
Abstract
Background:
To address the urgent housing needs of individuals experiencing unsheltered homelessness and substance use disorder (SUD) living in an encampment, Boston established six harm reduction low-threshold shelter (LTS) sites in January 2022.
Methods:
To understand the LTS guest experience of persons who had been living in the tent encampment, assess early outcomes of the LTS service model, and inform concurrent implementation of this new shelter model, the Boston Public Health Commission implemented a point-in-time survey of 50 individuals who moved from the encampment into LTS three to six months after the encampment closure. The in-person survey assessed participant experience, quality of life, and service access.
Results:
Seventy-two percent to 90.0% of survey participants reported improvements in sleep quality, food security, and connection with others since moving into LTS. Sixty-eight percent to 92.0% of participants indicated increased access to mental health and healthcare providers and housing navigation services. Over 80.0% of respondents reported increased confidence in overdose response since moving into LTS, and almost half reported being in some form of treatment for SUD. Importantly, 90.0% of participants agreed that they had hope for the future.
Conclusion:
Harm reduction transitional shelter spaces remove access barriers to people experiencing unsheltered homelessness and SUD and promote safety, well-being, and access to critical support services and housing navigation.
Keywords
Highlights
A novel low-threshold shelter (LTS) program in Boston improved self-reported quality of life, well-being, access to services, and hope for the future among guests during the early months of its initiation.
Housing First and harm reduction policies at LTS promote early engagement in medical, housing navigation, case management, and substance use services among unsheltered people who use drugs.
Introduction
More than two-thirds of individuals with a history of homelessness in the United States also have histories of substance use disorder (SUD).1,2 Individuals who have experienced homelessness in Massachusetts have drug-overdose fatality rates up to 30 times higher than the general population. 3 In Boston, one in four deaths among unhoused people can be attributed to a drug overdose. 4 Emergency shelter and housing policies often create significant obstacles for people who use drugs,5,6 including requiring sobriety and/or treatment as conditions for admission6-9 and lack adequate harm reduction and supportive services to encourage retention.
Harm reduction programs, practices, and policies have been shown to prevent death and infectious disease transmission, reduce the use of costly healthcare services, and increase access to and use of substance use treatment and other beneficial services. 10 “Housing First” is an evidence-based model that offers a person-centered approach without prerequisites for sobriety or treatment.11,12 Empirical studies have shown that Housing First models, particularly those informed by harm reduction principles, can lead to improved health and housing outcomes, reduced public system costs, and stabilized or improved substance use outcomes.11-15 Although harm reduction-informed services have been identified as critical for addressing the needs of persons with SUD, 16 they are not frequently integrated into shelter and housing models. 12
In 2021, the convergence of the opioid epidemic, housing crisis, and the COVID-19 pandemic contributed to the expansion of a large encampment occupied by approximately 145 unsheltered people who use drugs near the “Mass. & Cass” intersection of Boston. 17 The City of Boston and the Boston Public Health Commission (BPHC) addressed this public health emergency by working with the State and community providers to establish six low-threshold shelters (LTS) with over 200 beds. LTS sought to address barriers to traditional shelter—such as feeling disrespected by staff, concern for physical safety, lack of security of belongings, and need for harm reduction and other services—as was identified by a cohort of unsheltered individuals with SUD in a Boston study. 18 As such, rather than focusing on abstinence or SUD treatment, these LTS utilized a harm reduction and Housing First approach to ensure that unsheltered individuals had an alternative place to stay when the encampment closed in January 2022. 19 In addition to allowing guests to come and go, LTS provide a dedicated room or bed, secure storage, clinical and harm reduction services, and access to permanent housing navigation services.20,21 BPHC conducted a survey with LTS guests who had previously lived in the encampment to understand their initial experience, assess early outcomes, and inform future LTS implementation.
Methods
In December 2021, BPHC censused 145 unsheltered individuals with SUD who were living in the Mass. & Cass tent encampment before its resolution in January 2022. From April to July 2022, trained BPHC interviewers conducted a point-in-time in-person survey with a convenience sample of individuals from the December census who had resided in any of the six LTS. The survey protocol was developed by BPHC staff with knowledge and training in survey methodology and experience working with people with SUD. The survey was not subject to IRB review, as it was implemented to inform the delivery of a new public health service.
Interviewers provided participants with verbal and written information about the survey and obtained verbal consent. Surveys were administered in English or Spanish with an average duration of 18 minutes. A $25 gift card was given to participants upon completion.
Survey items were developed based on five domains that LTS were designed to impact: (1) well-being; (2) quality of life; (3) access to medical care and other services; (4) harm reduction and substance use; and (5) hope for the future. These domains were derived from barriers to shelter identified by individuals experiencing unsheltered homelessness and SUD that LTS aimed to address (i.e., respect, safety, storage, service access). 18 LTS guest experience questions were informed by an existing shelter client experience survey 22 and outcomes expected because of LTS program model (i.e., hope for the future).23,24 The 40 questions, primarily Likert and multiple-choice, focused on LTS guest demographics, LTS experience, quality of life, and service access since moving into LTS. Two open-ended questions asked about what changed for the better and worse since moving into LTS.
Descriptive statistics were performed using Stata v16.1 (College Station, TX, USA). Transcribed text responses to the two open-ended questions were manually coded by two team members into the survey’s five thematic domains. Content analysis of the qualitative data was performed, and illustrative participant quotes were used to highlight key survey findings.
Results
Participant Characteristics
Of the 50 survey participants (Table 1), 24 (48.0%) were White, 10 (20.0%) were Black, 4 (8.0%) were American Indian/Alaska Native, and two (4.0%) identified as multiple races. Nineteen (38.0%) of the participants identified as Hispanic/Latino(a)(x). Over half of the participants were 35 to 44 years of age (52.0%), over half were male (58.0%), and the majority identified as heterosexual (80%). Sixty-six percent of respondents had lived in the tent encampment for one year or more. The substances used most reported by participants included opioids (78.0%), cocaine/crack (68.0%), methamphetamine (34.0%), and benzodiazepines (26.0%), with over three-quarters (76.0%) of participants reporting polysubstance use.
Baseline Characteristics of Survey Participants.
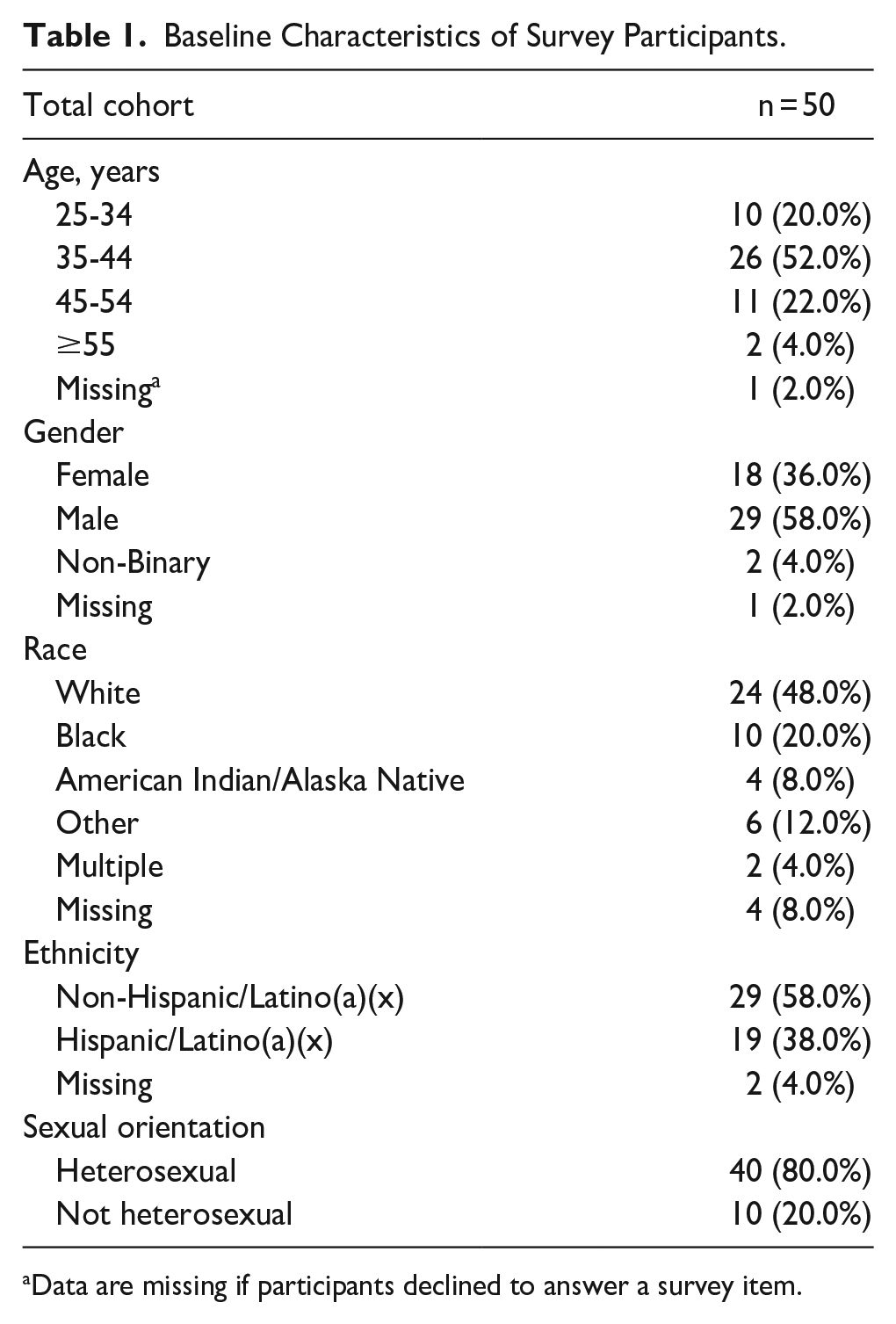
Data are missing if participants declined to answer a survey item.
Findings
Well-Being
“I have a safe place to stay. . .the support is not far.” – Latinx female LTS guest
When asked about how they were treated within LTS sites, a vast majority of participants agreed or strongly agreed that their sexual orientation (97.9%), gender (95.7%), and racial/ethnic (97.9%) identities were respected by LTS staff (Table 2). Most participants agreed or strongly agreed that they trusted staff (72.9%) and other guests (62.0%) (Table 2). In addition, 61.2% of participants reported improvement in connection with others since moving into LTS (Table 3).
Participant Rating of Experience at LTS
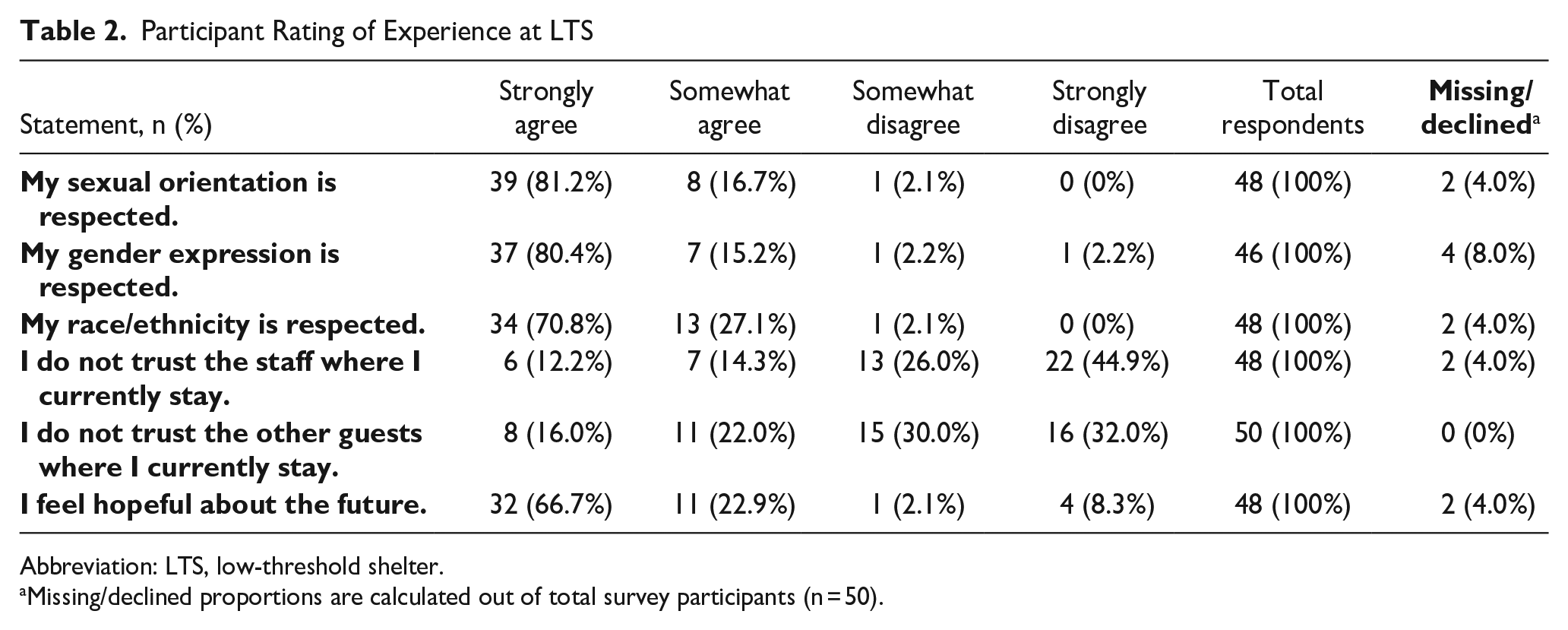
Abbreviation: LTS, low-threshold shelter.
Missing/declined proportions are calculated out of total survey participants (n = 50).
Participant Rating of Change in Quality of Life Since Moving to LTS
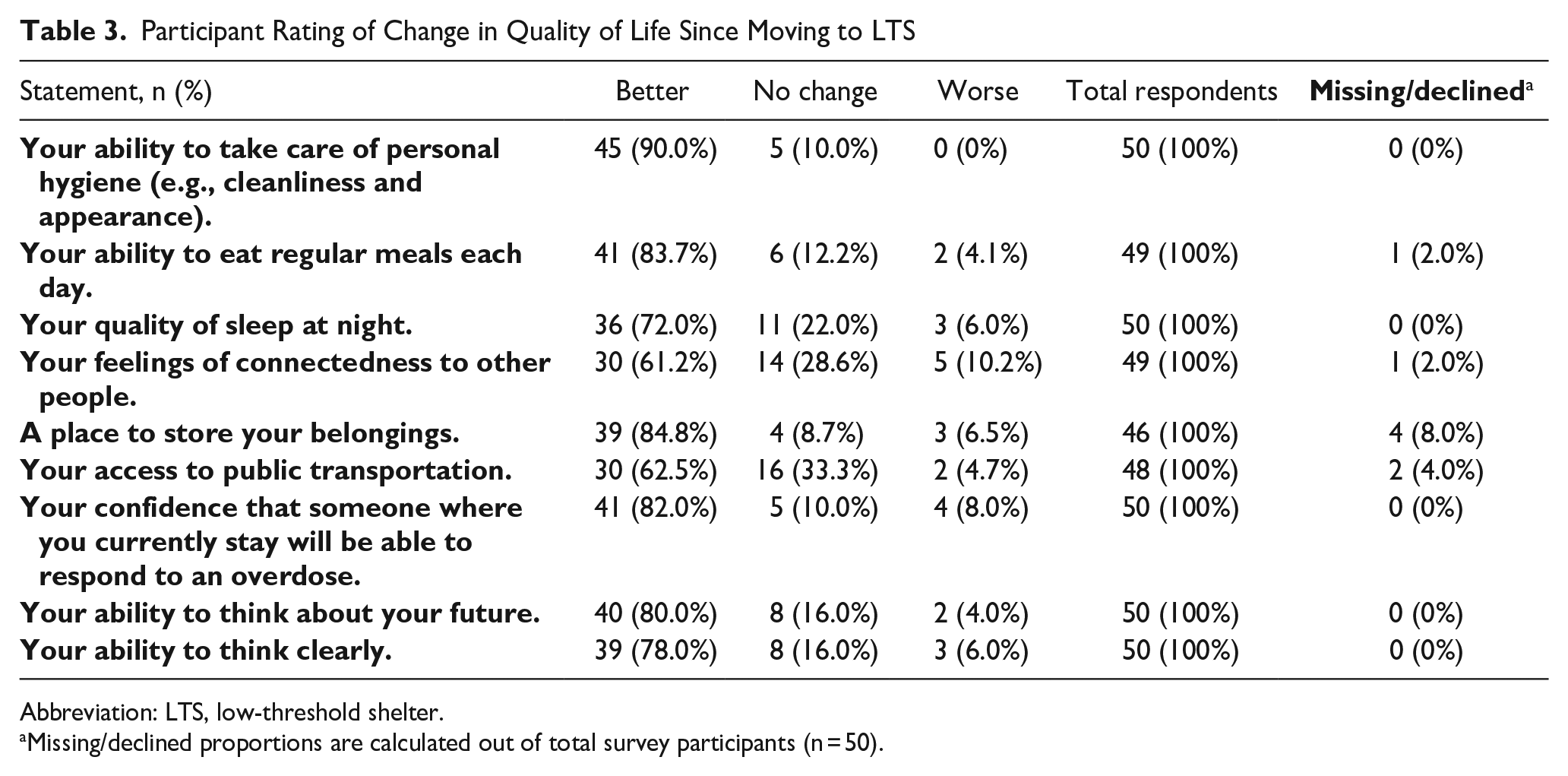
Abbreviation: LTS, low-threshold shelter.
Missing/declined proportions are calculated out of total survey participants (n = 50).
Quality of Life
“Rest time. . .body-wise and appearance-wise. . .are better. I’m not worried about my next meal or where I am going to sleep at night.” – Black male LTS guest
This quote represents the range of quality-of-life improvements that were reported by participants since moving to LTS. A vast majority reported better ability to take care of personal hygiene (90.0%), access to food and nutrition (83.7%), and quality of sleep at night (72.0%). Most participants (84.8%) indicated better ability to safely store their personal belongings and improved access to public transportation (62.5%) (Table 3).
Access to Services
“I’m not homeless now; I have resources provided so I can get situations resolved. Housing, medical, and whatever is needed is provided.” – White male LTS guest
Participants were asked whether they had access to medical services and whether they had gained or maintained that access after leaving the encampment. Most participants reported having access to a medical provider (82.0%) and a mental health provider (68.0%). Among participants who had provider access, 26.8% and 32.4%, respectively, reported gaining that access after moving to an LTS (Figure 1).
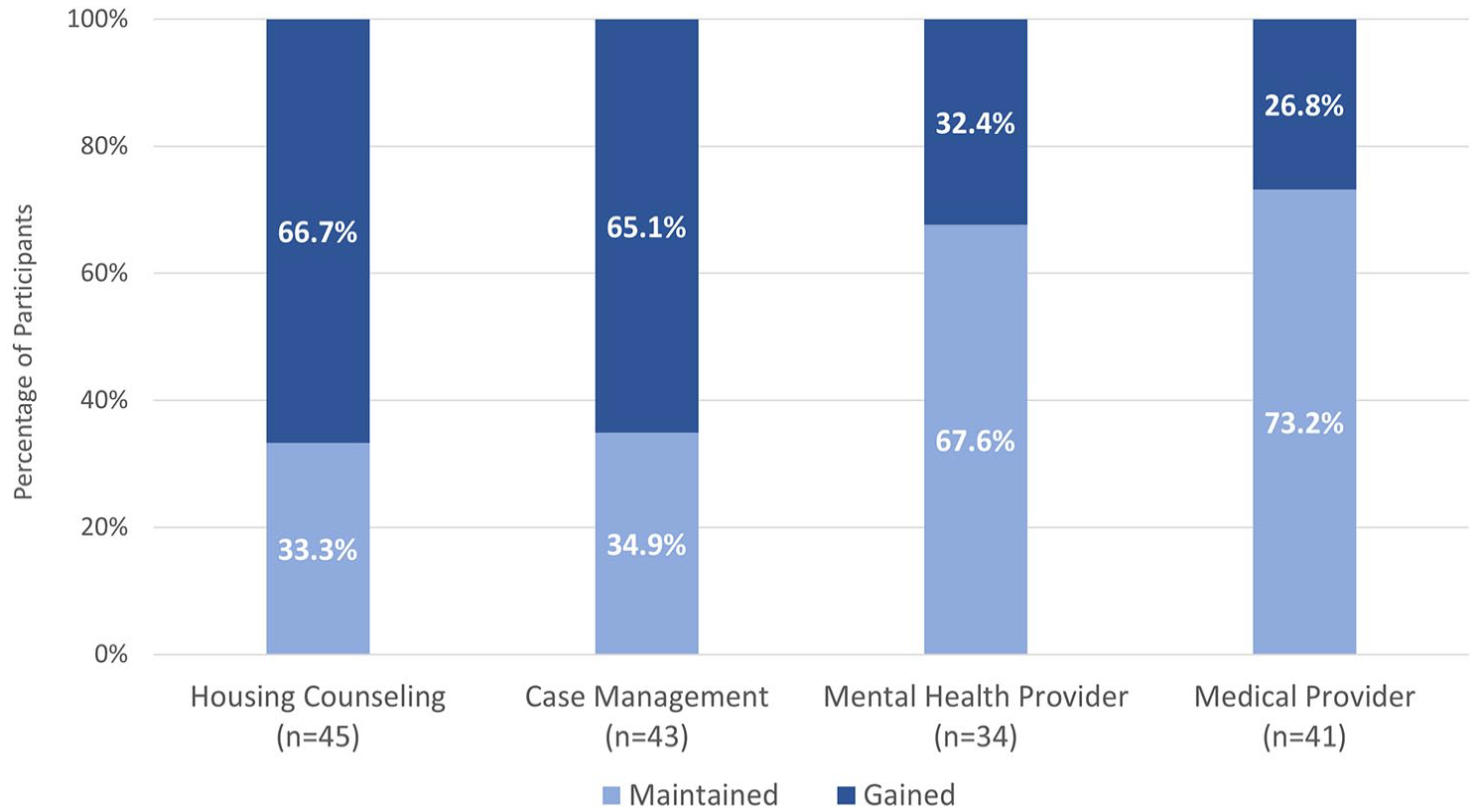
Participant self-reported access to housing navigation and case management services since moving to LTS.*
Participants were also asked about their access to non-medical services after leaving the encampment. Housing navigation is a core component of the LTS model. Nearly all participants (91.8%) reported being connected to housing counseling, and 86.0% were connected to case management. Notably, approximately two-thirds of those participants indicated that they gained access to housing counseling (66.7%) and case management (65.1%) since moving to LTS (Figure 1).
Substance Use and Harm Reduction
“I’ve got a home after 14 years. I’m not using (drugs). I relapsed, but I didn’t go overboard. . .Each time, a longer time sober. – Unknown race/ethnicity female LTS guest
As the quote above captures, most respondents (70.8%) reported decreased frequency of any substance use since moving to LTS. Among the 54% of participants who reported polysubstance use with opioids and cocaine/crack, 66.7% reported decreased use frequency. Participants also reported increased confidence that an overdose would be reversed by someone (82.0%) since moving into LTS (Table 3). Furthermore, while SUD treatment is not a requirement for stay and LTS are designed for people who use drugs, nearly half of the respondents (44.9%) reported some form of SUD treatment, with 61.9% among those starting treatment within the prior six months of survey administration. Of note, most of these respondents (86.4%) reported using medication for opioid use disorder.
Future Hope
“Started having hope and faith and believing in myself.” – Black male LTS guest “My overall future, I can see things coming together a lot easier.” – White male LTS guest
These quotes highlight the finding that 89.6% of participants agreed or strongly agreed with the statement, “I feel hopeful about the future” since moving to LTS (Table 2). Similarly, and related, a large proportion of participants reported that their ability to think clearly (78.0%) and to think about the future (80.0%) was better since moving into LTS (Table 3).
Discussion
The LTS participant survey provided important guest feedback on the changes that LTS set out to effect within three to six months of moving from the encampment into LTS. Findings highlight the crucial role of shelter-based harm reduction policies in fostering support for people who use drugs, improving well-being, overdose safety, social cohesion, and service access.
The early experiences and participant acceptance of the Boston LTS, Massachusetts’ first harm reduction shelter model, fill gaps in the literature regarding the implementation of interventions for the dual public health crises of homelessness and SUD. Our survey findings during the start-up phase of LTS provide promising strategies for addressing the immediate needs of people with SUD experiencing homelessness. Specifically, the early positive experiences of guests demonstrated that Boston’s LTS policies, staffing, and housing services made LTS effective at engaging unsheltered individuals with SUD who had previously lived in an encampment and did not utilize traditional shelter.
Recent publications about the Boston LTS interventions further bolster these findings by highlighting longer-term outcomes of LTS.20,21,25,26 One study of a Boston LTS with co-located clinical services found that in the first year, 100.0% of guests engaged with case management, 49.0% engaged with SUD treatment, and 25.0% moved to permanent housing. 21 Two qualitative studies of the Boston LTS sites25,26 found that guests benefited from having their basic needs met in a safe and stable environment serviced by supportive, “non-judgmental and trustworthy” 26 staff. These studies reinforce our findings that LTS are accepted by guests and result in increased access to and engagement with clinical and behavioral health providers, case management, housing navigation, and other supportive services.
In addition, the findings from this assessment were applied to inform Boston LTS operations. Specifically, guest feedback was used to revise the LTS Practice Guidance (Supplemental Appendix A), integrate LTS referral processes with street outreach activities, guide BPHC’s expansion of LTS spaces in their large emergency shelter, and sustain funding for the LTS model beyond initial funding.
There are some limitations to these survey findings. First, the survey sample only included individuals from the encampment census who were placed in and stayed at LTS, and does not include the experience of those who did not move into LTS. Second, data on the types and frequency of services provided to participants at each LTS were not gathered. As a result, we could not determine the impact of different LTS service models on participant outcomes. Lastly, convenience sampling and a small sample size did not allow for statistical analyses of outcomes by LTS site or participant demographics.
Future BPHC studies will assess variation in LTS guest experience by race, gender, and age, along with long-term outcomes by program model, including subsequent permanent housing placement, retention, and service engagement. Additional studies will also evaluate which LTS policies and practices are most effective at improving long-term individual-level outcomes.
Conclusion
LTS plays a key role in sheltering people experiencing chronic unsheltered homelessness and SUD who had previously lived in an encampment. Within the first three to six months of moving from an encampment into a harm reduction-focused LTS, participants experienced their stays positively and reported improvements in quality of life, well-being, access to medical and housing services, substance use frequency and treatment uptake, and hope for the future. Boston’s LTS can serve as a model for municipalities aiming to address sheltering strategies for people living in encampments in compassionate, client-centered, stabilizing, and effective ways.
Supplemental Material
sj-pdf-1-saj-10.1177_29767342251344398 – Supplemental material for “From Homelessness to Safety”: Short-Term Outcomes of Low-Threshold Shelter on Individuals Experiencing Substance Use Disorder and Unsheltered Homelessness
Supplemental material, sj-pdf-1-saj-10.1177_29767342251344398 for “From Homelessness to Safety”: Short-Term Outcomes of Low-Threshold Shelter on Individuals Experiencing Substance Use Disorder and Unsheltered Homelessness by Sunday Taylor, Michele N. Clark, Sumaiya Miah, Bhav Jain and Bisola O. Ojikutu in Substance Use & Addiction Journal
Footnotes
Acknowledgements
We would like to thank all the Boston low-threshold shelter guests, staff, and BPHC staff who participated in and administered the survey.
Author Contributions
ST: developed evaluation, designed and implemented survey, interpreted results, and contributed to the writing of the manuscript. MNC: developed evaluation, designed survey, interpreted results, and contributed to the writing of the manuscript. SM: analyzed and interpreted results, created tables and figures, and contributed to the writing of the manuscript. BJ: cleaned and processed data, analyzed results, drafted tables and figures, and reviewed final manuscript. BOO: developed evaluation, provided critical review of survey tools, results, manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: BPHC evaluation team time was supported through City of Boston funding. Stipends for the participant gift cards were funded with American Rescue Plan Act (ARPA) funds.
Compliance,Ethical Standards,and Ethical Approval
Institutional Review Board approval was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.