
Abstract
Prenatal alcohol exposure and fetal alcohol spectrum disorders (FASDs) remain critical public health issues. Alcohol use in pregnancy is a leading preventable cause of birth defects, developmental disabilities, and learning disabilities. Alcohol screening and brief intervention (SBI) is effective at reducing excessive alcohol use. However, this clinical preventive service remains critically underutilized in primary care. In 2014, the Centers for Disease Control and Prevention called for the creation of FASD Champion programs to promote clinician education about FASDs. Six professional health organizations and groups providing reproductive and child health services set out to create FASD Champion programs. The American College of Obstetricians and Gynecologists FASDs Prevention Program was created to focus on reducing alcohol-exposed pregnancies. The American Academy of Pediatrics’ Champion program maintains the goal of improving health outcomes for children with FASDs by improving pediatricians’ diagnostic capacity. The American Academy of Family Physicians has prioritized training family physician champions to improve the delivery of alcohol SBI among adult patients. The University of Alaska Anchorage has partnered with the National Association of Nurse Practitioners in Women’s Health, the American College of Nurse-Midwives, and the Association of Women’s Health, Obstetric, and Neonatal Nurses to assure advanced practice registered nurses and midwives have the knowledge and skills to prevent alcohol-exposed pregnancies and FASDs. The American Association of Medical Assistants has prioritized expanding the knowledge and skills of medical assistants related to promoting alcohol-free pregnancies. Finally, the Champions program at the University of Texas at Austin was established to train health social workers in alcohol SBI. Through the advocacy, education, and mission of these 6 health sectors in collaboration with national organizations and educational institutions, the evidence-based approach of alcohol SBI is being disseminated throughout the United States to reduce the harmful effects of prenatal alcohol exposure.
Highlights
The Centers for Disease Control and Prevention-sponsored Collaborative for Alcohol-Free Pregnancy has successfully been implemented in 6 health sectors: Obstetrics and Gynecology, Pediatrics, Family Medicine, Nursing, Medical Assistant Programs, and Social Work.
Fetal Alcohol Spectrum Disorder (FASD) champions within these 6 sectors educated over 7800 clinicians and trainees about the dangers of alcohol use in pregnancy between 2018 and 2022.
Stigma, bias, and trauma are prevalent and must be highlighted in tandem with FASD education.
Background
Prenatal alcohol exposure and fetal alcohol spectrum disorders (FASDs) remain critical public health issues. Recent data show that nearly 1 in 7 pregnant people report current drinking, meaning at least 1 drink of any alcoholic beverage in the past 30 days. 1 Furthermore, about 1 in 20 pregnant people report binge drinking, defined as consuming 4 or more drinks on 1 occasion at least once in the past 30 days. 1 While few estimates for the full range of FASDs are available, experts estimate that up to 1 in 20 U.S. school children may have FASDs. 2 In addition, prenatal alcohol use is a leading preventable cause of birth defects, developmental disabilities, and learning disabilities. 3
More than 30 years of research has revealed that alcohol screening and brief intervention (SBI) is effective at reducing excessive alcohol use. A recent systematic review of SBI to reduce alcohol exposure in pregnancy, which included 11 randomized control trials and more than 12 000 patients, concluded that SBI may be effective in promoting abstinence or reducing alcohol use in pregnant and postpartum people. 4 A major limitation in interpreting these results centered on the self-reported outcomes that may have been impacted by social stigma, self-stigma, and recall bias. In addition, effective interventions were longer in duration with more frequent engagements compared to ineffective interventions. 4 Regardless of these limitations and based on the overwhelming body of evidence of efficacy for SBI that spans decades long, the U.S. Preventive Services Task Force and many other organizations recommend alcohol SBI for all adults in primary care, including pregnant people. 5 Yet, this clinical preventive service remains critically underutilized in primary care. A 2020 Centers for Disease Control and Prevention (CDC) report found that although 81% of adults in 13 states and Washington, D.C. reported being asked by their healthcare provider about alcohol use, only about 38% reported being asked about binge drinking during a routine checkup in the last 2 years. 6 Among adults who reported being asked about their alcohol use in the past 2 years and reported current binge drinking, 80% (or 4 of 5 persons) were not counseled to reduce their drinking. 6
To combat the effects of excessive alcohol use and prenatal alcohol exposure among people who can become pregnant, in 2018 the CDC put out a Notice of Funding Opportunity for the creation of national partnerships to address prenatal alcohol and other substance use and FASDs. The goals of this CDC-funded Collaborative for Alcohol-Free Pregnancy were to (1) promote the prevention of FASDs, (2) encourage early identification and management of infants and children with FASDs through national medical societies and professional organizations with active health professional memberships, (3) implement alcohol SBI within healthcare systems providing women’s health services, (4) raise awareness about the risks of prenatal alcohol exposure and improve understanding about individuals affected by FASDs, and (5) promote the prevention of FASDs and care of individuals living with these conditions. To attain these goals, a “champion” model was employed by 6 professional health organizations and groups answering this call to prevent FASDs.
The “champion” model has been around since the 1960s and focuses on implementing innovative measures through the use of “change champions” who communicate, educate, and promote novel organizational messaging. 7 Effective champions tend to exhibit 6 key elements: influence, ownership, physical presence at the point of change, persuasiveness, grit, and participative leadership style. 8 Champion programs have been found in many sectors of healthcare to help implement change. 9 In this document, we will present narratives from all 6 health sectors that have created FASD Champion programs.
American College of Obstetricians and Gynecologists FASDs Program
The goal of the American College of Obstetricians and Gynecologists (ACOG) FASD Prevention Program is to reduce alcohol-exposed pregnancies. To reduce bias, ACOG recommends that routine questionnaires or verbal screening for substance use disorders be applied equally to all people, regardless of age, sex, race, ethnicity, or socioeconomic status. 10 Trained obstetrician-gynecologist champions support this effort by engaging and educating peers, residents, and others in related medical fields regarding the prevalence of risky drinking and FASDs, the effects of alcohol exposure in pregnancy, and the effectiveness of alcohol SBI and referral to treatment. There are 19 ACOG FASD champions spanning all 12 ACOG districts and 98 sections inclusive of several countries in South and Central America. In alignment with ACOG guidance, ACOG FASD champions lead presentations on FASD prevention and develop and share resources, including educational handouts and online training available for continuing medical education credit. ACOG FASD champions also participate in writing articles for newsletters and other media outlets and act as spokespersons for eliminating alcohol exposure to pregnancy. All resources and presentations are offered free of charge and incorporate a variety of options including presentations at grand rounds. Dedicated ACOG staff provide seamless continuity and organization across districts for champions.
Since June 2019, ACOG FASD champions have given more than 200 presentations educating over 4800 individuals about the risks of prenatal alcohol exposure. Champions have successfully provided educational sessions for 30% (95/300) of ob-gyn residency programs.
A unique attribute of presentations given by ACOG champions is the inclusion of birth mothers as co-presenters providing testimonials regarding their experience during pregnancy and now as parents to children affected by prenatal alcohol exposure. This collaborative presentation occurs in partnership with FASD United (formerly NOFAS) and is consistently highlighted by attendees as a powerful adjunct to the learning experience. Since transitioning to co-presentations for grand rounds 75% (109/144) of these presentations have included a birth mother.
The COVID-19 pandemic created the need for pivoting from in-person educational engagement by ACOG FASD champions to virtual presentations and more focused social media engagement. Through the implementation of virtual learning, there has been an expansion in reach providing presentations and newly implemented residency Journal Clubs focused on the effects of prenatal alcohol exposure. There has also been a launch of social media campaigns emphasizing the prevalence of prenatal alcohol use, FASDs, and associated birth defects and developmental disabilities. Virtual presentations have allowed consistent involvement of birth mothers at each seminar and increased reach across all ACOG districts and sections.
Obstetrician-gynecologists provide a point of entry to health care for a large segment of the population. Educating residents, attendings, and others in the medical field about the dangers of prenatal alcohol exposure will help to identify at-risk patients. The training and use of alcohol SBI will facilitate referral of those who are highly motivated to eliminate alcohol use, thereby improving both prenatal and child health.
American Academy of Pediatrics: Approaches to Reaching Healthcare Providers Regarding FASDs Awareness and Prevention
The American Academy of Pediatrics (AAP) Champion program was established with the overarching goal of improving health outcomes for children with FASDs by improving pediatricians’ diagnostic capacity and addressing the role of stigma and bias in screening for prenatal alcohol exposure. The Champion program was implemented by the FASD regional education and awareness liaisons with representation from each of the 10 AAP districts. The champions serve as subject matter experts and provide clinical oversight to AAP educational programming regarding FASDs (eg, conference presentations, grand rounds).
In partnership with the University of California San Diego and the University of Wisconsin Madison, an environmental review was completed to assess the educational needs of pediatricians. The training needs for this audience include (1) understanding FASD screening, assessment, and diagnostic standards; (2) arranging care coordination; (3) recognizing implicit bias; and (4) providing family support. In response, a series of 4 educational modules were developed for use by the FASD champions. These were used in live-learning instruction (webinars, grand rounds, conferences) and served as the basis for online curricula and blended learning. Annually, this education reached over 750 learners per year or approximately 3000 learners in a 4-year period.
Pediatricians play an important role in the identification of children with prenatal alcohol exposure and access to integrated care for children with FASDs. 11 Each of the 4 modules reinforced universal screening for prenatal alcohol exposure as an effective method for overcoming stigma and reducing implicit bias. Through these training sessions, learners were encouraged to reframe parents with risky levels of alcohol consumption as individuals with a chronic health condition rather than individuals who used alcohol during pregnancy. Furthermore, learners were provided with a sample script and a methodology for developing their talking points to improve their comfort level in discussing prenatal alcohol exposure with families. Specifically, 1 module used a contact-based educational strategy as taught by a pediatrician and parent pair. While research predicted the efficacy of this approach, the results proved to be pivotal in facilitating pediatricians’ ability to internalize a recovery-friendly and family-centered approach to this patient population. 12 Specifically by having a parent of a child with FASD emphasize from a parent’s perspective how meaningful it was to be addressed with recovery-friendly and family-centered language, pediatricians became more open to this approach and regularly reassessed their assumptions about who consumed alcohol during pregnancy.
American Academy of Family Physicians: Alcohol SBI Office Champions Quality Improvement Model
Alcohol SBI offers an evidence-based approach to help patients make healthier choices regarding their alcohol use. Family physicians are in a prime position to address excessive alcohol use in adults, especially among people who can become pregnant to prevent FASDs. In 2019, the American Academy of Family Physicians recruited family medicine practices to participate in the alcohol SBI Office Champions Quality Improvement Program. The goal of the program is to train family physician champions and office champions to improve the delivery of alcohol SBI among adult patients; lead efforts to reduce rates of excessive alcohol use and prevent FASDs; integrate alcohol SBI and other system changes into daily office routines; and determine whether the Office Champions Quality Improvement Model is feasible, effective, and sustainable for all family physicians. Family physicians may not be using validated tools to objectively screen for excessive alcohol use in clinical practice and may also lack self-efficacy in patient counseling. This program gives family medicine practices the opportunity to implement underutilized health screening tools for alcohol SBI within primary care and focuses on physicians treating people with excessive alcohol use problems as they would any other illness.
Physician champions are responsible for ensuring that fellow clinicians and staff support the project, while office champions are responsible for facilitating the internal project team, recommending strategies, and implementing office system changes to integrate the revised alcohol SBI activities into the clinic workflow. During 3 years of program implementation, each of the 14 practices conducted 50 random chart reviews from patients seen within the past 12 months during baseline, mid-, and endpoint, with an aggregate total of 2723 patient charts reviewed. The evaluation found a 20% increase in alcohol SBI, a 45% increase in the use of the AUDIT-C screening tool by endpoint, and a 28% increase in the provision of brief intervention by endpoint. The sustainability survey showed 83% of champions were confident enough to continue the ASBI program in their practice.
The program hopes to reduce stigma and increase patient receptiveness by informing patients that everyone gets screened. Implementing universal alcohol screening helps practices provide more equitable health care. In implementing alcohol SBI within the office routines, family medicine practices face many barriers and challenges, such as shifting healthcare system priorities; the need to maintain clinic engagement; patient resistance to alcohol SBI; time constraints on performing brief intervention; insufficient institutional buy-in; and a lack of access to behavioral health integration. Resources from this project will help family medicine practices overcome barriers and incorporate effective alcohol SBI.
Women’s Health Nurses and Midwives Collaborative for Alcohol-Free Pregnancy
Since 2018, the University of Alaska Anchorage has partnered with the National Association of Nurse Practitioners in Women’s Health (NPWH), the American College of Nurse-Midwives, and the Association of Women’s Health, Obstetric and Neonatal Nurses to assure advanced practice registered nurses (APRNs) and midwives have the knowledge and skills needed to prevent alcohol-exposed pregnancies and FASDs. This partnership is known as the Women’s Health Nurses and Midwives Collaborative for Alcohol-Free Pregnancy (WHNMCAP).
WHNMCAP team conceptualizes a champion as any APRN or midwife who engages in efforts to raise awareness among their colleagues and/or clients about FASDs and the health risks of alcohol misuse (including alcohol-exposed pregnancies). Champions promote effective strategies for reducing alcohol use during pregnancy (ie, alcohol SBI). Content expertise is not required, which allows for the recruitment of interested people who are then trained and supported in their champion efforts. To reach potential champions across all 3 organizations, WHNMCAP developed a novel six-part video series, I am a champion because . . . in which champions from across the discipline shared their stories about how they first learned about FASDs and why they became champions for FASD awareness and prevention. These videos were then shared on the WHNMCAP website and YouTube channel, made available through virtual conference booths at conferences, and played as advertisements at the 2021 NPWH annual conference. The series has been further expanded upon in the new FASD Champions Connect webinar series, where existing champions share their stories and answer questions about how their work makes them champions. These discussions often include a significant focus on health equity and stigma and have included the perspectives of individuals and families affected by FASDs. To accommodate the target audience’s busy clinic schedules, these short webinars are recorded for later viewing on WHNMCAP’s YouTube channel.
The WHNMCAP team found several barriers to implementation. Outreach and champion recruitment were conducted across 3 different organizations with different organizational structures. These structures included state-based sections and chapters, where not all states had representation. One organization did not divide its membership by state or regionally. This required us to have a flexible approach to implementing champion recruitment and engagement.
Partner organizations did not have an existing champions’ network upon which to build these efforts; the recruitment, networking, and support program described here had to be developed from the ground up. Furthermore, champions may be perceived as content experts, which potential champions may find intimidating. WHNMCAP needed to reduce this perception to leverage interest in promoting FASD awareness and prevention strategies and recruit people to be champions.
Finally, the development of the video series and FASD Champions Connect was done partly in response to the COVID-19 pandemic, as it limited a planned approach to outreach opportunities, champion recruitment, and training through conference presentations and exhibition booths. The pandemic also shifted focus to a comprehensive website for champion recruitment and support, which also hosts links to online training, materials to share with clients, information about the alcohol SBI implementation in clinical practice, and the development of a modular online curriculum that focuses on students’ education in APRNs and midwifery programs. These resources are shared through a WHNMCAP champion listserv and widely distributed through the partners’ social media networks.
American Association of Medical Assistants: Promoting Alcohol-free Pregnancies
The unique role and value of medical assistants in contributing to efficient clinics and high-quality patient care are repeatedly noted in recent healthcare workforce literature and research. 13 However, low wages, high turnover, inconsistent requirements around certification across states, and no universal requirements in medical assistant training programs created challenges for developing and maintaining this workforce. 14 Funding in 2014 from the CDC to the Center for the Application of Substance Abuse Technologies at the University of Nevada, Reno (UNR) and the American Association of Medical Assistants (AAMA) was used to address some of these workforce issues by expanding the knowledge and skills of medical assistants related to promoting alcohol-free pregnancies.
The AAMA is the only organization devoted exclusively to the medical assisting profession. In 2021, the AAMA reported that there are over 87 000 certified medical assistants or CMAs. In response to the CDC funding, a steering committee including AAMA representatives, medical assistant educators, and current CMAs led the efforts to help UNR staff create training activities and products. Specifically, these training activities and products were tailored to medical assistants focusing on the promotion of alcohol-free pregnancies and alcohol SBI. The use of medical assistants to provide information and messaging is essential because CDC research shows that alcohol use during pregnancy continues to be a public health concern. 1
The UNR and the AAMA found the most influential champions were medical assistant educators who instruct students in professional schools and community colleges. Two medical assistant educators identified by the AAMA joined the steering committee and provided feedback on curricula, promoted products and training, served as liaisons to medical assistant regulating/accreditation bodies, developed the curricula, facilitated connections with state medical assistant educators’ associations, and promoted the integration of curricula and standards within medical assistant certification. The unwavering support of these medical assistant educator champions enhanced the role of the medical assistant workforce in their states as advocates for alcohol-free pregnancies and alcohol SBI.
Medical assistants are often considered the bridge between patient and practitioner. 13 In this role, medical assistants can form effective relationships with patients while sharing messages about health and alcohol use. Based on UNR and the AAMA’s partnership, medical assistant educators can serve as key champions promoting both knowledge and skills at the pre-service level regarding the promotion of alcohol-free pregnancies.
Social Work at The University of Texas at Austin: Promoting Alcohol SBI
As one of the largest professions in the healthcare sector, social work can play a key role in the primary prevention of alcohol-exposed pregnancies. To help support this effort, the Health Behavior Research and Training Institute (HBRT) at The University of Texas at Austin (UT-Austin) Steve Hicks School of Social Work partnered with the National Association of Social Workers (NASW) to train and educate social workers in alcohol SBI. At over 750 000 strong, social workers are the largest providers of mental and behavioral health services in a broad range of settings, including schools, community clinics, child welfare, and correctional facilities. NASW is the largest membership association of professional social workers in the nation, with 55 state and territorial chapters as well as specialty social work associations. Together, HBRT and NASW developed and disseminated alcohol SBI messaging to reach a national social work audience. In addition, the HBRT team established the Champions program in 2020 to train health social workers within the UT-Austin community. In partnership, HBRT and UT-Austin’s Dell Medical School have built the Champions program on a foundation of expertise in alcohol SBI as well as a commitment to healthcare innovation. HBRT brings more than 20 years of experience in evidence-based interventions to prevent alcohol-exposed pregnancies, while Dell’s Department of Health Social Work is the first of its kind in a U.S. medical school, bringing together social work students and faculty on healthcare teams that include medical, nursing, and pharmacy professionals.
The program was envisioned to include 2 in-person trainings (1.5 hours each) as well as 3 CDC training modules (1 hour each) to be completed at participants’ own pace, for a total of 6 hours. Training needs for this group include (1) understanding of recent trends in risky drinking during pregnancy; (2) learning the prevalence of FASDs and other health effects of risky drinking during pregnancy; and (3) becoming familiar with alcohol SBI, including recommended screening instruments. Over 2 years, 15 champions have been trained from diverse departments, including the Musculoskeletal Institute, Gastrointestinal Clinic, Post-COVID clinic, and Women’s Health Department. Two key concepts have been embedded throughout the training to address health equity and implicit bias. One is that the increase in excessive drinking among people who could become pregnant is a significant public health issue since rates of alcohol-related harms increase at lower levels of drinking compared to men. At the same time, the training has emphasized universal screening—that is, screening for all adults 18 and older—as the U.S. Preventive Services Task Force recommends.
The COVID-19 pandemic has posed a barrier to implementation of the program. Although many social workers have faced increased workloads as they serve patients dealing with COVID-19, 15 the champions trained at Dell Medical School are better prepared to integrate primary prevention into routine practice.
Lessons Learned and Emerging Themes
Following the call to action by the CDC in 2014, 6 health sectors mobilized to create FASD prevention programs. These FASD Champion programs in partnership with several national health organizations and universities have focused on clinician education regarding the risks of prenatal alcohol exposure and training to utilize the evidence-based approach of alcohol SBI. While all 6 sectors were funded through the CDC, there was no specific format in which outcomes had to be presented and no specified structure for how SBI had to be implemented. Some disciplines used in-person or live training programs which allowed for real-time numeric accounting of educational reach. The 2 disciplines that utilized an online or curriculum-based approach did not have specific numbers to indicate reach, rather those videos and curricula were their products.
In compiling the experiences across these 6 health sectors, several themes emerged. At least 3 health sectors utilized the existing infrastructure of their health organization to implement their FASD Champions program. This approach provided a broad reach for education and implementation. Several organizations and groups utilized presentations at grand rounds, online modules, and social media to increase awareness of the deleterious effects of prenatal alcohol exposure (Figure 1). Through ACOG and AAP alone, more than 7800 OBGYNs, pediatricians, and trainees in these fields have received education and training to reduce FASDs. In addition, incorporating the patient’s voice proved extremely compelling for audiences where birth mothers shared their experiences.
Best practices for fetal alcohol spectrum disorders champion programs.
According to the Society for Maternal-Fetal Medicine, ACOG, the Substance Abuse and Mental Health Services Administration, and the U.S. Preventive Services Task Force universal screening of all patients are recommended.16–19 This approach is thought to promote equity in the identification of risky drinking and management through referral to behavioral health specialists. In addition to alcohol SBI and FASD education, many organizations have incorporated stigma and bias education for clinicians caring for this patient population. A recent analysis revealed that research participants viewed patients with children diagnosed with FASDs as more different, with greater disdain, and more to blame than patients with mood disorders alone or substance use disorders. 20 Trauma-informed care is also being incorporated into education. Trauma is common in patients who go on to have a child with an FASD. One study found that among 80 birth mothers of children with fetal alcohol syndrome, which is one condition along the continuum of FASDs, 95% reported a history of sexual, physical, or emotional abuse as a child or adult. 21
While all 6 health sectors note success in forming their FASD Champion programs, several pointed out challenges. Barriers to implementation at the clinician level included time constraints to perform alcohol SBI and a lack of access to behavioral health services for referral. Challenges with champion recruitment were also encountered. FASD champions are not content experts, but rather content advocates. Through telling their story and sharing their passion for this work, recruitment efforts improved. Lastly, several groups described the need to pivot during the COVID-19 pandemic. The pandemic removed several opportunities for in-person training at national meetings and resulted in a large shift to virtual presentations for several health sectors.
Conclusions
The CDC-sponsored Collaborative for Alcohol-Free Pregnancy has successfully been implemented in 6 health sectors. Several best practices for implementing SBI for alcohol use in the prenatal period were identified across 6 disciplines. Aligning and collaborating with national organizations provides established broad networks and infrastructure to spread the word and capture a large audience. Capitalizing on existing membership of national organizations and potentially their communication mechanisms (eg, monthly emails/newsletters) will help programs reach a broad audience quicker with their SBI messaging. Once stakeholders have been identified utilize in-person (eg, Grand Rounds) and virtual platforms (eg, social media campaigns, online modules) to engage and provide education. We strongly encourage partnering with patient groups at the outset of developing SBI educational materials and throughout implementation to ensure the educational output reflects their perspective and values as well, elevating patient experiences during SBI education delivery so that clinicians can self-reflect on their approach to SBI, and sharing patient stories when implementing FASD SBI education (eg, through sharing brief testimonials in video, anecdote or printed form). Each champion sector continues this work and has identified the next steps of implementation (Table 1). Lastly, stigma, bias, and trauma are prevalent and must be highlighted in tandem with FASD education. Eliminating prenatal alcohol exposure and FASDs through clinician education remains the primary focus of our 6 champion programs.
Implementation of Champion Programs for Alcohol SBI Across 6 Health Sectors.
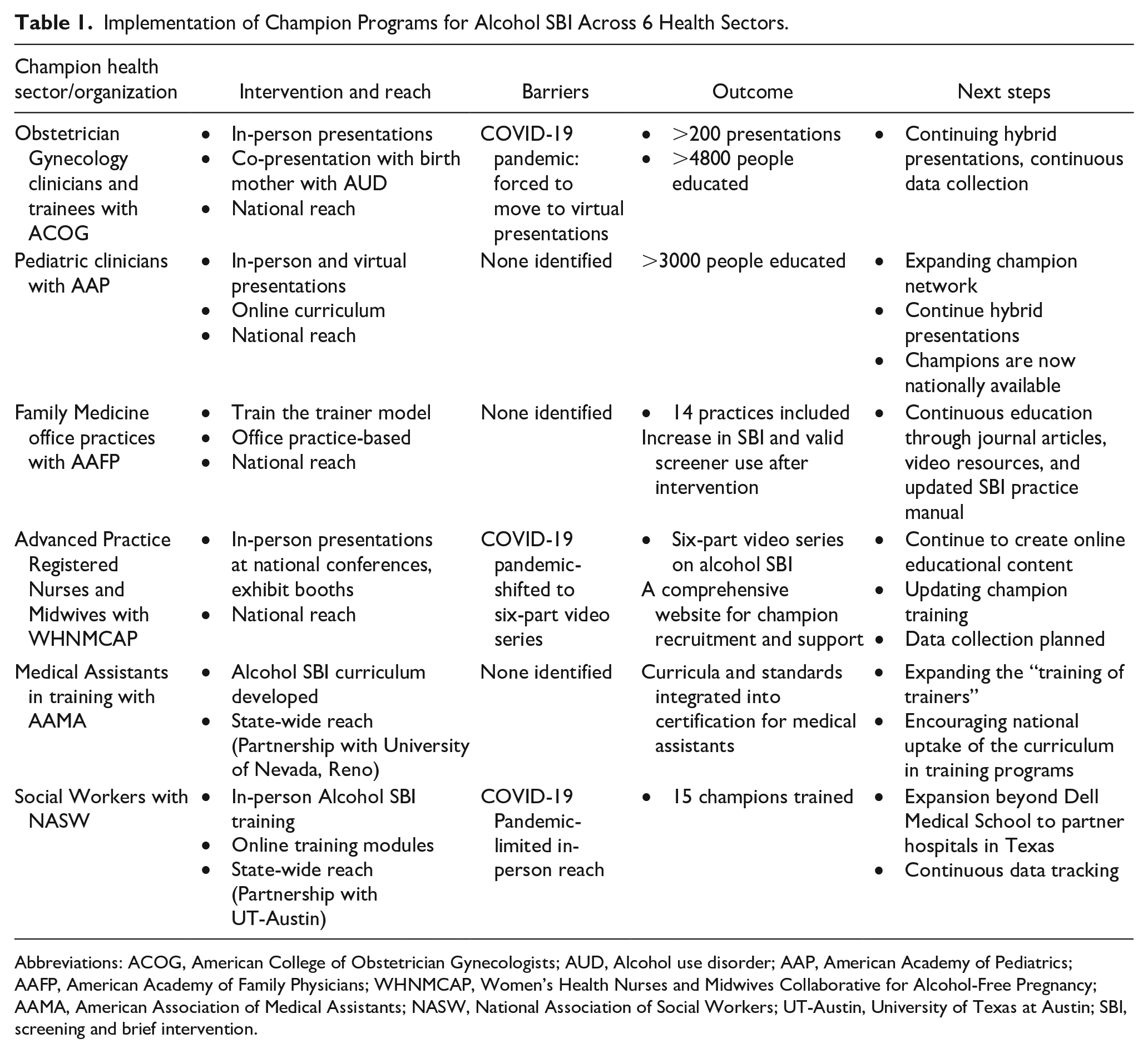
Abbreviations: ACOG, American College of Obstetrician Gynecologists; AUD, Alcohol use disorder; AAP, American Academy of Pediatrics; AAFP, American Academy of Family Physicians; WHNMCAP, Women’s Health Nurses and Midwives Collaborative for Alcohol-Free Pregnancy; AAMA, American Association of Medical Assistants; NASW, National Association of Social Workers; UT-Austin, University of Texas at Austin; SBI, screening and brief intervention.
Footnotes
Acknowledgements
We would like to thank our partner organizations: American Academy of Family Physicians (AAFP), American Academy of Pediatrics (AAP), Health Behavior Research and Training Institute/UT-Austin, Steve Hicks School of Social Work (HBRT), American College of Obstetricians and Gynecologists (ACOG), University of Nevada, Reno (UNR), American Association of Medical Assistants (AAMA), University of Alaska Anchorage (UAA), Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN), American College of Nurse-Midwives (ACNM), and National Association of Nurse Practitioners in Women’s Health (NPWH).
Author Contributions
CT, KY, and TM compiled, refined, and edited all health sector narratives. CT and KH drafted the Background, ACOG narrative, Lessons Learned, and Conclusion sections. VS drafted the American Academy of Pediatrics (AAP) narrative. HS and AH drafted the American Academy of Family Physicians (AAFP) narrative. AE drafted the Women’s Health Nurses and Midwives Collaborative for Alcohol-Free Pregnancy narrative. KP, MS, TD, and JH drafted the American Association of Medical Assistants (AAMA) narrative. KS, MV, and DL drafted the Social Work at the University of Texas at Austin narrative. All authors read and approved the final manuscript.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention cooperative agreements CDC-RFA-DD18-1801, CDC-RFA-DD18-1803, and CDC-RFA-OT18-1802. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Compliance,Ethical Standards,and Ethical Approval
Not applicable.
Consent for Publication
Not applicable.