
Abstract
Background:
Lifesaving medications for opioid use disorder (MOUD) exist; however, most people with opioid use disorder (OUD) do not receive treatment. Hospitalization is one important opportunity to engage people with OUD and offer treatment, including MOUD. Between 2018 and 2020, 6 public hospitals in New York City launched the “Consult for Addiction Treatment and Care in Hospitals” (CATCH) program to provide interprofessional addiction consult services to hospitalized patients.
Methods:
This qualitative study aims to add perspectives from 30 racially and ethnically diverse people with opioid-related diagnoses who were hospitalized at a CATCH hospital between October 2019 and April 2021. We used purposive sampling to recruit demographically diverse individuals who accepted or declined aspects of CATCH services. Interviews were audio-recorded, transcribed, and coded for emergent themes using grounded theory techniques. The framework of structural vulnerability was utilized to highlight how social context impacts patients’ experiences of healthcare, and in turn affects their addiction trajectories.
Results:
Participants overwhelmingly accepted MOUD to manage withdrawal symptoms during hospitalization, and many planned to continue MOUD after discharge. Participants appreciated the interprofessional support of CATCH teams which included medical providers, social workers, addiction counselors, and peers. While participants felt that CATCH made holistic addiction treatment including MOUD more accessible, structural issues created barriers to continuing treatment long term. Some participants still felt stigmatized or “punished” for their drug use by non-CATCH providers.
Conclusion:
CATCH met an urgent need for nonjudgmental care and medical management of opioid withdrawal. Additional interventions that address broader needs, including housing and social supports, as well as trust-building healthcare encounters for patients who have been historically marginalized, are needed to meet the public health goal of preventing overdose and reducing drug-related morbidity for this population.
Highlights
Thirty hospitalized people with opioid use disorders were interviewed about their experiences with an addiction consult service—the “Consult for Addiction Treatment and Care in Hospitals” (CATCH) program.
Participants described experiences of withdrawal management and connection to treatment.
Participants declined aspects of CATCH due to housing, transportation, insurance, program barriers.
Comparing prior hospitalizations to CATCH, participants felt improved trust and advocacy.
Introduction
Opioid-related overdose deaths in the United States remain high, exceeding 80 000 in 2023. 1 Opioid use disorder (OUD) can be treated with highly effective medications for OUD (MOUD). However, most people with OUD do not receive MOUD.2,3 MOUD treatment rates are lower among racial and ethnic minoritized groups who also experience disproportionately high rates of overdose death.4-6
Hospitalization is one important opportunity to engage people with OUD and offer treatment and harm reduction services, including MOUD. 7 People with OUD are hospitalized at high rates 8 and have an elevated risk of mortality postdischarge. 9 During hospitalization, people with OUD are often undertreated for opioid withdrawal and receive inadequate pain management, resulting in more patient-directed discharges and fewer linkages to treatment.10-12 Despite efforts to improve utilization of MOUD, 13 many hospital providers lack addiction training and experience.14,15
Hospital addiction consult services (ACSs) are increasingly being implemented across the United States to fill gaps in addiction care for hospitalized patients.16-20 ACSs increase quality of care, provide withdrawal and pain management, and link patients to postdischarge treatment.16,17,19 Patients who use substances report less judgmental and more humanizing interactions with the ACS compared with other hospital providers, and have a better understanding of MOUD after ACS engagement.11,21-25 ACSs also benefit hospital providers, who report feeling inadequately prepared to treat addiction. 10
NYC Health and Hospitals (H + H), a large public hospital system in New York City (NYC), 26 launched an interprofessional ACS—the “Consult for Addiction Treatment and Care in Hospitals” (CATCH) program—at 6 hospitals between 2018 and 2020. CATCH teams, compromised of medical providers, social workers, addiction counselors, and peer counselors, provide treatment recommendations (including MOUD), counseling, harm reduction education and resources, and linkage to treatment. H + H serves a diverse group of patients, many of whom are low-income and from racial and ethnic minoritized groups. 26 CATCH hospitals are located in 4 NYC boroughs (Bronx, Manhattan, Brooklyn, and Queens) and provide care to communities living in some of the highest-risk areas for overdose in NYC.26,27 These communities have distinct local histories pertaining to substance use, violence, housing, and access to healthcare that shape individuals’ risk environment.26,28
This qualitative study, part of a pragmatic trial of the effectiveness of CATCH for increasing postdischarge initiation and engagement in MOUD, 29 aims to add perspectives from a demographically diverse group of people with opioid-related diagnoses hospitalized at CATCH hospitals. We employ the theoretical framework of structural vulnerability 30 to describe and contextualize major factors impacting patients in the community and during hospitalization; to investigate the impact of the CATCH program on individuals; and to understand benefits and barriers to care faced by patients with opioid-related diagnoses when interacting with the healthcare system. Structural vulnerability refers to an individual or group’s risk for negative health outcomes through their interface with socioeconomic, political, and cultural hierarchies.30,31 People are understood to be structurally vulnerable when their “location in society’s mutually reinforcing power hierarchies (socioeconomic, racial, cultural) and institutional and policy-level statuses (eg, immigration status, labor force participation) constrain their ability to access healthcare and pursue healthy lifestyles.” 30
Rather than focusing only on the clinical encounter, which risks universalizing patient experiences,32,33 this study included interview questions about the context of peoples’ lives, inquiring into their initial exposures to drug use and their broader social context outside of the hospitalization. Previous studies have explored patient experiences in the context of an ACS; however, most were conducted in areas with lower rates of poverty than the communities served by the CATCH hospitals, and with a majority of White participants.21-25,34 We add to the literature on patient perspectives by considering how structural vulnerabilities affect patients’ experiences with an ACS and focusing on the overlapping vulnerabilities that shape healthcare experiences.
Methods
This study is reported following the COnsolidated criteria for REporting Qualitative Research checklist 35 (see Supplemental Material).
Sample and Recruitment
To identify potentially eligible participants for qualitative interviews, CATCH staff informed the research team of hospital patients who had a CATCH consult ordered and an opioid-related diagnosis. CATCH staff provided potentially eligible participants with a flyer describing the study. Interviewers approached potential participants face-to-face and explained the research study objectives and recruitment process. Purposeful sampling was used to recruit individuals with varying demographics (age, race, ethnicity, and gender) and to include at least 1 patient at each hospital who declined some aspects of CATCH services (eg, MOUD, post-discharge follow-up). We sought to include participants who declined CATCH in order to understand how the program could be improved more broadly. Eligible patients were (1) 18 years or older; (2) hospitalized with a diagnosis of OUD and/or opioid-related poisoning; (3) able to provide informed consent; (4) had sufficient English fluency. Participants provided written informed consent prior to the interview. The Institutional Review Board at NYU Grossman School of Medicine approved this study.
Data Collection
A semistructured interview guide (see Supplemental Material) was developed as part of the larger pragmatic CATCH trial 29 and was broadly informed by the Consolidated Framework for Implementation Research (CFIR). 36 The guide focused on the “inner setting” domain of CFIR, and specifically on the patient experience of medical care and OUD treatment. It additionally asked about an individual’s background and substance use history to contextualize and provide a deeper understanding of their responses. The guide was revised in 2020 to include questions related to COVID-19.
Two trained interviewers (J.F., L.T.) conducted semistructured interviews from October 2019 to April 2021 using the semistructured interview guide. At the time of this study, J.F. was a research associate and L.T. was a medical student and anthropology graduate student volunteering on the study. Both women were trained in conducting interviews and had several years of experience working in qualitative research. Interviews were conducted privately, in-person during hospitalization, except for one which was conducted privately at the hospital’s outpatient clinic after discharge. Interviews were audio-recorded and lasted between 13 and 94 minutes; participants were compensated $50. Race, ethnicity, and gender were self-reported. Interviews were transcribed and de-identified for analysis.
Data Analysis
Data were analyzed using a grounded theory approach, aiming to gain a robust understanding not only of whether CATCH was helpful, but why/why not, and how it was experienced. 37 Three coders (C.K., L.T., Y.R.-A.) independently coded transcripts using NVivo software (Lumivero, version 12). 38 Coders completed line-by-line coding, inductively using 3 initial transcripts to generate a shared codebook, meeting frequently to discuss concepts’ meanings and engage in case comparison. Subsequent transcripts were coded with frequent meetings to reach inter-coder reliability and resolve coding discrepancies through discussion. Temporality, structural vulnerability, and the COVID-19 pandemic were sensitizing concepts used as interpretive devices to organize analysis of themes after the initial codebook was generated. 39 Codes and themes were revised until new data did not require new codes and no new themes were identified, indicating theoretical saturation. Ultimately, themes related to COVID-19 did not achieve saturation and were not included in this manuscript, while the other 2 sensitizing concepts formed the conceptual framework.
Results
Most participants were men (n = 22, 73.3%) with an average age of 46.4 years (range: 23-63; Table 1). Participants self-identified as non-Hispanic Black (n = 5, 16.7%), non-Hispanic White (n = 7, 23.3%), Hispanic (n = 13, 43.3%), or Hispanic in combination with another race (n = 5, 16.7%). A majority (n = 21, 70.0%) had a high school education or lower. Nine participants (30.0%) refused some aspect of CATCH services, as determined by CATCH teams.
Participant Characteristics.
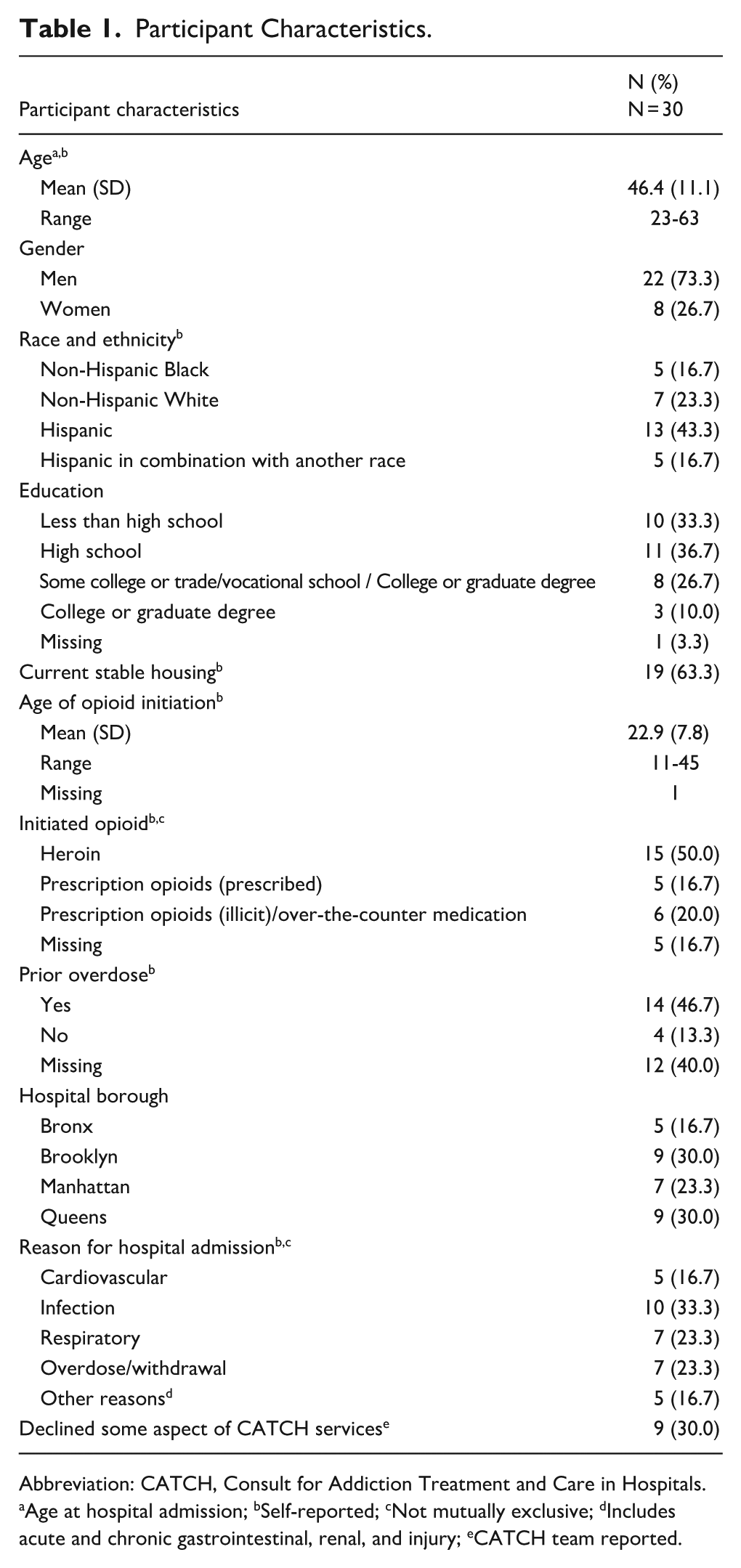
Abbreviation: CATCH, Consult for Addiction Treatment and Care in Hospitals.
Age at hospital admission;
Self-reported;
Not mutually exclusive;
Includes acute and chronic gastrointestinal, renal, and injury;
CATCH team reported.
Within the dominant framework of structural vulnerability which emerged from the data, data were organized across 2 organizing themes: (1) how structural vulnerabilities shaped trajectories of drug use and experiences with healthcare; (2) how CATCH facilitated engagement and treatment for patients experiencing structural vulnerabilities. Subthemes emerged within each theme as described below. Subthemes reinforced the concept of structural vulnerability, describing how power hierarchies both within and outside of healthcare systems constrain access to healthcare and shape people’s life chances.
How Structural Vulnerabilities Shaped Trajectories of Drug Use and Experiences With Healthcare
Participants described histories of structural vulnerability, including early exposure to drug use (often from loved ones), food and financial insecurity, periods of homelessness, exposure to physical and sexual violence, incarceration, previous drug overdose events, multiple prior hospitalizations, and multiple co-morbidities in addition to OUD. These vulnerabilities, coupled with discrimination in healthcare and treatment burdens, shaped drug use and reinforced barriers to healthcare and OUD treatment.
Violence and Trauma Driving Opioid Use and Limiting Treatment
Many participants described exposure to violence and trauma as a reason for initiating or continuing their drug use. One participant described returning to opioid use after witnessing the murder of his brother in front of their apartment building. Another participant stated, “I had some trauma, and because of trauma, I do heroin, and it makes me forget about it” (P14).
One participant described physical trauma (gunshot wound) as a reason they became dependent on prescription opioids, and later transitioned to using street opioids after losing access to their medications: “I tried to get them refilled so many times, and the doctor said, well, you don’t need it. So, then if I woulda continued persisting, it was gonna raise red flags that I had a problem. So, that’s why I had to stop that and go to the street” (P18).
Housing Precarity Multiplying Risks
For many participants, unstable housing was associated with continued opioid use and limited access to healthcare. One participant explained using heroin as a means of coping with the struggles of being unhoused: “The other time I relapsed, I was homeless, and I was sleeping outside. The first night, I was outside, and it was freezing outside. It was too cold to sleep. And then, as soon as the morning came, I had $20 in my pocket. I don’t have a sleeping bag. I don’t have shit. Like, I can’t do this. So, I just went and used. And, immediately, it’s just an intense relief, and, you know, I’m able to go do what I need to go do to survive” (P12).
Another participant described his fear that a hospital admission might compromise his space at the shelter: “I’ve been in the shelter for a year now. I was afraid that when I came [to the hospital], I was gonna lose my bed, and I wouldn’t have nowhere to live. And I didn’t wanna live in the street. ‘Cause I lived in the street before, you know? It’s not easy, especially in the wintertime, you know?” (P21).
Loneliness and Abandonment Exacerbating Drug Use
Participants expressed feelings of loneliness and abandonment that were often a driver of substance use. One participant explained, “I just feel so lonely. I feel depressed. You know? I feel alone like abandoned, like everybody abandoned me. Once they get everything they need from me, they just abandon me. So I think that makes me run backwards. I start going backwards. Once I start feeling like that, I go backwards and I pick up [relapse]” (P2).
Another stated, “If you’re alone, you’re not gonna really—if you’re alone and you don’t try to do nothin’, you’re not gonna get clean.” (P25).
Barriers From Treatment Burdens and Punitive Care
Experiences such as discrimination in healthcare, inaccessible programs, and insurance lapses create additional obstacles to engaging in or remaining in treatment. Several participants voiced a view that some healthcare providers are punitive toward patients who use opioids. One participant said: “They make you feel bad. One minute it could be all, I’m tryin’ to help you,’ and the minute you say, ‘I’m on methadone,’ they treat you differently. You can’t stay still because your joints are hurtin’ so much that no matter where you turn, you can’t get satisfaction. And I know doctors know. But I guess they do it to make you feel guilty. They figure, they got themselves into it, let them feel it for a little while, and it might make them want to stay clean” (P22).
For participants who had previously accessed OUD treatment, treatment burdens and insurance lapses limited their desire for future engagement and retention. One participant said regarding a methadone program: “Sometimes there could be, like, you know, 50 people in line waiting, or sometimes your counselor wants to see you, and you’d be stuck there for a half hour, an hour, and then you’d be late to work. It’s very, very difficult, going there every single day” (P10).
Transportation and accessibility were also barriers: “I mean I didn’t have no money to travel all over the place. It was too far for me to go up there” (P15). Another participant was told she would have to go to a methadone clinic for treatment, which she felt was inaccessible: “I’m not gonna do that because I’m in a situation where I’m in a wheelchair. What if it rained? I’m not gonna wanna go there” (P9).
Insurance lapses led to abrupt discontinuation of medications. For example, 1 participant discussed a prior experience with a program stopping methadone treatment because of an insurance issue: “They were supposed to wean me down, and, because my credentials weren’t working, they just said, ‘We can’t medicate you no more because you have no means of payment.’ I was like, ‘Yeah, but you can’t just kick me out like that’” (P22).
Participants’ experiences of housing instability, social isolation, violence, and trauma shaped how they used opioids and engaged with healthcare, underscoring their potential unmet needs during hospitalization. Past negative experiences with healthcare, including punitive care and treatment burdens, created additional barriers to initiating or maintaining treatment.
How CATCH Facilitated Engagement and Treatment for Patients Experiencing Structural Vulnerabilities
Most participants described positive interactions with the CATCH team during hospitalization, including adequate and timely access to withdrawal management and more humanizing care, compared with past hospital experiences. Participants emphasized that the CATCH team acted as their advocate by engaging with the primary medical team, local treatment programs, and pharmacies on their behalf.
Acute Withdrawal as Priority
Participants overwhelmingly felt that the CATCH team met their needs for inpatient withdrawal management. Participants compared prior hospital admissions to explain that inpatient management of opioid withdrawal was crucial and had previously been poorly managed. One participant described making plans to self-treat his withdrawal either with diverted MOUD or illicit opioids when he anticipated a possible hospitalization, which he now no longer needed to manage alone. Another stated, “[CATCH doctor] met my needs 100 percent. I told him exactly what I needed, and he was like, ‘That’s what we do. We can get you started on [MOUD]’” (P10).
When asked about MOUD, many participants described the benefits of initiating during their hospitalization, but emphasized the importance of receiving withdrawal management before they could fully engage in conversation about treatment after discharge. Some declined treatment referrals at least temporarily, citing withdrawal symptoms: “They [CATCH team staff] were askin’ me if I wanted to go into a program. I was a little down. I didn’t wanna answer that question. I didn’t get any methadone yet. I wasn’t feelin’ good” (P25). These instances of declining care highlighted the need to manage acute withdrawal symptoms adequately, which often built trust in addition to providing relief, prior to attempting referrals.
Connection and Consistent Humanization
Participants gave examples of CATCH teams providing additional supports that they had not received during prior hospitalizations. One participant explained that his experience with the CATCH counselors changed his perspective on presenting to the hospital, which he had delayed in the past: “I came in for chest pain, right? But before I came here, I was thinking, if I go into the hospital with chest pain, what am I gonna do about my addiction problem? They’re not gonna give me anything. . . . So that’s why I delay so many times coming here. But when I did come to the hospital, and I saw them here, I realized, ‘Oh, they got these counselors here that come and work with you.’ I felt better” (P26).
Another participant, who had been treated by the CATCH team during multiple hospital admissions, said: “I never met such a team that works together. You know what? They’re beautiful. They work with me at any given time. They never give up on me. Never, never, never, never have they ever given up, you know” (P16). Another remarked, “They put in effort. In other places, they don’t. So it’s nice to have people that actually cared” (P20). Here, participants emphasized that team-based collaboration, tenacity, consistent availability, and effortful care were crucial aspects of CATCH that facilitated engagement with services.
Many participants described the CATCH team advocating for them. When participants felt that their primary team was planning to discharge them from the hospital too quickly, members of the CATCH team advocated on their behalf. One participant stated, “[CATCH medical provider] broke his neck for me. He will literally respectfully argue with these doctors, . . . He’d fight. [CATCH medical provider] fights for his clients” (P17).
CATCH Eases Postdischarge Treatment Barriers
Participants varied in how they imagined their care after hospital discharge. For some, MOUD served as short-term withdrawal management only. Others planned to continue MOUD long term after receiving it during hospitalization: “I’m not gettin’ off the methadone. That’s a wrap” (P7).
Participants emphasized that housing, transportation, and insurance-related barriers after discharge made easy access to inpatient care and outpatient follow-up important: “The convenience of everything definitely increased the chances of my success” (P10). This participant further explained that starting MOUD during hospitalization made it possible to imagine engaging in ongoing treatment. “It mighta not worked out as well as this if I had the time to get released from here and then had to wait another week to go to this other thing, ‘cause, what am I gonna do in that week if I was active? You know, it could get complicated” (P10).
One participant explained that a CATCH medical provider went with him to the outpatient treatment program and advocated for his admission postdischarge: “Really, she saved my life, and she gave me this chance. I tried so many times, and they turned me down. I was thinking, ‘Oh, my god, lady. You don’t know.’ [Laughter] But I said, ‘It’s okay. Let’s try again. What bad can happen?’ But I don’t know what she told them, but I guess she told them I was desperate, really desperate, so I was lucky. They accepted me” (P14).
Despite CATCH relieving some barriers to treatment, past experiences with insurance and outpatient program requirements were difficult to overcome and made some participants reluctant to initiate MOUD while in the hospital. In some cases, this limited the ability of CATCH teams to establish postdischarge treatment plans that were acceptable and feasible. For example, 1 participant explained that he could not receive buprenorphine from his preferred outpatient substance use treatment program until he resolved a Medicaid restriction that was placed on his insurance. After several social workers consulted together on his case, he was told he needed to go in person to the main Medicaid office (more than 1.5 hours away by train) to speak with someone about removing the restriction. While he had been interested in attending the outpatient program, he did not want to go into opioid withdrawal: “Because I ain’t got no buprenorphine in my body, I’m not going to go there and sit sick” (P5). The insurance restriction altered what the CATCH team could offer; ultimately, he accepted a short-term methadone taper during hospitalization.
Other Hospital Providers “Punishing.”
While CATCH was generally seen as improving the hospital experience, some participants still reported feeling stigmatized and/or “punished” for their drug use by other healthcare providers during hospitalization. These negative experiences, despite the presence of CATCH, continued to shape participants’ receptivity to healthcare, including MOUD.
For example, 1 participant reported feeling punished by the primary medical team because he left the hospital for an hour to get money and identification: “But the doctor punished me. He said no because I stepped out for a minute and came right back, I didn’t use. I’m supposed to still be getting [the same dose of buprenorphine], and you’re going to bring me back down and make me suffer.” The next day, when offered buprenorphine, he decided against taking it. “I said, ‘You had to give it to me when I needed it yesterday. Take it and shove it’” (P1).
Discussion
These interviews illustrate the complex needs of hospitalized people with OUD. Many participants described violence, trauma, and social isolation coupled with unstable housing and medical co-morbidities impacting their opioid use. Structural vulnerabilities and past negative experiences with healthcare shaped their access to and experiences with MOUD before, during, and after hospitalization. With CATCH, participants described more supportive hospital experiences with providers who were knowledgeable advocates providing urgently needed MOUD for withdrawal management.
Participants emphasized the importance of consistently supportive care that reshaped their trust and expectations of healthcare. These findings further recent insights into how ACSs can have long-lasting effects on patients’ trust in healthcare systems.21,22,25 Distressing interactions with medical teams that feel punitive or stigmatizing can erode engagement in care well beyond a single encounter.40,41 Participants declined some aspect of CATCH if they felt their acute withdrawal was not yet adequately managed or if they perceived that a healthcare provider was attempting to “punish” them in some way. In contrast, participants who described humanizing and supportive interactions with CATCH staff members described a downstream impact to this kind of support, particularly when it was felt repeatedly, as when providers “never, never, never” gave up on them. Receiving consistently nonjudgmental and compassionate care from ACS staff provides a mechanism to build trust during inpatient hospitalizations, and such interactions increased participants’ willingness to engage in longer-term care.21,22,25 Within the hospital’s hierarchy, ACSs are well-positioned to address discrimination and stigma toward patients with OUD through advocacy, education, and hospital policy change.21,22,25
Structural vulnerabilities limit one’s ability to access healthcare and achieve health 30 and such constraints were deeply felt by participants. Current and past experiences of structural vulnerabilities shaped participants’ perceptions of OUD treatment outside of the hospital and were a major barrier to engagement. While CATCH made MOUD more accessible in the hospital, participants anticipated structural issues (eg, methadone access, transportation, insurance) that would remain barriers to treatment after discharge. Some participants declined aspects of CATCH services, usually citing barriers to care outside the hospital, either experienced in the past or anticipated for the future, that shaped the care they wanted inside the hospital. Patients have previously described perceiving treatment without access to their basic needs as “futile.” 11 While CATCH teams included social workers and peers, overcoming negative perceptions of past treatment experiences and the realities of housing unaffordability, transportation, and insurance restrictions were often insurmountable to address during a limited hospital stay. In addition to structural-level changes to methadone access, insurance, and housing availability, interventions that build patient rapport and address social concerns after hospitalization could improve health outcomes for patients with OUD.42,43
Most participants in this study were from racial and ethnic minoritized groups and described histories of criminalization and social abandonment related to substance use that were consistent with well-documented impacts of structural racism. Premature death rates rose sharply in NYC in 2020, and were highest for men, Black individuals, and people living in neighborhoods with higher poverty. 44 Rates of fatal overdose among Black populations overtook overdose rates among White populations during the period of this study, 45 and racial and ethnic disparities in buprenorphine access persist despite improvement efforts.5,46 Past experiences of provider stigma, discrimination, and mistrust in healthcare, driven by structural racism, result in racial and ethnic minoritized patients being less likely to seek or receive addiction services, including ACS consults, inpatient MOUD, and postdischarge MOUD treatment.47,48 Continuing to develop an in-depth understanding of what constitutes a reparative and trust-building healthcare encounter from the perspectives of racialized patients is an important step toward achieving equity in MOUD treatment and reducing overdose rates.
Limitations
The results of this study represent the experiences of hospitalized patients with OUD from 6 NYC public hospitals that implemented CATCH. The sample was limited to participants with opioid-related diagnoses that may not reflect the experiences of those who use other substances. We attempted to recruit a diverse group of participants; however, the majority were men. While this reflects the hospital’s population of OUD patients, the needs of women and gender-diverse people need to be explored, as do experiences of non-English speaking patients. Federal restrictions on MOUD were relaxed during the course of this study. Since implementation of the policy changes have varied across time and location, participants’ experiences with OUD treatment may differ from those under the current policies. Participants were recruited during their hospital stay, limiting their ability to fully discuss their transition to postdischarge SUD treatment. Finally, participants may have perceived interviewers as part of the CATCH team or as healthcare representatives and responded more positively than they would have otherwise.
Conclusions
CATCH services met an urgent need for humanistic care and medical management of opioid withdrawal for hospitalized patients. Structural vulnerabilities continue to shape experiences with healthcare and access to MOUD treatment. Additional services and interventions that address broader needs, including housing and social supports, as well as trust-building healthcare encounters for patients who have been historically marginalized, are needed to meet the public health goal of preventing overdose and reducing drug-related morbidity for this population.
Supplemental Material
sj-pdf-1-saj-10.1177_29767342251392696 – Supplemental material for “They Never, Never, Never Give Up on Me”: Perspectives on an Addiction Consult Service From Hospitalized People Who Use Opioids at 6 New York City Public Hospitals
Supplemental material, sj-pdf-1-saj-10.1177_29767342251392696 for “They Never, Never, Never Give Up on Me”: Perspectives on an Addiction Consult Service From Hospitalized People Who Use Opioids at 6 New York City Public Hospitals by Lauren Textor, Carla King, Yasna Rostam-Abadi, Jasmine Fernando, Noa Appleton, Amanda M. Bunting, Adetayo Fawole, Charles Barron, Daniel Schatz and Jennifer McNeely in Substance Use & Addiction Journal
Supplemental Material
sj-pdf-2-saj-10.1177_29767342251392696 – Supplemental material for “They Never, Never, Never Give Up on Me”: Perspectives on an Addiction Consult Service From Hospitalized People Who Use Opioids at 6 New York City Public Hospitals
Supplemental material, sj-pdf-2-saj-10.1177_29767342251392696 for “They Never, Never, Never Give Up on Me”: Perspectives on an Addiction Consult Service From Hospitalized People Who Use Opioids at 6 New York City Public Hospitals by Lauren Textor, Carla King, Yasna Rostam-Abadi, Jasmine Fernando, Noa Appleton, Amanda M. Bunting, Adetayo Fawole, Charles Barron, Daniel Schatz and Jennifer McNeely in Substance Use & Addiction Journal
Footnotes
Acknowledgements
The authors would like to thank study participants and hospital staff who made this study possible. We would also like to thank NYC Health and Hospitals’ Office of Behavioral Health, who are instrumental in developing and sustaining the CATCH program, including Omar Fattal, Marc Manseau, Lynsey Avalone, and Kayna Pfeiffer.
Author Contributions
All authors contributed to conceptualization and design of the study. LT and JF collected the data. LT, CK, and YR-A conducted the formal analysis and wrote the original draft. All authors were involved in data interpretation and in reviewing and editing the manuscript.
ORCID iDs
Ethical Considerations
The Institutional Review Board at NYU Grossman School of Medicine approved this study.
Consent to Participate
Written informed consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by NIDA grant R01DA045669 with additional support from NCATS grant UL1TR001445 and NIH T32 GM008042.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.