
Abstract
Individuals with substance use disorders (SUD) often encounter challenges in healthcare, including provider attitudes, stigma, and gaps in clinical education. For pregnant and birthing individuals with SUD, these challenges are further compounded by moral blame, judgment, clinician burnout, and limited institutional support. Each of the aforementioned factors are barrier to evidence-based, person-centered care, and contributes to adverse outcomes for both birthing individuals and newborns. This study aims to address those barriers by designing and implementing a stigma-reduction and clinical empathy training package tailored for the intrapartum healthcare workforce. Focusing on the in-patient labor and delivery period, the intervention aims to foster institutional change, grow clinician confidence, and promote a culture of empathy and understanding. The proposed intervention, Interprofessional Simulation Program for Clinical Resilience and Empathy (INPSIRE), will include multi-component training modules and an adaptive intervention designed to address provider clinical knowledge, stigma, and burnout among clinicians and will promote the use of practical tools for demonstrating clinical empathy and support. In developing the intervention, the study will examine quality and stigma in intrapartum care from clinician and patient perspectives through focus group discussions, key informant interviews, restorative justice story circles, and postpartum patient interviews. Drawing insights from these qualitative methods, the INSPIRE intervention will then be co-designed with stakeholders to ensure relevance and effectiveness. The impact of the INSPIRE intervention will be evaluated using a quasi-experimental design, assessing its effects on healthcare team outcomes, patient outcomes, and scalability. Through self-directed online learning and in-person team simulation, the INSPIRE intervention aims to enhance provider skills, promote respectful care, and ultimately improve maternal health outcomes for individuals with SUD.
Highlights
Deep qualitative work will inform the intervention development
Human-centered participatory design will engage the target audience in co-creating the intervention
Testing of the intervention will occur across a large cadre of healthcare team members and will allow us to examine changes at the individual and unit levels.
Introduction
The intersection of substance use disorder (SUD) and pregnancy presents a complex and often overlooked challenge within the realm of maternal health. Pregnant individuals with SUD have a higher risk of experiencing maternal morbidity and mortality than pregnant people without SUD. This risk can be particularly high for individuals living in rural areas, and those with limited access to care.1,2 Many factors contribute to the increased morbidity and mortality among pregnant individuals with SUD, including the pervasive bias and stigma pregnant people with SUD face within the healthcare system.3,4 Bias can manifest through both conscious and unconscious actions, based on preconceived notions, beliefs, or stereotypes, often resulting in unequal treatment. Stigma, characterized by a cognitive division of “us” versus “them,” manifests through labeling, stereotyping, and separation. 5 When pregnant and birthing individuals with SUD experience bias and stigma from their healthcare providers, it can erode their trust in the healthcare system and contribute to poor outcomes for both the birthing individual and their newborn.6–9 Stigmatizing language and discriminatory treatment can contribute to decreased engagement in postpartum care and suboptimal adherence to recommended treatments.10,11
Provider burnout, a prevalent issue among healthcare professionals caring for vulnerable populations, amplifies the negative impact of bias on the quality of care provided.7,8 Burnout, characterized by emotional exhaustion, depersonalization, and reduced personal accomplishment, can impair a provider’s ability to empathize with, and effectively support, pregnant individuals with SUD. This can lead to disengagement, rushed care, or even a tendency to rely on stereotypes when making clinical decisions. As a result, the care provided to this population may be compromised, further contributing to poorer health outcomes for both the birthing individual and newborn. Addressing these systemic challenges is imperative to improving clinical outcomes and mitigating the burden of maternal morbidity and mortality.
Recognizing the urgent need for intervention, efforts must be directed toward developing provider-focused strategies to mitigate stigma and enhance the delivery of respectful, person-centered maternity care for individuals with SUD. Existing approaches have yielded promising results, emphasizing the need for comprehensive, multi-level solutions.12–15 These include interventions aimed at fostering individual empathy and motivation, 16 promoting resiliency and mindfulness, 17 refining clinical skills, 18 transforming team culture, 19 and implementing adaptive learning strategies tailored to meet the diverse needs of healthcare providers.
Research indicates that enhancing clinical empathy skills among healthcare providers can effectively reduce bias and stigma toward marginalized populations, including individuals with SUD, while also mitigating provider burnout and promoting respectful maternity care.20,21 Despite this evidence, there remains a notable gap in evidence-based interventions targeting the enhancement of clinical empathy, specifically during the intrapartum period.
This paper presents the protocol for the development and evaluation of the Interprofessional Simulation Program for clinical Resilience and Empathy (INPSIRE), a multi-component training intervention for intrapartum healthcare teams that aims to enhance provider skills, promote respectful care, and ultimately improve maternal health outcomes for individuals with SUD. The INSPIRE project is one of two research projects nested within the ELEVATE Maternal Health Center of Excellence at the University of Utah (U54HD113169, PI Metz, 2023-2030). For a conceptual model describing the relationship between structural, institutional, and interpersonal actionable modifiers of maternal morbidity and mortality, as well as the activities of the ELEVATE Center (including INSPIRE), and expected outcomes, see the ELEVATE Center Commentary. 22
Methods
Overview
In response to the critical gap in interventions to support intrapartum providers who care for patients with SUD, the INSPIRE study seeks to develop a comprehensive bias-reduction and clinical empathy training package for the intrapartum healthcare workforce. We have chosen the intrapartum period for the focus of the intervention for a number of reasons: (1) the period of time from admission to discharge represents the longest encounter with most healthcare providers during a person’s pregnancy; (2) the peri-delivery episode has been associated with high levels of provider bias and discrimination, 23 and (3) birth is a transformational time and quality affirming care during this time has the potential to affect patient self-efficacy in the future. 24 By fostering institutional change, supporting providers in knowledge and skill acquisition, and promoting a culture of empathy and understanding, this research project aims to improve clinical outcomes and promote equitable care for pregnant individuals with SUD while also supporting healthcare providers’ emotional well-being and resilience.
Our team will develop and evaluate a multi-component training package to promote clinical empathy for patients with SUD called INSPIRE (Figure 1). INSPIRE is anchored in a team simulation curriculum to reduce SUD stigma improve healthcare team functioning and communication, and support resilience to burnout. Providers will have access to interactive web-based learning materials before and after the in-person simulation to bolster knowledge, skills, and motivation. INSPIRE will be tested in a rigorous trial powered to measure both provider and patient outcomes.
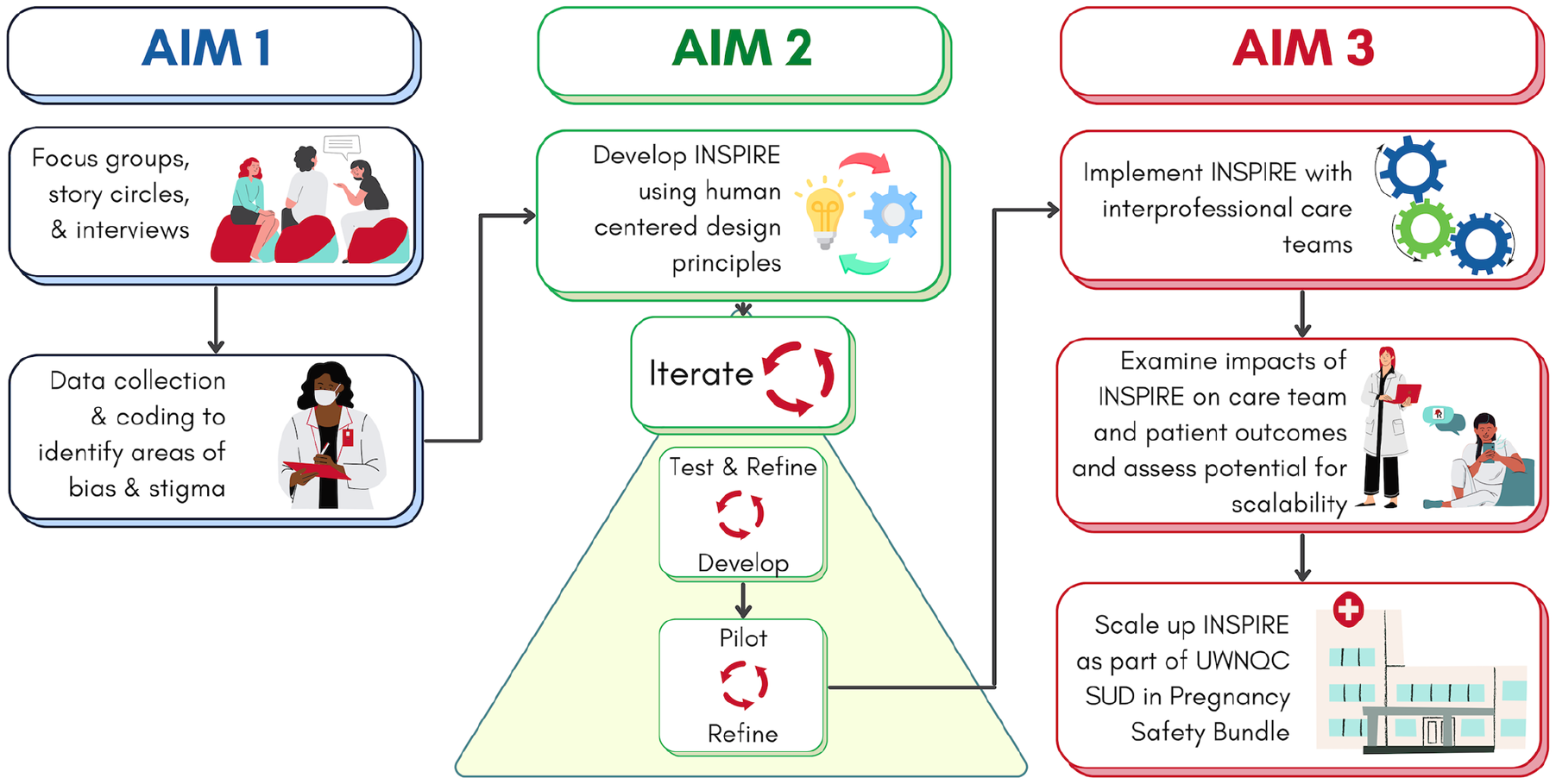
Study overview.
Aim 1: Examine Attitudes and Stigma in Intrapartum Care for Individuals With SUD From Provider and Patient Perspectives
Aim 1 of our study will provide a locally contextualized understanding of quality and stigma in intrapartum care using a robust qualitative approach (Table 1). First, we will conduct focus group discussions (n = 8 groups; n = 10-12 individuals per group) with a diverse range of healthcare professionals across the state of Utah, with an emphasis on rural health facilities. Focus groups will include multidisciplinary providers from all departments (emergency room/triage, labor and delivery, pediatrics) who encounter patients during their intrapartum stay. Purposively selected key informant interviews with healthcare team members (n = 16) will allow us to gather deeper insights into these issues.
Summary of Qualitative Data Collection.
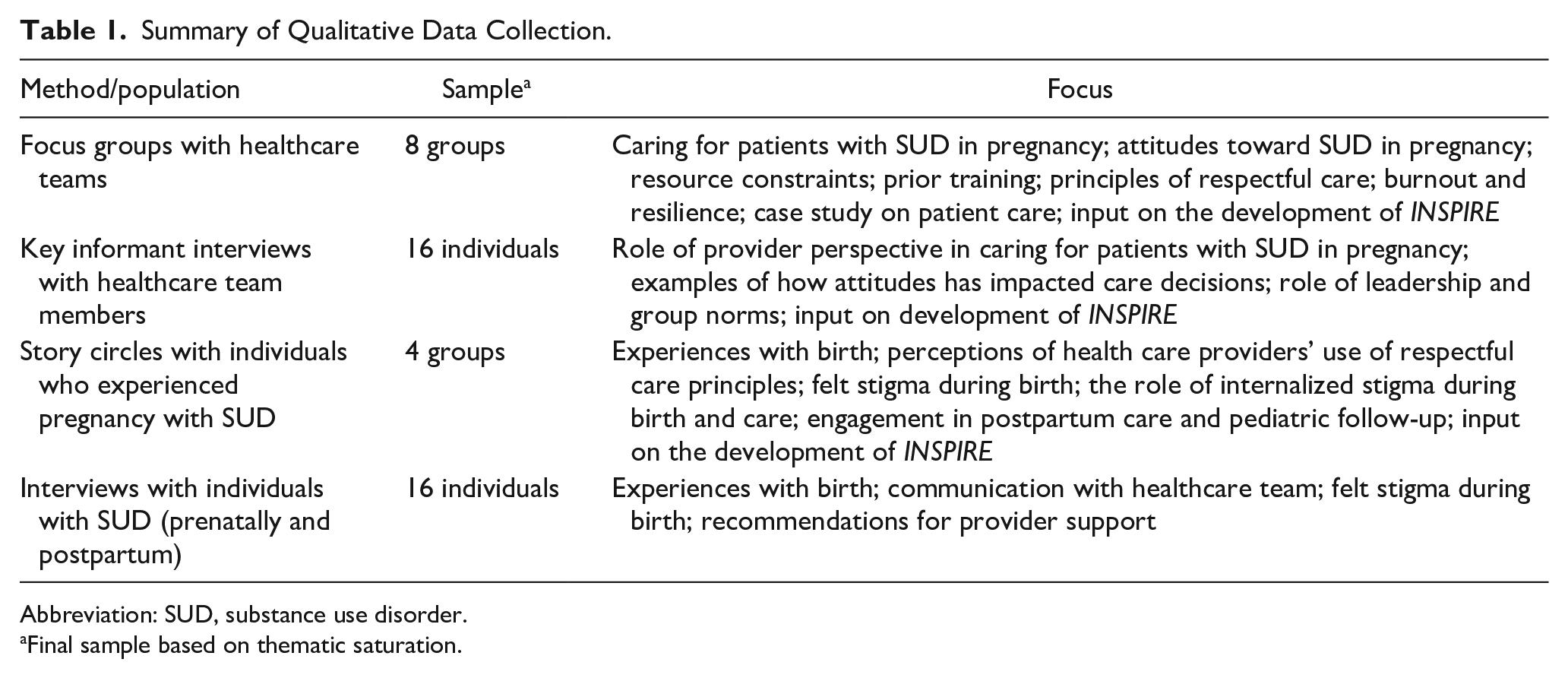
Abbreviation: SUD, substance use disorder.
Final sample based on thematic saturation.
In parallel, we will explore the lived and living experiences of pregnant and postpartum individuals with SUD. We will facilitate restorative justice story circles (n = 4-6 groups; n = 10-15 individuals per group), providing a safe space for participants to share their personal narratives and perspectives. In addition, we will conduct prenatal and postpartum interviews with patients with SUD (n = 16), where we will explore their experiences and interactions with healthcare providers during their prenatal and intrapartum care.
Some participants involved in the qualitative data collection of Aim 1 will be invited to work with a narrative strategist to record their stories. These stories will be integrated into the INSPIRE curriculum to center the experiences of stakeholders.
The methods of Aim 1 will allow us to uncover the nuanced ways in which stigma, provider attitudes, and burnout intersect to shape intrapartum care for individuals with SUD. We will also be able to identify examples of growth, empathy, and resilience in the provider workforce. Through a comprehensive understanding of these dynamics from both provider and patient standpoints, we can inform the development of targeted intervention strategies aimed at mitigating stigma, improving provider–patient relationships, and ultimately enhancing maternal health outcomes in this vulnerable population.
Aim 2: Develop INSPIRE
Aim 2 of our study is dedicated to co-creating the INSPIRE training package. We will use participatory, human-centered design frameworks25,26 to co-design the INSPIRE intervention with stakeholders from healthcare facilities across the state. Drawing insights from Aim 1, we will collaborate with a stakeholder advisory board to create intervention content that addresses clinical empathy, provider knowledge, stigma, and burnout. The use of human-centered design principles, including prototyping the intervention across various facilities statewide, will help ensure scalability and sustainability.
The curriculum will include 3 core modules: an online training module on SUD and childbirth, a 4-hour in-person team simulation, and interactive training on core counseling techniques using artificial intelligence (AI) feedback. Depending on the design process, these modules may be augmented by booster modules (eg, burnout, clinical empathy, and stigma) designed to cater to the diverse learning needs of participants. Content will be hosted on an online learning management system that participants can continue to access after the completion of the intervention.
Aim 3: Evaluate the INSPIRE Package
For Aim 3, we will evaluate the INSPIRE intervention at the University of Utah using a quasi-experimental design. We will enroll care team members (n = 500) from diverse clinical settings, including Labor and Delivery (L&D), Postpartum/Newborn service, and the Emergency Department (ED). We will assess the impact of INSPIRE on participating healthcare teams and the patients they care for, and we will collect process data to determine the potential for scalability. Most healthcare-system training focuses only on nurses and physicians, but there is strong evidence that other members of the healthcare team influence the patient’s experience.27,28 Considering the broader team is especially important in intrapartum care, where patients see a wide variety of staff during their in-patient stay. Enacted stigma microaggressions, or neglect from any of these individuals can undermine a patient’s perception of the care experience. The INSPIRE intervention will extend beyond typical groups to include other members of the clinical team (eg, medical assistants, EMT, social work, reception).
Our evaluation strategy includes measuring the impact of the INSPIRE intervention on both healthcare providers and patients (Figure 2). The primary provider outcome is provider attitudes toward individuals with SUD, which will be assessed at baseline, midline, and 6 months. The primary patient outcome is person-centered maternity care. To measure the impact of the intervention on patient outcomes, we will survey individuals with SUD giving birth at the facility in the year prior to the INSPIRE intervention and the year after the completion of the training. We will enroll individuals who are immediately postpartum with current or treated SUD (n = 100 in each time period) and a matched cohort of individuals birthing without SUD (n = 200). The proposed measures are described in the Protocol Supplement but will ultimately be determined after the final design of the project.
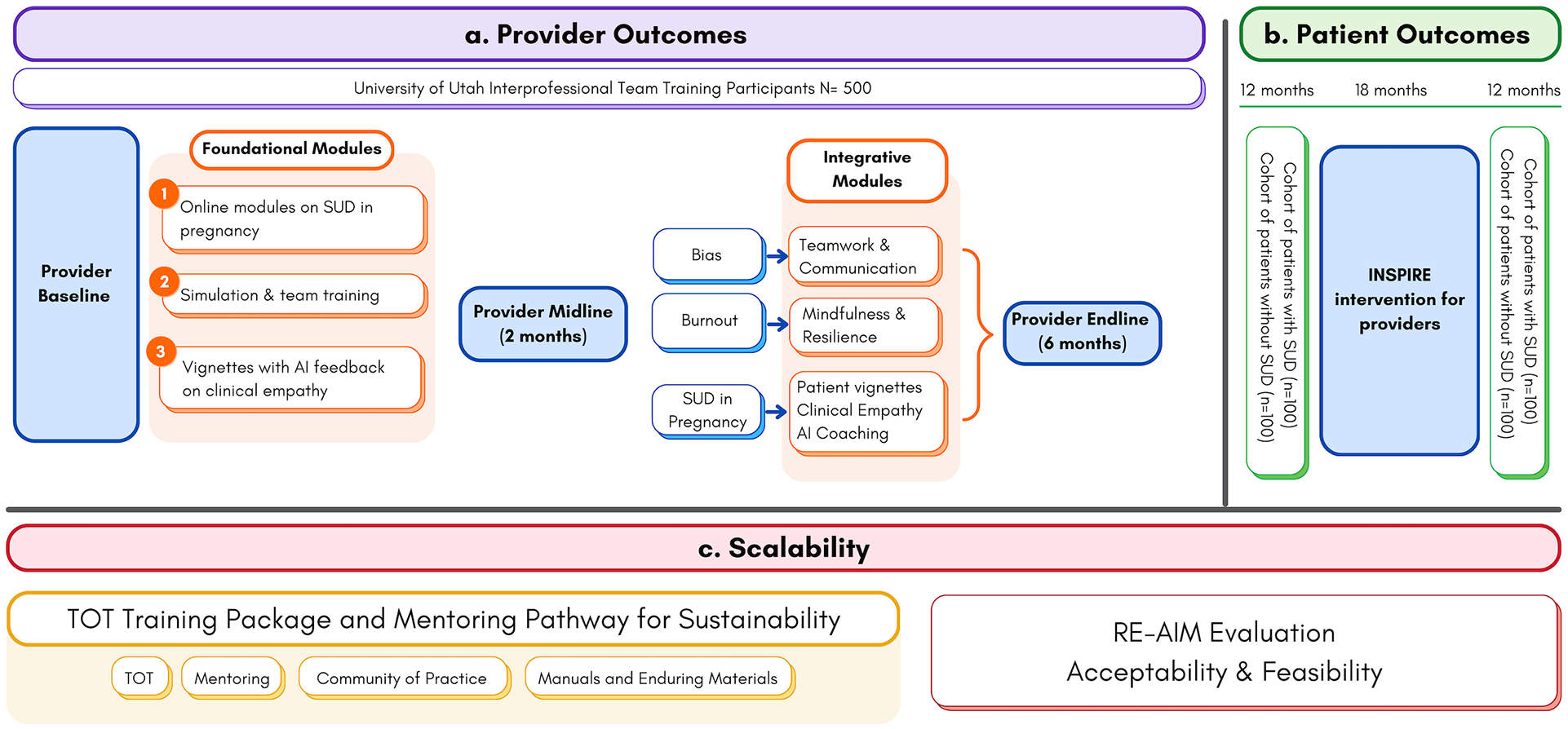
Design of Aim 3.
Concurrent with measuring provider and patient outcomes, we will measure process indicators to examine the potential for INSPIRE to be scaled and sustained to achieve maximum impact. While simulation learning for obstetric and neonatal emergencies is well established and endorsed by accreditation agencies and healthcare systems, the INSPIRE intervention aims to augment its impact by integrating simulation training with modules addressing stigma, burnout, and clinical empathy and making it applicable to all sizes and locations of healthcare facilities. We will assess the potential for widespread program implementation using the RE-AIM framework.29,30
Discussion
This study will develop and evaluate a training program aimed at improving intrapartum care for individuals with SUD. The goal is for the INSPIRE intervention to cultivate a culture of empathy, understanding, and resilience within interprofessional teams, ultimately enhancing care delivery and improving maternal and neonatal outcomes.
INSPIRE is innovative in several ways: it incorporates inter-professional teams, combines in-person simulation and online learning, and employs adaptive design and human-centered design to meet the needs of stakeholders. While most SUD-related training focuses on individual clinical disciplines, INSPIRE brings together physicians, nurses, midwives, social workers, and other healthcare providers, supporting a team-based approach to care. Although simulation is widely used for obstetric skill building, the application of simulation to improve SUD-related maternity care is novel.
There are related models in other clinical domains that highlight the value of simulation, participatory design, and adaptive learning. For instance, highly fidelity simulation-based programs, like the type of simulation proposed in INSPIRE, have successfully improved neonatal resuscitation and newborn outcomes, care during obstetric emergencies, and teamwork.31–34 INSPIRE adapts simulation training for SUD-related obstetric care, a previously unaddressed gap. In addition, healthcare institutions have successfully implemented interactive training programs to address implicit bias in healthcare,35,36 but few have tailored these specifically for SUD in maternity care. Training models leveraging participatory design principles, such as the MAMA interprofessional team-training program, have been implemented to reduce stigma and improve respectful maternity care for other marginalized groups. 33 The INSPIRE program proposes a similar model to integrate stigma reduction strategies into hands-on clinical training to enhance care for individuals with SUD. Other adaptive learning frameworks (eg, the AMA’s Adaptive Learning Initiative) have demonstrated the effectiveness of tailored training. 37 INSPIRE applies this methodology to an underserved patient population, ensuring targeted competency development. 38 Drawing from this evidence base, INSPIRE incorporates best practices in simulation, participatory design, and adaptive training to create uniquely focused training for interprofessional teams.
Simulation training has been proven to enhance clinician self-efficacy in providing evidence-based obstetric care and promoting person-centered, respectful care.21,39–41 Simulation training can help providers navigate the stress and discomfort that may arise in caring for birthing individuals with SUD, 42 enabling them to develop clinical and interpersonal skills to recognize and mitigate their negative attitudes. By equipping providers with the skills and confidence to deliver compassionate, evidence-based care, INSPIRE has the potential to address a critical gap in medical education and improve maternity care for individuals with SUD.
In INSPIRE, the simulation training will be book-ended by interactive online content that helps providers develop the knowledge, skills, and motivation to provide high-quality, respectful care for patients with SUD. Not all providers are the same, and intervention content and dose should reflect different needs. Unlike traditional one-size-fits-all training, INSPIRE’s adaptive structure will customize content based on individual needs including, clinical settings, provider knowledge gaps, and self-efficacy levels, allowing effective and resource-efficient training delivery.43,44
Finally, our human-centered and participatory design process engages local stakeholders, including providers and birthing individuals with lived and living experiences, in co-designing the INSPIRE intervention, enhancing its real-world relevance and adoption. Participatory design25,26 in health system interventions enhances solution efficacy and improves future adoption and sustainability.26,45–50 This collaborative approach positions INSPIRE for successful integration into a statewide implementation in partnership with the Utah Department of Health, ensuring broader reach and long-term sustainability.
The potential impact and significance of INSPIRE extends beyond its immediate training objectives. This project addresses a critical gap in the current healthcare landscape, ensuring that birthing individuals with SUD receive equitable, respectful, and evidence-based care. Provider attitudes, burnout, and poor teamwork contribute to adverse outcomes for both birthing individuals and newborns, and a comprehensive intervention that centers both the provider and the individual receiving care can go a long way to mitigate the effects of these factors. The INSPIRE intervention aims to foster institutional change and promote a culture of empathy and understanding toward people with SUD and within healthcare teams, which has the potential to improve clinical outcomes.
The intrapartum period represents a critical window of opportunity to improve outcomes for individuals with SUD and their newborns. This period is often marked by heightened medical vulnerability, pain management challenges, and significant emotional distress, making it a time when provider interactions can profoundly shape a patient’s experience of care. Research indicates that negative provider attitudes, bias, and punitive policies targeting individuals with SUD during pregnancy can lead to delayed care-seeking, inadequate pain management, and increased psychological distress,51,52 all of which contribute to adverse maternal and neonatal outcomes. By focusing on this pivotal stage, INSPIRE aims to equip healthcare teams with the skills to deliver trauma-informed, evidence-based, and compassionate care when patients need it most.
INSPIRE directly addresses real-time decision-making, communication strategies, and clinical management during labor and delivery, ensuring that providers are prepared to navigate complex patient needs without stigma or bias. This focus on intrapartum care not only enhances maternal and neonatal outcomes but also builds trust between patients and the healthcare system, increasing the likelihood of continued engagement in care and long-term recovery support.
Our strategy for scaling up the INSPIRE intervention follows a multi-phase implementation approach. We will collaborate with the Utah Department of Health and professional healthcare organizations to incorporate INSPIRE into statewide provider training programs, ensuring its adoption across clinical settings. INSPIRE will augment the State offerings and align with current State efforts to implement the AIM Care for Pregnant and Postpartum People with Substance Use Disorder Safety Bundle, a National effort to improve the quality of care for pregnant patients with SUD. 53 INSPIRE will provide a tangible and actionable training package that meets the standards of best practices, enhances provider preparedness, and improves maternal and neonatal outcomes—all targets of the AIM Safety Bundle.
Beyond Utah, the adaptive design of INSPIRE makes it scalable and customizable for different healthcare systems and other states currently implementing the AIM Safety Bundle. We will actively seek partnerships with health agencies in other states to facilitate its broader implementation. To reach a wider audience, we will share our findings through presentations at national conferences (eg, AMERSA, APA, ACOG, SMFM) and publications in peer-reviewed journals. These efforts will engage both academic and clinical stakeholders, positioning INSPIRE as a replicable model for improving intrapartum care for individuals with SUD nationwide.
At the end of the study period, we expect to have a fully developed, evidence-based training program that enhances provider resilience, reduces stigma, and improves maternal and neonatal outcomes. By embedding INSPIRE within statewide and national initiatives, we aim to create a sustainable model that transforms intrapartum care for individuals with SUD and serves as a blueprint for future provider training efforts.
Supplemental Material
sj-docx-1-saj-10.1177_29767342251333641 – Supplemental material for Protocol for the INSPIRE Study: A Training Package for the Intrapartum Team to Promote Respectful and Non-stigmatizing Care for Patients with Substance Use Disorder
Supplemental material, sj-docx-1-saj-10.1177_29767342251333641 for Protocol for the INSPIRE Study: A Training Package for the Intrapartum Team to Promote Respectful and Non-stigmatizing Care for Patients with Substance Use Disorder by Susanna R. Cohen, Assumpta Nantume, Jami Baayd, Olivia R. Hanson, Marcela C. Smid, Rebecca Simmons, Erin P Johnson, Karen W. Tao, Torri D. Metz, Alexandra Gero, Justin D. Smith, Connie Wilson and Melissa H. Watt in Substance Use & Addiction Journal
Footnotes
Author Contributions
SC and MW originated the INSPIRE Project. SC and MW are the Co-Leads of INSPIRE. TM is the PI of the ELEVATE CENTER. SC, MW, AN, and OH worked collaboratively on the first draft of the manuscript. All authors revised the manuscript for critical content and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The INSPIRE study is a project in the University of Utah ELEVATE Maternal Health Center of Excellence, funded by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health (U54HD113169, PI, Torri Metz). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Compliance,Ethical Standards,and Ethical Approval
The University of Utah Institutional Review Board has approved the ELEVATE Center (IRB #00167838) and INSPIRE (IRB #00167800).
ORCID iDs
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.