
Abstract
Background:
Caregiver problematic substance use (SU) is a common adverse childhood experience that is associated with the development of SU disorders in adolescence and poor health outcomes. Most pediatricians do not currently screen for caregiver SU, missing an opportunity to provide targeted prevention counseling to at-risk youth and their families. The objective of this study was to assess whether pediatric residents’ screening-related competencies, beliefs, and training were associated with current screening practices and/or preparedness to screen in the future.
Methods:
Baseline surveys from a quality improvement initiative to increase screening for household SU in pediatric primary care were e-mailed to all pediatric residents at an academic medical center. Surveys assessed residents’ current screening practices, preparedness to screen in the future, screening-related competencies, receipt of SU training, beliefs about screening, perceived caregiver acceptability of screening, and stigma about caregiver SU.
Results:
Residents agreed screening for household SU is a pediatrician’s responsibility and beneficial for patients and families, yet only 5% universally screened. Preparedness to screen in the future was positively associated with reported screening-related competencies and receipt of training on SU screening during residency.
Conclusions:
Most residents did not universally screen for household SU, thereby missing opportunities for targeted secondary prevention of adolescent SU. Trained residents who reported competence in addressing families’ concerns were more likely to feel prepared to screen in the future, suggesting education that addresses caring for affected families, reviews available resources, and improves pediatrician confidence may be particularly impactful.
Highlights
Pediatric trainees feel screening for household substance use (SU) is important and beneficial for patients and families.
However, few trainees universally screen for household SU in practice.
Given the association between receipt of SU screening training and screening behaviors, provider education may be an opportunity to increase family-engaged prevention of adolescent SU.
Investigating barriers to screening is another important next step in promoting a family-focused approach to adolescent SU prevention.
Introduction
In the United States, approximately 1 in 4 children live with a caregiver with a substance use disorder (SUD). 1 This common adverse childhood experience is associated with child depression, anxiety, chronic health conditions, and the development of SUD in adolescence.2-4 The inter-generational transmission of substance use (SU) is multifactorial and moderated by genetic, environmental, and socioeconomic risks.
Addressing caregiver SU may be an important strategy to prevent adolescent SU, a National Institute on Drug Abuse’s 2022-2026 Strategic Plan priority. 5 Pediatricians provide health risk assessments and prevention counseling throughout childhood and have a unique opportunity to identify and support families affected by SU to prevent related consequences. The American Academy of Pediatrics (AAP) recognizes the importance of addressing family SU, encourages universal screening for caregiver SU, and promotes related clinical competencies.2,6
Screening, Brief Intervention, and Referral to Treatment (SBIRT) is an evidence-based way to detect and respond to SU that is recommended by the United States Preventive Services Task Force for adults and the AAP for adolescents.7-9 SBIRT is cost-effective and has been successfully implemented in primary care, mental health, and emergency department settings.10-13 A family-focused approach to SBIRT (F-SBIRT) has the potential to reduce adolescent SU and related consequences. 14 Prior work has shown high caregiver acceptability of screening for caregiver SU, including in families with household SU.15,16 Provider support and treatment resource provision may spur caregiver substance-related behavior change and improve caregiver-provider relationships. 16 However, most pediatricians do not screen.17,18 Stigma and insufficient knowledge are likely barriers to pediatrician efforts to address caregiver SU.19,20
Educational interventions may be one way to improve screening for caregiver SU, yet current pediatric curricula focus on adolescents’, not caregivers’, SU. Pediatrician receipt of SBIRT training is associated with improved provider attitudes, knowledge, and behaviors. 21 Pediatric residency curriculum incorporating role-play and supervised practice is associated with the use of SBIRT and improved confidence addressing adolescent SU. 22 The development of efficacious educational interventions to improve care for caregivers with SU requires understanding learners’ attitudes and improving confidence around caregiver SU screening. 23
This study examined pediatric residents’ screening-related competencies, receipt of SU training, opinions about screening, perceived caregiver acceptability of screening, and stigma about caregiver SU, and whether these were associated with current screening practices and/or preparedness to screen in the future.
Methods
Sample
This study is a cross-sectional analysis of baseline surveys from a quality improvement initiative to increase screening for caregiver SU in pediatric primary care. Anonymous Qualtrics survey links were e-mailed in April 2021, July 2022, and July 2023 to all pediatric residents (n = 200) at an urban academic children’s hospital in a community with a high prevalence of household SU. 24 If residents completed the survey multiple times, the earliest survey was included in analyses. The survey introduction explained the purpose of the survey and definitions for household (“any family members in the home”) and SU (“alcohol, marijuana, and illicit drug use”). Given the focus on household SU, “SU screening” will be used to refer to household screening unless otherwise indicated. A snack or $5 gift card was provided on completion of the survey. The IRB exempted this study as quality improvement.
Outcome Measures
To assess current screening practices, residents were asked “In the past year, how often have you screened for SU in the household in the primary care clinic?” Responses included “every well-child visit,” “most well-child visits,” “occasionally,” “only if specific concerns about SU,” and “never.” Preparedness to screen in the future was assessed by resident agreement (“agree,” “disagree,” and “unsure”) with the statement “I feel prepared to screen for household SU, even if I don’t have access to social work or similar support in my future practice.”
Independent Variables
Independent variables included resident screening-related competencies, receipt of SU training, opinions about screening, perceived caregiver acceptability of screening, and SU-related stigma (Table 2). 20 Residents specified when they received training (medical school or residency), and whether training covered SU general screening, prevention, and/or treatment (dichotomous response). Post-graduate year (PGY) 1 residents in 2022 and 2023 were not asked about residency training as the survey was distributed at the start of their residency. Categorical variables were used to assess competencies (“agree,” “disagree,” and “unsure”). Likert scales (1 = strongly disagree, 10 = strongly agree) were used to assess opinions, perceived caregiver acceptability, and stigma.
Surveys also assessed resident PGY and future career plans.
Analysis
The distribution of current screening practices, screening preparedness, and independent variables were examined using descriptive statistics. Resident preparedness to screen for caregiver SU in the future and screening competencies were dichotomized to “agree” versus “disagree” and “unsure.” Current screening practices were dichotomized to “ever screened” versus “never screened” given the response distribution.
Bivariate analyses (Chi-Square) were used to assess the association of screening practices and preparedness with training, screening competencies, and confounders. Logistic regression models assessed the association of screening practices and preparedness with resident opinions, perceived caregiver acceptability, and stigma. An alpha level of .05 was used for all analyses. All analyses were performed using R 4.1.2.
Results
Resident Descriptive Variables
Residents with variable post-residency career plans completed a total of 161 surveys (response rate 81%) (Table 1). Of these, 33 were completed post-intervention (21%), 7 were completed by the same resident at an earlier time point (4%), and 25 were excluded due to missing outcome data (16%) for an analytic sample of 96 surveys.
Resident Demographics.
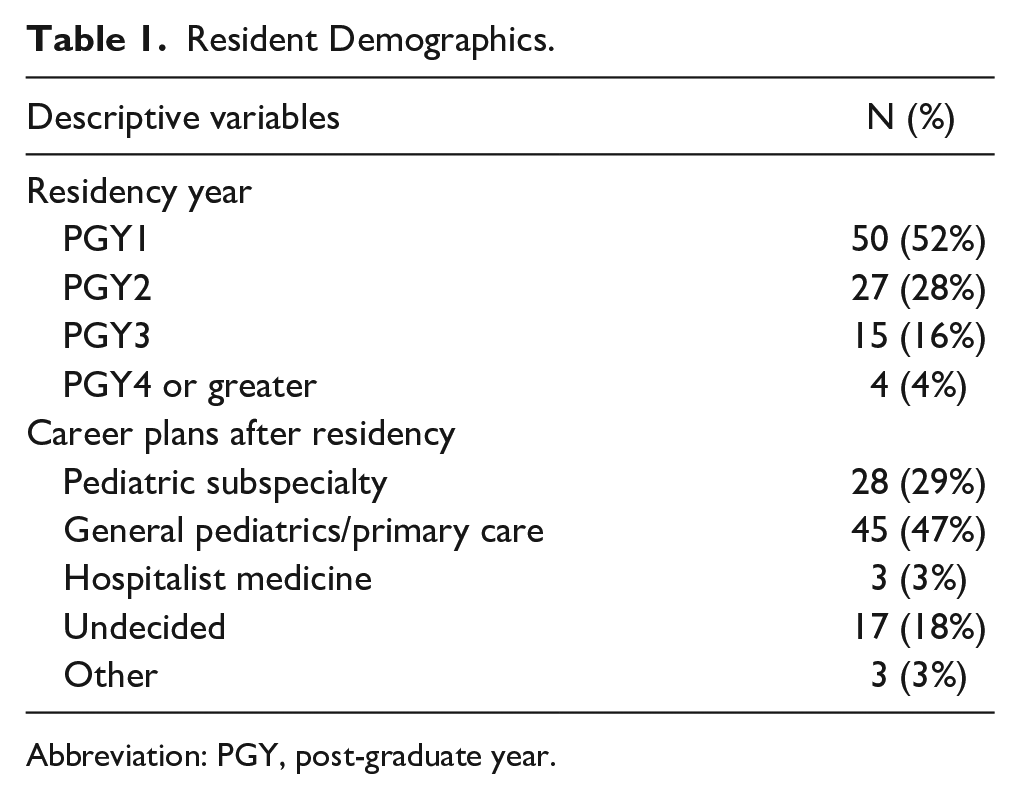
Abbreviation: PGY, post-graduate year.
Screening Practices
Eighty-nine percent of residents reported ever screening for household SU. Few residents screened at every (5%) or most (16%) annual well visits; 41% screened only when specific concerns about SU arose. Only 34% of residents felt prepared to screen for household SU in the future (Table 2).
Resident Screening Practices and Preparedness, Screening Competencies, Receipt of SU Training in Medical School and Residency, and Opinions Regarding Pediatrician Screening, Caregiver Acceptability, and Stigma Around Caregiver SU.
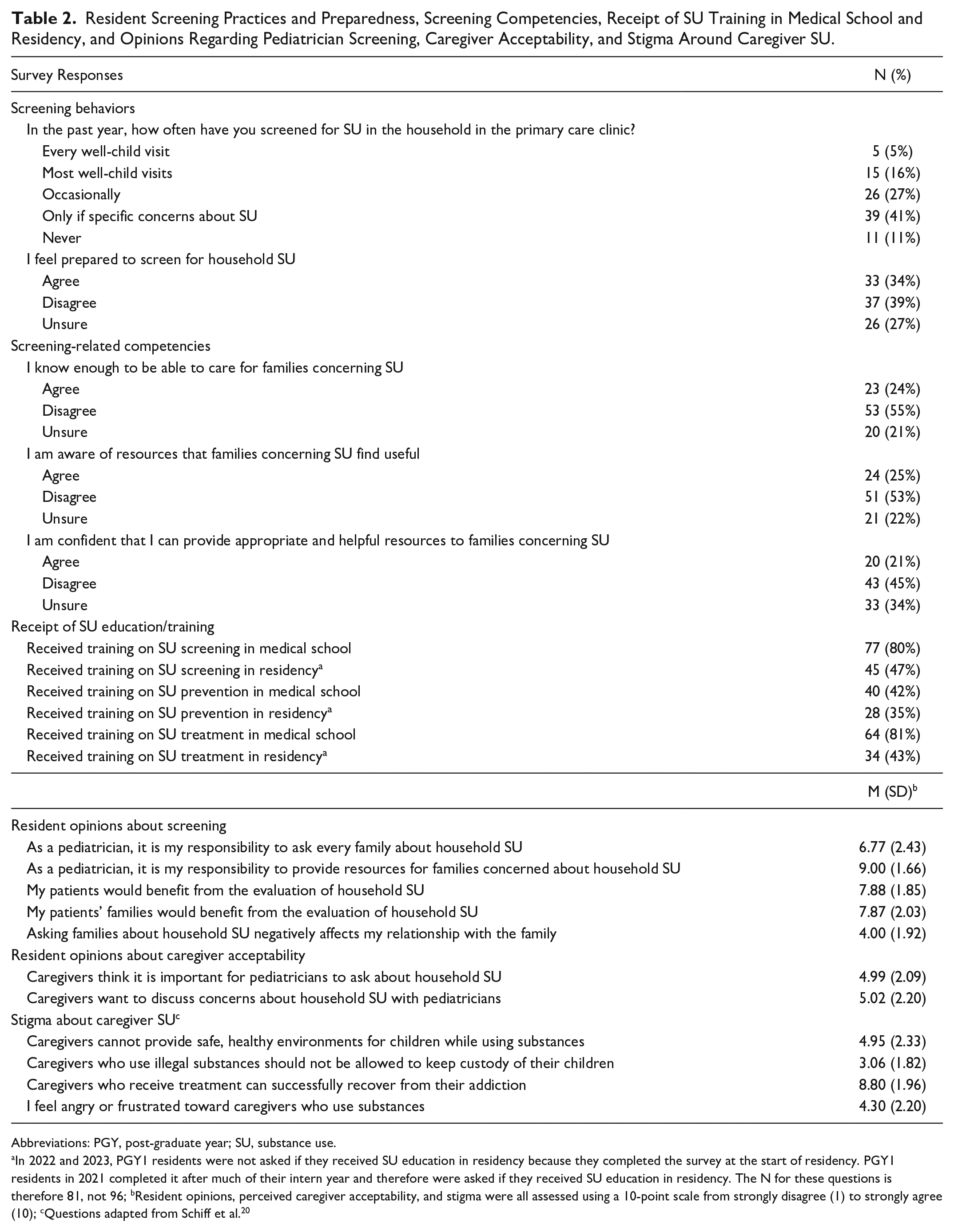
Abbreviations: PGY, post-graduate year; SU, substance use.
In 2022 and 2023, PGY1 residents were not asked if they received SU education in residency because they completed the survey at the start of residency. PGY1 residents in 2021 completed it after much of their intern year and therefore were asked if they received SU education in residency. The N for these questions is therefore 81, not 96; bResident opinions, perceived caregiver acceptability, and stigma were all assessed using a 10-point scale from strongly disagree (1) to strongly agree (10); cQuestions adapted from Schiff et al. 20
Screening Competencies and Opinions
Most residents did not report screening-related competencies, including caring for families with concerning SU (76% disagreed or unsure), awareness of resources (75%), and confidence in providing resources to families (79%) (Table 2). On a 10-point Likert scale (1 = strongly disagree, 10 = strongly agree), residents agreed that screening is a pediatrician’s responsibility (mean [SD] = 6.77 [2.43]) and beneficial for patients (7.88 [1.85]) and families (7.87 [2.03]). Residents were neutral about whether caregivers think SU screening is important (Mean [SD] = 4.99 [2.09]) or want to discuss SU-related concerns with their child’s pediatrician (5.02 [2.20]). Residents disagreed that caregivers with SU should lose custody and agreed caregivers receiving treatment can recover from addiction. They were neutral about feeling frustrated toward caregivers with SU and whether caregivers can provide safe environments for children (Table 2).
Receipt of SU Training
Residents reported receipt of training on SU screening, prevention, and treatment during medical school and residency varied (Table 2). Most residents (80%) received SU screening training during medical school, but only 47% received this training in residency.
Training and Screening Practices
Residents who received training on SU screening in residency were more likely to feel prepared to screen in the future compared to residents who did not receive training (OR 3.06, 95% CI 1.15-8.16) (Figure 1). Receipt of SU screening training during medical school and receipt of SU prevention or treatment training were not associated with screening preparedness.
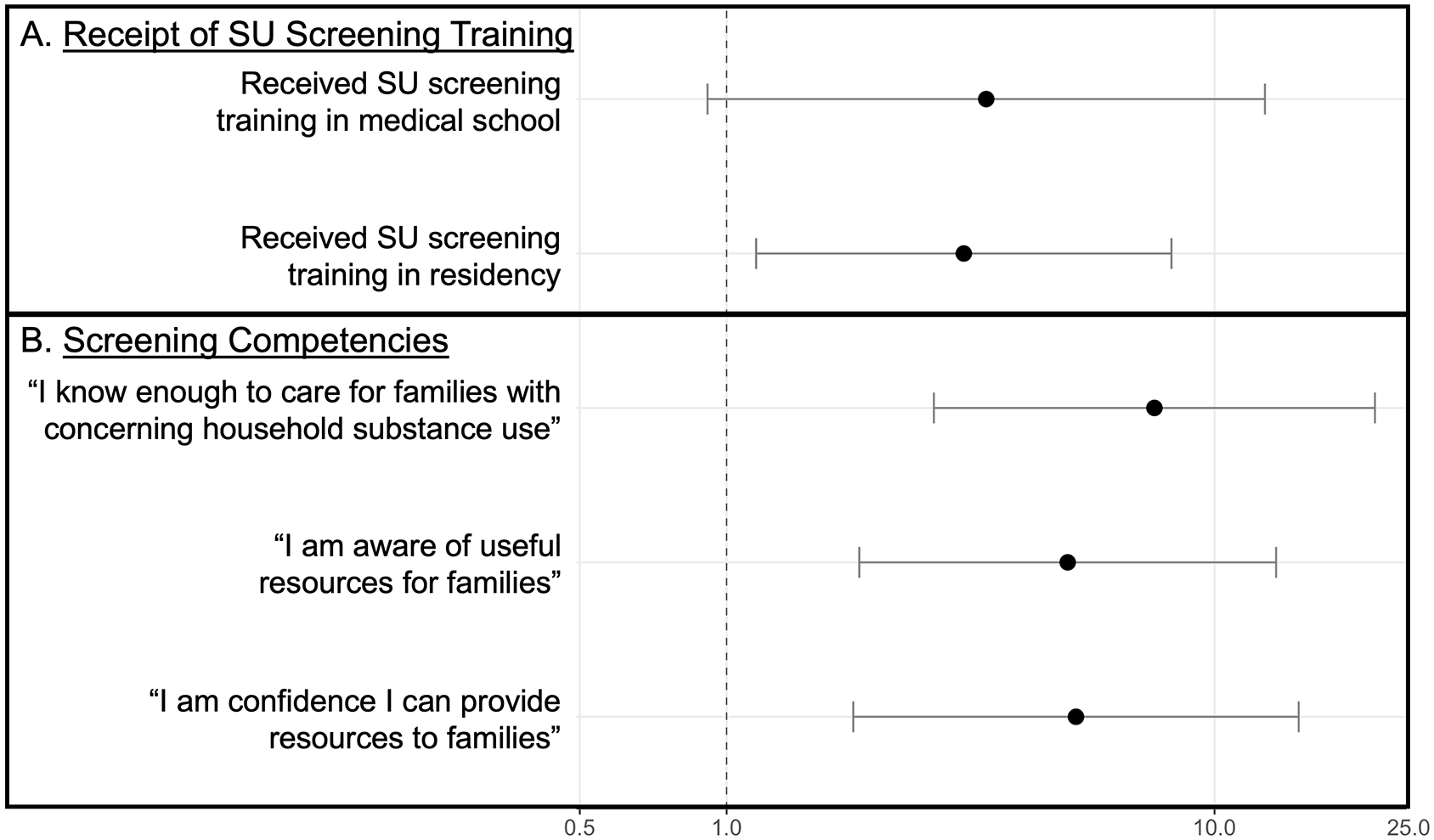
Odds of resident preparedness to screen for household SU by (a) receipt of SU screening training and (b) screening competencies.
Screening Competencies and Practices
Residents who reported sufficient knowledge to care for families (7.53, 2.66-21.32), awareness of resources (5.00, 1.87-13.37), and confidence in providing resources (5.20, 1.82-14.88) were more likely to feel prepared to screen in the future than residents who did not report competencies (Figure 1). There were no significant associations between screening preparedness and opinions about screening, perceived caregiver acceptability of screening, stigma about caregiver SU, residency PGY, or future career plans. Given the small number of residents who reported screening, analyses lacked the power to detect differences in screening behavior by independent variables (analyses not shown).
Discussion
In this study of pediatric residents, 95% reported they do not universally screen for household SU despite most residents agreeing that screening is a pediatrician’s responsibility and benefits patients and families. This adds to the existing literature on screening for intrauterine opioid exposure by suggesting providers are similarly reluctant to screen broadly for household SU exposure throughout childhood. 18 Furthermore, only 34% of residents felt prepared to screen for household SU in the future.
Our findings build upon prior work highlighting structural and policy barriers to addressing SU in primary care, including insufficient time, limited resources, and concerns about when to involve child protective services.25,26 Residents’ concerns about caregiver acceptability of screening may also be a barrier and may perpetuate resident discomfort discussing SU, recovery, and relapse with mothers. 20 Although prior work showed high caregiver acceptability of pediatrician screening, there remains a need to investigate and disseminate caregiver goals for family-centered, non-stigmatizing, and equitable provider response to caregiver SU.
Provider stigma around caregiver SU may also be a barrier to screening. Although associations between screening and stigma did not reach statistical significance in this study, prior work has found stigma negatively impacts patient care. 19 Residents were neutral about caregivers’ ability to provide safe environments for children. This ambivalence, combined with limited guidance on assessing safety in families affected by caregiver SU, may make residents hesitant to screen for concerns they feel poorly prepared to address. Furthermore, residents who hold stigmatizing views of caregiver SU may be more likely to incorporate bias into screening habits, as suggested by our finding that almost half of residents only screened if concerned about potential caregiver SU. However, our analyses did not differentiate between people who universally screened and those who selectively screened, potentially obscuring how stigma affected screening.
Providers who selectively screen miss opportunities for universal primary prevention and potentially perpetuate stigma about which families appear to have substance-related concerns. Failure to universally screen for SU likely contributes to racial and ethnic disparities in receipt of SU counseling and treatment.27,28 Non-universal screening may particularly target Black families and mothers, who are more likely than white women to undergo urine toxicology testing at childbirth, have children placed in foster care, and remain separated from their children.29,30
Tailored education interventions may provide opportunities to address these barriers. Screening preparedness was associated with receipt of residency SU screening training, which is consistent with prior work showing SU-specific training improves providers’ knowledge, attitudes, and self-efficacy in caring for patients with SU.20,31,32 Our results suggest it may be particularly beneficial to emphasize caregiver acceptability of screening and how provider support and linkage to resources may spur caregiver behavior change.15-17
The finding that residency training but not medical school training was associated with screening preparedness suggests training that is more immediately applicable to trainees’ clinical practice may be more efficacious. However, more residents reported receipt of training in medical school than residency, highlighting a need to improve education in both settings.
Limitations of this study include the small sample of residents from a single institution, which limits the power to detect differences in screening behaviors and preparedness by resident opinions, perceived caregiver acceptability, and stigma. The phrasing of certain questions may have implications for results. While “concerning SU” was not defined in the competency questions, this term was specifically used to elicit how trainees would respond to family-defined concerns and to emphasize that pediatricians are not expected to diagnose adult SUDs. Asking whether residents felt prepared to screen in the future without social work support was meant to assess residents’ comfort with screening without external support but may have led residents to underreport preparedness. Lastly, we did not explicitly ask about training on household SU screening. Although this prevents an analysis of how household-focused training may impact screening behaviors, our findings suggest even general screening training may positively influence willingness to screen for household SU.
Conclusions
Our results suggest that SU screening education and screening competencies—specifically knowledge of caring for affected families, awareness of resources, and confidence in providing resources—may empower providers to screen for caregiver SU. These findings have informed the development of a quality improvement and educational initiative to improve household SU screening. Future evaluations of this work will elucidate how this initiative can be improved and expanded to other settings (ie, medical schools) to promote universal household SU screening with the ultimate goals of preventing adolescent SU, decreasing stigma, and supporting families.
Footnotes
Author Contributions
JC contributed to the conceptualization and implementation of this study, completed analyses, and wrote this manuscript. SJC and TM contributed to the implementation of this study. RA and HA contributed to the conceptualization of the study. PAM contributed to the conceptualization and implementation of this study. All authors reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Authors are supported by the National Institutes of Health (K01DA035387, R25DA033211, T32HD052459) and the Health Resources and Services Administration (MCHB LEAH T71MC00009). Sponsors were not involved in (1) the study design, (2) the collection, analysis, and interpretation of data, or (3) the writing of the report.
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board approval was not required.