
Abstract
Background:
Few patient-facing educational materials and interventions exist for the prevention of injection drug use-related infective endocarditis (IDU-IE). We developed a patient and clinician-informed website for patients about IDU-IE to promote education and prevention strategies.
Methods:
This mixed-methods study integrated surveys and semi-structured interviews with patients and clinician to develop a patient website about IDU-IE. Patient participants included hospitalized adults with an opioid use disorder, history of injection drug use, and an injection drug use-related infection. Interprofessional healthcare clinicians including trainees participated. A baseline survey and semi-structured interviews were conducted with patients to understand knowledge of IDU-IE and preferences in educational materials content and format. Interviews were analyzed using rapid qualitative analysis. Results informed development of the patient website. Finally, patients and clinicians provided 2 rounds of survey feedback after reviewing the website, assessing the likelihood of using and recommending it to others, helpfulness of information in the website sections, and content satisfaction.
Results:
Patient participants (n = 15) reported low baseline understanding of injection practice and risk of IDU-IE. After reviewing the website (n = 17), patients reported they were very likely to recommend the website as a reference for themselves (mean of 4.3; 4 = very likely) and for others (mean = 4.3). They found the following sections, on average, to be very helpful (4 = very helpful): complications from injection drug use (4.4), safer injection practice (4.4), and information about infective endocarditis (4.4). Patients on average were satisfied with the website content overall (4.8). Clinicians (n = 27) reported, on average, being very likely to recommend this website to a patient (4.4) and to use the website to counsel patients (4.1).
Conclusions:
A patient and clinician-informed website on IDU-IE is acceptable for patients and clinicians to use as a patient education resource to help prevent IDU-IE-related harms.
Highlights
Mixed methods were used to develop a patient and clinician-informed website for prevention and education about injection drug use-related infective endocarditis.
Patients with opioid use disorder found the content on the website to be informative.
Introduction
Hospital admissions secondary to injection drug use-related infective endocarditis (IDU-IE) have surged in the United States in parallel with the opioid overdose epidemic, with a 238% increase in hospitalizations from 2000 to 2013. 1 The incidence rate of endocarditis among patients with opioid use disorder (OUD) increased from 3.7 in 2011 to 30.1 in 2022 which is 3 to 8 times that of patients without IDU. 2 Patients with IDU-IE have high mortality, morbidity, and risk for repeat infections if injection drug use continues.3-5 It is crucial that patient-centered interventions are developed to educate people who inject drugs (PWID) about IDU-IE for primary, secondary, and tertiary prevention. 6
The Substance Abuse and Mental Health Services Administration (SAMHSA) Harm Reduction Framework conceptualizes harm reduction as a set of services, an approach, and a type of organization, embodying various pillars, principles, and practice areas designed to provide people who use drugs (PWUD) with information, resources, and support to reduce negative consequences of substance use, such as IDU-IE. 7 Harm reduction is part of the broader continuum of care, meeting people where they are to reduce risk, improve outcomes, and increase service engagement. While many resources have been directed to prevent HIV/hepatitis C transmission among PWID, specific harm reduction education is lacking for IDU-IE despite evidence that simple techniques like cleaning one’s skin prior to injection may decrease complications of IDU. 8 In addition, clinicians may lack knowledge about harm reduction approaches and confidence in discussing harm reduction and safer injection practices with their patients.9,10 One study found that education for PWID on safer injection practice reduces high-risk injection practices. 11
The Health Belief Model (HBM) is a theoretical framework to inform patient education resources. The HBM states that the foundation of health-related behaviors are 2-fold; an individual’s perception of disease severity and susceptibility, and the belief that a specific action can help prevent or cure a disease. 12 An individual will select their course of action based on their perception of the disease while considering the benefits and barriers to this health-related behavior. 12 Based on this theory of change, a patient education resource that describes complications related to IDU and specific injection behaviors that reduce risk of IDU-IE could potentially change PWID injection practices.
Furthermore, technology to provide patient education, treat substance use disorders, and develop addiction prevention programs is proliferating.13-15 There is also increasing demand for quality harm reduction education, 16 but there is heterogeneity in the quality and content of these resources. 15 Accessible education that has been peer reviewed and patient-informed would be a valuable tool to prevent IDU-IE.
The goal of this project was to develop and assess the acceptability of a patient- and clinician-informed website with comprehensive, accurate information on the risks of IDU, methods to minimize harms of IDU, and prevention strategies to reduce the risk of IDU-IE. Due to the stigma surrounding this topic, creation of this website can additionally assist with normalizing conversations about harm reduction within the medical field and provide clinicians with a resource they can use to counsel patients. We hypothesize that an educational website on IDU and IDU-IE-related harm reduction is feasible to develop and acceptable to patients and clinicians.
Methods
This mixed-methods study used surveys and semi-structured interviews with patients and surveys of clinicians. Baseline patient surveys and interviews occurred between November 2021 and June 2022. The website was developed from June to November 2022. Round 1 of feedback from patients and clinicians occurred between November 2022 and May 2023. The website was revised based on Round 1 of feedback from June 2022 to May 2023. Round 2 of feedback from patients and clinicians occurred from May to June 2023 (Figure 1). The Yale University Institutional Review Board approved this study.
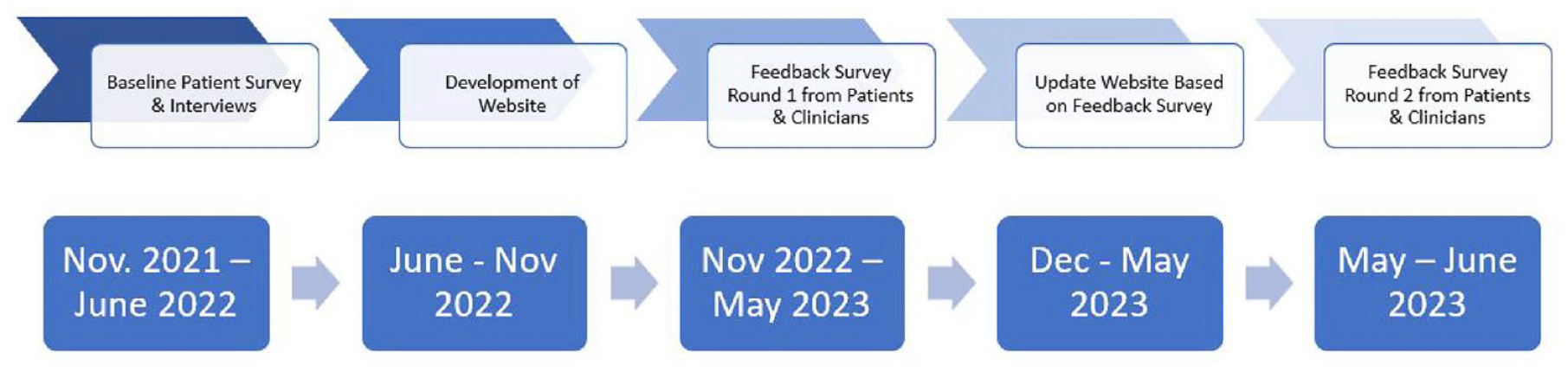
Overview of mixed methods utilized in this study, and the iterative process of improvement of the web applications.
Baseline Patient Survey
A cross-sectional preexisting survey was modified and reviewed by 3 experts for content validity (MBW, KLS, Shawn Cohen [SC]), 1 individual with lived experience of OUD, 1 social worker (RMR), and 1 public health professional (ETB), for face validity (Supplemental Appendix, Survey 1A). 17 From November 2021 to June 2022, this baseline survey was administered using Qualtrics to English-speaking patients with an OUD diagnosis, current or past IDU, and active hospitalization at Yale New Haven Hospital (YNHH) with a serious bone, endovascular, or skin and soft tissue infection, using a convenience sample of individuals who received an addiction medicine consult identified through the electronic medical record on days team members were able to recruit patients. 18 Informed by the HBM theoretical framework, the Baseline Patient Survey assessed patient experience and knowledge about (1) existing IDU practices, (2) relationship between injection practice and perceived risk of IDU-IE, and (3) barriers to safer injection practices. Responses to this survey informed the first iteration of the website. Participants received a $25 gift card for completing the survey. Results from the Patient Baseline Survey and informal content input from addiction medicine clinicians created the first iteration of the patient website.
Qualitative Data Collection
Semi-structured interviews further explored aforementioned patients’ preferences for and experiences of educational resources on safer injection (Supplemental Appendix, SS interview). Participants were informed their responses would be used to help design a patient education resource on harm reduction. They were asked to review preexisting materials as follows: 2 educational videos, 1 phone-app, and 2 printed handouts on harm reduction (see Supplemental Appendix for details). Interview participants were recruited using a convenience sampling approach from among those who completed the Baseline Patient Survey and were amenable to completing an interview. Interviews were audio-recorded via Zoom® and transcribed using Trint®. Interviews were conducted in person and via Zoom® by CAC, RMR, ETB, and Peyton Canaiss (PC). Participants were compensated with a $25 gift card for completing the interview.
Rapid Qualitative Analysis
A rapid qualitative analysis was conducted on the semi-structured patient interview data. Rapid analysis was employed so insights from the data could be integrated expediently into the real-time development and iteration of the website. 19 Templated summaries were produced for each interview, structured around key questions derived from the interview protocol (eg information sought on safer injection/other complications, preferred ways to learn about safer injection, barriers to safer injection, and dissemination of safer substance use information). These were subsequently organized within a matrix tool used to elicit themes. 19 For standardization, each team member summarized the same interview, followed by a group meeting to compare templated summaries. Each interview was then assigned to a single team member. All team members (CAC, ETB, RMR, KLS, MBW) contributed to templated summary development. Three members of this team were internal medicine and addiction medicine physicians (CAC, MBW, KLS), 1 was a public health professional (ETB), and 1 a social worker (RMR). After summarizing each patient interview, the research team reviewed the matrix tool and, employing an iterative process, identified possible themes. Findings informed revisions to the website content and design.
Patient Website Feedback Survey
After the initial website was created, a second, separate group of patients reviewed it and provided feedback through an online survey. Two rounds of feedback surveys were completed between iterative website revisions administered via Qualtrics from November 2022 to May 2023, and a second round of feedback occurred between May and June 2023 Convenience sampling was used to recruit individuals with a diagnosis of OUD and diagnosis of active or prior IDU who actively had an addiction medicine consult at YNHH hospital. The survey sought to understand the following: (1) how helpful was each website section (5-point Likert scale: not at all helpful to very helpful), (2) how likely are you to use the website, recommend it, and/or change your injection practices (5-point Likert scale: extremely unlikely to extremely likely), (3) satisfaction with the website (5-point Likert scale: extremely dissatisfied to extremely satisfied), and (4) how difficult was it to read the website, understand information, and find information (5-point Likert scale: very difficult to very easy). Likert scale questions were followed by open-ended questions (eg, How can we make this website better? What did you like best about this website? (Supplemental Appendix Survey 2A).
Clinician Website Feedback Survey
Clinicians commonly offer health educational materials to patients. To understand how clinicians perceived this resource, a survey was created for clinical trainees (addiction medicine fellows and primary care internal medicine residents from a single academic hospital) and practicing clinicians with a known interest in addiction medicine from diverse geographic areas in the United States (physicians and advanced practice providers) and administered in a voluntary, anonymous format using Qualtrics from November 2022 to May 2023, and a second round of survey feedback occurred from May to June 2023. Convenience sampling was used and clinicians were recruited via email. Trainee participants received a $25 gift card for completing the survey. Survey items included (1) how likely are you to (a) use the website as a personal reference and (b) recommend it to a patient (5-point Likert scale: extremely unlikely to extremely likely), (2) confidence in counseling a patient on harm reduction before versus after reviewing the website (5-point Likert scale: not at all confident to extremely confident), (3) how helpful was the information listed in each section of the website (5 point Likert scale: not helpful at all to extremely helpful), and (4) satisfaction with (a) information, (b) graphics, (c) navigation (5-point Likert scale: not at all helpful to extremely helpful). Likert scale questions were followed by open-ended questions (eg, How can we improve this website for clinicians? How can we make this a better resource for patients? (Supplemental Appendix Survey 3A).
Results
Patient Baseline Survey
Fifteen individuals completed the Patient Baseline Survey; 53.3% were female with an average age of 42 years and an age range from 28 to 61 years old (Table 1).
Demographics of Survey Participants in the Baseline Survey, Patient Website Feedback Survey, and Clinician Website Feedback Survey.
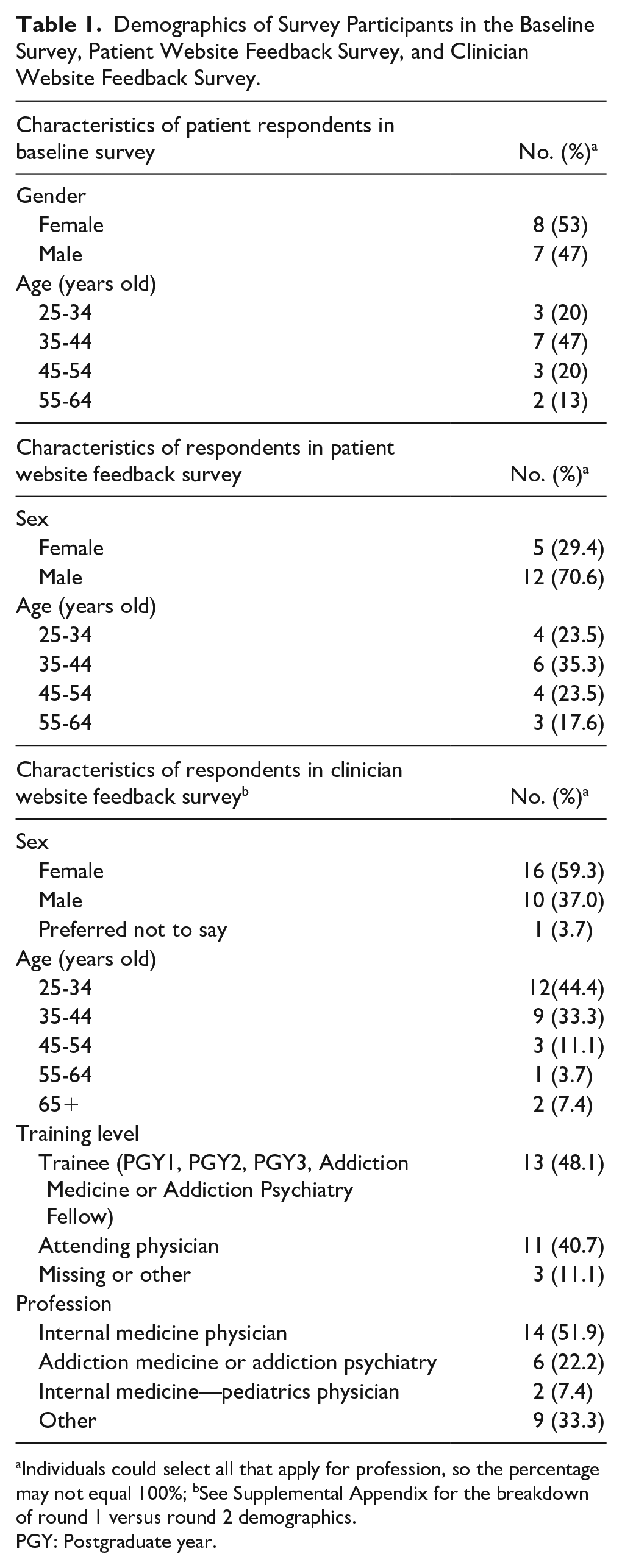
Individuals could select all that apply for profession, so the percentage may not equal 100%; bSee Supplemental Appendix for the breakdown of round 1 versus round 2 demographics.
PGY: Postgraduate year.
All (100%) Patient Baseline Survey participants reported injecting opioids (heroin or fentanyl), and 20% also injected cocaine. On average, participants reported injecting 2 to 3 times each day. Participants rated the following injection-related practices as having no risk, slight risk, or moderate risk for developing IDU-IE: using tap or bottled water (71.4%), reusing a cooker (46.7%), not cleaning skin before injection (33%), licking the skin or needle prior to injection (33.3%), using spit to dissolve a substance (28.6%), reusing their own cotton (26.7%), sharing cottons with others (20.0%), sharing a cooker with others (13.3%), having an untreated abscess or skin infection (13.3%), reusing their own needle or syringe (13.3%), injecting cocaine (13.3%), and injecting heroin/fentanyl (13.3%; Figure 2). Participants reported running out of injection supplies and experiencing opioid withdrawal as common barriers to safer injection practice.
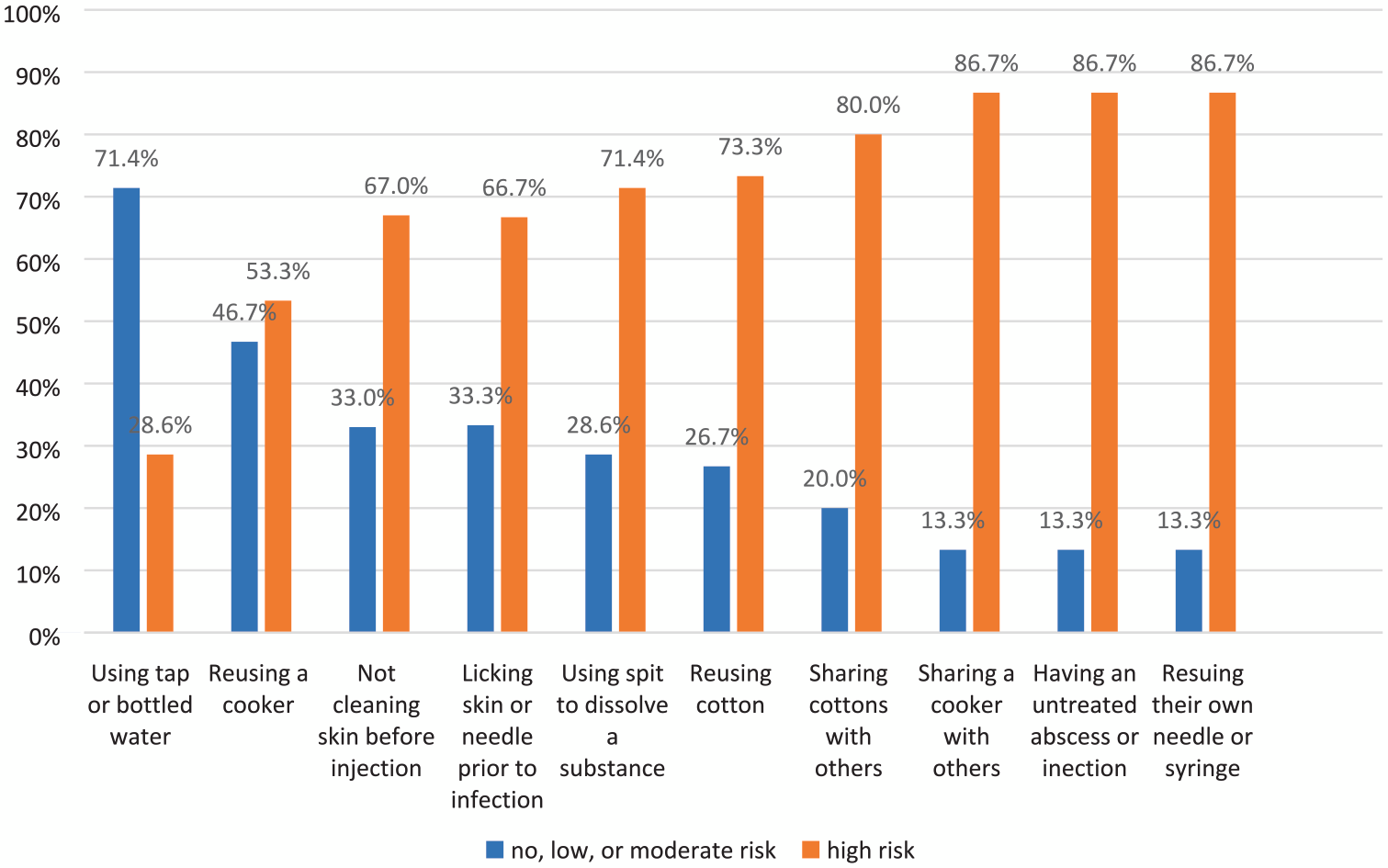
Injection drug practice and perceived risk of the practice giving an individual injection drug use-related infective endocarditis.
Rapid Qualitative Analysis of Patient Interviews
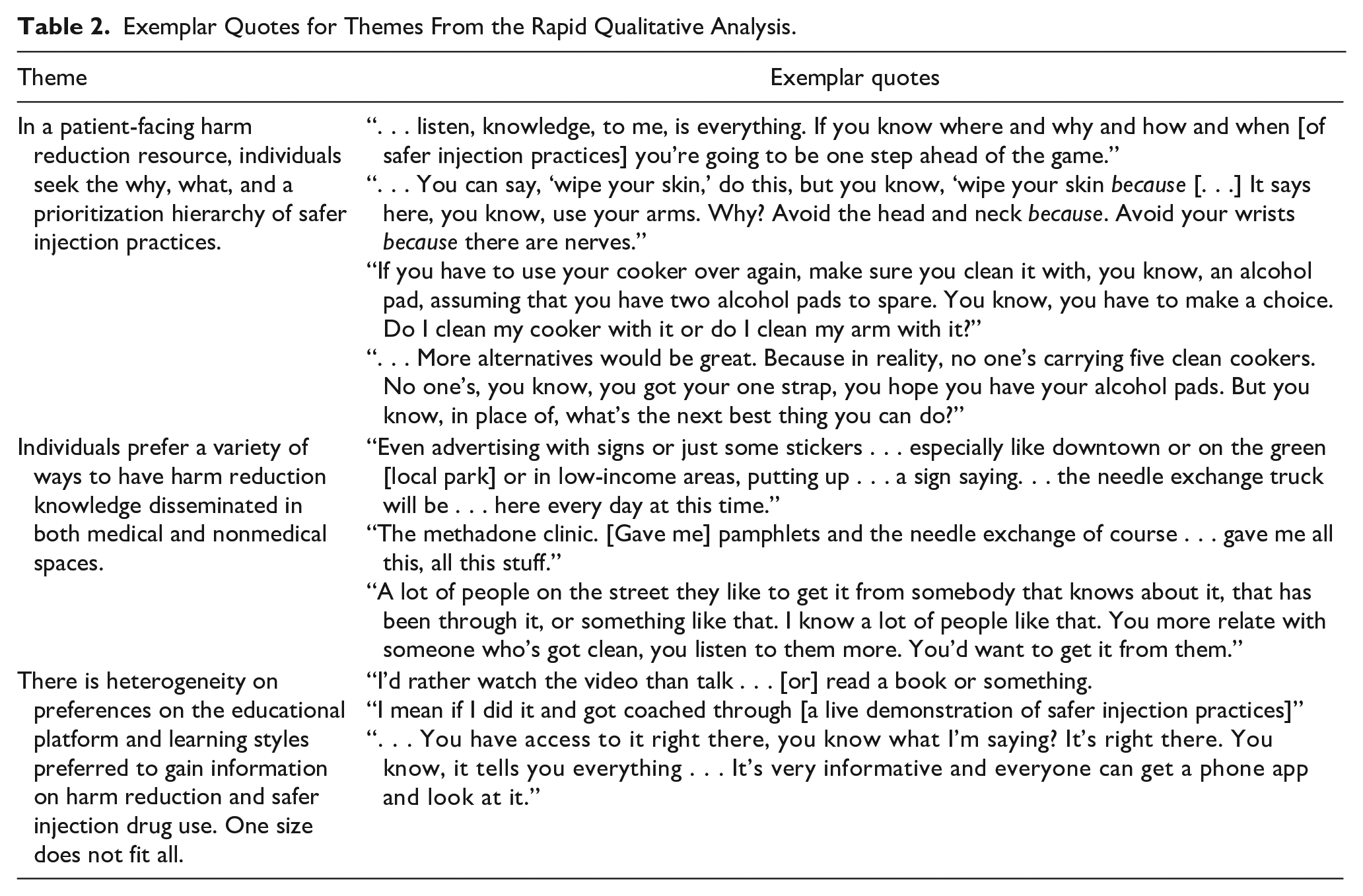
Using templated summaries and a matrix tool, 3 themes were identified related to IDU-IE education (Table 2).
Exemplar Quotes for Themes From the Rapid Qualitative Analysis.
Theme 1: In a Patient-Facing Harm Reduction Resource, Individuals Seek the Why, What, and a Prioritization Hierarchy of Safer Injection Practices
Participants wanted to know the reasons why certain safer injection practices were recommended compared to other practices. One individual stated, “It’s [harm reduction video is] great, but maybe more why . . . ” requesting that educational content not only instruct on best practices but explain “. . . here’s why we’re doing this [use new cooker].” In addition, they sought the details of precisely what could be done to use more safely and, where applicable, how various options compared in terms of safety. For example, one participant wanted the details on pros and cons of different water sources. “If there is significant information that has to do . . . with the type of water you use when it comes to tap water versus the saline . . . stuff like that, that would informative,” they shared. Real-life barriers may prevent individuals from using safer injection practices. Participants sought educational resources that acknowledge and respect the reality that PWID may not be able to use all the ideal practices and sterile supplies all the time, often for reasons out of their own control. As one participant put it while discussing use of sterile equipment when injecting, “In a perfect world, we’d all like to have fresh water, clean cookers, clean cottons, fresh needles. But that’s just not how it is.” Another, “you’re going to use whatever you can find.” Participants described wanting to better understand what practices are most essential for reducing risk, so they would have knowledge on how to adapt injection practices to the different environments and circumstances they may find themselves in and prioritize the highest-impact practice changes they can make with the materials available to them.
Theme 2: Individuals Prefer Harm Reduction Knowledge Disseminated in Both Medical and Nonmedical Spaces
There was heterogeneity in preferences for where harm reduction education should be disseminated. Some individuals preferred medical spaces such as opioid treatment program clinics, classes in community or medical sites, syringe service programs, or their doctor’s office. One individual stated: “I mean, my clinic (OTP), that’s probably the best venue,” while another wanted to broaden access outside of addiction treatment settings and recommended the emergency room: “And if I could walk into any E.R. or any urgent care facility and say, ‘Hey, I need information on X’ without being judged . . . I think you’d capture a wider range of people.” Others sought information from nonmedical spaces such as learning from a friend, from community outreach in common areas, or a mobile syringe service program. Some commented that they preferred both learning from peers and medical professionals, to confirm the information that they had received was accurate (see Table 2).
Theme 3: There Is Heterogeneity in Terms of Format and Learning Styles Preferred to Gain Information on Harm Reduction and Safer Injection One Size Does Not Fit All
When not learning this information directly from friends or the medical community, individuals expressed a wide range of views on the format in which they would prefer to learn about safer injection. Some sought out specific learning formats such as videos, pamphlets, websites, and phone applications. One individual reported: “They’re [videos] more, they get your attention . . . Nothing beats watching a video.” Another person stated how common access to phones are and a preference for accessing resources on their phone “[be]cause you have access to it [phone app] right there . . . You know, it tells you everything . . . everyone can get a phone app and look at it.”
Others preferred print media so they could have a way to reference the information later, which may be relevant to individuals without regular access to a phone or internet. Some participants requested concrete hands-on demonstrations or coaching to learn about safer injection practices. Overall, one size does not fit all for patient education on safer injection practices (Table 2).
Patient Feedback Survey
Participants were asked to provide feedback after reviewing a draft of the website. A total of 2 rounds of feedback were collected. In Round 1, the response rate was 63.6% (7/11) and in Round 2, the response rate was 76.9% (10/13). For Round 1, see participant demographics in Table 1, and Supplemental Appendix Table 2A.
Round 1 Survey Results
When asked to rate how helpful each section of the website was on a 5-point Likert scale (3 = somewhat helpful, 4 = very helpful), participants gave the following average ratings: safer injection practices (4.2), alternatives to injection drug use (3.6), information about infective endocarditis (3.3), other complications from injection drug use (4.0), overdose prevention (3.9), and treatment resource/harm reduction (4.0; Figure 3A-C). Participants were also asked to indicate on a 5-point Likert scale (4 = very likely) how likely they were to use the website as a reference (4.0 on average), to recommend it to others (4.2), and to change their own substance use practice (4.3; Figure 3A-C). Satisfaction was reported on a 5-point Likert scale as follows: information on the website (4.6 on average), pictures on the website (3.9). Difficulty with the website (4 = very easy) was rated on average as follows: read the website (4.3), understand the information (4.1), and find information (4).
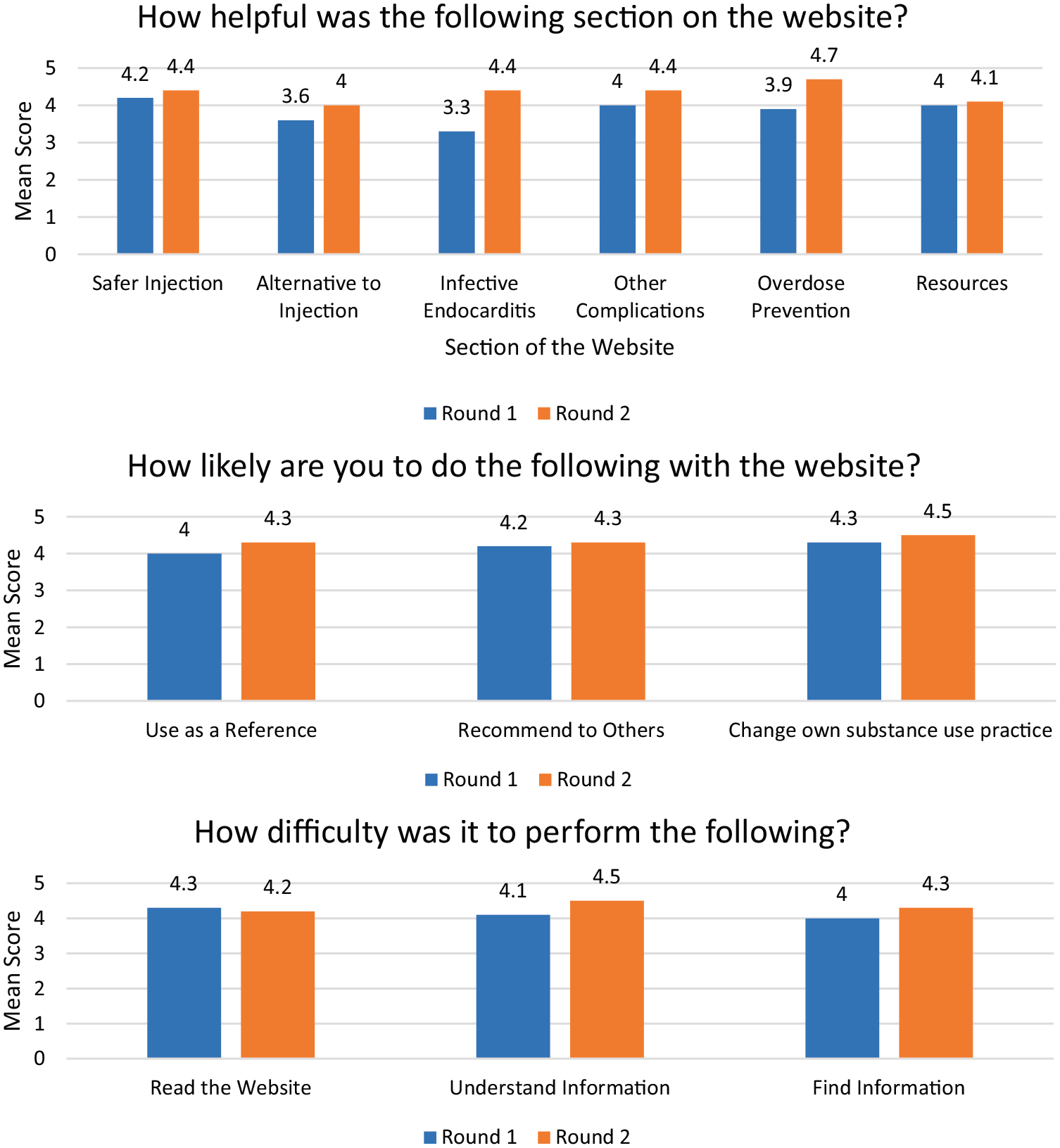
Patient feedback on the developed website in round 1 and round 2 of the iterative intervention on a 5-point Likert scale.
Round 2 Survey Results
When asked how helpful each section of the website was on a 5-point Likert scale (4 = very helpful; 5 = extremely helpful), participants gave the following average ratings: safer injection (4.4), alternatives to injection (4.0), information about infective endocarditis (4.4), other complications from injection drug use (4.5), overdose prevention (4.7), and treatment resource/harm reduction (4.1; Figure 3A-C). Participants indicated via a 5-point Likert scale (4 = very likely) how likely they were, on average, to use the website as a reference (4.5), recommend it to others (4.5), and change their own substance use practice (4.5). Satisfaction was reported on a 5-point Likert scale as follows: information on the website (4.8 on average), pictures on the website (3.9). Difficulty with the website (4 = very easy) was rated on average as follows: read the website (4.2), understand the information (4.5), and find information (4.3).
Clinician Feedback Survey
The combined results of Rounds 1 and 2 are reported here, with a combined response rate of 23.2% (27/116; see Table 1, and Supplemental Appendix Table 1A for additional details). Clinicians were asked how likely they were to perform the following on a 5-point Likert (4 = very likely): recommend this website to a patient (4.4. on average), use the website as a personal reference to counsel patients (4.1; Figure 4). On average, clinicians rated their confidence in their ability to counsel patients on safer substance use before reviewing the website as 2.3 (2 = slightly confident) and their confidence in their ability to do so after reviewing the website as 3.1 (3 = moderately confident; Figure 4). In addition, participants provided the following average ratings for helpfulness of sections of the website (4 = very helpful): alternatives to injection (4.3), harm reduction resources (4.3), safer injection (4.1), overdose prevention (4.0), infective endocarditis (3.9), and other complications (3.9).
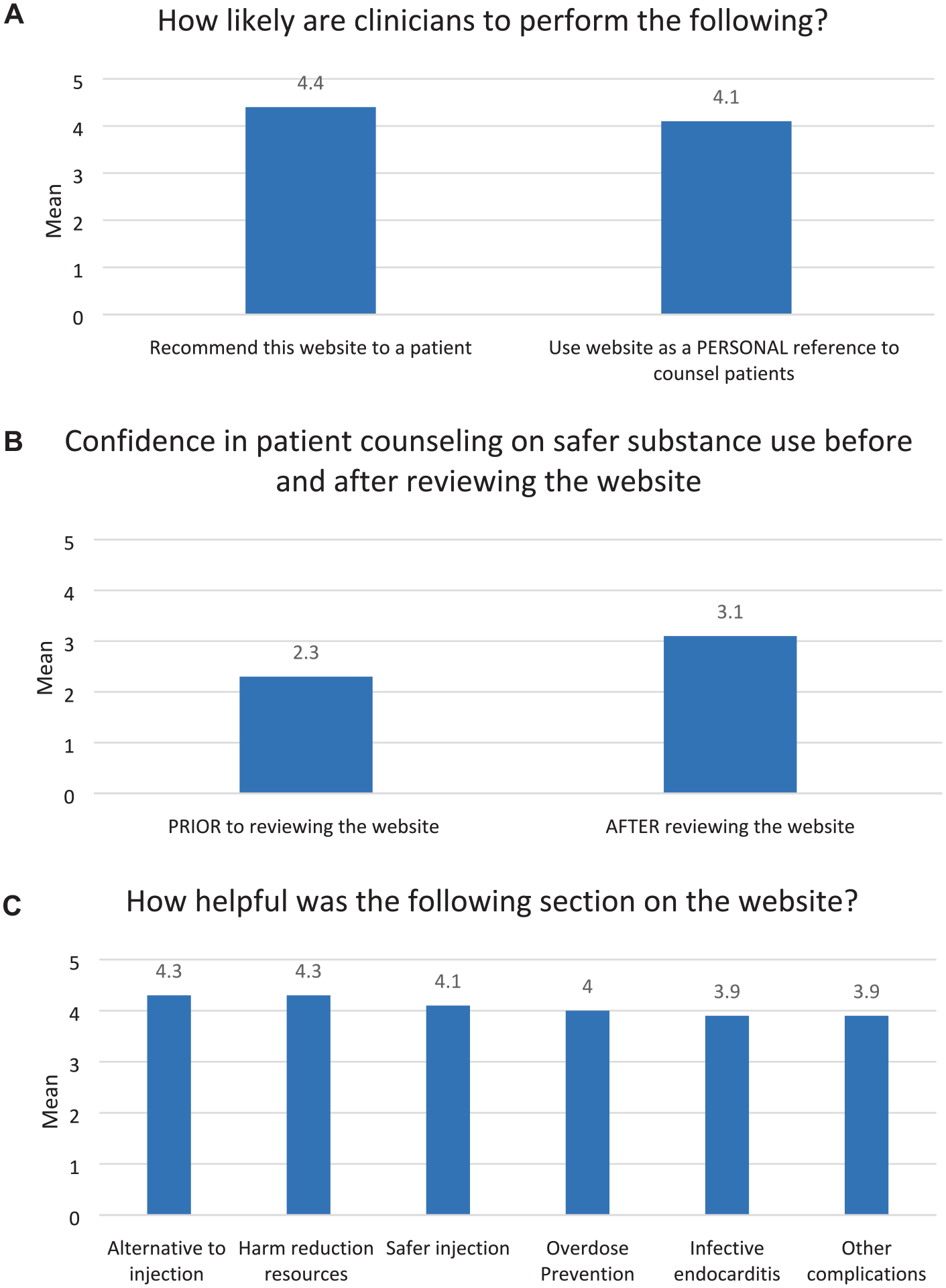
Clinician feedback on the website on a 5-point Likert Scale.
Discussion
This mixed-methods study informed the development of a highly rated patient and clinician-informed website to address IDU risks, IDU-IE, prevention of injection drug-related harms, and treatment options for substance use disorders. The final website can be freely viewed at SaferSubstanceUse.org (Figure 5). Baseline knowledge of the patient participants in this study showed low awareness of the serious risks associated with IDU and infectious complications of IDU, emphasizing the importance of having widely available accurate information that not only discusses HIV, hepatitis C virus (HCV), and overdose prevention but also harms of other less widely recognized infections related to IDU such as IDU-IE. Multiple rounds of patient and clinician feedback informed revisions to the website and average ratings trended higher in Round 2 of feedback. PWID reported that they were very likely to use the website as a reference, recommend it to a friend or family member, and change their own substance use practices based on information learned from the website. Clinicians reported that they were likely to utilize the website as a professional reference to counsel patients as well as recommend this website to patients as a reference.
Website homepage.
While there is extensive literature on targeted interventions to decrease HIV and HCV in PWID, a large gap exists in interventions designed for IDU-IE. Results of this study demonstrated that there were gaps in knowledge on how specific injection practices relate to risk of IDU-IE, such as nearly 30% of patients reporting only a low to moderate risk for very high-risk injection practices. Based on the HBM, we included information on the website to address knowledge gaps found in the baseline survey, in the hopes that individuals will change their behavior based on their perception of behavior and risk of disease severity and susceptibility. The website developed as part of this study could serve as a base to develop additional harm reduction educational interventions or digital therapeutics as ways to prevent IDU-IE.
One strength of this study is the website was found to be acceptable and accessible to patients in a hospital setting. Patients could be provided this website to use on their smartphone during their hospital stay and clinicians could suggest certain portions of the website for the patient to view based on their individual educational needs. If unable to view on a smartphone, providing tablets to view the website from guest services may be an option. Potential applications in the outpatient setting include clinicians pulling up the website during an office visit to provide tailored patient education and providing the website link to patients, along with specific content recommendations, in patients’ ambulatory instructions. Other educational interventions have been designed but they may be limited in their accessibility, as they are at cost or require an in-person educator along with an initial and booster educational session which may not be feasible in all settings. 17 Our website also allows clinicians to have access to this information to help their patients.
Education alone is unlikely to significantly decrease complications of IDU. Acknowledging this, the website developed as part of this study provides patients with options for safer injection practices and equipment. For instance, if a patient does not have ready access to a sterile syringe, understanding how to clean a syringe with bleach can offer a safer alternative than the continual reuse of an uncleaned syringe.
We believe that this step affected results of the Round 2 patient feedback survey, which indicated an average of “very useful” for each of the various sections of the website. Themes identified during the qualitative rapid analysis directly informed the revision process. For example, resources were added and text revisions made to describe the “why,” and “what,” and to provide a prioritization hierarchy of safety for different practices and supply options. Within results, we found a heterogeneity in preferred format and resources for learning about harm reduction. Individuals interviewed described various preferences for a particular format, aligning with common preferred learning style(s) such as visual, auditory, reading, and kinesthetic (VARK model). 20 Those who preferred video may prefer a visual style of learning, and those who prefer print material suggest a reading learning style preference. Based on these results, we included visual, auditory, and reading resources on the patient website. Future versions with an expanded budget could build on this by adding additional short video clips and other interactive, visual content.
This study has several limitations. Our patient baseline and website feedback survey data were gathered from a single site, with a small number of participants recruited in the hospital setting. Thus, results may not be generalizable. We lack response rate data from the Patient Baseline Survey and interviews, making it challenging to determine the scope of nonresponse bias in this sample. Our clinician survey results had a low response rate and could introduce nonresponse bias. We acknowledge that access to this intervention in the real world has implementation barriers such as: laptop or tablet access, smartphone access, and internet access. Rapid qualitative analysis focuses on a high-level, general analysis, and may not be able to characterize detailed, nuanced findings. In addition, due to real-world constraints, we were unable to conduct interviews until data saturation, so it is possible key themes were missed.
Future research should determine if harm reduction websites can affect patient behavior and decrease the negative consequences that individuals who use substances experience. In addition, content created could serve as a base to develop additional interactive digital therapeutic harm reduction interventions to target prevention of IDU-IE.
A patient and clinician-informed website on IDU-IE has helpful information for both patients and clinicians to use as a patient education resource, and participants in this study were overall satisfied and reported that they would likely use the content. This study adds to the body of literature supporting engagement of people with lived experience in the feedback process for patient education materials.
Supplemental Material
sj-docx-1-saj-10.1177_29767342241267077 – Supplemental material for Development of a Patient and Clinician Informed Website on Injection Drug Use Related Infective Endocarditis
Supplemental material, sj-docx-1-saj-10.1177_29767342241267077 for Development of a Patient and Clinician Informed Website on Injection Drug Use Related Infective Endocarditis by Carolyn A. Chan, Rebecca Minahan-Rowley, Emma T. Biegacki, Kimberly L. Sue and Melissa B. Weimer in Substance Use & Addiction Journal
Footnotes
Acknowledgements
We would like to acknowledge Shawn Cohen, MD, for this review of the survey and website content. In addition, we are grateful for Peyton Cabaniss, MPH, for her assistance in conducting patient interviews. We extend our gratitude to Heather Strycharz for her assistance as the web developer for the patient website.
Authors’ Note
A portion of the baseline survey results were presented at the Society of General Internal Medicine National Conference via a poster on May 13, 2023.
Author Contributions
CAC, KLS, and MBW originated the project. MBW obtained project funding. CAC, RMR, ETB, conducted the semi-structured interviews and disseminated the surveys. CAC, RMR, ETB, KLS, and MBW conducted the qualitative analysis. CAC and MBW conducted the quantitative analysis. All authors participated in interpreting the results, contributed to the writing of the manuscript, provided critical feedback to the manuscript, and approved the final manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to acknowledge the Yale New Haven Hospital Medical Staff Fund for providing funds for patient and resident gift cards, as well as providing funding for the development of the website.
Compliance,Ethical Standards,and Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. The Institutional Review Board (IRB) at the Yale University acted as the central IRB, whose review was accepted and the study protocol deemed exempt. All participants provided verbal informed consent for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.