
Abstract
Background:
Adolescent (12-17 years) and young adult (18-25 years) nonmedical use of prescription tranquilizer medication (ie, short-acting benzodiazepines) is linked to high rates of other substance use and psychopathology. Using probability-based US survey data, we sought to identify nonmedical tranquilizer use motive latent classes by age group and identified links between latent class membership and other substance use and mental health outcomes.
Methods:
Data were from the 2015 to 2019 National Survey on Drug Use and Health (67 971 adolescents; 69 432 young adults), with motive data from 889 unweighted adolescents and 2819 unweighted young adults. Latent class analysis identified subgroups based on motives, accounting for the complex sampling, and with the most likely class membership assigned via a modal approach. Logistic regression linked latent class membership to substance use, mental health, and sociodemographic characteristics.
Results:
Analyses revealed 5 adolescent latent classes: Relax (35.0%), Multi-Motive (26.3%), Experimenter (22.0%), Sleep (9.2%), and Emotional Coping (7.4%). There were also 7 young adult classes: Relax (30.2%), Sleep (18.8%), Multi-Motive/High (17.1%), Experimenter (13.9%), Emotional Coping/Relax (12.8%), Multi-Motive/Self-Treatment (4.8%), and Other Drug Enhancement (2.4%). Within those engaged in nonmedical use, the adolescent and young adult multi-motive classes with frequent endorsement of “to get high” had the highest odds of other substance use and mental health concerns.
Conclusion:
Latent class profiles based on nonmedical tranquilizer use motives differ between adolescents and young adults, though the Multi-Motive classes with frequent endorsement of “to get high” are in greatest need of identification and intervention.
Highlights
We formed adolescent and young adult nonmedical tranquilizer motive latent classes.
Model fit suggested that 5 and 7 classes in adolescents and young adults, respectively.
Multi-motive/high classes had the poorest substance use and mental health profiles.
Nonmedical use warrants intervention, with multi-motive classes in greatest need.
Introduction
Prescription tranquilizers are short-acting medications often used to treat anxiety or insomnia and are almost exclusively benzodiazepine medications. 1 While appropriate (or medical) tranquilizer use can reduce anxiety or insomnia, 2 nonmedical use of prescription tranquilizer medication poses significant risks, including increased likelihood of accidents, other substance use, and substance use disorder (SUD) symptoms.1,3 Nearly 11 000 US overdose deaths involved a benzodiazepine in 2022, a 25% increase since 2015, and a nearly 70% increase since 2010. 4 Nonmedical tranquilizer use is characterized as any use without a prescription and/or use in ways not intended by the prescriber, including at higher doses, non-orally, or with other psychoactive substances. 1 While less prevalent than nonmedical prescription opioid or stimulant use, nonmedical prescription tranquilizer use is also a threat to public health and is relatively understudied. 1
McHugh and colleagues 3 found that 2% of the US population engaged in nonmedical benzodiazepine use annually over 2015 to 2019, with roughly 18% of those who had any benzodiazepine exposure (ie, medical and/or nonmedical use) engaged in nonmedical use. The highest nonmedical use rates were in young adults, 18 to 25 years, 3 with the 2022 US National Survey on Drug Use and Health (NSDUH) estimating that 2.2% of young adults engaged in past-year nonmedical tranquilizer use. 5 While nonmedical tranquilizer use is less common in adolescents (12-17 years), at 0.4% in the 2022 NSDUH, they are another key population in which to study nonmedical tranquilizer use. Adolescent substance use initiation is linked to poor outcomes in adulthood,6,7 and odds of other concurrent substance use and mental health symptoms are particularly elevated in adolescents and young adults engaged in nonmedical tranquilizer use. 8
Given the risks of nonmedical prescription tranquilizer use, research identifying potential mechanisms underlying such nonmedical use and highlighting high-risk groups could be valuable in informing prevention and treatment interventions. Motives for substance use, including nonmedical tranquilizer use, capture the intended goals of use or nonmedical use, 9 and identification of motives could point to undertreated symptoms to address more safely and effectively. For instance, nonmedical tranquilizer use to promote sleep or relieve anxiety can be treated with non-pharmacological interventions, such as cognitive-behavioral therapies or exercise10-12 or using medications with lower potential for nonmedical use, such as orexin antagonists for sleep or selective serotonin reuptake inhibitors for anxiety.13-15
This research had 3 main aims. First, we aimed to derive latent classes of adolescents and young adults, separately, based on nonmedical prescription tranquilizer use motives. Second, we aimed to identify differences in latent class profiles between adolescents and young adults. We considered these age groups separately, as many young adults assume responsibility for medication management in the transition from adolescence 16 and may utilize different medication sources for nonmedical use. 17 Finally, we evaluated links between latent class membership and sociodemographic, mental health, and other substance use correlates. To accomplish the aims, we used aggregated data from the 2015 to 2019 NSDUH.
Materials and Methods
The NSDUH is a national probability-based survey of US residents ages 12 and older that provides national estimates of substance use and related behaviors. The survey methodology employs an independent, multistage area probability design, with oversampling of adolescents and young adults, and survey weights produced using US Census data. To foster honest and valid reporting, the NSDUH uses audio computer-assisted self-interviewing (ACASI) for sensitive topics like substance use behaviors, consistency checks based on prior answers, and skip-outs. For 2015 to 2019, the weighted household screening response rate ranged from 79.7% to 70.5%, and the weighted interview rate ranged from 69.7% to 64.9%,18-22 similar to other national surveys. 23
We used the 2015 to 2019 NSDUH over newer data for 2 reasons. First, methodological changes prevent aggregation of the 2020 to 2022 data with prior years or aggregation of the 2020 data with any other NSDUH data. 24 Second, only 66 adolescents and 313 young adults provided nonmedical tranquilizer use motive data in the 2021 to 2022 NSDUH, preventing stable latent class estimation, likely due to COVID-19-related declines in tranquilizer diversion and nonmedical use. 25 The Texas State University IRB approved the NSDUH, and the first author’s IRB exempted this research from further oversight. Readers are referred to other resources18-22 for specific NSDUH methodological details.
For these analyses, 67 981 adolescents and 69 432 young adults were included. Of these, 889 adolescents and 2819 young adults engaged in past-year nonmedical use and provided data on nonmedical tranquilizer use motives.
Measures: Nonmedical Tranquilizer Use Motives
Participants were asked about any lifetime tranquilizer medication, which includes nonmedical use. Those with lifetime use were asked about nonmedical use specifically, or use “in any way a doctor did not direct” that includes use without a prescription, use more frequently and/or at higher doses than prescribed, or in any other non-directed way (eg, non-orally). This assessment uses both trade and generic medication names with medication pictures to foster accurate recall. Those with lifetime tranquilizer nonmedical use are asked about the timing of the most recent episode.
Motives are only assessed among those with past-year nonmedical use: “What were the reasons you used [specific tranquilizer(s)] the last time in any way a doctor did not direct you to use it/them?” Motives were to relax or relieve tension, experiment or see what it’s like, to feel good or get high, help with my sleep, help me with my feelings or emotions, increase or decrease the effect(s) of some other drug, because I am “hooked” or have to have it, and the other reason I reported. Answers were dichotomous (yes/no). Per prior research, 26 we excluded “other reason”, as they are coded back into the pre-existing categories when possible and are heterogeneous (eg, suicidality and “peer pressure”).
Measures: Substance Use, Mental Health, and Sociodemographic Characteristics
Substance use characteristics included 30-day binge alcohol use, 30-day cannabis use, past-year nonmedical prescription opioid use, past-year nonmedical prescription stimulant use, any past-year non-nicotine SUD, and past-year nicotine dependence. For non-nicotine SUD, the DSM-IV criteria captured abuse or dependence diagnoses from alcohol, cannabis, cocaine, heroin, hallucinogens, inhalants, methamphetamine, prescription opioids, tranquilizer/sedatives, and stimulants. Past-year nicotine dependence was assessed using the Nicotine Dependence Syndrome Scale. 27 Per US National Institute on Alcohol Abuse and Alcoholism (NIAAA) guidelines, binge drinking was defined as consumption of 4 (females) or 5 (males) alcoholic drinks at one occasion. 28
The mental health measures included DSM-IV major depression for all participants with suicidal ideation and serious psychological distress (SPD) 29 assessed only in young adults.
Included sociodemographic characteristics were age (ordinal from 12 to 23 years with 24/25 aggregated in the public use files), race and ethnicity (self-reported, using US Census Bureau categories), sex, household income, population density in area of residence, uninsured status, housing instability (ie, ≥2 past-year residential moves), and living in poverty. Educational status was included and defined as adolescents currently in school or young adults currently in college, or having graduated. In young adults, sexual minority identity (ie, gay, lesbian, or bisexual) was also captured; the 2015 to 2019 NSDUH does not assess this in adolescents.
Data Analyses
Analyses used both Mplus 8.11 (Muthén & Muthén, Los Angeles, CA) and Stata 18 (Stata Corp, College Station, TX). First, we conducted latent class analysis (LCA) in Mplus, using the 7 nonmedical tranquilizer use motives as binary indicators. All LCA models were estimated via robust full-information maximum likelihood methods, incorporating the NSDUH’s complex sampling features and weighting. All models employed a minimum of 800 000 random starts and 20 iterations to prevent local maxima from impacting model estimation, and the best log-likelihood values were replicated. Once the best-fitting model was selected in each age group (see Results), each respondent’s most likely class membership was estimated using a modal approach. 30 As a sensitivity check, we also used the 3-step methodology for regressions in Mplus. 31 Given that our final latent class solutions evidenced strong class separation (entropy) and data suggesting that modal assignments were based on high probabilities, and given that there were minimal differences between the results from the modal and BCH approaches, we focused on results from the modal approach below.
Following latent class estimation, we used cross-tabulations to estimate sociodemographic characteristics by modal class membership, using design-based Rao-Scott tests (converted into F-values) to evaluate omnibus differences among latent classes. Finally, design-based logistic regression models estimated odds ratios of the sociodemographic, mental health, and substance use characteristics by latent class. These models adjusted for sex, age, race and ethnicity, income, and population density, given evidence of differences in these characteristics by latent classes. Separate models were fitted by age group, and separate models within each age group set different reference classes, with one set using those without past-year nonmedical tranquilizer use (who were not included in the LCA) as the reference group. Another set used the relax latent class as the referent, as nonmedical tranquilizer use to relax is linked to relatively lower rates of concurrent substance use and mental health concerns in adolescents and young adults. 32
Results
Latent Class Structure
Due to the complex sampling features of the NSDUH, only Akaike Information Criteria, Bayesian Information Criteria (BIC), and sample size-adjusted BIC are available in Mplus. Model fit relied on BIC because it accounts best for the NSDUH’s complex sampling, 33 with differences of ≥10 points favoring the lower BIC model. 34 Class separation was evaluated using entropy, with values of 0.8 or greater indicating good separation, and the final model was chosen by considering both model fit and interpretability. 35 Fit indices are provided in online-only Supplemental Table A.
In adolescents, the 5-class model (see Supplemental Figure 1) had the lowest BIC (5467.054) and strong entropy (0.89). The largest class in this model was the Relax class (an estimated 35.0% of adolescents with nonmedical tranquilizer use), with 100% endorsement of “to relax”, lower endorsement of “to sleep” (18.2%) and “to help with emotions” (15.4%), and very low endorsement of other motives (≤3%). A Multi-motive class (26.3%) had high levels of endorsement of “to get high,” “to relax,” and “to help with emotions” (all ≥65%), and moderate endorsement of “to experiment” (49.6%) and “to sleep” (32.2%), and the Experimenter class (22.0%) had 100% endorsement of “to experiment,” 28.6% endorsement of “to get high,” and infrequent endorsement of other motives (≤5%). Finally, there were smaller Sleep (9.2%) and Emotional Coping (7.4%) classes. These 2 classes had 100% endorsement of the motive used to name the class and low endorsement of all other motives (≤5%); the one exception was 10.2% endorsement of “to get high” in the Sleep class.
In young adults, a seven-class solution was selected (see Supplemental Figure 2). While both the 6- and 8-class solutions were within 10 points of the BIC of the seven-class scale (16 860.408, 16 866.631, and 16 871.412 for 6, 7, and 8, respectively) and entropy above 0.80, the 7-class solution provided a good balance of parsimony and interpretability. The 6-class solution was similar to the 7-class solution, though it had a larger and more heterogeneous “Relax” class, with over 20% endorsement of both “to sleep” and “to help with emotions”; the purer “Relax” class and the 2 Multi-Motive classes that were split by greater recreational (ie, Multi-Motive/High) and psychopathology symptom-focused motives (ie, Multi-Motive/Self-Treatment). The eight-class solution created a third Multi-Motive group, reducing the sample size of the Multi-Motive classes by splitting the Multi-Motive/High class.
The largest young adult class was the Relax class (30.2% of young adults engaged in nonmedical tranquilizer use), characterized by 100% endorsement of “to relax” and low endorsement (≤7%) of other motives. This class was followed by 4 classes containing an estimated 12% to 19% of the sample engaged in nonmedical use: Sleep (18.8%), Multi-motive/High (17.1%), Experimenter (13.9%), and Emotional Coping/Relax (12.8%). The Sleep class had 100% endorsement of “to sleep,” 39.2% endorsement of “to relax,” and low endorsement (≤6%) of other motives. The Multi-motive/High class had high levels of endorsement of “to relax,” “to get high,” “to help with emotions,” and “to sleep” (all >50%), with relatively frequent endorsement of “to experiment” (40.7%) and “to alter other drug effects” (24.3%). All members of the Experimenter class endorsed “to experiment,” with lower levels of “to get high” (19.9%) and “to relax” (11.3%); those in the Emotional Coping/Relax class were marked by 100% endorsement of “to help with emotions,” 48.3% endorsement of “to relax,” and 10.2% endorsement of “to get high.”
The final 2 young adult classes were the Multi-motive/Self-treatment (4.8%) class and the Other Drug Enhancement class (2.4%). The former class was marked by very high endorsement (>80%) of “to relax,” “to sleep,” and “to help with emotions,” along with 20.7% endorsement of “to get high.” The Other Drug Enhancement class had relatively high rates of endorsement of “to alter other drug effects” (87.6%) and “to get high” (43.3%), and the highest endorsement of “because I am hooked” of any class (14.5%). Sociodemographics of adolescents and young adults by latent class are captured in Tables 1 and 2, respectively. Significant differences between latent classes were observed in adolescents by sex, race and ethnicity, and population density in the area of residence. For young adults, significant differences between latent classes were observed for sex and race, and ethnicity.
Estimated Distributions of Sociodemographic Characteristics by Latent Class, in Adolescents (n = 67 981).
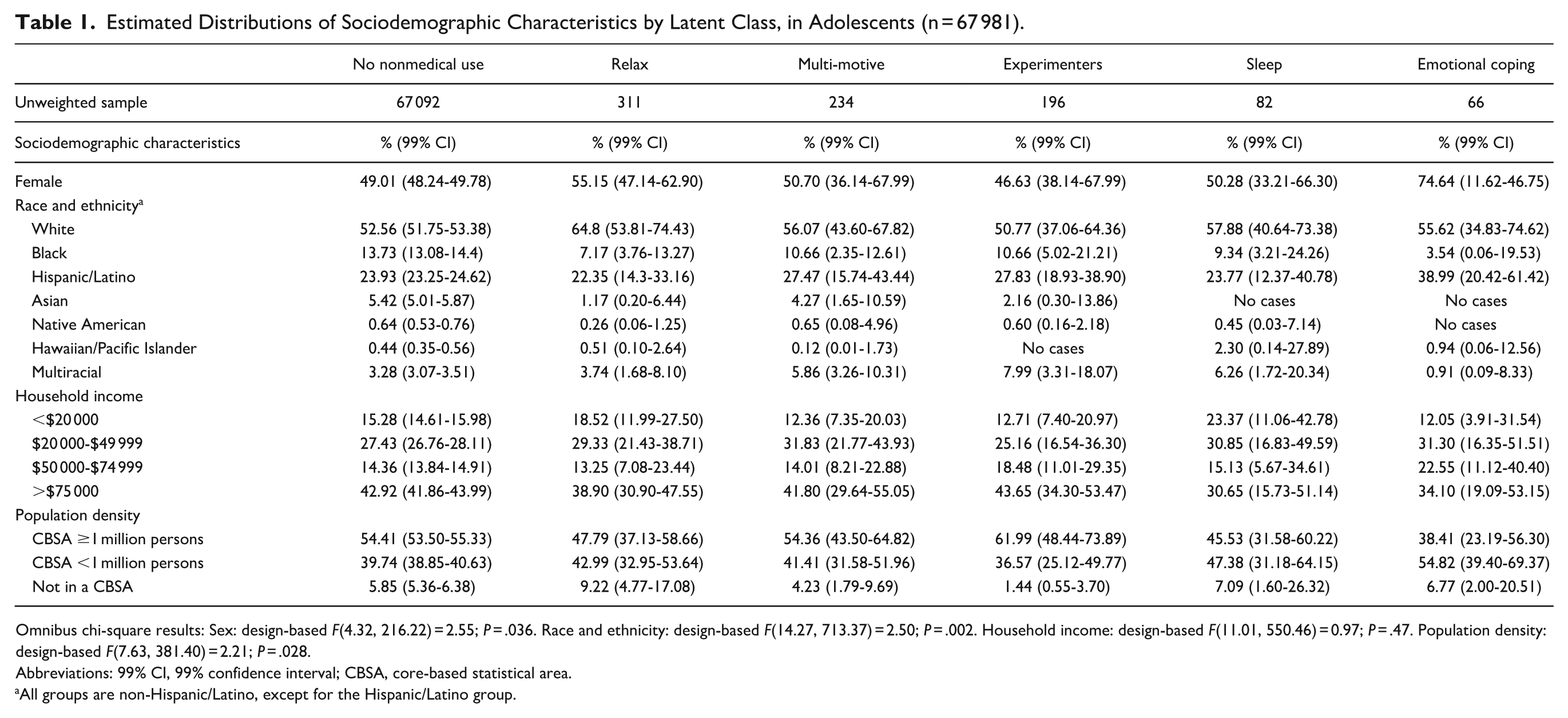
Omnibus chi-square results: Sex: design-based F(4.32, 216.22) = 2.55; P = .036. Race and ethnicity: design-based F(14.27, 713.37) = 2.50; P = .002. Household income: design-based F(11.01, 550.46) = 0.97; P = .47. Population density: design-based F(7.63, 381.40) = 2.21; P = .028.
Abbreviations: 99% CI, 99% confidence interval; CBSA, core-based statistical area.
All groups are non-Hispanic/Latino, except for the Hispanic/Latino group.
Estimated Distributions of Sociodemographic Characteristics by Latent Class, in Young Adults (n = 69 432).
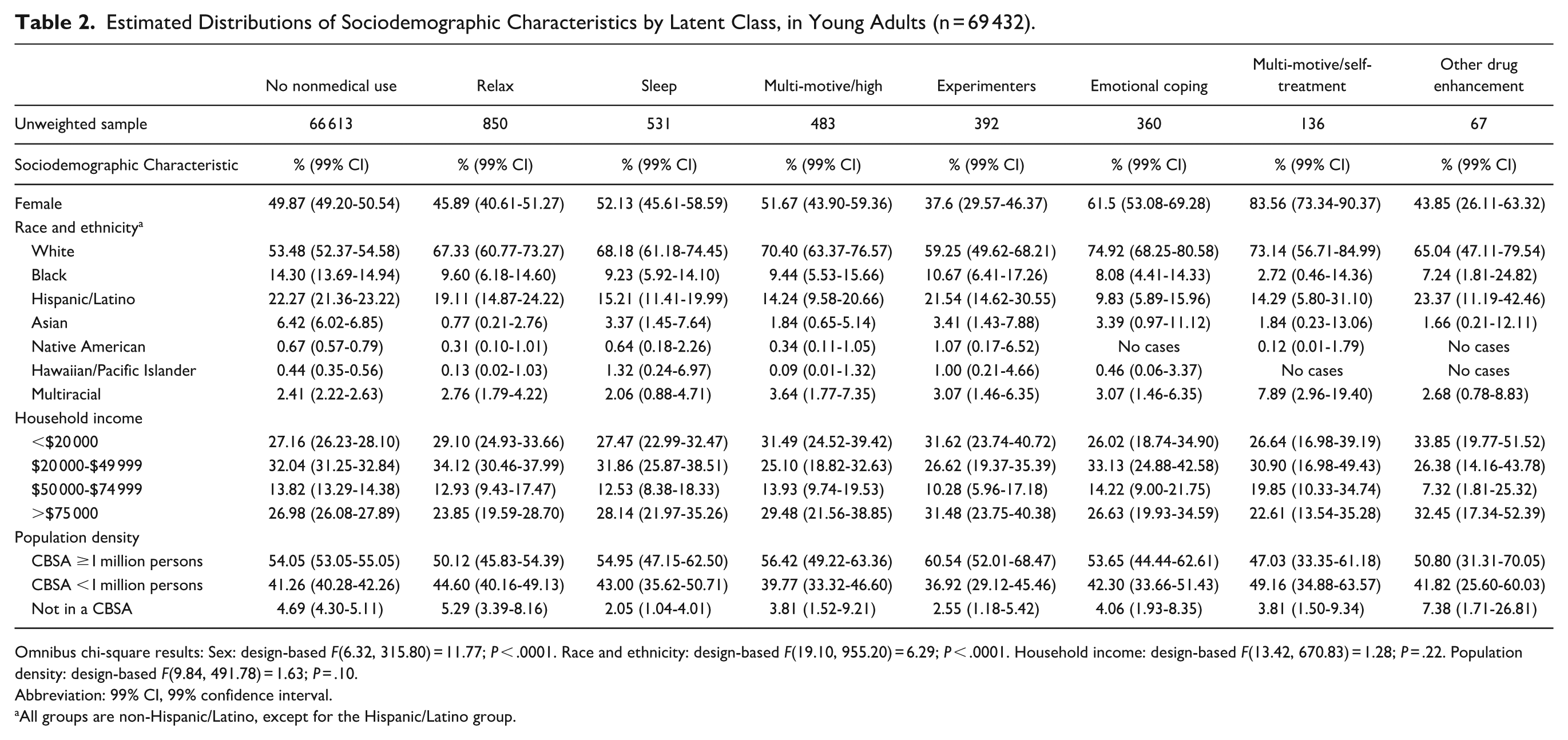
Omnibus chi-square results: Sex: design-based F(6.32, 315.80) = 11.77; P < .0001. Race and ethnicity: design-based F(19.10, 955.20) = 6.29; P < .0001. Household income: design-based F(13.42, 670.83) = 1.28; P = .22. Population density: design-based F(9.84, 491.78) = 1.63; P = .10.
Abbreviation: 99% CI, 99% confidence interval.
All groups are non-Hispanic/Latino, except for the Hispanic/Latino group.
Characteristics of Adolescent Latent Classes
Per Table 3, adolescents with any nonmedical tranquilizer use had significantly higher odds of concurrent other substance use and past-year major depression than those without nonmedical use, with odds ratios well below 1.0 versus the Relax reference group. The Multi-Motive latent class has significantly higher odds of all forms of substance use, except for 30-day binge alcohol use (eg, aOR = 3.05 for past-year nonmedical prescription stimulant use), and past-year major depression (aOR = 2.43) versus the reference Relax class. The other 3 nonmedical tranquilizer use latent classes did not differ significantly from the Relax class on measures of substance use and past-year major depression, and there were few significant sociodemographic differences between groups. When using the BCH method to estimate odds, only 2 significant differences were found: first, past-year nicotine dependence was no longer significantly more common in the Multi-Motive class versus the Relax class; second, past-year major depression was significantly more common in the Emotional Coping than in the Relax class.
Logistic Regression Models of Substance Use, Mental Health, and Sociodemographic Characteristics as a Function of Tranquilizer Misuse Motive Latent Class Membership with the Relax Latent Class as Reference, in Adolescents (n = 67 981).
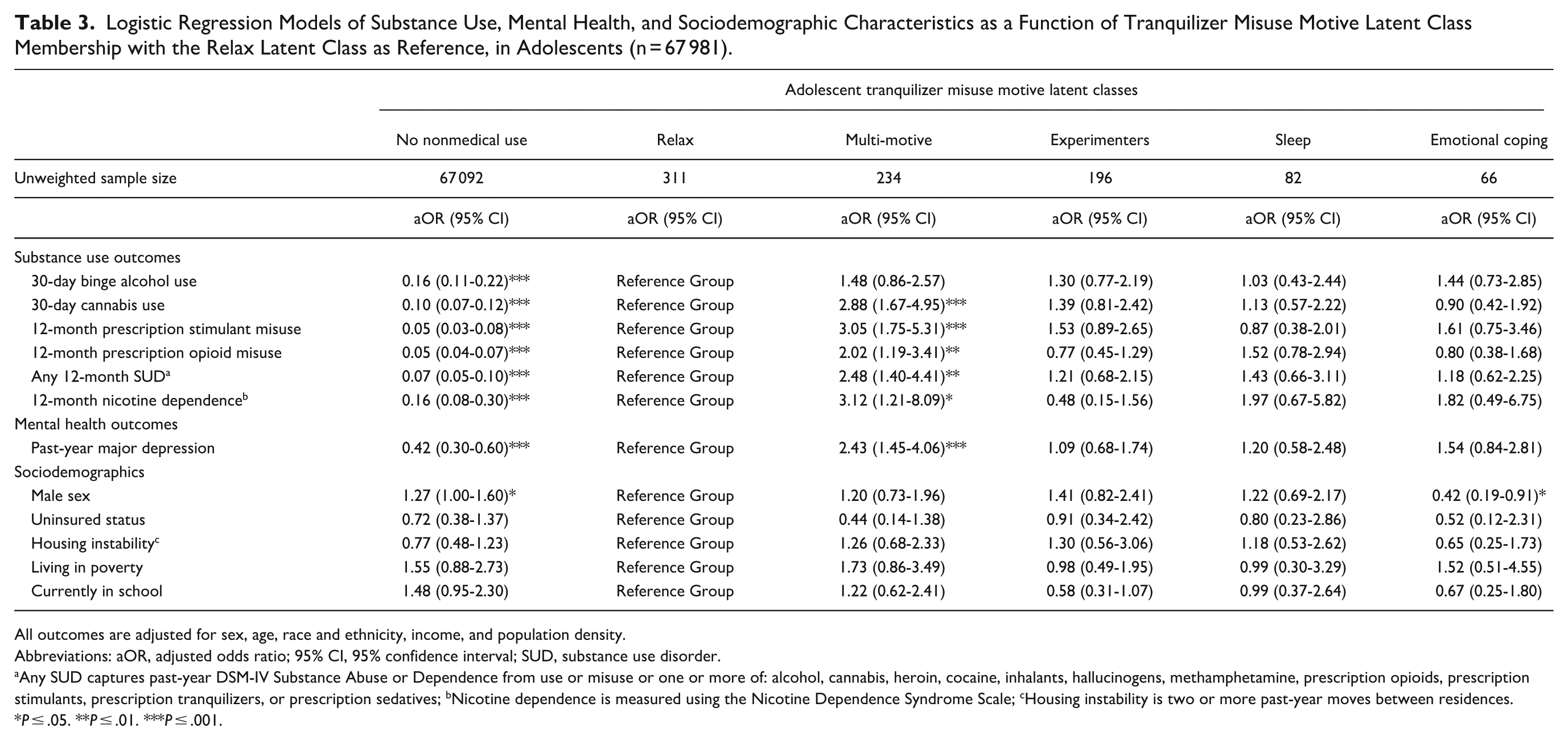
All outcomes are adjusted for sex, age, race and ethnicity, income, and population density.
Abbreviations: aOR, adjusted odds ratio; 95% CI, 95% confidence interval; SUD, substance use disorder.
Any SUD captures past-year DSM-IV Substance Abuse or Dependence from use or misuse or one or more of: alcohol, cannabis, heroin, cocaine, inhalants, hallucinogens, methamphetamine, prescription opioids, prescription stimulants, prescription tranquilizers, or prescription sedatives; bNicotine dependence is measured using the Nicotine Dependence Syndrome Scale; cHousing instability is two or more past-year moves between residences.
P ≤ .05. **P ≤ .01. ***P ≤ .001.
Characteristics of Young Adult Latent Classes
Similarly, young adults engaged in nonmedical tranquilizer use had significantly elevated odds of all substance use and mental health outcomes versus young adults without past-year nonmedical use, except for past-year nicotine dependence and past-year major depression in the Experimenter latent class (comparison not shown in Table 4). Per Table 4, those in the Experimenter group had significantly lower odds of past-year nonmedical prescription opioid use, nicotine dependence, SPD, and suicidal ideation but slightly higher odds of past-year nonmedical prescription stimulant use versus the Relax class. On the other hand, the Multi-motive/High class had significantly higher odds of all substance use and mental health outcomes than the Relax class, except for 30-day binge alcohol use. The Emotional Coping/Relax and Multi-Motive/Self-Treatment classes had significantly higher odds of all mental health concerns than the Relax latent class (aOR range = 1.89-3.35), without significant substance use differences. Finally, there were only very limited differences between the Relax and either the Sleep or Other Drug Enhancement classes. As with adolescents, only 2 significant changes were found when using the BCH method, both for male sex: males were no longer less common in the Sleep versus the Relax class but became more common in the Experimenter than in the Relax class.
Logistic Regression Models of Substance Use, Mental Health, and Sociodemographic Characteristics as a Function of Tranquilizer Misuse Motive Latent Class Membership with the Relax Latent Class as Reference, in Young Adults (n = 69 432).
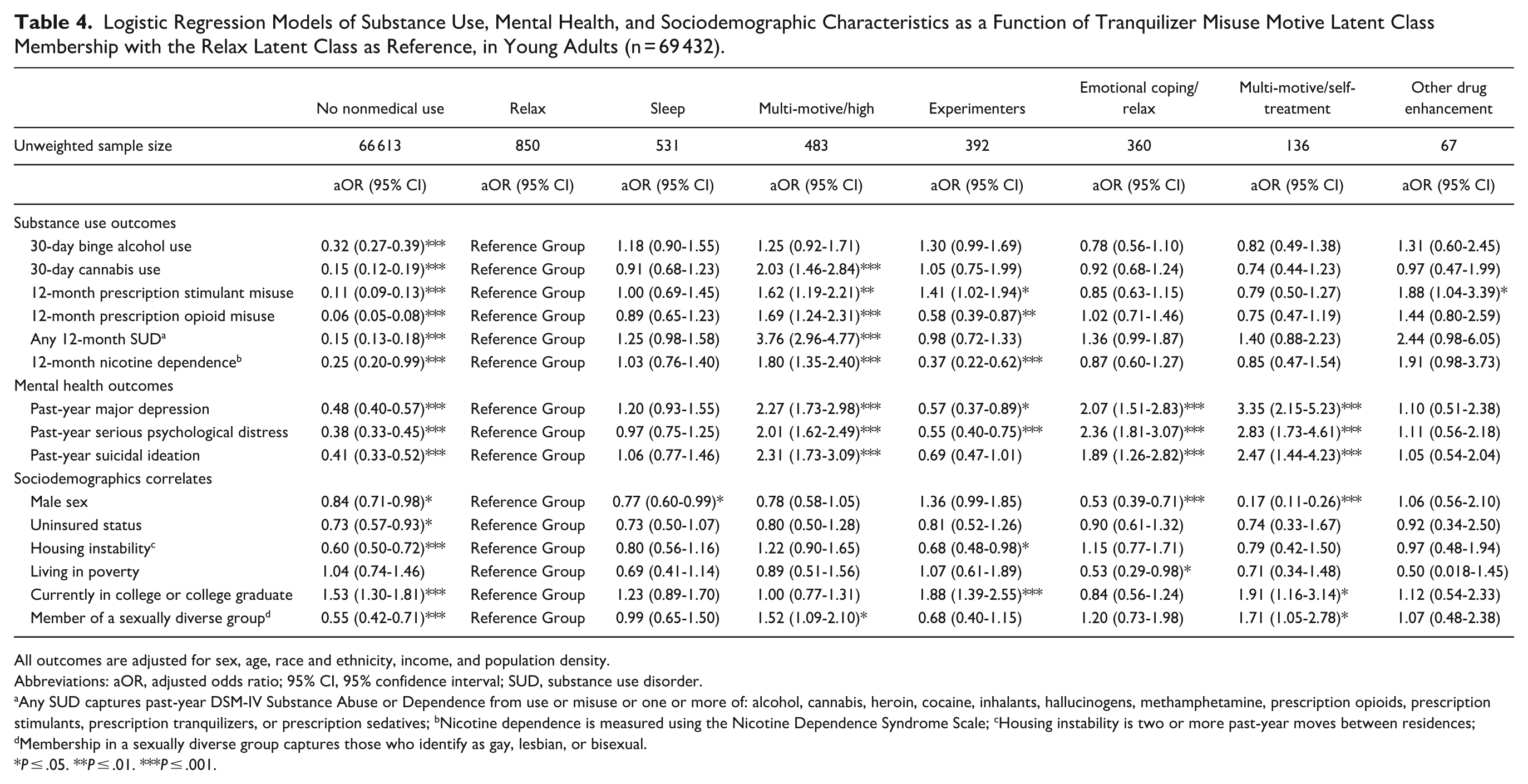
All outcomes are adjusted for sex, age, race and ethnicity, income, and population density.
Abbreviations: aOR, adjusted odds ratio; 95% CI, 95% confidence interval; SUD, substance use disorder.
Any SUD captures past-year DSM-IV Substance Abuse or Dependence from use or misuse or one or more of: alcohol, cannabis, heroin, cocaine, inhalants, hallucinogens, methamphetamine, prescription opioids, prescription stimulants, prescription tranquilizers, or prescription sedatives; bNicotine dependence is measured using the Nicotine Dependence Syndrome Scale; cHousing instability is two or more past-year moves between residences; dMembership in a sexually diverse group captures those who identify as gay, lesbian, or bisexual.
P ≤ .05. **P ≤ .01. ***P ≤ .001.
Discussion
Our results indicated that there are 5 and 7 latent classes of adolescents and young adults, respectively, engaged in past-year nonmedical prescription tranquilizer use based on the motives for such nonmedical use. Notably, McCabe and Cranford 36 also found 5 latent classes of adolescents based on nonmedical tranquilizer use motives, with broadly similar classes. This research expands on that by adding young adults and finding both similarities and differences between the adolescent and young adult latent classes that may point to different profiles and processes by age group. Both age groups had a Relax latent class that was the largest by prevalence (>30%), and both had Sleep, Experimenter, and Emotional Coping latent classes.
Nonetheless, the differences between adolescents and young adults are notable and suggest that these age groups should be considered separately when possible. While these age groups shared Sleep and Experimenter classes, the young adult sleep class was over twice as large (18.8%, vs 9.2% in adolescents), while the Experimenter class was nearly halved (13.9% in young adults vs 22.0% in adolescents). Moreover, the single Multi-motive class in adolescents (26.3%) was split into 2 Multi-motive classes in young adults, with 1 (17.1%) marked by very frequent endorsement of “to get high” and the other marked by (4.8%) self-treatment motives (ie, “to relax,” “to sleep”). Given the cross-sectional nature of the NSDUH, this research cannot identify whether these differences are based on unique characteristics of the samples, age differences, and/or cohort effects. Future research should examine within-person longitudinal changes in nonmedical prescription use motives and other processes (eg, sources) from adolescence into adulthood.
In both age groups, any nonmedical prescription tranquilizer use, regardless of motive profile, was linked to a higher prevalence of other substance use, SUD, and mental health concerns, with very limited exceptions, versus the Experimenter group in young adults. This mirrors prior research highlighting nonmedical tranquilizer use as a higher-risk behavior.1,3 Within those engaged in nonmedical use, another consistent finding was that membership in a Multi-motive class with frequent endorsement of “to get high” signaled the greatest levels of substance use engagement and mental health concerns, similar to prior research on nonmedical prescription opioid use. 26 While no clear differences existed between the remaining adolescent latent classes (ie, Relax, Sleep, Experimenter, and Emotional Coping), young adults had a pair of latent classes in the Emotional Coping and Multi-motive/Self-treatment classes with elevated odds of mental health concerns versus the Relax latent class. The Relax, Sleep, and Other Drug Enhancement latent classes were similar in young adults, but the small sample size of the Other Drug Enhancement class, the nearly significant ORs for past-year non-nicotine SUD and nicotine dependence (vs the Relax class), and the highest endorsement of any class of “because I am hooked” suggest that this class may warrant further study with a larger sample.
Clinically speaking, these results first highlight that any engagement in nonmedical tranquilizer use signals an elevated likelihood of concurrent other substance use and mental health concerns, versus adolescents and young adults not engaged in nonmedical use. Ongoing monitoring of medication adherence in adolescents and young adults prescribed these medications is needed, along with counseling about the risks of nonmedical use to both the prescribed young person and parents/caregivers. Furthermore, adolescents and young adults in the Multi-motive and Multi-motive/High classes (respectively) need identification via screening and significant intervention to address their high levels of substance use and mental health concerns. Finally, attention to mental health symptoms is needed in young adults who endorse nonmedical use to help cope with emotions, particularly when combined with sleep and anxiety concerns.
Limitations
Many limitations of this study result from the secondary analysis of cross-sectional survey data. First, causality cannot be inferred due to the cross-sectional nature of the data. Second, both self-report and selection biases may be present. Despite concerns about these biases, the evidence strongly indicates that self-report substance use data are valid, 37 and the use of ACASI methods, medication pictures, and trade and generic medication names in the NSDUH nonmedical tranquilizer use assessment promoted accurate and valid reporting of nonmedical use and motives.18-22 Another limitation is that the data on motives for nonmedical tranquilizer use only captured the most recent nonmedical use episode, which obscures both within-person change in motives over time and the possibility that individuals may have engaged in nonmedical use for a broader set of motives than would be captured in a single episode. Finally, the Emotional Coping and Sleep latent classes in adolescents and the Other Drug Enhancement class in young adults had relatively small sizes, ranging from 66 to 82. These smaller latent classes may have resulted in unstable estimated regression coefficients, and given the wide confidence intervals noted for many estimated regression coefficients, results involving these latent classes should be interpreted with caution. Replication of these class structures with other data would better establish the validity of these smaller classes.
Conclusions
Our results suggest 5 adolescent and 7 young adult latent classes of nonmedical tranquilizer use motives. While 4 classes were similar between these age groups, the sizes of these classes sometimes differed by age group, and young adults had more multi-motive classes. Longitudinal research is needed to better characterize whether and how within-person motives change into adulthood. In both adolescents and young adults, members of multi-motive classes marked by frequent endorsement of “to get high” had the highest levels of concurrent other substance use and psychopathology symptoms, highlighting a need to identify and intervene with these individuals. Finally, any nonmedical tranquilizer use was linked to higher odds of other substance use, SUD, and mental health concerns, reiterating the high-risk nature of such nonmedical use.
Supplemental Material
sj-docx-1-saj-10.1177_29767342251370827 – Supplemental material for Latent Classes of Nonmedical Prescription Tranquilizer Use Motives in US Adolescents and Young Adults
Supplemental material, sj-docx-1-saj-10.1177_29767342251370827 for Latent Classes of Nonmedical Prescription Tranquilizer Use Motives in US Adolescents and Young Adults by Ty S. Schepis, Philip T. Veliz, Brady T. West, Jason A. Ford and Sean Esteban McCabe in Substance Use & Addiction Journal
Footnotes
Data Availability Statement
Author Contributions
TSS: Conceptualization, Data Curation, Formal Analysis, Funding Acquisition, Methodology, Software, Writing – Original Draft, Writing – Review & Editing. BTW: Conceptualization, Methodology, Writing – Review & Editing. PTV: Conceptualization, Funding Acquisition, Methodology. JAF: Conceptualization, Writing – Review & Editing. SEM: Conceptualization, Funding Acquisition, Writing – Review & Editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The NSDUH is funded by the Substance Abuse and Mental Health Services Administration (SAMHSA), and this work was supported by the National Institutes of Health, grant numbers R01DA043691, R01DA031160, R01CA276500, and P50DA05403901. Dr. Schepis was also supported by a faculty fellowship from the Texas State University Translational Health Research Center. None of the funders had any role in this study’s design, the collection, analysis, or interpretation of data, the writing of the report, or the decision to submit the paper for publication.
Compliance,Ethical Standards,and Ethical Approval
The Research Triangle Institute IRB approved the National Survey on Drug Use and Health (NSDUH), and the first author’s IRB exempted this research from further oversight (IRB #7143).
Informed Consent Statement
Informed consent was obtained from all participants, and all NSDUH procedures were consistent with the Declaration of Helsinki ethical principles and the Belmont Report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.