
The verbal fluency test is a short test of verbal functioning. It typically consists of 2 tasks: category fluency and letter fluency (sometimes called phonemic fluency). 97
Working Memory
We use the Letter-Number Sequencing Test to evaluate the spatial span forward. The test is administered according to the rules in the Wechsler Adult Intelligence Scale (WAIS-IV) manual. 98
Sample Size
The determination of the sample size and power of the study are based on the data of a pilot study. 99 We have considered the differences in physical fitness (cardiorespiratory fitness) levels between pre- and posttreatment to assess the sample size requirements for the 3-way analysis of variance (ANOVA). 100 We expect to detect an effect change of 2 ml/kg/minute in cardiorespiratory fitness, considering a type I error of 0.05 with a statistical power of 0.85 if we consider a minimum of 13 participants per group. Assuming a maximum loss at follow-up of 20%, we have decided to recruit 16 participants (≈50% women) for each study group. A total of 80 participants (≈50% women) are enrolled in the BEER-HIIT study. Based on previous randomized control tricals (RCTs) and on our own experience,41,50,52 we think the sample size is realistic and accessible.
Statistical Analysis
All outcome variables will be verified for normality, and the results will be expressed as mean and standard deviation. For between-group comparisons at baseline (T-Water vs T-Beer vs T-0.0 Beer vs T-Ethanol), we analyze continuous variables with the 1-way ANOVA or the nonparametric method of Kruskal-Wallis and Chi-square tests, as appropriate. We use General Lineal Models to assess the training effects [time (pre-post 10-week intervention) × group interactions] on the primary and secondary study outcomes. We perform Bonferroni post hoc tests with adjustment for multiple comparisons to determine the differences among all groups. We analyze the data according to the intention-to-treat principle 101 and handle missing data resulting from dropouts or noncompliance using multiple imputation methods. To fully appreciate the potential influence of missing responses, we will perform sensitivity analyses to examine whether the imputation method affects the outcomes. In addition, multiple regression will test potential moderators of the outcomes. We will test each potential moderator individually. We will also explore the influence of demographic variables (ie, gender, education, average alcohol intake, or self-reported physical activity levels) in our primary and secondary outcomes. All analyses are performed using the Statistical Package for Social Sciences (SPSS, v. 25.0, IBM SPSS Statistics; IBM Corporation). The graphical presentations are prepared using GraphPad Prism 5 (GraphPad Software).
Discussion
There are many reasons for exercising. Most sports and exercise participants are motivated mainly by social factors such as the desire to have fun or be active, pursue interests and be stimulated, engage in challenges, or expand skills. 102 Although little is known about the affective and psychological responses over time to a highly demanding training program due to diverse populations and training protocols, recent shreds of evidence suggest that HIIT may be a viable strategy for obtaining positive results in affective and enjoyment. 103 As part of the recovery process and social relationship after practicing exercise, beer is the most popular alcoholic beverage among healthy adults, being mainly consumed with meals.27,104,105 Actually, the consumption of beer, and more rarely other alcohol-containing beverages, is often encouraged as a social aspect of sporting events, for example, to facilitate team bonding and as part of post-match celebration and relaxation. 106 However, because of the ethanol contained in beer and its deleterious effect, this practice may not be advisable, particularly when the exercise is very demanding or when the individual is training to improve physical fitness or maintain overall health.
Although the multiple and negative effects of high intakes of alcohol have been widely studied and demonstrated,107,108 the effect of moderate alcohol doses after exercise is not clear and it is currently under debate.32,38,109 Some studies indicate that postexercise alcohol intake may have a detrimental effect on muscle recovery. 110 Other investigations have suggested that beer consumption could be associated with increased waist circumference. 111 In contrast, prospective studies have disproved this phenomenon popularly referred to as “beer belly.” Furthermore, some research has shown that alcohol-containing beverages may decrease performance, specifically affecting reaction time, fine motor control, levels of arousal, and judgment. 112 However, we can find contradictory and inconclusive results, which may be explained by the different exercise models, alcohol doses, types of beverages, and participant characteristics, including their habitual alcohol intake. 113 To the best of our knowledge, there are no published studies investigating the effect that a moderate consumption of beer or alcohol, within the context of a normal life situation, may have on the adaptive response to a highly demanding physical training program designed to improve physical fitness or psychological and mental health in healthy individuals.
The BEER-HIIT study investigates, in conditions reflecting the real-life situation of young, healthy individuals, the possible interference of regular but moderate beer intake or its alcohol equivalent on the benefits that the practice of intensive training may have on physical and mental variables and clarifies the role played by ethanol. Specifically, we characterize the consequences of training versus non-training. Then, we study the effects of simultaneously consuming alcohol-containing beer, alcohol-free beer, and sparkling water with alcohol added. Furthermore, our study claims to evaluate the psychological changes resulting from the performance of a highly demanding training program and the psychological consequences of this practice.
Despite these strengths, this trial presents several limitations. As with many of the studies that examine the effects of alcohol consumption, our research presents some design limitations, largely because of ethical issues that prevent randomized trials of alcohol consumption. 114 First, based on ethical reasons, all participants are informed of the convenience of regular physical activity, but to be included in a group submitted to highly demanding training (therefore susceptible to cause stress and injuries) must remain a personal option. Second, our study only includes young, healthy adults; hence, we cannot extend the results to older or less healthy individuals. Third, participants are not purely randomized for receiving alcohol or not. Again, based on ethical considerations and following the advice of the ethical committee (321-CEIH-2017), it does not seem appropriate to push a healthy young adult to drink alcohol if he/she does not desire or have the habit.
The findings from this study have a social and scientific interest as well as significant implications for our understanding of training and its effect on physical performance and mental health. It also could help understand the psychological responses during a training intervention in a real context. Furthermore, this study can provide answers to a particular interest of society about the convenience, or not, of consuming beer or alcoholic beverages while being involved in a highly demanding training program. Finally, this study could help understand the role that alcohol may play in subjective perceptions, mood state, and psychosocial variables while undergoing an intensive training program.
Supplemental Material
sj-docx-1-saj-10.1177_29767342241253388 – Supplemental material for Investigating the Alcohol Effects on the Response to Strenuous Exercise Training: Protocol for a Multidisciplinary Intervention Study in Young Healthy Adults—The BEER-HIIT Study
Supplemental material, sj-docx-1-saj-10.1177_29767342241253388 for Investigating the Alcohol Effects on the Response to Strenuous Exercise Training: Protocol for a Multidisciplinary Intervention Study in Young Healthy Adults—The BEER-HIIT Study by Cristina Molina-Hidalgo, Alejandro De-la-O, Lucas Jurado-Fasoli, Francisco J. Amaro-Gahete, Andrés Catena and Manuel J. Castillo in Substance Use & Addiction Journal
Supplemental Material
sj-docx-2-saj-10.1177_29767342241253388 – Supplemental material for Investigating the Alcohol Effects on the Response to Strenuous Exercise Training: Protocol for a Multidisciplinary Intervention Study in Young Healthy Adults—The BEER-HIIT Study
Supplemental material, sj-docx-2-saj-10.1177_29767342241253388 for Investigating the Alcohol Effects on the Response to Strenuous Exercise Training: Protocol for a Multidisciplinary Intervention Study in Young Healthy Adults—The BEER-HIIT Study by Cristina Molina-Hidalgo, Alejandro De-la-O, Lucas Jurado-Fasoli, Francisco J. Amaro-Gahete, Andrés Catena and Manuel J. Castillo in Substance Use & Addiction Journal
Footnotes
Acknowledgements
The authors would like to thank all the participants who participated in the study for their time and effort. We acknowledge Ms. Ana Yara Postigo-Fuentes for helping proofread the English text. This study is part of the corresponding author’s Doctoral Thesis conducted in the Psychology Doctoral Studies of the University of Granada, Spain.
Author Contributions
CMH participated in the design of the study, contributed to data collection, data reduction/analysis, and interpretation of results, and contributed to the manuscript writing – original draft; ADLO contributed to interpretation of results and participated in the manuscript writing – review and editing; LJF participated in the manuscript writing – review and editing; FAG participated in the design of the study, contributed to the interpretation of results and participated in the manuscript writing – original draft; AC participated into the manuscript writing – review and editing; MC participated in the design of the study and participated in the manuscript writing – review and editing.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors have no conflicts of interest directly relevant to the content of this article. Manuel J. Castillo is a former member of the Centro de Información Cerveza y Salud (CICS) Scientific Advisory Board. The funders had no role in the design of the study, the collection, analysis, or interpretation of data, the writing of the article, or the decision to publish the results.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Centro de Información Cerveza y Salud (CICS, Madrid, Spain) under Grant (29 870 €). The CICS does and will not participate, provide opinion, or interfere with the design of the study, methods to be used, interpretation, or scientific publishing of the results. ADlO. and FJAG. are supported by the Spanish Ministry of Education under a training grant (FPU14/04172 and FPU15/03960).
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board approval was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.