
Abstract
Background:
Heroin-assisted treatment (HAT) is an evidence-based treatment option for opioid use disorder (OUD), available in a limited number of countries. Norway implemented a 5-year HAT project in 2022, aiming to assess its effectiveness and its potential integration into the country’s OUD treatment system. This study describes and compares patients’ baseline characteristics from the Oslo and Bergen HAT clinics, providing a comprehensive picture of the unique population and the real-world application of HAT.
Methods:
This cross-sectional study examines the baseline characteristics of consenting HAT patients within the first 2 years of operation (n = 86). Self-reported questionnaires gathered sociodemographics, previous treatment experiences, self-reported crime, and substance use, as well as motivations and expectations for treatment. Comparisons between the clinics were carried out using t-tests, Mann–Whitney U tests, Chi-square, and Fisher’s exact test.
Results:
The majority of the patients were enrolled at the Oslo clinic (76%) and were male (80%). At admission, the average age was 45.9, with a significantly younger group in Bergen (42.5 vs 47.3, P < .05). While no patients reported being unhoused, 17% noted unstable housing within the preceding month. Unemployment was prevalent (91%) alongside previous treatment experiences (95%), with a median of 2 prior medication types. In the 3 months preceding HAT initiation, 78% of patients reported being victims of crime, and 44% committed at least one crime. Over their lifetime, 2 in 5 participants (41%) had experienced an unwanted overdose and 43% had shared syringes and equipment.
Conclusion:
This study reveals a cohort experiencing societal marginalization, including unstable housing, unsatisfactory prior OUD treatment, high-risk behaviors, and frequent interactions with criminal activities, predominantly as victims. While the Oslo and Bergen clinics serve a similar patient profile, notable differences emerged in the reasons for discontinuing past OUD treatment and crime-related factors.
Keywords
Highlights
During the initial 2 years of Norway’s HAT program, 86 patients were enrolled, with the majority located in Oslo.
The patients exhibited vulnerabilities across multiple areas, such as unstable housing, unemployment, unsatisfactory past treatment, and risk behaviors.
Upon admission, patients expressed high expectations and motivation for the treatment.
The Norwegian HAT program is successfully engaging a marginalized demographic in need of such targeted interventions.
Introduction
Individuals with opioid use disorder (OUD), in particular individuals who inject drugs, are at heightened risk of all-cause and overdose-specific mortality.1,2 To address the chronic nature of OUD and reduce the risk of severe events and death, engagement and retention in OUD treatment are of particular clinical relevance.3-5 The use of medication for OUD is a widely recognized treatment approach, with methadone, buprenorphine, and a combination of buprenorphine/naloxone being common first-line therapies.6-8 Despite opioid agonist treatment (OAT) being proven to be highly effective in stabilizing and improving OUD,6,9 not all individuals start or stay in treatment long-term. 10
For a specific subset of individuals, heroin-assisted treatment (HAT) represents a viable evidence-based treatment option.11,12 HAT often adheres to strictly defined treatment criteria specifically targeting individuals with chronic and severe OUD. These patients have often undergone multiple OAT attempts and are impacted by complex health and social challenges. HAT entails the self-administration of pharmaceutical heroin (diacetylmorphine), mainly either by injection or tablets, in a supervised setting. 12 Evidence from previous studies and systematic reviews conducted in different settings consistently indicates the positive impact of HAT. It has been shown to reduce criminal activity and illicit drug use, improve health and retention rates, and enhance patient satisfaction.10,13-16
Since its initiation in 1994 in Switzerland, the availability of HAT has expanded to national health treatment systems in other countries, including the Netherlands, Germany, Denmark, and Canada. HAT trials conducted in Spain and Belgium were initiated, but have since been concluded,17,18 while the HAT pilots in Luxembourg, Norway, and Scotland are currently ongoing.19-22 In Norway, after a decade-long political discussion, 23 a 5-year HAT pilot project has been approved and started in 2022. This project aims to assess the effectiveness of HAT and its potential integration into the country’s OAT system. Further details regarding the project evaluation plans are outlined in the published protocol paper. 24
Although the treatment is delivered under the same national public health system and patients from both involved cities are enrolled in the same overall program, there may be local variations in the population it attracts and serves. Despite uniform conceptualization, nuances such as geographical differences, along with procedural and systemic variations could influence patient inclusion and engagement. This may potentially result in disparities in treatment access, with broader implications for health equity across locations. The objective of this study is to describe the baseline characteristics of patients entering into Norway’s HAT program within the first 2 years of implementation in the two cities of Oslo and Bergen and to compare the patient characteristics between those enrolled at the two clinics.
Methods
Study Setting
In Norway, the population of people who inject drugs was estimated to be nearly 8000 in 2021. 25 At the end of 2023, approximately 8500 individuals were in OAT. 26 It is estimated that within the Norwegian context, between 70 and 80% of the target group is receiving treatment. 27 Norwegian OAT is intended to be easily accessible, with short waiting lists and no fee for patients. In addition, it is integrated with psychosocial therapy and is designed to be a long-term treatment. 28 Despite high levels in access,29,30 research conducted within Norwegian context has revealed variations in patient retention rates,31,32 in line with findings from international systematic reviews.3,33 In 2023, 363 drug-induced fatalities were recorded in Norway, indicating a rising trend in the last decade.34,35 Heroin and other opioids continue to be identified as the leading causes of death and notably, the number of deaths caused by synthetic opioids was the highest recorded. 35
The Norwegian HAT pilot was introduced in Norway’s two largest cities, Oslo (about 706,000 inhabitants) and Bergen (nearly 270,000 inhabitants). 36 The clinic in Oslo opened in January 2022 and is located within the Oslo University Hospital complex. In March 2022, the clinic in Bergen was opened in a temporary location. It was subsequently relocated to another temporary location where it currently operates, with future plans to relocate to a final location within the Haukeland University Hospital. In the catchment area of Oslo University Hospital which serves approximately 523,400 individuals, the number of patients receiving OAT increased, from slightly over 800 in 2022 to around 1000 in 2023.26,30 Similarly, the larger Bergen area, with a catchment population of 465,200, also reported an increase in OAT participants from 778 to around 1100 over the same period.26,30 The differing healthcare service provision structures in the two cities impact their respective OUD population pool, affecting the number of individuals eligible for HAT and ultimately influencing the program’s potential reach within each city.
The Clinic and the Treatment
The clinics operate daily, offering 2 sessions: one in the morning and another in the afternoon. Individuals can self-administer injectable or tablet medical heroin twice daily, once during each session, with some flexibility of attending less frequently if desired. Due to the short half-life of heroin, 37 for overnight opioid coverage, patients are primarily offered take-home methadone. Some patients were alternatively offered morphine sulfate depot tablets as an option. 38 From November 2023 onward, a 24-hour morphine depot preparation was also approved and made available as an additional overnight medication choice. 39 Take-home heroin doses are not available. The staff at the clinics consists of trained nurses and (at least one) medical doctor specialized in addiction medicine. The nurses dispense the medical heroin for patient self-administration, and they also offer additional healthcare services such as health checks and wound care. Moreover, patients have access to counseling and psychosocial support, including assistance with housing, finances, and employment, provided by social educators and social workers.
Patients may spend up to 2 hours at the clinic every day, moving through different rooms for various steps in the process. 15 Upon arrival, after a potential stop in the waiting room, patients undergo a prescreening conversation with the doctor or nurses in which medical conditions, opioid score, 40 and daily dosage needs are assessed. The daily heroin dosages can be adjusted based on individual needs and clinical judgment, with potential reduction if necessary. Once approved, patients proceed to the supervised injection booths (Figure 1). In order to ensure safe administration, specific guidelines have been established, which includes indications for intravenous injection (limits on attempts and time, restrictions on injecting in risky areas like the groin and neck) and indications for intramuscular injection. After injecting, patients remain at the clinic for a mandatory observation period. Throughout this phase, clinical staff monitors intoxication levels using the opioid score and assess respiratory function and any adverse events.

Injection booths in Norwegian HAT clinics, Oslo (left) and Bergen (right).
Two years into their operation, the clinics have developed slightly different clinical routines and operations. These differences, which may be influenced by potentially different patient pools, and local contexts, could affect the appeal of the treatment. Such variations include differing prescribing practices for medications beyond HAT, distinct approaches to mitigating medication diversion risks, discrepancies in meals offered, variations in staff composition, working hours, and budget allocations.
Referral Process and Inclusion Criteria
Individuals can be referred to HAT through 3 distinct paths: primary referrals from external entities such as the Norwegian Labour and Welfare Administration (NAV), general practitioners, municipal psychologists, doctors in low-threshold health-services, and selected specialist health services; secondary or internal referrals from treatment teams within OAT and other interdisciplinary specialized addiction treatment at the same hospital; lastly, tertiary referral involves self-referral from patients who personally request to be assessed for admission.
Following a referral, individuals undergo an evaluation interview to determine their eligibility by assessing if they meet the specific criteria set for the program. The inclusion criteria are: OUD based on ICD-10 definition, current or former heroin dependence, capacity for consent, Norwegian citizenship or valid residence permit, and registered address in the local Population Register for a minimum of 3 months in the catchment area for OAT of the 2 clinics. Exclusion criteria include pregnancy, current severe risk of violence and threats, and situations that would prevent from attending appointments in the near future (ie, planned incarceration).
In the first 2 years of operation, the clinics received 167 referrals (56 Bergen and 111 Oslo), of which 37% were declined (29% in Bergen and 41% in Oslo). Three-quarters of both referrals and rejections occurred in the first year. Overall, 52% of the referrals came from the conventional OAT service at the same hospital (77% in Bergen and 39% in Oslo). NAV was the second referrals source (13% of total; 11% in Bergen and 14% in Oslo), followed by general practitioners (12% of total, 7% in Bergen and 14% in Oslo). The predominant reason cited for refusal was an “admission pause” (ie, the clinic was at maximum capacity, as set by clinic managers; 28%) followed by “history of violence” (17%) and “medication in OAT” (ie, individuals continued or started medication in OAT; 16%).
Study Design and Sample
The Norway HAT project has a prospective cohort design. Patients may participate in HAT without engaging in the research study, which involves longitudinal assessments at various intervals (baseline, 3 months, 6 months, 1 year, and then annually thereafter). Baseline questionnaires are ideally obtained within the first 2 weeks of treatment start. For those who opt into the research, written informed consent is obtained. This study examines the baseline characteristics of all patients enrolled in HAT during the first 2 years of clinic activity (January 1, 2021 to December 31, 2023), who consented to research participation and completed the baseline questionnaire.
Measures
Upon enrolment in treatment, patients complete self-reported questionnaires digitally on tablets at the clinic, either alone or with staff support if needed. They report on multiple baseline measures, including sociodemographics, education, employment, past treatment history, crime, substance use, risk behaviors, and overdose history. The majority of these variables were assessed as dichotomous responses. Moreover, participants rated 13 different statements regarding their motivation for treatment and 12 statements regarding their expectations on a scale of 1 to 5, ranging from “not important” to “very important.” Responses of “not applicable” were excluded from the analysis.
Statistical Analysis
Frequencies and descriptive analyses were performed for the various measures. Comparisons between frequencies in the 2 clinics were conducted using Chi-square tests, and Fisher’s exact test when expected frequencies were low. t-Tests and Mann–Whitney U tests were employed according to data distributions. The statistically significant level was considered as P-value < .05. All analyses were conducted using R version 4.2.3.
Results
Sociodemographic, Education, and Employment
Of 92 research participants, 6 were removed due to incomplete baseline questionnaires. Therefore, the sample size resulted in 86 patients, with the majority (71%, N = 61) enrolled in Oslo. Between the first day of medical heroin and the completion of the baseline questionnaire a median 13 days passed [interquartile range (IQR): 4.0–29.3]. The mean age at the first day of medical heroin administration was 45.9 [standard deviation (SD) 10.0], with a significantly younger group in Bergen (Table 1). The majority of patients were male (80%), and born in Norway (N = 75, 87%) with 20% having at least one parent born in a different country (N = 17).
Patient Demographics Upon Enrolment Into the Heroin-Assisted Treatment Clinics in Oslo and Bergen.
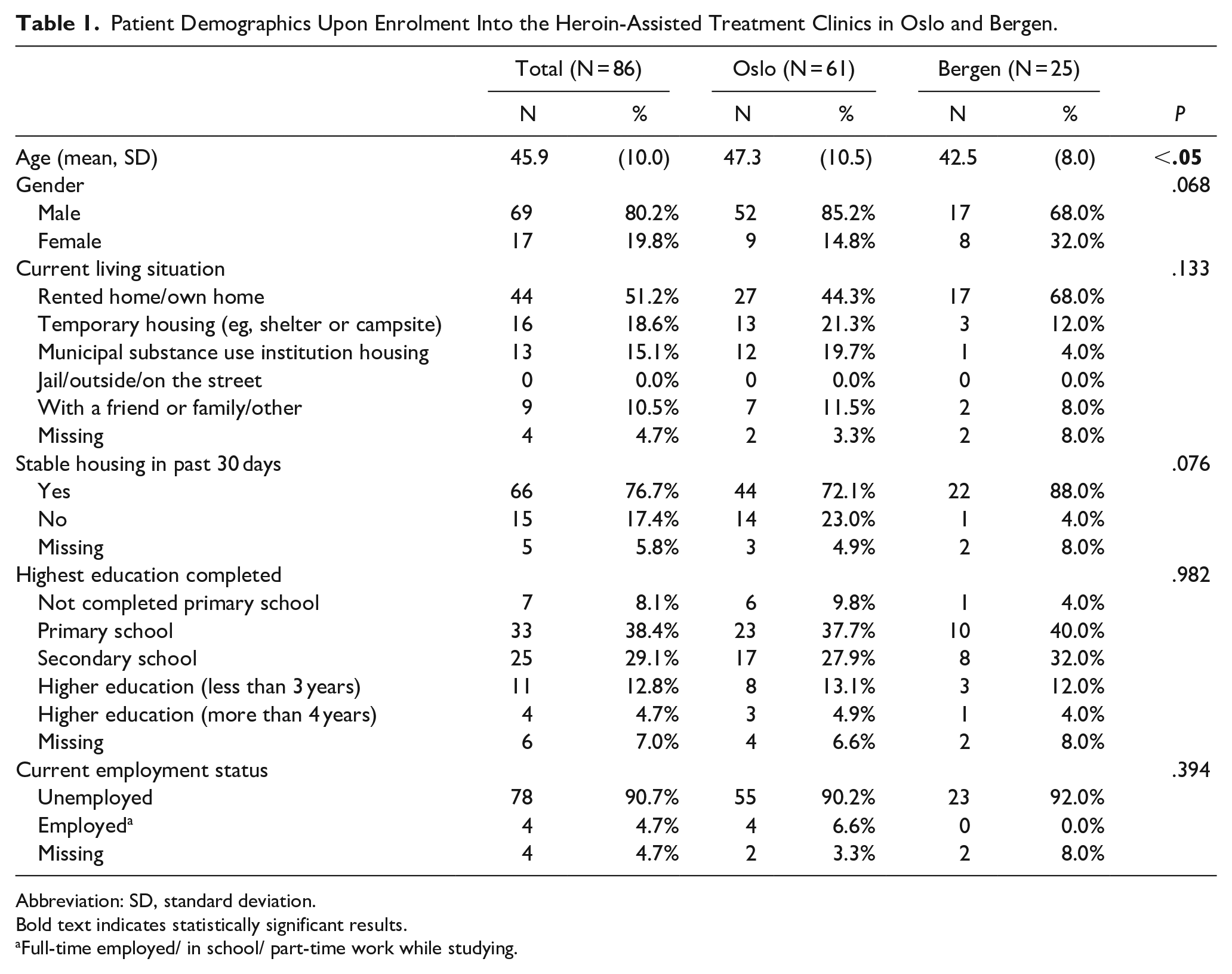
Abbreviation: SD, standard deviation.
Bold text indicates statistically significant results.
Full-time employed/ in school/ part-time work while studying.
Among participants, 43% had children (N = 37). As Table 1 shows, half of the participants (51%) lived in owned or rented housing. No participants reported being unhoused at the start of treatment. A larger proportion of participants in Bergen reported stable housing in the past 30 days as compared with Oslo (88% vs 72%), although the difference was not statistically significant. Nearly all participants were unemployed at the start of treatment, with only 4 patients reporting part-time work. Nearly half of the participants (N = 40, 47%) had not completed secondary school education and 20% of the sample reported having reading or writing difficulties (N = 17). Aside from age, no significant sociodemographic differences between Bergen and Oslo participants were observed.
Previous Treatment Prior to Starting HAT
Nearly all of the patients (N = 78, 95%) reported previous treatment experiences for substance use disorders. All patients that reported not having had previous treatment were enrolled in Oslo (N = 4, 5%). In terms of previous treatment, methadone was the most commonly prescribed medication (73%), followed by buprenorphine (51%). The median number of types of medications prescribed prior to HAT admission was 2 [IQR 1–2.8]. The majority of the patients (N = 62, 72%) defined their previous treatment discontinuation as voluntary. While there was a higher percentage of patients who left their previous treatment involuntarily in Oslo compared to Bergen (21% vs 12%), this difference was not statistically significant. Table 2 details the participants’ reasons for interrupting their previous treatment.
Previous Treatment Experiences of Heroin-Assisted Treatment Patients in Oslo and Bergen.
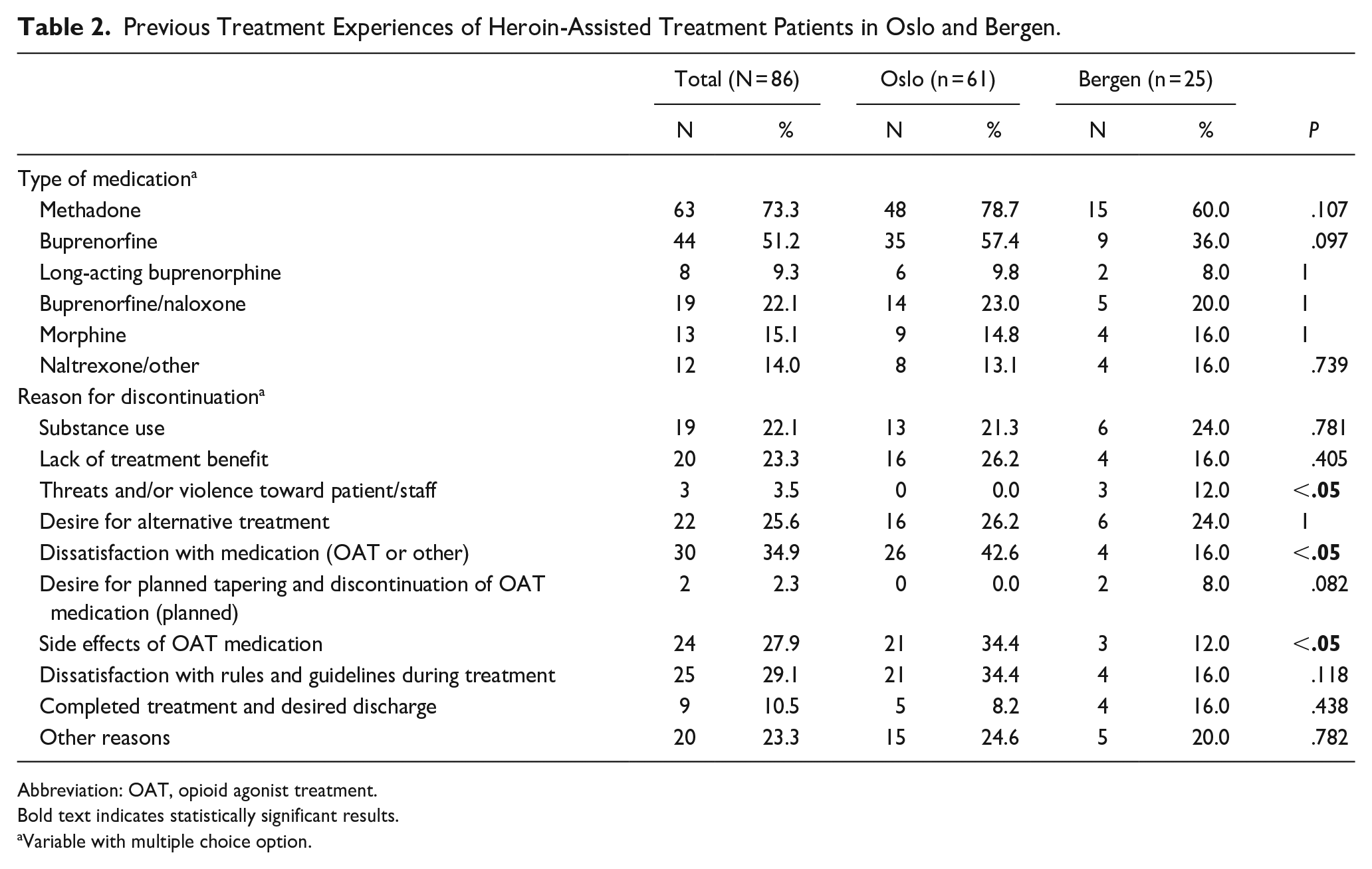
Abbreviation: OAT, opioid agonist treatment.
Bold text indicates statistically significant results.
Variable with multiple choice option.
Experienced and Committed Crime
HAT patients reported both committing crime and being a victim of crime prior to starting in HAT. In the 3 months before HAT initiation, 70% of the patients (N = 53) were victims of at least one type of crime, with a significantly higher percentage in Oslo than in Bergen (70% vs 40%, P < .05). Theft was reported by more than half (N = 49, 57%), with a median of 2 incidents in the past month. Approximately one-third (30%) suffered psychological violence or threats, with a median occurrence of 3.5 times in the past month, while a smaller percentage (13%) faced physical violence (Table 3).
Self-Reported Crime-Related Variables Upon Enrolment Into the Heroin-Assisted Treatment Clinics in Oslo and Bergen.
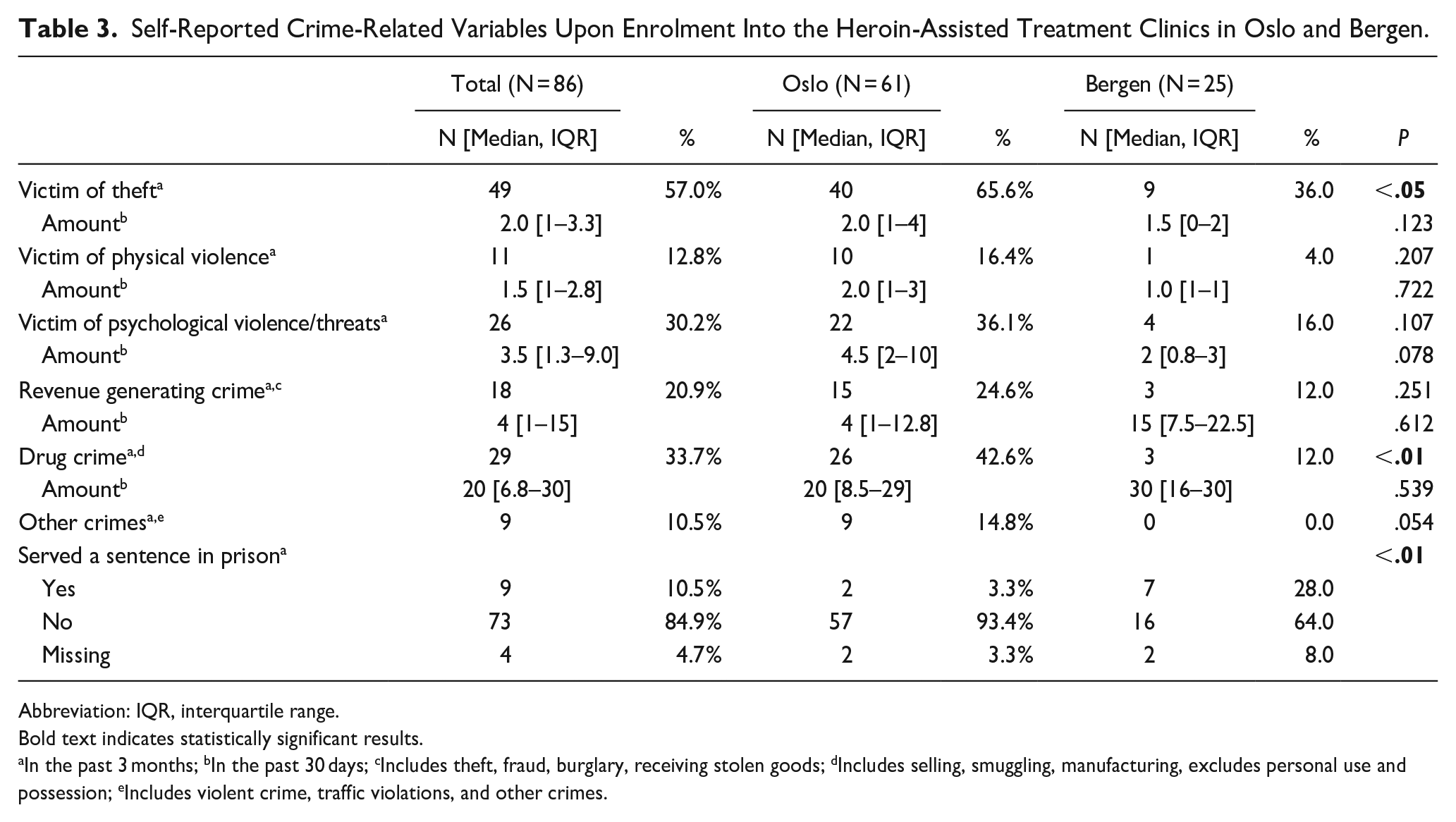
Abbreviation: IQR, interquartile range.
Bold text indicates statistically significant results.
In the past 3 months; bIn the past 30 days; cIncludes theft, fraud, burglary, receiving stolen goods; dIncludes selling, smuggling, manufacturing, excludes personal use and possession; eIncludes violent crime, traffic violations, and other crimes.
Thirty-eight patients (44%) reported committing at least one crime in the three months prior to HAT initiation, with a significantly higher proportion in Oslo compared to Bergen (56% vs 16%, P < .01). A third (34%) of the participants reported committing a drug crime, with a significantly higher proportion in Oslo than Bergen. Recent violent crime was reported by 5 participants. A significantly higher proportion of Bergen participants reported having served a prison sentence in the 3 months prior to HAT initiation (28% vs 3%, P < .01).
Substance Use and Overdose Experience
Table 4 describes the lifetime substance use among study participants. Nearly all patients (90%, N = 77) reported the use of illegal heroin, a high proportion of patients also reported lifetime use of benzodiazepines, amphetamine/methamphetamines, and cannabis (86%). The median number of lifetime use of substances was 16 [IQR 13–17]. In terms of risk behaviors, 43% (N = 37) of participants reported having previously used a syringe that was used by others, as well as other injecting equipment (cooking spoon, filtering equipment, cotton balls, or rinsing water for syringes). Of those patients, 5% shared a syringe (N = 4) and 22% had shared equipment (N = 19) in the previous 30 days. There was a statistically significant difference between the 2 cities regarding the latter risk behavior (Oslo: N = 17, 28%; Bergen: N = 2, 8%, P < .05).
Self-Reported Lifetime Use and Overdose Experience of Heroin-Assisted Treatment Patients in Oslo and Bergen.
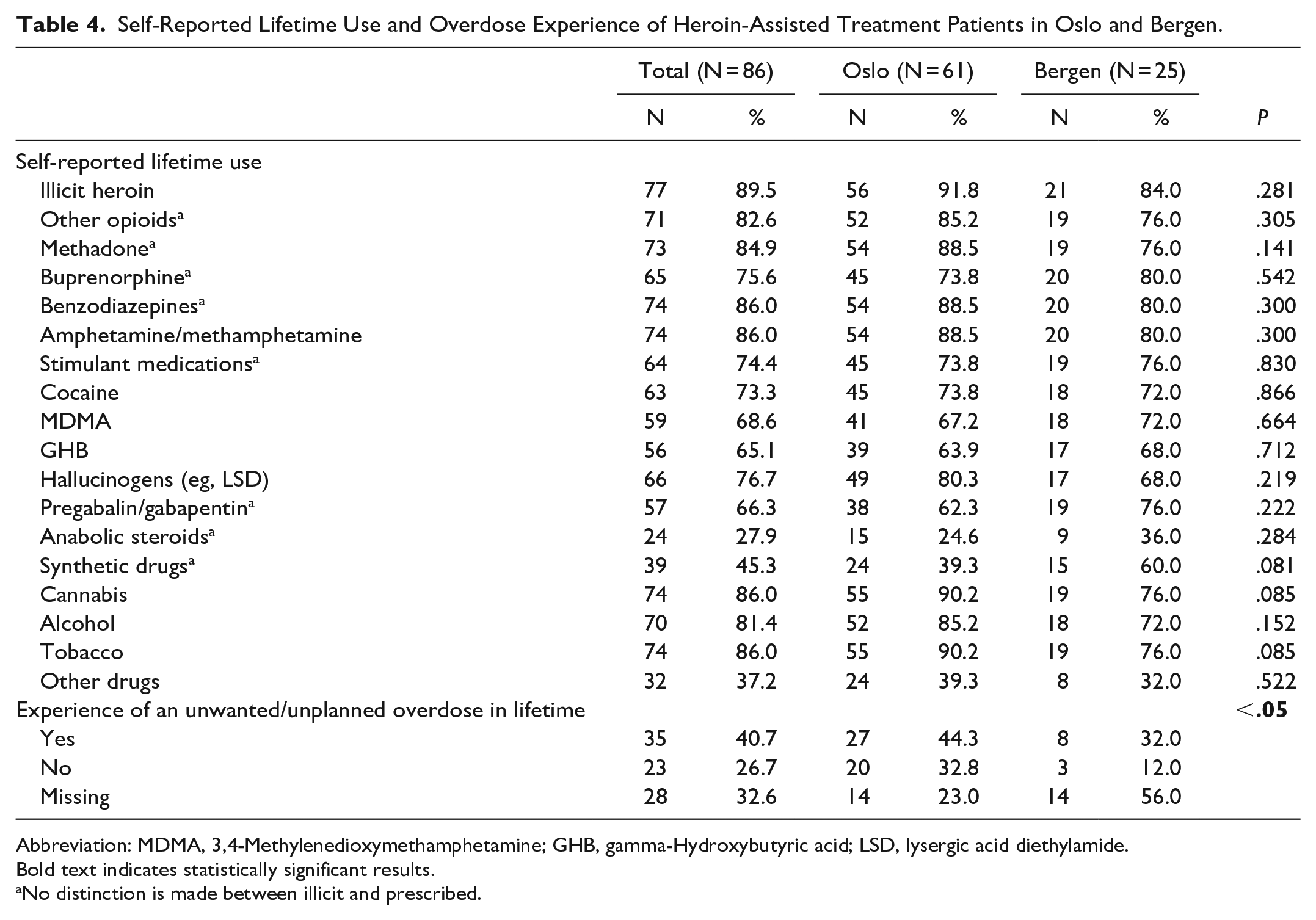
Abbreviation: MDMA, 3,4-Methyl enedioxy methamphetamine; GHB, gamma-Hydroxybutyric acid; LSD, lysergic acid diethylamide.
Bold text indicates statistically significant results.
No distinction is made between illicit and prescribed.
Unwanted or unplanned overdoses during their lifetime were reported by 41% of the participants (N = 35), with a median of 2.5 occurrences [IQR 1.3–5]. The median lifetime overdoses in Oslo and Bergen were 2 [IQR 1–5] and 3 [2–15], respectively. Among all patients, 6% had experienced 1 or more unwanted overdoses in the month prior to HAT initiation (N = 5).
Motivation and Expectations Upon Entering in HAT
When asked about the motivations for engaging in HAT (Figure 2), the response options with the highest average scores were “I need heroin, and want to get it in a legal, controlled and safe manner” (M = 4.9, SD = 0.42) followed by “I think it will contribute to an increased quality of life for me” (M = 4.5, SD = 0.85). The motivations that were scored lowest were “I want closer follow-up” (M = 3.0, SD = 1.39), “I want an intoxicating effect” (M = 3.0, SD = 1.41) and “The control in OAT made it difficult for me” (M = 3.0, SD = 1.74).
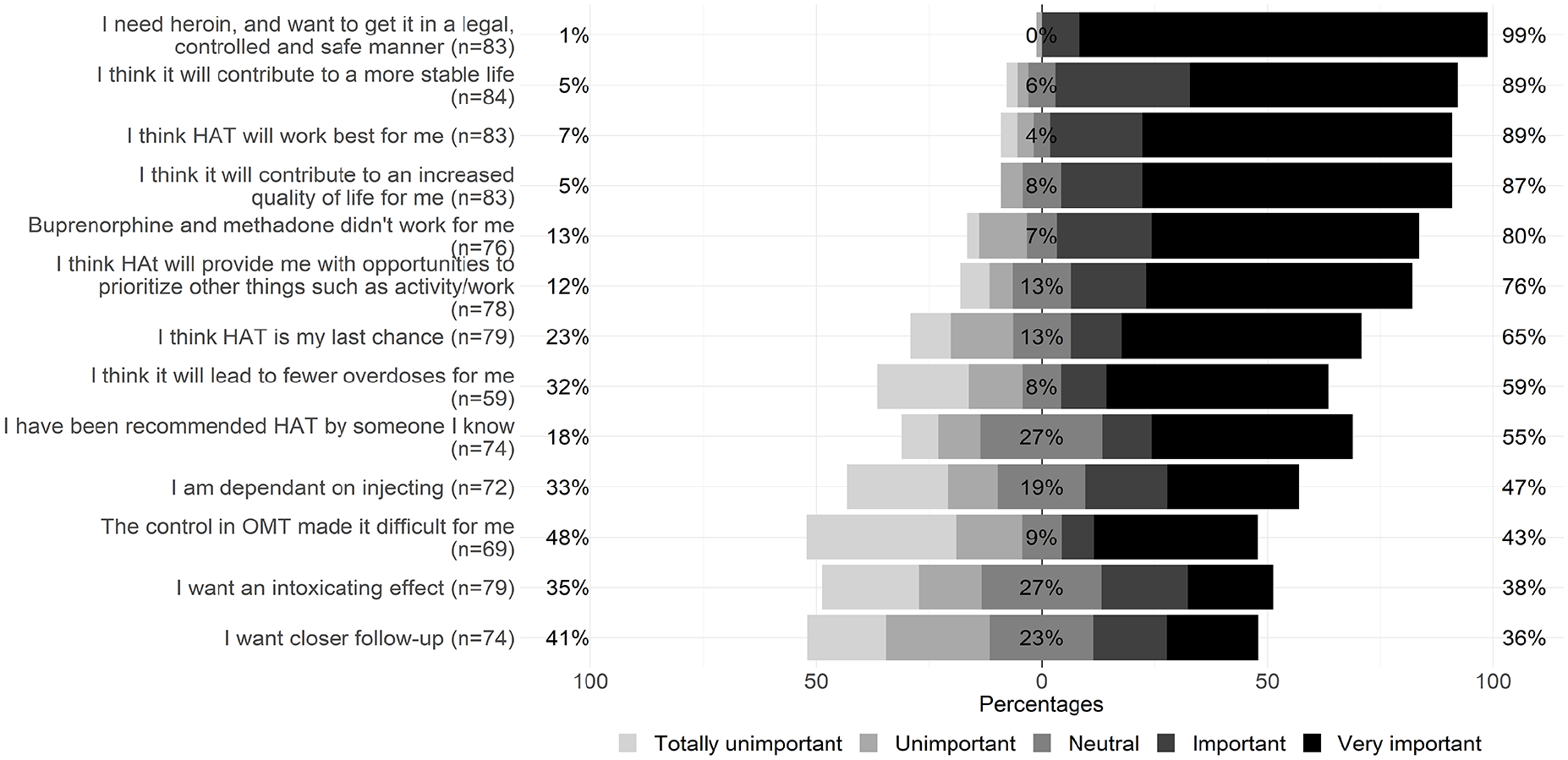
Patients reported motivations: Scoring of statements answering to question “How important are the following reasons to you when applying for heroin-assisted treatment?”. Likert plot scale with diverging stacked bar charts. The bars are centered at neutral response and their respective percentages are shown. The percentages reported on the left refer to the proportion of negative responses (totally unimportant, unimportant), while the positive responses (important, very important) are on the right. The answers options are arranged in descending order according to the positive proportion.
Patients’ expectations from the treatment are shown in Figure 3. The options with the highest average score were “I expect to satisfy my opioid addiction” (M = 4.6, SD = 0.77) and “I expect to have a better quality of life” (M = 4.5, SD = 0.79). The lowest scored expectations were “I expect life to be somewhat similar to before” (M = 2.7, SD = 1.48) and “I expect to have better housing conditions” (M = 3.7, SD = 1.40). More information can be found in Supplemental Materials.
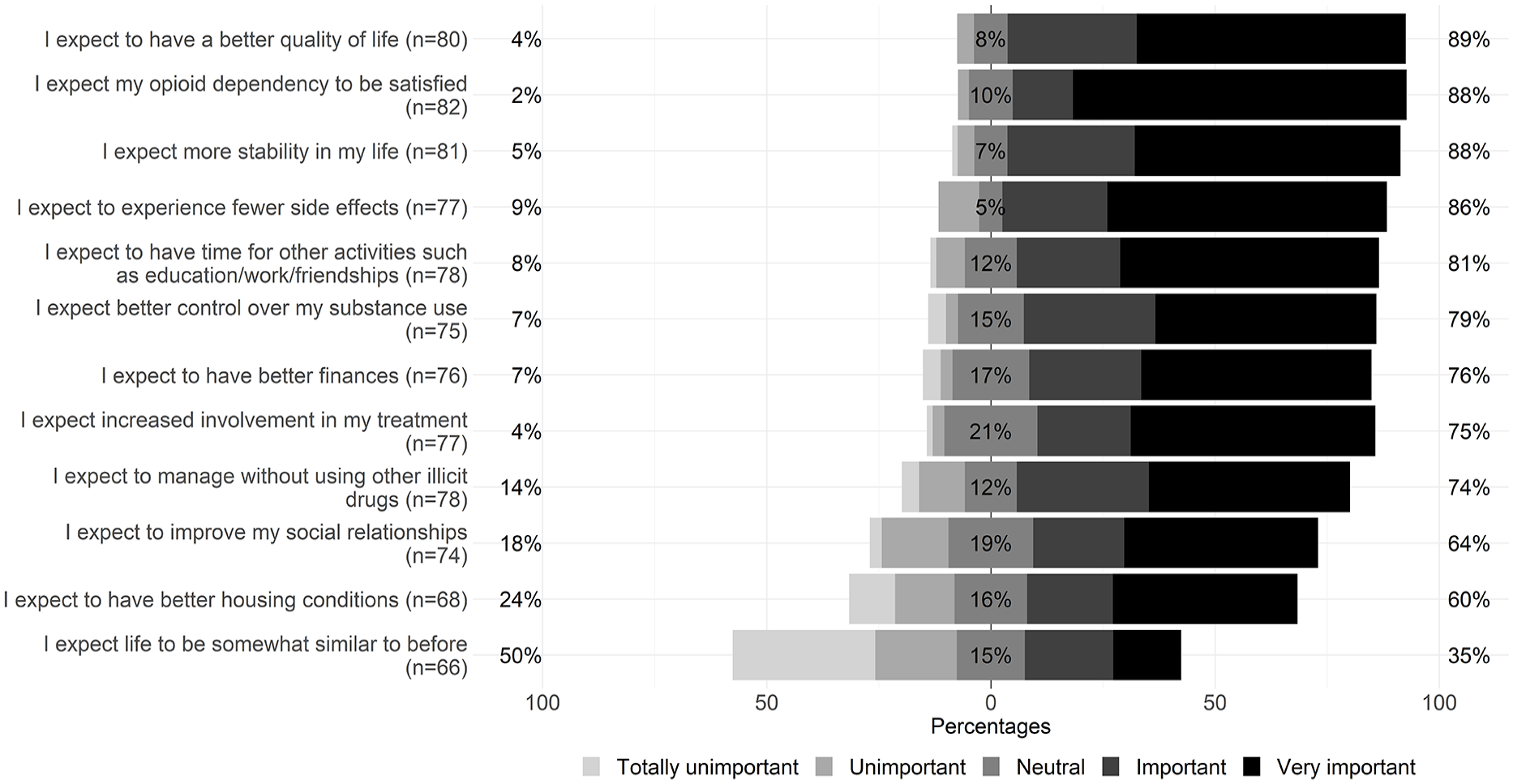
Patients reported expectations: scoring of statements answering to question “How important are the following expectations to you in regard to heroin-assisted treatment?”. Likert plot scale with diverging stacked bar charts. The bars are centered at neutral response and their respective percentages are shown. The percentages reported on the left refer to the proportion of negative responses (totally unimportant, unimportant) while the positive responses (important, very important) are on the right. The answers options are arranged in descending order according to the positive proportion.
Discussion
This study describes patients who enrolled in Norway’s first HAT program. The baseline characteristics present an overall marginalized group, many with housing instability, previous unsatisfactory treatment experiences, exposure to crime (both as victim and perpetrator), and risk behaviors. The findings demonstrate that the Norwegian HAT program seems to reach the targeted at-risk population.
The gender distribution of this population is consistent with other HAT programs41,42; while the proportion of women in Norwegian OAT is higher (Bergen and Oslo both 28%). 30 The mean age at admission to HAT in Norway is higher than in HAT programs conducted in other countries.41,42 Nevertheless, the mean age aligns with the aging Norwegian OAT population (OAT mean age in Bergen = 46.3 and in Oslo = 49.5). 30 With nearly half of the participants not attaining basic education, a figure notably higher than the 20% in the general population of the 2 cities, 43 this group exhibits lower educational level, in line with a prior Norwegian OAT study. 44 The high prevalence of disengagement from education, employment, or training also mirrors the trend seen in the broader Norwegian OAT population (Bergen = 87%; Oslo = 81%).30,44
None of the HAT patients in this study reported homelessness, which may be attributed to the Norwegian municipalities’ responsibility to provide housing for those facing a housing market disadvantage, including individuals with substances use disorders.45,46 However, one-third of study participants live in temporary housing such as a shelter or municipal institutional housing, which is a higher proportion than observed among Norwegian OAT patients. Despite a fraction of the latter OAT group experiencing homelessness (4% in Bergen, 2% in Oslo), only 9% live in temporary housing, although there is a disparity between Bergen (7%) and Oslo (24%). 30 In contrast, the majority of OAT patients report renting or owning their homes. 30 Despite having housing accommodation, a notable percentage (17%) in this study reported recent housing instability, particularly in Oslo. However, in comparison with previous HAT studies, the percentage of individuals considered to have poor housing is considerably lower.41,47 In Canada, for example, three-quarters of HAT patients reported precarious housing 41 and one-third of HAT patients in Denmark report homelessness. 47 Having precarious housing remains a significant source of vulnerability for individuals with OUD and can impact their treatment outcomes 3 and recovery. 46
For other HAT programs, previous treatment experience is an intrinsic admission criterion. Norwegian admission criteria allow for those with no previous treatment, offering entry for a potentially hard-to-reach group. While this makes up a small proportion, it is possibly relevant. Haasen et al 48 found that HAT patients with no previous OAT experience had similar benefits in terms of outcomes and retention compared with those with previous experience, despite having a more severe drug use profile. This inclusivity enabled the most marginalized to access the services and engage in treatment, offering a possibility for recovery. HAT may serve as the initial step in their treatment trajectory, potentially leading to more standard types of OAT.
As previously reported, 15 dissatisfaction with past OAT experiences is common in this group. Our study shows patients often disliked OAT structure and regulatory aspects, as well as the medications and their side effects. Some significant differences in discontinuation reasons are reported across the 2 clinics, and it may reflect the different structuring of OAT services in these cities.
Participants in this study reported a notable level of recent crime victimization, with a multiple number of incidents per victim. High levels of victimization are also reported in the OAT population, and are associated with more severe substance use, poor mental health, and homelessness. 49 While this population is vulnerable both as victims and perpetrators of crimes, in our study, the latter role seems to be connected to their involvement in the “drug scene” and revenue-generating crimes. Notably, patients in Oslo reported significantly higher crime exposure than those in Bergen, potentially reflective of Oslo’s capital city status. A recent systematic review of randomized controlled trials of HAT revealed a significant reduction in criminal behavior among participants, particularly in drug-related and property offenses. 13 Violent crime was reported infrequently by HAT patients in this study. This may be due to the clinics’ exclusion of patients with a history of extreme violence.
Polysubstance use has been recognized as a potential predictor for leaving HAT and OAT.3,50 Participants in our study reported lifetime use of multiple types of substances, most frequently heroin or other opioids and benzodiazepines. Others have highlighted the complexity of polysubstance use in HAT clinics’ populations.47,51,52 Providers reported challenges in negotiating and managing the risks of polysubstance use, as they had to balance client safety by withholding doses with the desire to retain patients and avoid risk of disengagement from treatment. 51 In Denmark, the use of alcohol and benzodiazepines does not necessarily preclude individuals from receiving treatment, as long as their treatment and functionality remain intact. 53 Furthermore, in the discussion about polysubstance, there is a growing emphasis on the specific issue of cocaine use among a distinct group of HAT patients.47,52,54
Participants in this study exhibited strong motivation for engaging in HAT, which aligns with a previous study. 55 Others have reported high satisfaction with HAT, although the highly structured setting has been viewed as a barrier for some patients.15,51 In this study, participants expressed several expectations for their engagement in the new treatment. The highest scored expectation related to improvement in their quality of life, which is consistent with the aim of the program. The emphasis on quality of life in both motivation and expectations is encouraging, as HAT has been shown to improve quality of life.56,57
Strengths and Limitations
This study acknowledges a set of specific limitations. First, our analysis relies on a relatively small sample size, reflecting the niche target demographic of the Norwegian HAT program; yet it is representative as almost all of HAT patients in Norway are included in the study, and enhancing the validity of our findings despite some missing data. The intent of this study was not to generalize or determine causality, but to provide an in-depth description of the profile of this particular patient group. Accordingly, these findings should be regarded in their specific context and not extended beyond this distinct population. Despite these constraints, the study offers a thorough, nuanced portrait of the cohort.
Second, this study employs self-reported data, collected within the clinical environment and occasionally with staff assistance, and as such it may introduce potential biases such as social desirability, particularly given the sensitivity of the topics addressed. Participants’ awareness of the project’s evaluative nature might also lead to underreporting of counternormative behaviors. While these factors can affect the accuracy of self-report measures, their impact on the overarching goals of this baseline article is likely relatively limited, as the primary objective is to establish an initial understanding of the patient population’s characteristics, rather than assess treatment outcomes or behavioral changes.
Conclusion
The findings from the initial 2 years of enrollment in Norway’s HAT underscore the high levels of marginalization experienced by this cohort, confirming the HAT program’s success in engaging a high-risk population in need of specialized treatment. The Oslo and Bergen clinics cater to a similar patient profile across several explored dimensions, with some differences observed in crime-related factors. By capturing the complexities of this vulnerable demographic, the study highlights the critical role of HAT in addressing the multifaceted challenges of OUD within this specific subset. However, after 2 years of operation in the 2 largest cities, a relatively low number of admissions have taken place. This may partly reflect the limited population that finds the program sufficiently attractive, but it may also reflect limited treatment capacity at the 2 clinics during the program’s initial phase. This aspect should be explored further. Moving forward, planned research initiatives aim to further explore the impact of the HAT program on participants’ outcomes.
Supplemental Material
sj-docx-1-saj-10.1177_29767342241271991 – Supplemental material for Patient Characteristics From Norway’s First Heroin-Assisted Treatment Clinics
Supplemental material, sj-docx-1-saj-10.1177_29767342241271991 for Patient Characteristics From Norway’s First Heroin-Assisted Treatment Clinics by Francesca Melis, Thomas Clausen, Charlotte Castel, Omid Dadras, Silvana De Pirro, Lars Henrik Myklebust, Ann Oldervoll, Linda Elise Wüsthoff and Desiree Eide in Substance Use & Addiction Journal
Footnotes
Acknowledgements
We are deeply grateful for the clinic staff and study participants, whose combined involvement is essential to this research.
Author Contributions
FM has been involved in conceptualization, data curation, formal analysis, writing–original draft, writing–review and editing. TC has been involved in conceptualization, project administration, writing–review and editing, supervision. CC has been involved in implementation and verification of the statistical analysis, writing–review and editing. OD has been involved in writing–review and editing. SDP has been involved in writing–review and editing. LM has been involved in writing–review and editing. AO has been involved in writing–review and editing. LW has been involved in conceptualization, writing–review and editing. DE has been involved in conceptualization, writing–review and editing, supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Directorate of Health; Norway, Evaluation of HAT clinics research grant; 20/00546.
Compliance,Ethical Standards,and Ethical Approval
REK approval (195733).
ORCID iDs
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.