
Abstract
Background:
Hospital policies play a role in healthcare providers’ decision-making about reporting birthing people who use drugs to child welfare. This study sought to understand how these specific hospital policies are made.
Methods:
We conducted semi-structured interviews with healthcare professionals involved in developing or revising hospital policies related to child welfare reporting for birthing people who use drugs. The interview guide was informed by an implementation science framework and focused on participants’ experiences developing or revising these policies. We coded transcripts inductively, focusing on themes that emerged in the interviews themselves, and deductively, focusing on pre-determined aspects of the policy development process.
Results:
Participants (N = 16) were physicians (69%), registered nurses (19%), and social workers (12%). The sample was drawn from all regions of the United States. Two themes emerged in data analysis. The first theme was that urine drug testing policies for pregnant and birthing individuals are seen as part of hospital child welfare reporting policies. Specifically, participants often described child welfare reporting policies as including criteria for urine drug testing and explained that the connection between urine drug testing and child welfare reporting policies was by design. The second theme was that the content of hospital child welfare reporting policies is a result of hospital politics and a focus on legal compliance. They described the legal compliance aspects of the hospital policies as serving to protect the institution and, occasionally, individual employees from legal consequences.
Conclusion:
The content of hospital policies regarding birthing people who use drugs appears influenced by political and legal considerations more than considerations of patient or public health.
Highlights
Hospital urine drug testing policies for pregnant and birthing people are seen as part of hospital child welfare reporting policies.
The content of hospital child welfare reporting policies is informed by hospital politics and attention to legal compliance.
Introduction
Among more than 200,000 infants investigated by child welfare agencies yearly in the United States (US), about one-fourth of investigations stemmed from reports made by medical professionals, one-third of which related to substance use. 1 These numbers have increased dramatically over the past two decades. 1 There are also significant racial inequities in these investigations, with American Indian/Alaskan Native parents’ infants investigated 1.5 times more often than white infants, and Black infants investigated two times more often than white infants. 1
Research has historically focused on adverse consequences of pregnant and parenting people’s drug use to children.2-4 More recently, research has started to examine the effects of policies and healthcare practices adopted in response to pregnant and parenting people’s substance use, and has found that many of these policies and practices not only do not help, but instead relate to increased adverse consequences.5-8 One particular area of focus has been on medical professionals’ reporting to child welfare agencies related to birthing people’s drug use and the racial inequities in such reporting, given recent attention to the adverse consequences for the health and well-being of child welfare reporting and involvement.9-12 Reporting can harm children by preventing maternal presence, which mitigates neonatal stress processes at birth, and by placing children in a foster care system that often does not meet the needs of children in its care.11,12 Adverse health consequences for birthing people who use drugs include increased risk of overdose, pregnant people avoiding prenatal care and treatment out of fear of being reported, and having children removed.8,13-15
Two recent studies have qualitatively examined how physicians make decisions about reporting individual birthing people and infants to child welfare related to substance use.16,17 These studies found that physicians perceived a hospital or state policy as requiring them to report substance use at birth. Even when a hospital policy did not explicitly require reporting, having a hospital policy in place prompted attention to the question of whether a report should be made for patients. 17 This qualitative research found that physicians sometimes disagreed with reporting practices when they perceived the reporting as primarily due to hospital or state policy requirements. 16 However, these physicians also believed that the reporting they did served a health-focused purpose: protecting infants from harm and linking birthing individuals and parents to essential services. 17 These qualitative findings echo findings from a survey of more than 1,300 physicians in the early 2000s that found that physician actions in response to pregnant and birthing people’s substance use were influenced by their perceptions of the state policy environment and the presence of hospital protocols. 18
Despite multiple articles examining state and federal policies related to child welfare reporting requirements 19 and the content of different hospital reporting policies,20,21 the research has not examined the creation and development of hospital policies that relate to child welfare reporting of birthing people who use drugs. Hospital policies are likely influenced by federal and state laws. However, these laws are not prescriptive in terms of mandating use of specific hospital policies, nor do they dictate the exact contents of the policies, which provides hospitals with some flexibility in shaping their policies. Thus, understanding the process of creating and developing hospital policies related to child welfare reporting and birthing people who use drugs is important. There is some research available on factors related to hospital policy creation and implementation in general. 22 Yet, little research has examined the processes through which hospital policies are created, particularly regarding reproductive health topics. One study found that hospital abortion policies are created by those with institutional power and are influenced by personal beliefs and political considerations. 23 Yet, no literature we are aware of has explored how hospital policies relevant to birthing people’s drug use are created.
In this study, we conducted in-depth interviews with health professionals involved in developing hospital policies related to child welfare reporting related to birthing people who use drugs. The goal was to understand health professionals’ experiences creating such policies as well as factors they considered in developing or revising the policies.
Methods
This study conducted in-depth interviews with healthcare providers in decision-making roles at hospitals who were involved in developing or revising hospital policies related to child welfare reporting for birthing people who use drugs. This article adheres to the Consolidated Criteria for Reporting Qualitative Research 24 regarding key data collection and analysis aspects. Semi-structured interviews were used as the primary method of data collection.
Ethics
The protocol for this research was reviewed and approved by the WCG IRB. The analysis of de-identified transcripts does not meet the definition of human subjects’ research and thus did not need additional IRB review by University of California, San Francisco (UCSF).
Sampling and Recruitment
We used a combination of purposive and snowball sampling to identify health professionals who were involved in developing or revising hospital policies related to birthing people who use drugs. Participants were eligible for inclusion if they were at least 18 years old and self-identified as having a role in developing or revising hospital policies related to child welfare reporting during the birth hospitalization. We recruited purposively from the four regions of the U.S. to ensure geographic diversity. We used the term “child welfare” to indicate the state and county-level agencies receiving reports on child maltreatment.
We conducted outreach via email to listservs, professional organizations, and the researchers’ professional networks. The recruitment email described the purpose of the study and requested participation in a 45-minute interview regarding hospital policy related to child welfare and birthing people’s drug use. The first author followed up via email with interested participants and scheduled a mutually agreeable time for a conference or phone call using a scheduling program (Doodle). We focused our interviews on hospital-based healthcare professionals with clinically-focused administrative roles who were involved in the hospital policy development process.
Data Collection Procedure and Analysis
The first author conducted semi-structured interviews from May 2022 through November 2022. The interviewer was not known to any of the participants. The interviewer is a research scientist and has a background as a registered nurse in neonatal intensive care. The other members of the research team have backgrounds in public health, obstetrics, and addiction medicine. Each interview was conducted either via videoconference or audio-conference, depending on participant preferences, and audio-recorded using a separate, digital recording device. All participants provided verbal consent. Interviews ranged from 31 to 55 minutes. Our interview guide was informed by the Theoretical Domains Framework 25 and focused on learning about participants’ experiences developing and revising hospital policies related to child welfare and birthing people’s drug use. It asked participants to walk through their most recent process of developing or revising the policies. The guide was semi-structured in that it allowed participants to take the lead in describing this process, but it also included follow-up questions informed by domains from the implementation science framework. 17 These follow-up questions asked participants to describe who was involved in the policy development or revision process, factors they considered, how decisions were made, areas of consensus and disagreement, how people got information about any relevant legal requirements, and what emotions came up for them in the process.
Interview recordings were transcribed verbatim by online software, verified for accuracy, de-identified, and uploaded to Dedoose qualitative data analysis software for coding and analysis. While the interview guide included questions informed by an implementation science framework, the analysis for this article was primarily inductive, focusing on themes that emerged in the data. We did include some deductive aspects to get at some key questions we had—that is, the role of hospital administrators in policy development, use of research evidence in policy development, and public health or health purposes of policies. We note that all the authors believe that government and hospital policies related to pregnant and birthing people’s substance use should be informed by the best available research evidence and should be evaluated in terms of whether they improve or harm public health outcomes. This belief informed our decision to code deductively for any mentions of the use of research evidence or a public health/healthcare purpose to the policies. One researcher read three transcripts and came up with an initial code list, and then, the other researcher read additional transcripts to verify this code list and added codes to create a comprehensive list. Both researchers subsequently reviewed all transcripts, coded transcripts independently, and began to group codes together into the themes. Emerging themes were discussed, discrepancies were resolved, and two final themes emerged. The researchers then identified subthemes related to each theme. We checked how often different subthemes were mentioned and noted exceptions.
We also note that none of the authors has been directly involved in developing hospital policies, although the first author has clinical experience implementing such policies. The range of professional experiences the research team has, including a lead author new to the topic, forced us to discuss and interrogate implicit assumptions and check whether the interpretations came from the data or previous experiences. We also took other steps to ensure the credibility of our findings, including conducting member checks by sharing our preliminary findings with lawyers, clinicians, and people who have been involved in the child welfare system (who were not participants in the study).
Results
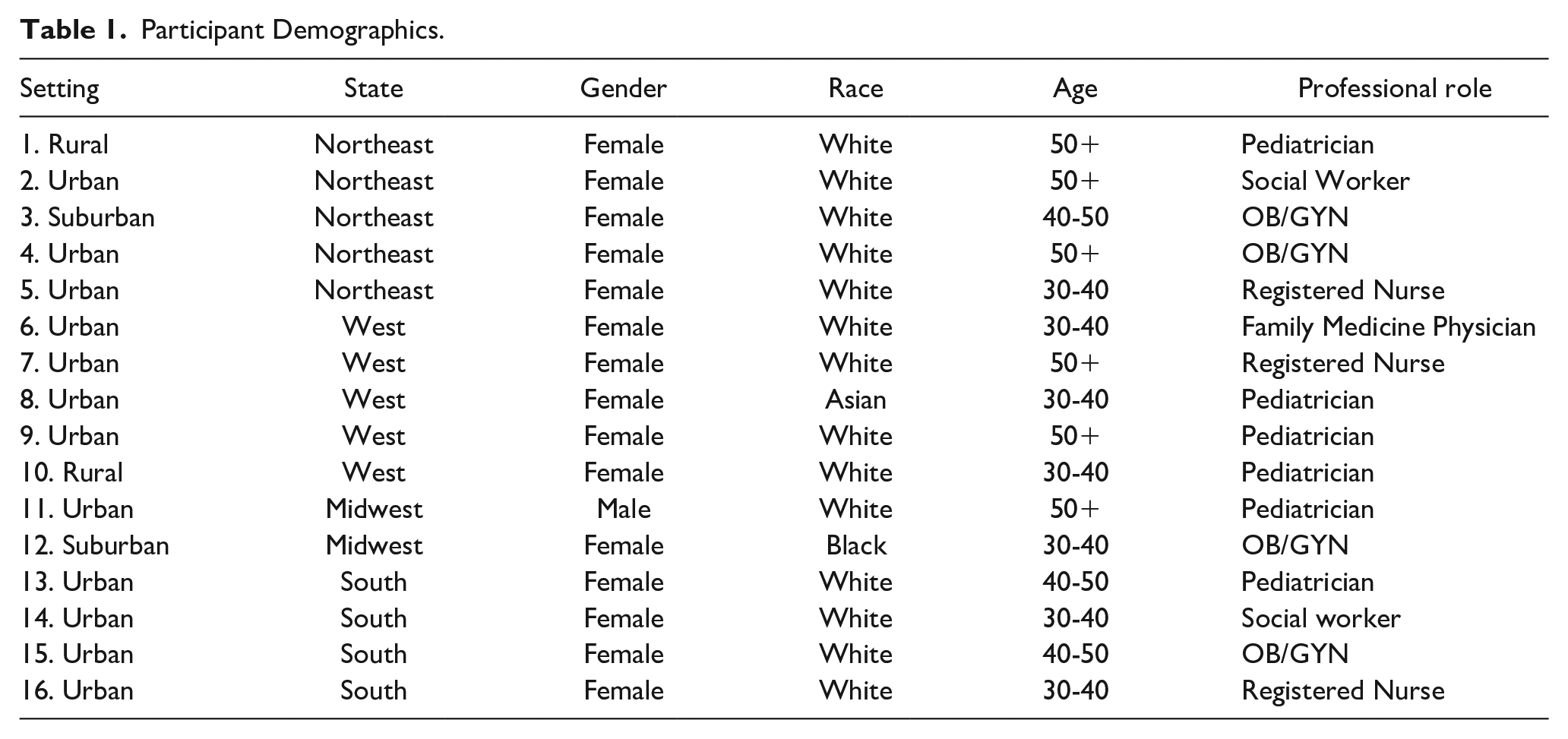
Participants (N = 16) were all health professionals with administrative roles. Two participants were from the same hospital, but from different departments. All four geographic regions of the U.S. were represented. Participants mainly self-identified as White (n = 14, 88%) women (n = 15, 94%). Most participants were physicians (69%), with nurses (19%) and social workers (12%) also represented. Table 1 illustrates participant demographics and professional roles.
Participant Demographics.
Two themes emerged during data analysis. The first was that hospital urine drug testing policies for pregnant and birthing people are seen as part of hospital child welfare reporting policies. The second was that the contents of hospital child welfare reporting policies appear to be a result of hospital politics and attention to legal compliance.
Theme 1: Hospital Urine Drug Testing Policies for Pregnant and Birthing People are Seen as Part of Hospital Child Welfare Reporting Policies
In most interviews, when the interviewer asked participants about their child welfare reporting policies, participants mentioned urine drug testing policies, suggesting that they saw the two policies as connected. Some participants made the connection between urine drug testing and child welfare policies explicit, describing their hospital urine drug testing policies as having the purpose of informing decisions about which patients to report to child welfare during the birthing hospitalization. They described the connection between urine drug testing policies and child welfare reporting as intentional within the policies, rather than merely a side effect of positive urine drug tests used for medical care decisions. Only one participant described a urine drug testing policy as having the purpose of informing medical care decisions for infants. In this single case, the participant described the purpose as ensuring that all infants who might experience neonatal withdrawal syndrome were identified before they left the hospital to effectively treat their withdrawal symptoms with pharmacologic or non-pharmacologic treatment. More typically, participants described their child welfare reporting policies as including criteria for both urine drug testing and descriptions of how the drug test results were relevant for reporting decisions.
Our current [child welfare reporting] policy is. . .more surrounding who to test for alcohol and well, mostly, drug use in our laboring and postpartum patients. And then our social worker does a review of patients that are thought to be high-risk. And then they are usually the ones who report to [child welfare].—Family Medicine Physician, West
Further describing the interconnection of the hospital urine drug testing and hospital reporting policies, a few participants mentioned that if they changed their hospital urine testing policies, this would change which patients they report to child welfare.
So, we decided as a hospital if someone screens on a urine screen for marijuana, that is reported, but if it is someone that is screened verbally and uses and there’s no urine screen done and there’s not felt to be any other concerns that you would file for [child welfare], that those people did not need to be filed on. . .I had them take marijuana off the urine screen for obstetric patients because that way, there’s a whole category of marijuana-exposed newborns that we don’t have to report unless we have another [reason].—OB/GYN, Northeast
Two participants mentioned that their hospitals had urine drug testing policies because the local child welfare agency wants the results. More commonly, though, were participants mentioning that they had their hospital urine testing policies in place to comply with what they saw state child welfare reporting and removal laws as requiring.
Any child that is born substance exposed. . .is a [required] referral to the [child welfare] department. . .We utilize a urine drug screen on mom, a urine drug screen on baby, and an umbilical cord drug screen for confirmatory testing. . .in order to get those results.—Social Worker, South
Theme 2: Hospital Child Welfare Reporting Policy Content is Informed by Hospital Politics and Attention to Legal Compliance
Hospital Politics
While a few participants alluded to the need—in concept—for hospital child welfare policies to be based in evidence, no participant described their hospital policy development process as including reviewing relevant research evidence. Instead, participants described the decisions about what hospital child welfare reporting policy content should include as about satisfying internal and external stakeholders, compromise, and focusing on fairness and justice, that is, political considerations.
Satisfying Stakeholders
One aspect of satisfying internal stakeholders, as described by participants, involved ensuring that personnel feel supported by the institution even when they are not fully comfortable with policies. For example, one participant described a hospital policy revision process focusing on reducing unnecessary child welfare reports, where the participant described one purpose of the policy as having social workers feel more supported by the institution when they do not report. By feeling more supported, this meant having social workers feel as if the institution would back them up if there was a legal case related to them not making a report on a particular infant. In another aspect of satisfying stakeholders, some participants also mentioned collecting feedback on the policy from individuals closer to the patients, aiming to make the patient experience of the policy feel less bad for the patients.
Sometimes [newborn] removal is necessary, sometimes that is what needs to happen and there are certain ways to do that so that people are feeling valued and heard versus blamed or punished.—Pediatrician, West One of our nurse midwives put [the policy] out to in particular a doula group to look over the language and make sure that it would resonate with the patients. Not that the patients would be seeing this policy, but that it would hold their, I don’t know, would be right by them.—Pediatrician, West
These efforts were connected to their focus on social and restorative justice. Most participants also mentioned social justice as a purpose of what they were trying to achieve with their policy. Specifically, they described their policy as focused on reducing actual and perceived bias and increasing equity in terms of child welfare reporting (including urine drug testing). They also described focusing on repairing harm, that is, on restorative justice.
Essentially, they brought in basically restorative justice practices into that. How do you maintain some dignity around the patient that you’re talking about?—Pediatrician, West
Political Compromise
Participants described even more explicit political aspects within the hospital and as well as outside the hospital that influenced the content of the policies. Within the hospital, participants described processes of getting to a consensus on the content of policies that were about political compromise. One participant described the process of defining the specific details of the policy, which, in their case, involved a birthing person needing to have been engaged in treatment and have negative urine drug tests for the 12 weeks before delivery in order to not be reported to child welfare.
How did you come to the 12 week? [I’d like to] understand how that defines stable:
And that was pushback from our hospital administration and the social work colleagues. . ..I think that some of us were pushing for a shorter timeframe of like 30 days, like the same we do for breastfeeding, but we couldn’t get much. 12 weeks is all we could get.—OB/GYN, South
Others described the political compromises they needed to make to get everyone in the hospital on board: So, I do anticipate that there will be some pushback, especially if I move away from urine drug screening in general, because I think that there, that is just sort of been like the tool, it’s like the hammer that everybody uses in this, in this context. And so I’ve been. . .balancing the thought that people really won’t be on board if there isn’t some sort of urine drug screening protocol.—Pediatrician, West If you do have to drug test, can you at least gain consent from the patient?—Registered Nurse, Northeast
Political Power
For others, the hospital politics they described were less about compromises between different groups within the hospital and more about which groups and institutions have power. This involved which groups have power within hospitals (e.g., social workers having less power than physicians). As a social work director explained: So, I was in the discussions of like pro versus con of like why we think this is an initiative that we should put into place, why we think this is important. So I was present for the presentation of the conversation, but I was not present for the voting of that conversation. That was exclusively with hospital administration and the OB providers, and they did leave it up to the OB providers to decide whether they wanted to put that in place. I was basically able, able to present my opinions on the subject. And then had to pass it into their hands at that point.—Social Worker, South
Hospital politics also involves which hospitals in a region have the power and influence to influence policies at other hospitals in the region. For example, two participants mentioned looking to larger, urban hospitals to guide their policy. Another participant mentioned that the smaller, community hospital where she worked did not want to follow the policy of a larger hospital in their region. The politics participants discussed were not only at the hospital level, though.
Legal Compliance
In terms of the purpose participants saw hospital policies as serving, a few participants mentioned that they believed that the policies could prevent harm to an infant or connect a birthing person to services. Yet, no participant described considering or having discussions about whether or how the hospital policy could improve healthcare (e.g., treatment or medication) or infant or maternal health outcomes nor did any participant describe examining relevant research evidence. Much more commonly mentioned were considerations of legal compliance and how to protect the institution, and occasionally individual employees, from legal consequences.
Legal Nuances and Consequences
Most participants described ways that decisions about hospital policies considered and addressed what they viewed as legal nuances such as the legality of the substance or whether a particular aspect of use during pregnancy is criminalized; what precisely needs to be reported (e.g., positive test alone v positive test plus other factors); or whether they perceived the law as requiring or prohibiting urine toxicology or requires consent for urine toxicology.
Participants mentioned multiple specific negative legal consequences of not having a hospital policy or of having a policy not fully in compliance with legal requirements. Particular negative consequences the hospital policy was supposed to help avoid included avoiding state-imposed fines, child welfare agencies communicating back that they did not report someone they should have, the state bringing a legal case against the hospital or individual employees for not reporting, and individual employees losing their license or job. No participant gave an actual example, though, of anyone experiencing such a consequence.
It’s a lot of fear about fines, licensing—OB/GYN, Northeast Their concerns were that. . .that use in the third trimester put the hospital at legal risk if that patient were to relapse or something was to happen to baby and we didn’t make a [child welfare] report.—OB/GYN, South
Legal Guidance, Review, and Approval
In terms of who influenced the final content of hospital policies, participants described the content of the hospital policies as subject to and heavily reliant on guidance, review, and approval from higher-level hospital administrators and external government agencies, primarily child welfare agencies. Some participants mentioned clinical, medical, or social work directors as involved in developing the hospital policies. The roles of these directors involved activities such as starting discussions, helping resolve conflicts getting people aligned on policy content, signing policies into effect, and participating in meetings. Much more common, though, in influencing the final content of the policies was the involvement of higher-level hospital administrators, such as risk management or legal or executive-level administrators. Almost all participants mentioned the involvement of hospital administrators in the development and/or approval of the specific contents of the hospital policies. This involvement included activities such as participating in conversations, providing legal interpretations, obtaining guidance from external agencies, considering financial implications, and reviewing or (more commonly) approving policies.
Participants also mentioned government agencies as involved in developing and revising the contents of the hospital policies. While two participants mentioned the health department as playing a small role in developing the hospital policy, almost all participants mentioned child welfare agency involvement in the development or revision of the hospital policies. This involvement included a child welfare agency representative: serving as a member of the workgroup working on the hospital policy; helping to resolve conflicts between hospital staff as to what the hospital policy should include; and providing guidance on policy content, including information the child welfare agency wants to know about patients who are reported. Providing guidance was the most common way participants mentioned child welfare agencies being involved. They described child welfare agencies as providing this guidance through presentations, one-on-one discussions, official guidance, review and feedback on draft policies, and, in one case, approving the hospital policy.
When we started our program, I called [child welfare]. I said, “What is it you guys want to know?” Because we need a little transparency about this, so we came up with a 32 week. . .plan where we had a list of what our local [child welfare] office wanted to know about people and we would help them and provide that at time of delivery.—OB/GYN, Northeast We also have involvement, we have a relationship with the head of investigations for the state of [x] with [child welfare], so. . .we sort of ran things by her as well.—Registered Nurse, South
In some cases, the child welfare agency’s involvement in the hospital policy guided toward more reporting.
They say they still want to be notified of marijuana.—Pediatrician, Midwest
In other cases, though, the child welfare agency guidance allowed for less reporting, and, as one participant described, was key to having the content of their hospital policy not include people taking medications for opioid use disorder.
We were working directly with the director of investigations at [child welfare] to talk about their guidance, their, how they’re interpreting CAPTA.. . .I think it was finally having it really specifically stated from them that they did not want those reports of people who are on buprenorphine and methadone and stable. I think that really helped turn the corner.—OB/GYN, South
Discussion
This study is the first to examine the processes through which hospital policies regarding child welfare reporting related to birthing people’s drug use are made. We found that the contents of hospital policies appeared to emerge through political compromise across different hospital departments and efforts to ensure legal compliance by involving hospital administrators and representatives from external child welfare agencies in the hospital policy development process.
Previous research has found that some physicians describe child welfare reporting decisions related to birthing people’s drug use as consequential for protecting infants from harm and connecting birthing people to important services, 17 that is, as relevant for public health. Findings from this study suggest, though, that people developing the hospital policies that influence physician behavior are not focusing on public health or medical care considerations as they are developing the policies. There is currently a lack of research that specifically evaluates the healthcare and health impacts of different hospital policies related to child welfare reporting of birthing people who use drugs. Also, no professional association recommends detailed content for hospital policy in this area. Yet, there is professional association guidance and related research that likely would be relevant for informing such hospital policies, for example recommendations regarding clinically appropriate use of urine drug tests, research about the relationship between child welfare reporting and pregnant people’s avoidance of care, and research about relationships between pregnant people’s substance use and subsequent child maltreatment.14,15,26-29 Study participants did not mention reviewing or considering any of this professional association guidance or research evidence or grappling with the lack of research evidence directly about the effects of different hospital policies. This disconnect between what individual providers believe is the consequence of not reporting (i.e., health and healthcare consequences, that infants will be harmed, and birthing people will not be connected to services), and the lack of consideration of research evidence or health outcomes in the policy development process is notable.
While avoiding the legal consequences for the institution and individual providers appeared to be a common motivator for the content of the hospital policies, no participant gave an actual example of someone experiencing such a legal consequence. It is possible that the small sample size made it so we did not identify anyone who had had this experience themselves. It is worth noting, though, that no participant gave a concrete example of anyone they knew or any institution experiencing such a consequence. This contrasts with research about provider decision-making about reporting individual patients, which finds that providers mention specific anecdotes from their own or their colleagues’ experiences about infants experiencing adverse outcomes after leaving the hospital as influencing their decisions. 17 In both instances, though, the focus of the hospital policies and individual practices appears to be on avoiding low-probability/high-hazard events. 29 A more evidence-informed discussion might also incorporate attention to the more commonly occurring events (such as child welfare investigation and family separation) and the effects on health and healthcare of these events for birthing people, infants, and families, for example, how testing and reporting get in the way of pregnant and birthing people getting care.14,15
Participants did acknowledge that hospital drug testing policies were typically focused on identifying birthing people who use drugs to inform child welfare reporting decisions, and not on informing medical treatment decisions for birthing people or infants. This is consistent with recent research that has found that clinical practice rarely differs after a urine drug test and that positive tests often lead to a child welfare report. 30 It is worth noting that the use of urine drug tests to identify substance use disorder, as some of these hospital policies seem to do, conflicts with medical professional society and public health agency recommendations. 31 While some people crafting the hospital policies did believe that there was a legal requirement for drug testing in their state, research suggests that physicians’ perceptions of legal requirements relevant to pregnant and birthing people’s drug use do not necessarily match the actual legal requirements in their state. 18 While often referenced information about state policies regarding urine drug testing32-34 has suggested that this is a requirement in multiple states, reviews of actual legal statutes indicate that fewer states require this testing. 35
Clinicians focusing on legal considerations rather than health-focused considerations about pregnant and birthing people’s substance use is an example of what has been termed blurred professional boundaries, 36 and, more recently, medico-legal hybridity. 37 The involvement of child welfare agencies in developing hospital policies suggests that the blurred professional boundaries are multidirectional. Hospital policies allowing for or even requiring testing based on requests from child welfare agencies for their cases is perhaps the most glaring aspect of these blurred boundaries and raises questions about the exceptions in the Health Insurance Privacy and Portability Act, which allow such information to be so freely shared with child welfare and other government agencies. 38
Limitations
There are several limitations to this study. First, while higher-level administrators (risk management, hospital legal) appear to be involved in developing the hospital policies, no one in these roles agreed to participate. Thus, we do not include their perspectives or understand how they thought about the policies. It is possible that they were considering other factors or focused on purposes different from those described by the mid-level administrators who participated. Similarly, we do not have the perspectives of the people who wrote the state or federal laws or representatives from the child welfare agencies who participated in the policy development process. It is possible and even likely that they were considering different factors than our study participants considered or even reviewed relevant research evidence. We do note, though, that other research has found that to the extent that state legislators who make decisions about policies related to pregnant people’s substance base their decisions on research evidence, they tend to focus on epidemiologic evidence about trends in the use of certain substances and health effects of this substance use during pregnancy, but not on whether the policies they are considering improve outcomes. 39 Similar research on how policymakers decide on child welfare policies and the research evidence they consider would be worthwhile. Second, it is worth acknowledging that, because the people we interviewed were in administrative roles, it is not surprising that they reported focusing on factors related to legal compliance and hospital politics. It is surprising, though, that they did not mention reviewing research evidence or focusing on the health outcomes related to the policies. Third, while participants came from all four U.S. geographic regions, fewer were from the Midwest than other regions, and only two were from rural regions. Third, while the themes were clear and robust in the data and people described a range of experiences in hospital policy creation, the sample was not large. There may be hospital policy development approaches that differ from those we identified. Fourth, research and policy change efforts and media coverage on the topic of urine drug testing and child welfare reporting have proliferated over the past 2 years.17,30,40-44 It is possible that people working on hospital policy changes more recently are having different experiences. Researchers should examine whether hospital policy development processes differ over time.
Conclusion
Hospital policies concerning birthing individuals who use drugs seem to prioritize political and legal considerations more than considerations of patient or public health. A focus on research evidence and focusing on whether practices dictated by the hospital policies meet the clinical needs of patients is needed.
Footnotes
Author Contributions
The authors confirm their contribution to the paper: study conception and design, KA, MT, SCMR; data collection, KA; analysis and interpretation of results, SCMR, KA; and draft manuscript preparation, SCMR, KA, MT. All authors reviewed the results and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Foundation for Opioid Response Efforts.
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board approval was not required.