
Abstract
Background:
Illicitly manufactured fentanyl (IMF) presence has increased reports of buprenorphine precipitated withdrawal and may impact medication for opioid use disorder (MOUD) experiences and preferences.
Methods:
Cross-sectional survey administered by a clinical research coordinator of adults treated by an addiction consult team or bridge clinic who had prior experience with MOUD.
Results:
Among 100 respondents surveyed, 36% identified as female, 11% black, 9% Hispanic, 79% white, 29% had stable housing, 93% used fentanyl, and 65% injected commonly. 51% were currently treated with methadone, 41% were currently treated with sublingual buprenorphine, 12% were currently treated with extended-release buprenorphine, and 1% were currently treated with extended-release naltrexone. Most reported their current MOUD managed withdrawal and cravings well; 83.7% for methadone, 70.4% for sublingual buprenorphine, and 91.7% for extended-release buprenorphine. 75.8% of participants who tried buprenorphine reported ever experiencing precipitated withdrawal. Even so, 43.1% of those not being treated with buprenorphine were willing to start. Two-thirds reported cravings or withdrawal had worsened since IMF and 55% said IMF impacted MOUD decision making; however, 59% did not feel more worried about taking MOUD since IMF. Most (86%) had heard about low-dose buprenorphine initiation, 52.3% of those who had heard of it had tried it, and 57.8% reported positive experiences. 40% had heard of high-dose buprenorphine, 60% of those tried it, and 54.2% had positive experiences. The factors most likely to increase participants’ willingness to start MOUD were immediate access (85%), rapid titration (87%), hearing positive things from friends (82%), and getting MOUD from their doctor (63%).
Conclusions:
Despite IMF impacting withdrawal, cravings, and MOUD decision making, most patients felt MOUD managed symptoms well. Experiences with alternative buprenorphine initiations were positive. Access to low-barrier treatment with immediate medication initiation, aggressive dose escalation, office-based treatment, and peer-based messaging around MOUD may increase treatment uptake.
Highlights
Despite illicitly manufactured fentanyl worsening withdrawal and cravings, most participants currently treated with medication for opioid use disorder (MOUD) reported it managed their cravings and withdrawal well and most did not report feeling more worried about trying MOUD.
Knowledge of low-dose buprenorphine initiation was more common than high-dose buprenorphine initiation; however, most individuals who had tried either approach reported a positive experience.
The most important factors that participants reported would increase their willingness to try MOUD were being able to start quickly, get to an effective dose rapidly, hearing positive things from peers, and being able to get MOUD from a doctor’s office.
Introduction
In 2024, there were 106 469 predicted overdose-related fatalities in the United States, with a majority of deaths involving illicitly manufactured fentanyl (IMF). 1 Overdose mortality has continued to rise despite increasing access to naloxone and medications for opioid use disorder (MOUD). Medications like buprenorphine and methadone are the gold standard for the treatment of opioid use disorder (OUD) and are associated with reduced overdose, decreased mortality, and improved rates of remission.2-8 Despite the evidence supporting MOUD effectiveness, a minority of people with OUD receive medication. A national claims study examining commercially insured and Medicare Advantage members between 2019 and 2017 found that only 12.5% received methadone or buprenorphine and 2.4% received naltrexone. 5 While MOUD treatment rates have improved over time, in 2022 only 25.1% of people with known OUD received medication treatment. 9 The changing street drug supply from predominantly heroin to IMF has also created new challenges when it comes to initiating MOUD.10-12 There have been growing reports of precipitated withdrawal occurring with buprenorphine initiation among people using IMF. One study collecting self-report data from participants entering addiction treatment centers found that the odds of reporting precipitated withdrawal was particularly high when initiating buprenorphine within 24 hours of last fentanyl use. 12 In contrast, some clinical trials have found low rates of precipitated withdrawal when buprenorphine is administered to individuals objectively experiencing mild to moderate withdrawal in medical settings. 13 Higher rates of buprenorphine precipitated opioid withdrawal may be due to the differing pharmacokinetics of fentanyl and its lipophilicity. 14 Regardless of the true incidence of buprenorphine precipitated opioid withdrawal, individuals with OUD may have heard about the potential for precipitated withdrawal from their social networks, which could influence treatment decisions. For example, a study examining online posts found a marked increase in comments about buprenorphine precipitated withdrawal. 15
As reports of buprenorphine precipitated withdrawal in the setting of fentanyl use have increased, an emerging body of literature has examined alternative buprenorphine initiation strategies, including low-dose initiation and high-dose initiation. Low-dose buprenorphine initiation protocols have been reported as case series, retrospective analyses, and reviews.16-19 High-dose buprenorphine initiation is another novel approach to initiating buprenorphine, which has now been studied in clinical trials. 20 To our knowledge, no studies have explicitly examined the impact of IMF on patient decision making practices around MOUD and patient knowledge of alternative buprenorphine initiation strategies.
The goal of this study was to examine how IMF has impacted patients’ experiences with MOUD, MOUD preferences, and knowledge and experience with novel MOUD induction methods.
Methods
This was a cross-sectional survey of adult patients with OUD at an urban academic medical center in Boston, Massachusetts, who had previous experience with prescribed or nonprescribed buprenorphine or methadone. Participants were either hospitalized and currently being cared for by an inpatient addiction consult team or were current outpatients of a low-barrier, outpatient bridge clinic. Participants were first informed about the study by their clinician. Interested participants were then approached by a clinical research coordinator (manuscript author, S.C.), who obtained verbal consent.
The survey instrument was developed by the study authors based on literature review and clinical expertise. This survey was pretested with 2 staff members and then subsequently with 3 patients with OUD, in order to ensure the acceptability and reproducibility of the instrument. The survey instrument assessed where participants received their information related to MOUD. Participants were asked about their past experiences with MOUD, including assessing how well it managed their craving and withdrawal and whether they ever experienced precipitated withdrawal. Participants who reported not currently being treated with MOUD were then asked about their willingness to start MOUD. Those who were very or somewhat unwilling were asked about why they were unwilling. Those who reported currently being treated with MOUD were asked about how well their current MOUD managed their withdrawal and cravings. All participants were asked about whether they had previously heard of low-dose and high-dose buprenorphine initiations, whether they had personally tried those approaches, and what their experience had been. Participants were asked about what factors influenced their decision making about choosing MOUD and how the presence of IMF has impacted their decision making around MOUD. We present descriptive statistics on the participant responses to survey items.
Data were analyzed on 10 June, 2024. This study was approved by the Mass General Brigham IRB.
Results
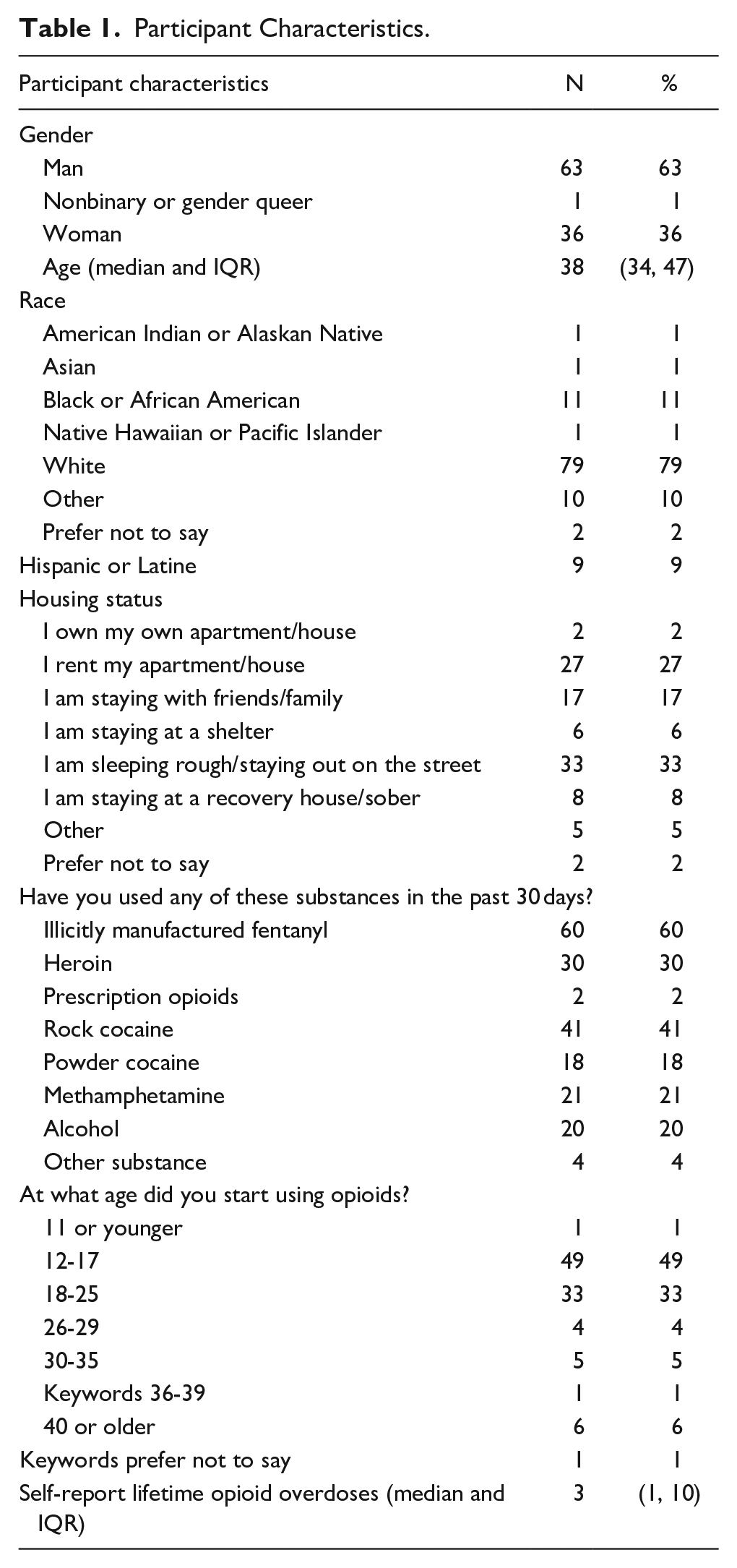
There were 100 respondents who completed the survey. The median age of the sample was 38: 36% identified as female, 63% as male, and 1% as nonbinary. Among those surveyed, 11% identified as black, 9% Hispanic, 10% other race, and 79% white (Table 1). Only 2% owned their own apartment or home, 27% rented, and the remainder did not have stable housing of their own. Most participants had used fentanyl (93%) and almost as many had used heroin (92%). Fewer (70%) had used prescription opioids. Stimulant use was common with 78% having ever used rock cocaine, 69% having ever used power cocaine, and 50% having ever used methamphetamine. Injecting was the most frequent means of use for fentanyl, with 64.5% identifying injecting as their most common route of use. Among the sample, half started using opioids before the age of 18 and the median number of lifetime overdoses in the sample was 3.
Participant Characteristics.
Nearly all participants (99%) had tried sublingual buprenorphine, and most (82%) had tried methadone. Only 38% had tried extended-release buprenorphine, and 21% had tried extended-release naltrexone. At the time of the survey, 51% were currently being treated with methadone, 41% were currently being treated with sublingual buprenorphine, 12% were currently being treated with extended-release buprenorphine, and 1% were currently being treated with extended-release naltrexone. Two people reported being currently treated with methadone and sublingual buprenorphine. All people that reported currently being treated with extended-release buprenorphine also reported being currently treated with sublingual buprenorphine.
For those currently being treated with methadone, 83.7% felt it was managing their withdrawal and cravings well or very well. For sublingual buprenorphine treated participants, 70.4% felt it was managing their cravings and withdrawal well or very well. For extended-release buprenorphine, 91.7% reported it managed their cravings and withdrawal well or very well (Figure 1). There was only 1 participant who was currently being treated with extended-release naltrexone who responded to this question, and they reported it managed their symptoms very well. Among those who reported their current medication was not managing their craving and withdrawal symptoms, they were asked why. Of those who answered in the methadone-treated group, the most common response was that the dose was inadequate, reported by 25%. For buprenorphine, no one said the dose was inadequate. For patients who had tried methadone treatment, 36.6% reported that they had stopped methadone treatment because it took too long to get to a dose that managed their cravings and withdrawal.
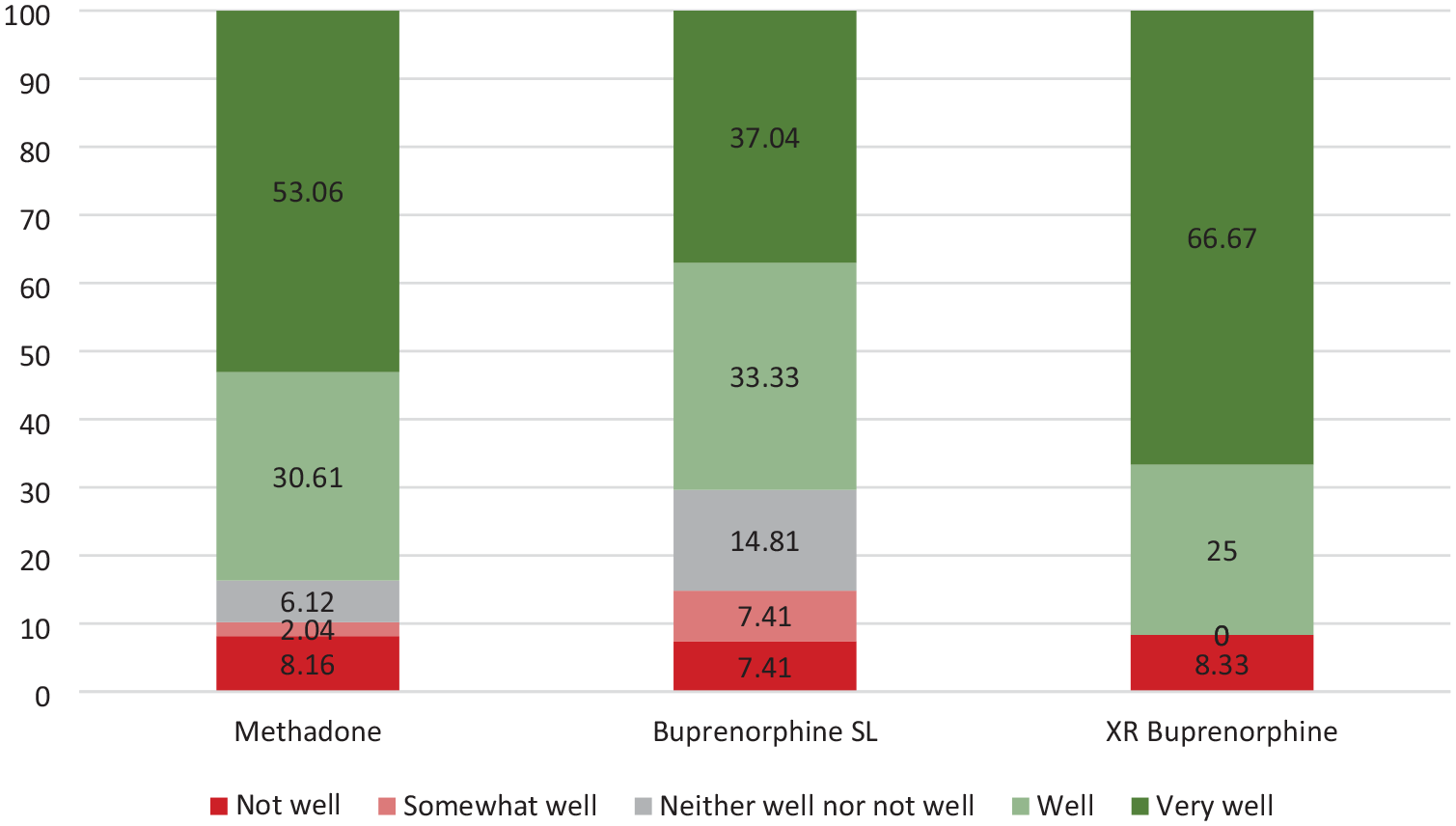
How well MOUD managed withdrawal/cravings among those currently being treated with MOUD.
Among participants who ever tried buprenorphine, 75.8% reported ever experiencing precipitated withdrawal because of the medication. Among participants who ever tried extended-release buprenorphine, 10.5% reported ever experiencing precipitated withdrawal because of the medication. Among participants who ever tried extended-release naltrexone, 23.8% reported ever experiencing precipitated withdrawal because of the medication.
Among participants who ever tried methadone, 59.8% reported ever needing to use other opioids on top of methadone to manage cravings or withdrawal. In contrast, among participants who had ever tried buprenorphine only 32.3% reported ever needing to use additional opioids and only 23.7% of those treated with extended-release buprenorphine, and 19.1% of those treated with extended-release naltrexone ever needed to use additional opioids. Among those who had never tried methadone, 22.2% of participants reported being somewhat or very willing to start taking methadone. Among participants who had previously taken methadone but were not currently being treated with it, 25.8% reported being somewhat or very willing to start taking methadone. For sublingual buprenorphine, 43.1% who had previously tried it were willing to start taking it (Figure 2). Only 1 participant had never tried sublingual buprenorphine and that person was not willing to start taking it. Among participants who had never tried extended-release buprenorphine, 37.1% were willing to start it and among those who had previously tried it, 69.2% were willing to start taking it again. For extended-release naltrexone, 15.2% of those who had never tried it were willing to start and 35% of those who had previously tried it were willing to start taking it.
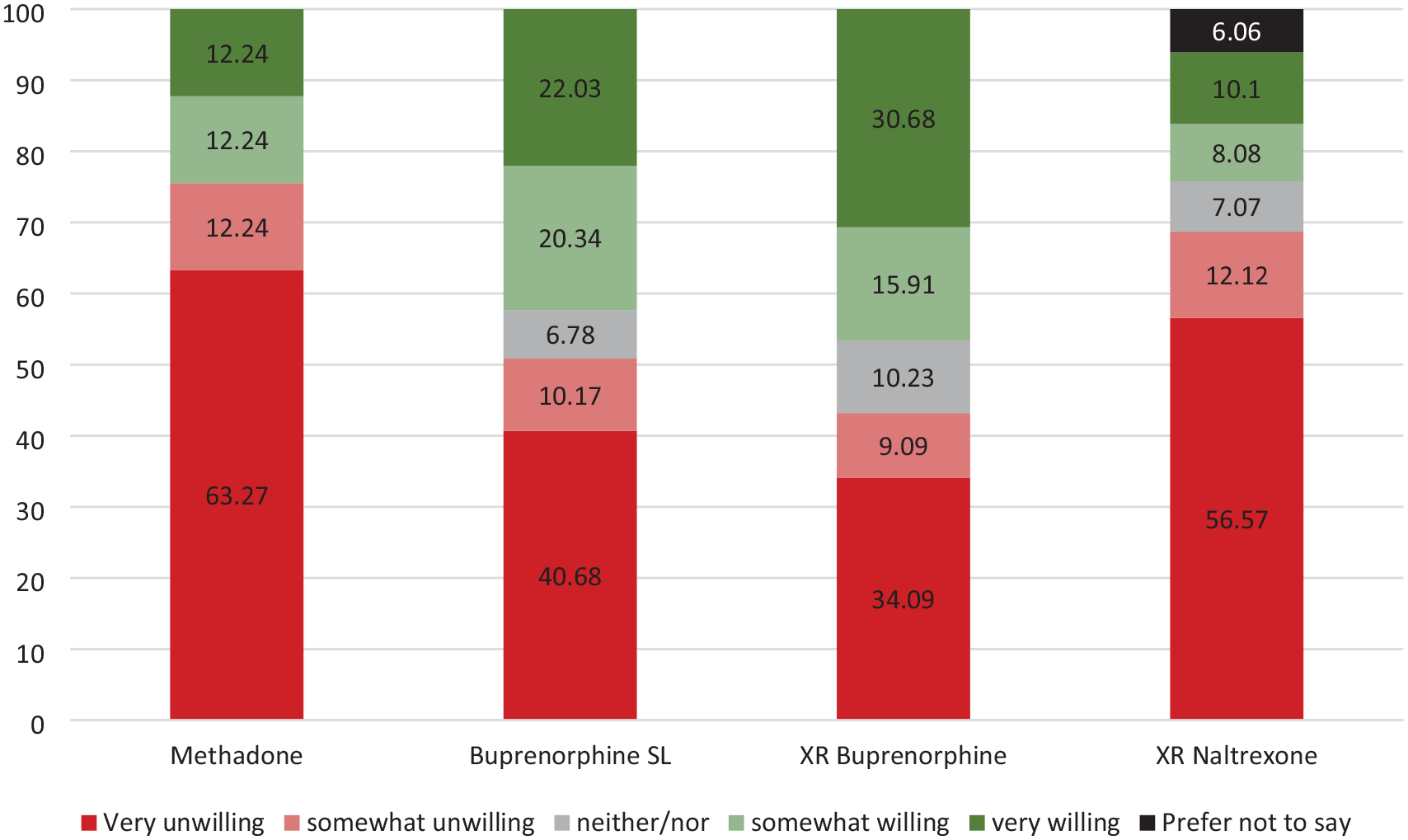
Willingness to try MOUD among those who had previously tried it.
When asked about the impact of IMF on symptoms and decision making, 66% agreed or strongly agreed with the statement that “since starting to use IMF, my cravings and/or withdrawal have been greater or more intense.” When asked about buprenorphine, 53.5% reported that since using IMF they had the experience of trying buprenorphine and having to stop it because it made them feel like they were in worse withdrawal.
Most (86%) participants had heard about low-dose buprenorphine initiation, and 46.5% of them had heard about it from their health care team and 38.4% heard about it from family or friends. About half (52.3%) of those who had heard about low-dose buprenorphine initiation had personally tried it and 57.8% reported their experience with low-dose initiation was somewhat or very positive. Only 20% reported a somewhat or very negative experience with low-dose buprenorphine initiation. Fewer participants had heard of high-dose buprenorphine initiation, with only 40% reporting knowledge about it. Half (55%) heard about it from their health care team, and 25% from family or friends. 60% of those aware of high-dose buprenorphine start had tried it with 54.2% reporting somewhat or very positive experiences with it and 33.3% reporting somewhat or very negative experiences with it.
Participants were asked about factors they considered when choosing a type of MOUD and whether different factors made it more likely, less likely, or had no impact on whether they would start MOUD. Overall, 85% reported being able to start medication quickly would make them more likely to choose MOUD, 87% reported that getting to an effective dose of medication quickly would make them more likely to choose MOUD, and 63% reported being able to get medication prescribed at their doctor’s office would make them more likely to choose MOUD (Figure 3). In contrast, 53% of participants said that having to get medication from an opioid treatment program (OTP) would make them less likely to choose MOUD. Hearing about MOUD from acquaintances was an important factor with 82% reporting they would be more likely to choose a type of MOUD that they heard positive things about from someone they knew. Feeling judged because of MOUD made 41% of respondents less likely to choose a medication. Having to travel a long way to get MOUD was an important factor for nearly 3 quarters of respondents, with 73% reporting it would make them less likely to choose MOUD. Being required to go to counseling or groups was another factor that 60% reported would make them less likely to choose MOUD. There were differences in the importance of factors related to MOUD decision making depending on what type of MOUD participants were currently being treated with. Those treated with buprenorphine reported that getting medication from their doctor’s office was a more important factor, with 70.4% saying it would make them more likely to start MOUD than 59.2% among those treated currently with methadone. Similarly, among participants being treated with buprenorphine 70.4% said having to go to an OTP would make them less likely to start MOUD, whereas only 38.8% of those currently treated with methadone reported the same. Hearing positive things about MOUD was important for all individuals, but this was especially true for extended-release buprenorphine and sublingual buprenorphine with 91.7% and 85.2% saying it would make them more likely to start MOUD than 75.5% for those treated with methadone. A majority of participants (62%) reported that their most important source for information related to MOUD was their health care team.
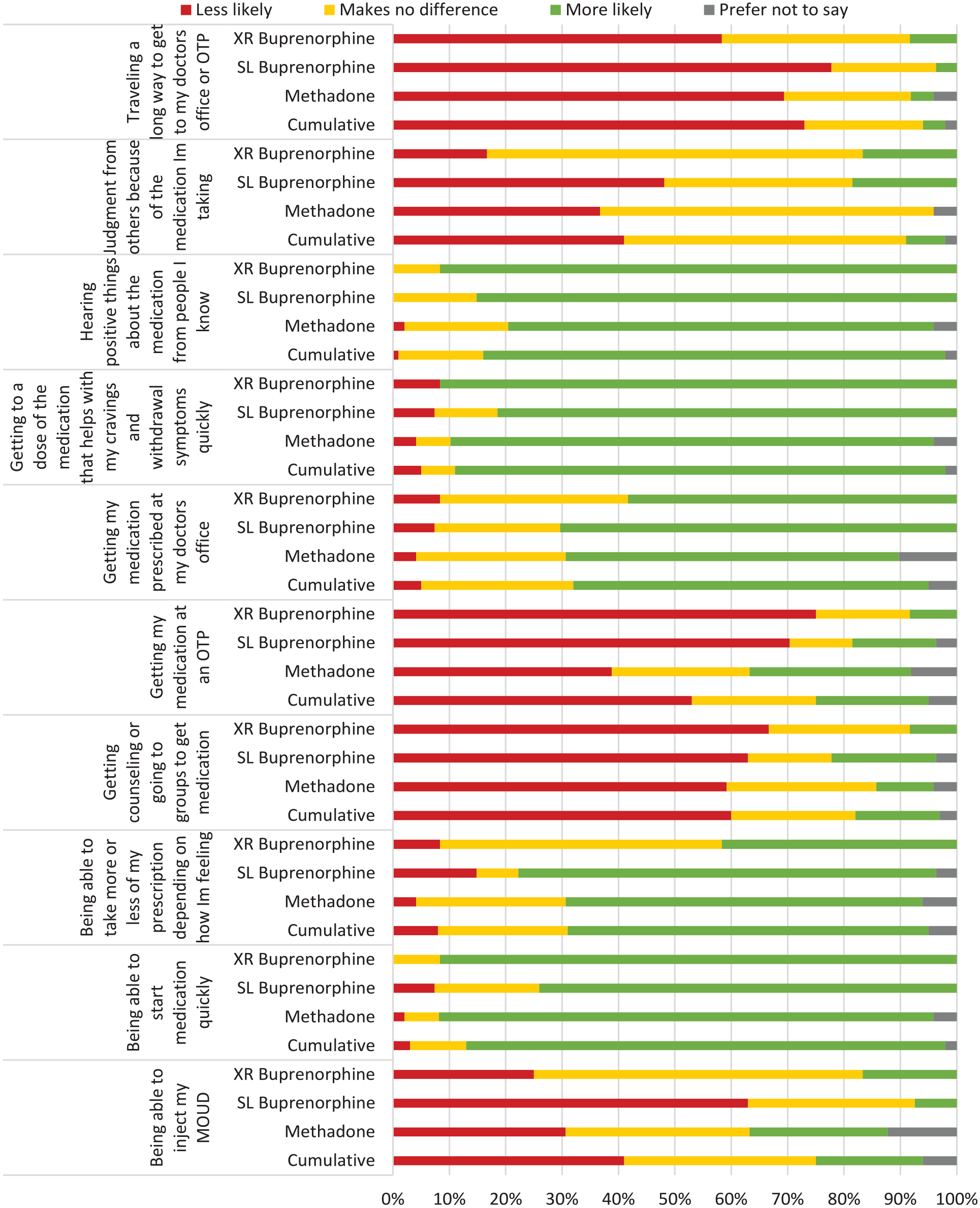
Factors impacting the likelihood of starting MOUD stratified by current type of MOUD treatment and cumulative among all participants.
For methadone, only 18% agreed or strongly agreed that they are less comfortable taking methadone now that IMF is around. For buprenorphine, only 27% agreed or strongly agreed that they were less comfortable taking buprenorphine now that IMF is around. Overall, 55% reported that IMF has impacted their decision making process around MOUD; however, 59% disagreed or strongly disagreed with the statement “because of IMF, I am more worried about taking MOUD.”
Discussion
In this study of patients with OUD being cared for by an addiction consult team or hospital-based bridge clinic who had tried MOUD in the past, 66% reported that their cravings and withdrawal symptoms were more intense since IMF came to dominate the drug supply and 55% reported that the presence of IMF had impacted their decision making around MOUD initiation. Despite these impacts, 59% did not feel more worried about trying MOUD since IMF. More participants had heard of low-dose initiation than high-dose initiation buprenorphine, and fewer participants had negative experiences with low-dose than high-dose initiation. Importantly, most participants who had tried both low- and high-dose initiation approaches for buprenorphine reported positive experiences with it. Although ever experiencing buprenorphine precipitated withdrawal was common in this study, participants were still largely willing to try buprenorphine treatment. For example, among those not currently being treated with buprenorphine who had tried it in the past, 43.1% more willing to try it again. This was notably higher than the percentage of participants not currently being treated with methadone who had tried it in the past who were willing to try methadone again (24.5%).
Most participants felt their current MOUD managed their symptoms well even in the era of IMF, which is an important testament to the efficacy of MOUD for fentanyl use disorder treatment. Participants treated with extended-release buprenorphine reported the best symptom management, with 91.7% of participants currently treated with it reporting it managed their cravings and withdrawal well or very well. Interestingly, all participants who were currently being treated with extended-release buprenorphine reported also being treated with sublingual buprenorphine, which may that utilizing supplemental sublingual buprenorphine is common in real-world settings. Two participants reported being currently treated with both methadone and sublingual buprenorphine, which likely represents patients undergoing a low-dose buprenorphine initiation.
Participants reported unique challenges with methadone and buprenorphine. More participants (59.8%) who had ever been treated with methadone reported needing to use other opioids on top of methadone to manage cravings or withdrawal, which may be related to the long time it takes to get to a therapeutic dose. In contrast, among participants who had ever tried buprenorphine only 32.3% reported ever needing to use additional opioids with sublingual and 23.7% with extended-release buprenorphine.
There were a range of factors that participants identified as important in decisions related to choosing a type of MOUD. Being able to start medication without delay, getting it from a doctor’s office, getting to an effective dose quickly, not being required to engage in counseling, and not having to go to an OTP were all rated as important elements in making treatment decisions. These findings emphasize the need for low-threshold treatment models, which makes MOUD immediately available and offer treatment initiation without barrier. This also highlights the need for changes to methadone regulation, where the current practice in the United States of limiting methadone to OTPs may make care unappealing and inaccessible to some. Amidst the fatal overdose crisis, adaptations to increase uptake of MOUD are urgently needed. These findings differ from a 2013 study of MOUD preferences, which found that participant choice of buprenorphine or methadone was driven by perceived differences in the pharmacology and health effects of the medication and not as much by structural differences in how treatment is delivered. 21 Our findings, however, echo some themes identified in a 2016 qualitative study of patients’ MOUD preferences where daily dosing and the structure of OTPs were highlighted as factors that turned some patients’ away from methadone treatment. 22
Participants also highlighted the value they placed on hearing from people they know about MOUD and the barrier of feeling judged as relevant aspects of their decision making around choosing MOUD. This builds on past research, which found that seeing friends or family have positive experiences with buprenorphine was one important factor in MOUD preferences. 21 This finding aligns with research on vaccine hesitancy, HIV treatment, and HIV preexposure prophylaxis, which has demonstrated the importance of trusted peers in overcoming hesitation about health-related interventions.23-25 This suggests there may be a powerful role for people who have themselves experienced treatment with MOUD to serve as trusted ambassadors to address medication hesitancy for OUD. Public health campaigns could also be helpful in amplifying positive messages about MOUD and addressing stigma to counter the feelings of judgment related to treatment, which hinder MOUD uptake. Ensuring people have accurate information about the availability of MOUD and the different medication options could help counter knowledge gaps, which have been identified in past research as barriers to MOUD selection.22,26,27
Limitations
This study was completed at an urban academic medical center with a robust addiction consult team and bridge clinic and may not be generalizable to other settings. The sample size of 100 participants may also limit generalizability. We did not survey participants who had never tried MOUD or who were not connected to care, and outcomes may be different in that population. In addition, this study was conducted in a state with universal health insurance coverage and reasonably good access to MOUD. Participants in this study may have had different experiences than individuals in states with less access to MOUD. Few participants in this sample were treated with extended-release naltrexone, making it difficult to draw conclusions on this treatment.
Conclusion
Despite IMF making withdrawal symptoms and cravings more severe, most participants were not more worried to try MOUD since IMF and felt both methadone and buprenorphine managed their symptoms well. Access to low-barrier treatment with immediate medication initiation, aggressive dose escalation, office-based treatment, no counseling requirements, and peer-based messaging around MOUD may increase treatment uptake.
Supplemental Material
sj-pdf-1-saj-10.1177_29767342251326339 – Supplemental material for Medications for Opioid Use Disorder: Patients’ Experience, Knowledge, and Preferences in the Era of Illicitly Manufactured Fentanyl
Supplemental material, sj-pdf-1-saj-10.1177_29767342251326339 for Medications for Opioid Use Disorder: Patients’ Experience, Knowledge, and Preferences in the Era of Illicitly Manufactured Fentanyl by Sarah Casey, Sydney Mcgovern, Susan Regan and Sarah E. Wakeman in Substance Use & Addiction Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Wakeman receives royalties for serving as an editor for textbooks by Wolter-Kluwer and Springer and as an article author for UpToDate and receives current grant support from NIDA and HRSA.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board approval was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.