
Abstract
Background:
Substance use in the perinatal period is a critical public health issue in the United States. Nurses play a significant role in promoting positive maternal-infant health outcomes for women who use substances in the perinatal period. However, many nurses have deficient knowledge, skills, and attitudes (KSAs) toward perinatal substance use (PSU), which can impede their ability to care for this population. Deficiencies in KSAs should be addressed during nursing school; however, few studies have described nursing students’ KSAs related to PSU. Understanding nursing students’ KSAs about PSU can inform the development of educational interventions to increase KSAs and improve outcomes for women with perinatal substance use and their infants. The purpose of this study was to describe the KSAs nursing students have toward PSU.
Methods:
This study used a mixed-methods approach. A sample of 46 undergraduate nursing students from 2 Midwestern universities was recruited to participate in an online survey. Of those nursing students, 16 completed interviews. Survey data were triangulated with interview themes to produce a deeper understanding of nursing students’ KSAs related to PSU.
Results:
Survey and interview data highlighted 4 themes which were related to KSAs of nursing students, including: (1) limited knowledge of PSU; (2) varied confidence in clinical skills; (3) biased attitudes toward PSU; and (4) recommendations for nursing education.
Conclusion:
The findings indicated that nursing students have limited knowledge, moderate levels of stigma, and varied skill sets when caring for women with PSU and their infants. Nursing curricula should consider including broader coverage of PSU using various and effective educational strategies (ie, simulation; AI) which incorporate the lived experiences of women with PSU.
Highlights
Nursing students report limited knowledge of perinatal substance use (PSU).
Nursing students hold stigma toward PSU.
Nursing students have varied skills related to PSU.
Background
Perinatal substance use (PSU) in the United States negatively impacts maternal-child health outcomes. The World Health Organization (WHO) (2025) defines the perinatal period as the time from 22 completed weeks of gestation through the end of 7 completed days after birth. 1 Substance use during pregnancy has been associated with a 50% increased risk for severe maternal morbidity compared to women who did not use substances. 2 Women with PSU are at greater risk for severe maternal morbidity events such as acute myocardial infarction and aneurysm. 3 Perinatal substance use has been associated with an increased risk for adverse birth outcomes compared to those without PSU. 4 In addition, PSU is a leading contributor to maternal mortality in the United States, accounting for 11.4% of pregnancy-associated deaths in 33 states between 2010 and 2019. 5 Rates of overdose among pregnant and postpartum women have increased 2 to 3-fold from 2017 to 2021 in the United States.6,7
The increasing rates of PSU have also adversely affected infant health outcomes. Rates of neonatal abstinence syndrome (NAS), a cluster of infant withdrawal symptoms from prenatal opioid exposure and other substances, have increased significantly from 4.0 to 7.3 per 1000 birth hospitalizations between 2010 and 2017 in 47 states and the District of Columbia. 8 Infants exposed to PSU (eg, alcohol, cannabis, opioids, stimulants, and tobacco) tended to have higher rates of preterm birth, low birth weight, admissions to the neonatal intensive care unit, and birth defects.9,10
Nurses make up the largest health care profession and provide education, labor and delivery support, postpartum recovery support, and breastfeeding assistance to women in the perinatal period. 11 However, nurses have reported lacking knowledge about PSU (eg, opioid use) and having the skills to adequately care for the women. 12 Studies have found that nurses often hold stigmatizing views and biased opinions toward women, which can interfere with quality perinatal care, women participating in recovery efforts, and engaging with their infants.13,14 For example, women with PSU have reported overhearing nurses who referred to them by offensive names, challenged their breastfeeding attempts, and treated them differently from women who do not use substances.14,15 Nurses have also expressed negative opinions about women with PSU and the need for more knowledge and skills to care for this population.13,14,16,17
Nursing students also provide direct care to women with PSU and have reported lacking knowledge and skills to adequately care, as well as being challenged with judgmental attitudes.18-20 In a study by Schuler and Horowitz, 20 nursing students’ attitudes toward PSU improved significantly in all practice settings except maternal-child health. Thus, a mentorship practicum alone may not address the unique educational challenges nursing students face when working with women with PSU and their infants. A gap in the literature exists to understand nursing students’ knowledge, skills, and attitudes (KSAs) toward PSU. The purpose of this study was to describe nursing students’ KSAs toward PSU. The findings can inform future development of tailored educational strategies aimed at improving the KSAs of future nurses to improve care of women with PSU and their infants.
This study was guided by Bloom’s KSAs taxonomy. 21 Knowledge refers to the facts and concepts learned and retained. Skills refer to abilities related to performing a task. Attitudes refer to feelings, emotions, beliefs, and values. Knowledge, skills, and attitudes are interrelated and thus influence each other. For example, nurses must have the necessary knowledge about PSU to provide evidence-based care. Further, knowledge about PSU and recovery trajectories can improve attitudes toward this marginalized population. 22
Methods
Design
A mixed-methods approach was used to allow for a comprehensive understanding of nursing students’ KSAs. Survey and interview data were collected.
Interview
We used a qualitative descriptive design to assess the KSAs of nursing students related to PSU. Qualitative description is a pragmatic research approach to describe health care or nursing-related phenomena.23,24 A qualitative descriptive approach produces straight descriptions with low interference from the researcher rather than focusing on culture or building theory as in other qualitative methods (eg, grounded theory and phenomenology).23,25
Survey
We used a cross-sectional design and survey methods to measure the KSAs of nursing students toward PSU.
Setting and Sample
We recruited nursing students from 2 large Midwestern nursing schools. Students were eligible if they: (1) were 18 years of age or older; (2) were currently enrolled in an undergraduate nursing program; (3) had completed their maternal-child course; and (4) could write and speak in English.
Instruments
Interview
Semi-structured interviews were conducted using an interview guide (Supplemental Appendix A) where questions were mapped to the 3 domains of Bloom’s KSAs taxonomy. 21
Survey
We administered the Modified Attitudes About Drug Use in Pregnancy Scale (MAADUP), 13 a single-factor measurement, to quantify nursing students’ attitudes toward PSU. Participants rate their agreement with each of the 13 items using a 1 (strongly agree) to 5 (strongly disagree) response scale. The total score is the mean across all items. Higher scores indicate more positive attitudes, while lower scores indicate more negative attitudes. Scores less than 3 reflect identified stigmatizing attitudes, and scores less than 2 suggest heightened stigmatizing attitudes. The MAADUP 13 has demonstrated validity and reliability among nursing samples.
We also administered the Person Centered- Drug and Drug Problems Perception Questionnaire (PC-DDPPQ) 26 which is a 20-item measure with a 5-factor structure with the 5 subscales: Role adequacy (having sufficient knowledge to perform the professional role), Role legitimacy (extent to which a provider may regard substance-use related care as part of their work responsibilities), Role support (providers perception related to the availability of support and advice), Role-related self-esteem (confidence in their ability to provide care for individuals who use substances), and Job satisfaction (experiencing satisfaction when working with individuals who use substances). 26 The PC-DDPPQ 26 uses a 5-point Likert scale, ranging from 1 “strongly disagree” to 5 “strongly agree.” The total score is the mean score across all 20 items, and subscale scores are the mean scores for items loading on each subscale, respectively. The investigative team mapped PC-DDPPQ 26 items to KSAs.
Demographic information collected in the survey included: (1) Age; (2) Race; (3) Ethnicity; (4) Gender Identity; (5) Marital Status; and (6) Level in Current Nursing Program (ie, junior, senior).
Study Procedures
This study received Institutional Review Board (IRB) approval at the authors’ institutions. We recruited a purposive sample of eligible nursing students from 2 Midwestern universities through email. The recruitment email provided study information and a QR code for an enrollment survey (using Qualtrics) that contained an informed consent document and an eligibility validation checklist. After consenting electronically, participants completed the M-AADUP scale, PC-DDPPQ, and demographic items. Those completing the survey had the option to provide their name, email address, and phone number to participate in an interview. The research team then contacted those who provided their contact information to set up a time for a virtual or phone interview. All participants were assigned a study ID to protect confidentiality, and contact information was deleted after the study was completed. We enrolled participants for interviews on a rolling, first-come basis, and participants were not informed of their individual survey responses. All participants chose to participate in the interview virtually. The interviews were audio-recorded and lasted approximately 30 to 45 minutes. Participants were informed that the term “substance use” broadly refers to all substances (eg, alcohol, illicit substances, and opioids). Participants were asked specifically about experiences related to perinatal substance use disorders (SUD) versus PSU in the interviews because PSU is not always readily identified in clinical settings. Focusing on PSU was used to help students focus on identified cases instead of conjecture. Participants were then asked questions related to PSU and perinatal SUD that were mapped to Bloom’s KSAs taxonomy. 21 Interviews were conducted by a trained research assistant or investigator at each university. Interview participants received a $15 gift card as compensation for their time.
Data Management and Analysis
Interview
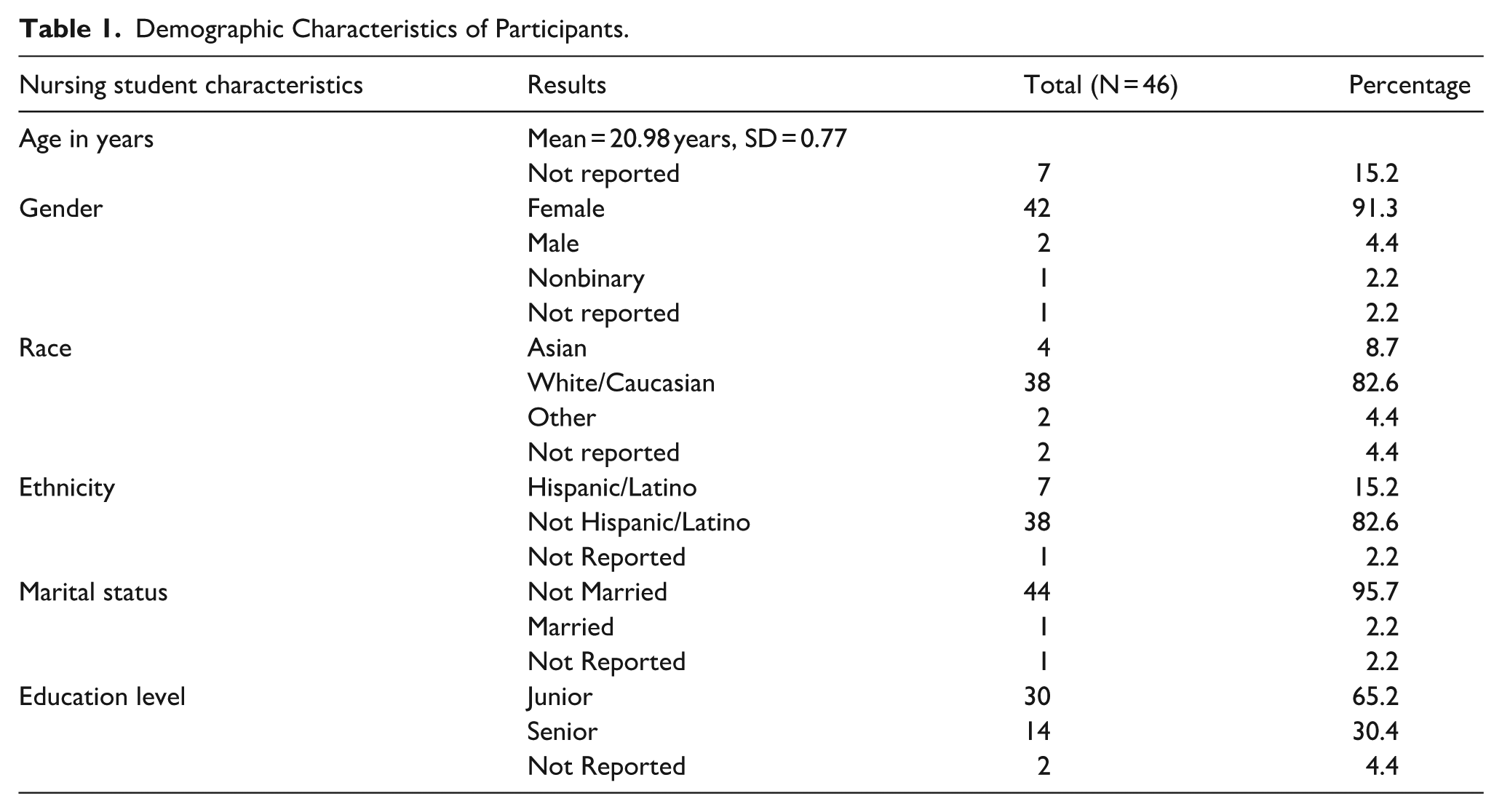
The audio-recorded interviews were transcribed using an IRB-approved transcriptionist and stored in a shared file that was only accessible to the research team. All participant information was de-identified and labeled with a study identification number. Qualitative data analysis was conducted using an inductive content analysis approach guided by 3 steps from Kyngas, 27 which include data reduction, data grouping, and the formation of concepts that can answer the research question. The researchers highlighted and extracted each text unit and assigned a code to each text unit. The research team then discussed and analyzed the open codes for similarities and differences to group the codes to form themes and subthemes. Themes were organized into 3 main domains: Knowledge, Skills, and Attitudes. To enhance trustworthiness, the research team was immersed in the data and discussed emerging analytic ideas. The researchers maintained an audit trail. A detailed description of the sample is provided in Table 1 to enhance the transferability of the findings to other contexts.
Demographic Characteristics of Participants.
Survey
Survey responses were exported from Qualtrics as a CSV file, cleaned in Excel, and analyzed in R Studio (version 2022.07.1). 28 Descriptive statistics described aggregate responses to each item and the total scale score. The 5 subscales from the PC-DDPPQ were mapped to the domains of the KSAs framework (Table 3). 21 The domains were inferred based on the definitions of each subscale described by Mahmoud et al. 26 The MADUUP (Table 4) was used to measure attitudes. Survey findings were triangulated with interview themes to provide a more comprehensive understanding of nursing students’ KSAs toward PSU. Findings between survey and interview data were compared to identify similarities, differences, and patterns between the data sources.
Results
A total of 46 participants completed the survey. Of the total number of participants (N = 46), a subset of 16 participants completed the interviews. Demographic characteristics can be found in Table 1.
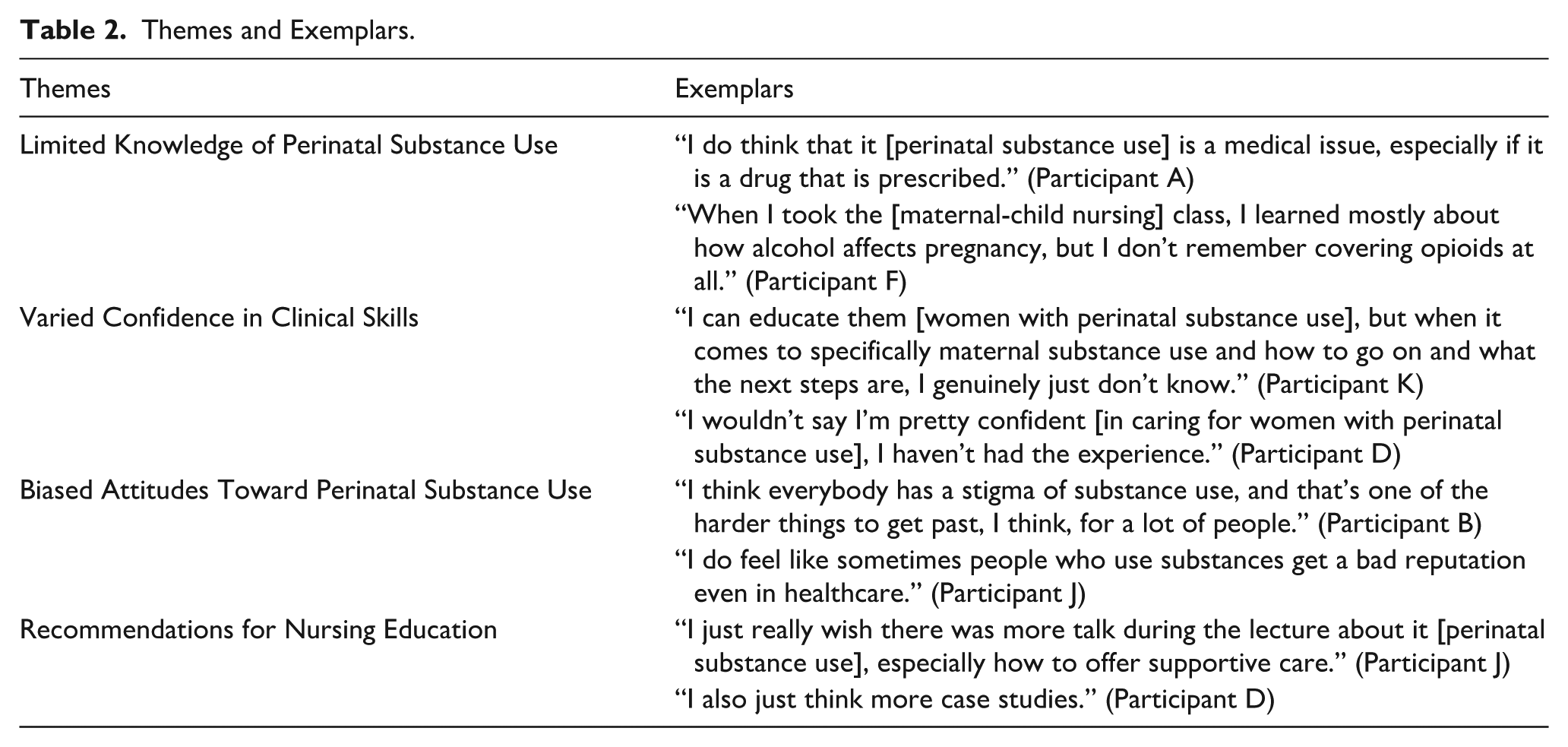
We identified 4 themes: (1) Limited Knowledge of PSU; (2) Varied Confidence in Clinical Skills; (3) Biased Attitudes Toward PSU; and (4) Recommendations for Nursing Education. Themes and exemplary quotes can be found in Table 2.
Themes and Exemplars.
Limited Knowledge of PSU
Participants described having limited knowledge about PSU and desired to better understand the condition. Most participants viewed PSU as a medical condition and reported having some knowledge on topics including the effects of certain substances (ie, alcohol, opioids) during pregnancy, signs and symptoms of substance use, and NAS. However, participants believed they lacked knowledge on the topic and that it was not adequately covered during didactic or clinical. One participant (Participant M) stated, “We got a brief introduction [to PSU] . . .like 15 minutes.” Another participant stated (Participant A), “We didn’t really talk about that [PSU] in clinical at all.” Survey results aligned with interview participants’ statements.
The results of the PC-DDPPQ (Table 3) demonstrated that participants were knowledgeable in some aspects of PSU, but there was room for improvement as seen through the Role Adequacy Scale (M = 3.47; SD = 0.59). Participants perceived themselves to be more knowledgeable regarding the psychological effects of using substances. Most participants (81%) reported feeling like they know enough about the psychological effects of drug use to carry out their role when working with individuals who use drugs (scores >4 on PC-DDPPQ; item 4; Table 3). However, aligned with interview data, students reported limited knowledge on how to communicate with women with PSU. More than half of participants (54%) reported limited knowledge on how to counsel individuals who use drugs (scores <3 on PC-DDPPQ; item 6; Table 3). Nearly 1 in 4 participants reported limited knowledge in advising patients about drug use (score <3 on PC-DDPPQ; item 7; Table 3).
Descriptive Statistics of Total and Subscale Scores of the PC-DDPPQ 26 Mapped to KSAs (N = 46).
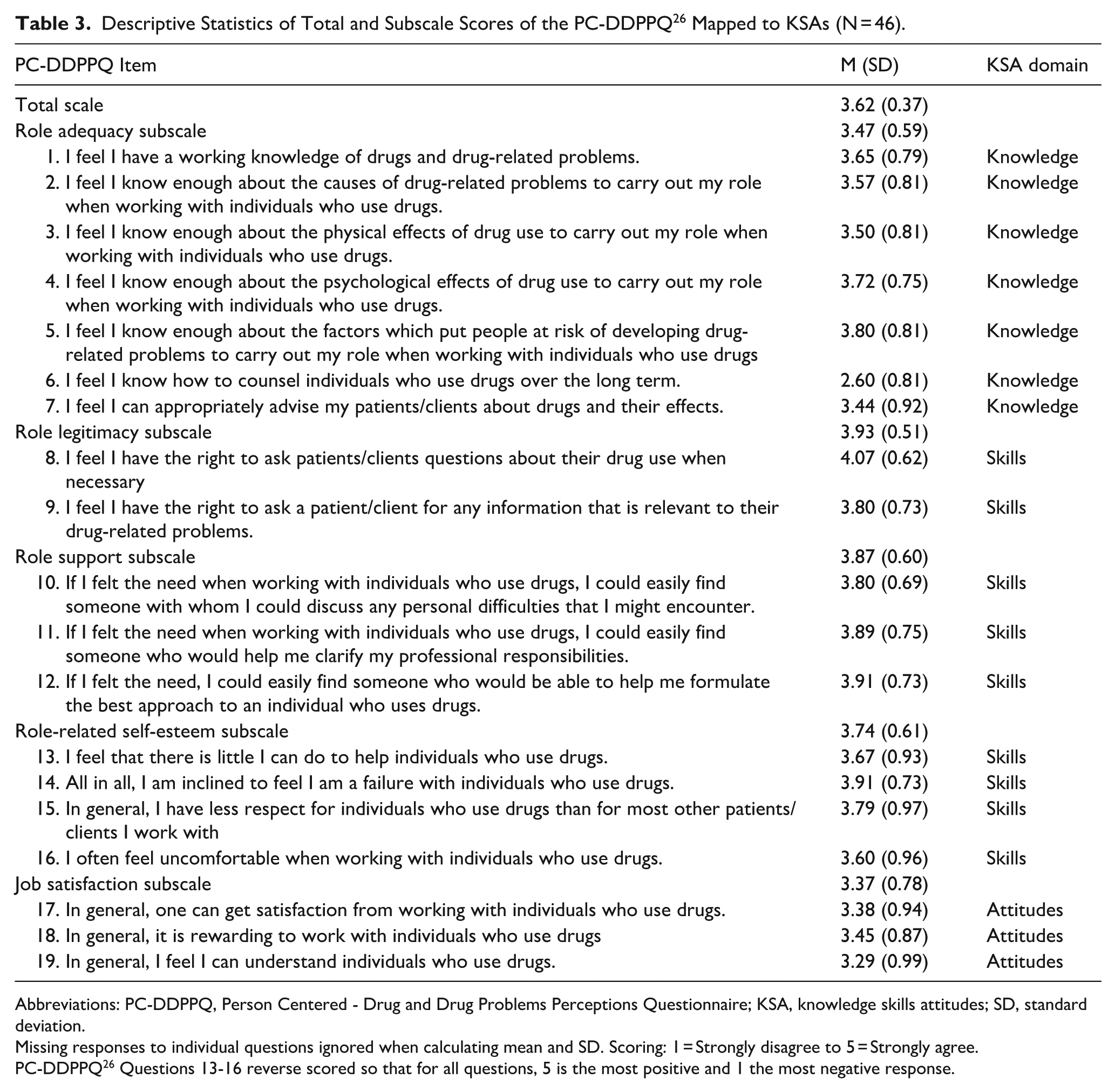
Abbreviations: PC-DDPPQ, Person Centered - Drug and Drug Problems Perceptions Questionnaire; KSA, knowledge skills attitudes; SD, standard deviation.
Missing responses to individual questions ignored when calculating mean and SD. Scoring: 1 = Strongly disagree to 5 = Strongly agree.
PC-DDPPQ 26 Questions 13-16 reverse scored so that for all questions, 5 is the most positive and 1 the most negative response.
Varied Confidence in Clinical Skills
Participants reported varied confidence levels in clinical skills when working with women with PSU and their infants. One participant stated (Participant A), “I felt confident about being able to assess neonates and look for signs [of NAS].” Another participant (Participant G) believed she could improve her confidence through self-directed learning and stated, “I know myself that if I do some of the self-teaching for myself, if I can review some of my notes, and if I can do my own kind of personal research, that I’ll feel pretty confident.” Other participants described not feeling confident and not feeling prepared. A participant (Participant A) stated, “I don’t think I could do it [provide care for women with PSU and their infants] alone.” Another participant (Participant H) stated, “I feel like if I was offered that assignment [to care for women with PSU and their infants], I would probably need a lot of guidance from my [precepting] nurse.” Participants identified that nurses play a major role in providing education to affected women and encouraging them on their recovery trajectory. However, participants lacked the skills to communicate therapeutically with the women. A participant (Participant K) questioned, “How do I actually talk to this woman?”
The results of the Role Self-esteem (M = 3.74; SD = 0.61), Role Legitimacy (M = 3.93; SD = 0.51), and Role Support (M = 3.87; SD = 0.60) of the PC-DDPPQ (Table 3) demonstrated that participants had overall moderate levels of confidence in their nursing skills when caring for this population. The results of the subscales varied, with the lowest scoring item being related to how uncomfortable participants felt when working with individuals who use drugs (M = 3.60; SD = 0.96; item 16; Table 3). The highest scoring item was related to participants feeling they had the ability to ask individuals about their substance use 4.07 (0.62).
Biased Attitudes Toward PSU
Participants discussed their own attitudes and the perceived attitudes of peers toward PSU. Participants recognized that they often struggle with their own stigma. Although participants reported that education related to stigma and its relationship with patient care was provided in their respective nursing curricula, they struggled to apply this knowledge to effectively reduce their own stigma toward women affected by PSU.
Participants provided examples of how stigma may emerge and negatively affect patient care and outcomes. One participant (Participant A) stated that some women are not “fit parents or guardians for their child,” emphasizing their concern for vulnerable infants and lack of confidence in women’s abilities to care for their infants. Regarding maternal care for an infant, the participant went on to state that, “There’s going to be some situations where the mom needs to go for longer periods, rehab, and maybe she’s not a fit caregiver and she’s not going to have access to her child for a little bit, and the child needs to be in foster care, or go to a supportive relative.” Further, they noted that variation in stigma among interdisciplinary care teams adversely affects patients, even if they, as students or nurses, have limited or no stigmatizing attitudes or behaviors toward PSU. One participant (Participant A) stated, “Obviously medical professionals want the best for [the patient], but not all of them emphasize that through compassion.”
The results of the MAADUP scale (N = 46) (Table 4) demonstrated moderate stigma toward individuals with PSU (M = 3.11; SD = 0.63). Roughly half of the participants (50%) had higher levels of stigma (mean scores <3; Table 4). Greater levels of stigma were noted for perceptions regarding drug and alcohol use as forms of child abuse (item 3 alcohol use: M = 2.48; SD = 1.01; item 4 use: M = 2.41; SD = 1.07). Despite participant concerns related to maternal involvement in infant care noted in the interviews, survey participants reported more positive attitudes (ie, less stigma) toward facilitating maternal involvement in holding infants (item 10: M = 3.91; SD = 0.72).
MAADUP Student Nurse Scores (N = 46).
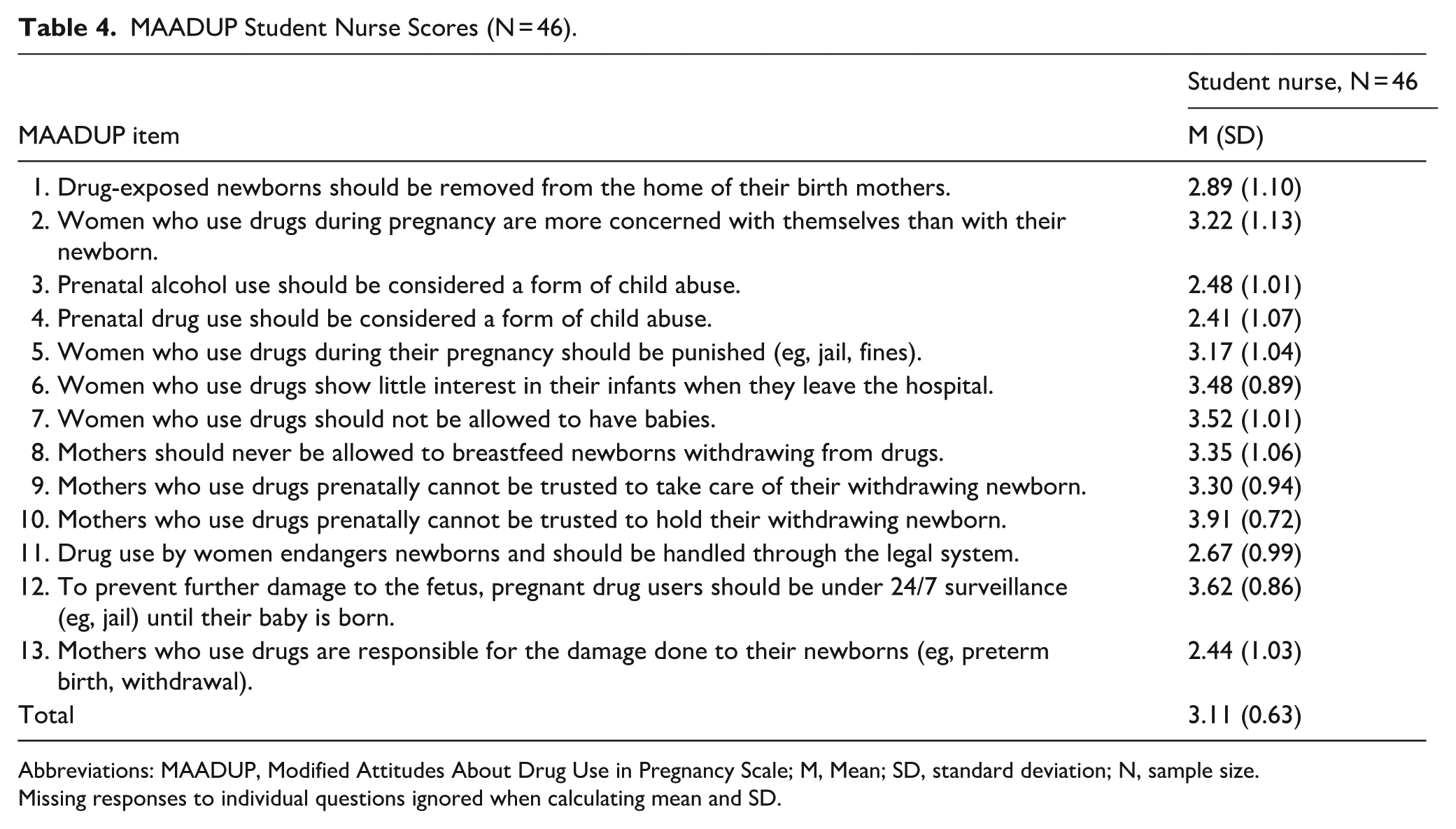
Abbreviations: MAADUP, Modified Attitudes About Drug Use in Pregnancy Scale; M, Mean; SD, standard deviation; N, sample size.
Missing responses to individual questions ignored when calculating mean and SD.
Recommendations for Nursing Education
Participants suggested that more lecture content, case studies, and clinical experiences at PSU would be helpful. One participant (Participant I) stated, “I think focusing part of that lecture on substance abuse disorder and pregnancy would be helpful.” To increase skills, participants (Participant L) desired more exposure and suggested that they would be assigned “easier” patients. Another participant (Participant K) stated, “I don’t know that I was exposed to a patient who was using [substances]. Clinical instructors should seek out those opportunities [for students]. It helps it [knowledge] click better.” Participants recommended that more time and practice should be spent on therapeutic communication. One participant suggested (Participant A), “I think learning how to give them open-ended questions and provide them with and be able to give adequate answers and having practice would be really beneficial.” Many participants suggested that simulation would be beneficial to improve attitudes toward women with PSU. Participants were particularly interested in the use of standardized patients and virtual reality. One participant (Participant O) stated, “simulations are a great way to address the gray and tough areas.”
Discussion
Nursing students expressed having some knowledge related to signs and symptoms of substance use, but desired more education on the topic. The desire for additional education and clinical training related to PSU mirrors findings from other studies.19,20 The lack of general knowledge regarding substance use treatment found in this study aligns with the findings of other studies,18,19 which highlights the importance of including content on recovery trajectories in nursing curricula. It is important to note that nursing students in a prior study viewed PSU as a choice, whereas in the current interview data, PSU was viewed more as a medical condition. 18 This could suggest that nursing students have a better understanding of the science of addiction, indicating progress in this aspect of nursing education.
Nursing students reported varied confidence in their clinical skills related to PSU. This resonates with prior research where many nursing students reported feeling uncomfortable and lacking adequate skills when working with this population, while others felt more comfortable with time and experience.19,20 Some nursing students in the current study reported not feeling confident in how to communicate with women with PSU. In other studies, nursing students believed they lacked the language and skills to communicate with the women. 19 Nursing students feared that discussion of addiction would appear offensive toward the women and avoided conversations on the topic. 19 Nursing programs are encouraged to provide education on effective communication strategies while also facilitating simulated experiences to develop communication skills.29,30
Nursing students were challenged by their negative beliefs about women with PSU. In other studies, nursing students reported holding negative beliefs and biases against women who used substances in the perinatal period.18,20 The attitudes of nursing students in our study were like those found among practicing perinatal nurses.13,14 This may be due to similarities in educational preparation and/or attitudes that are “passed down” by experienced nurses to new/student nurses through clinical experiences, nurse residency programs, and orientation.18,19 For example, Renbarger et al, 18 discovered that hearing nurse preceptors speak negatively about women with PSU reinforced nursing students’ biased attitudes. The similarities suggest that the issue of stigma toward PSU is a nursing discipline issue, but less stigma from nursing may be irrelevant if interdisciplinary members harbor greater levels of stigma.
Limitations
The sample was from 2 Midwestern universities and generalizations cannot be implied to the whole population. Results may differ by certain demographics (ie, age, gender), but this study was not powered to test these differences. This study focused broadly on PSU and differences between different types of substances (ie, marijuana, opioids), use behavior (ie, disordered, casual), and stage of recovery (ie, in treatment, not in treatment) could not be determined. More studies are needed to identify substance use gaps and areas for curricular improvement that exist. The survey data reported on PSU, while the interview data reported on perinatal SUD. This may limit direct comparability between the 2 sources of data. When administering the PC-DDPPQ, nurses may have been challenged due to their role as mandated reporters, which may have influenced how they responded to some of the items.
Implications
Nursing curricula should consider including broader coverage of PSU. 31 Curricula should incorporate multiple educational strategies to accommodate different learning preferences and activate different areas of the brain to help students retain content and motivate behavior change. 32 Curricula and educational interventions should be aimed at both nursing students and practicing nurses to promote stigma-free perinatal settings. Curricula and educational interventions should be aimed at both nursing students and practicing nurses to promote stigma-free perinatal settings. 33
Nursing faculty should consider incorporating the lived experiences of women with PSU in the curricula. Educational interventions that highlight the lived experiences of individuals with substance use have been shown to make positive changes in attitudes and stigma as well as knowledge.34,35 While prior studies show positive changes in knowledge and attitudes, more research is needed to evaluate the long-term impact.34,35
Simulations related to PSU should be considered for inclusion in nursing curricula. Simulations have been shown to improve the KSAs of students toward individuals who use substances and are increasingly being used in nursing curricula.36,37 Simulation-based learning has been shown to improve nurses’ knowledge and competencies, including their self-confidence, communication skills, and decision making.36,37 More research is needed to develop simulation-based interventions to address the care of women with PSU.
Contact-based education is needed to enhance the learning experiences associated with PSU. Studies are needed to further explore barriers to increasing nursing students’ exposure to PSU and how to overcome those barriers. One potential solution to filling this gap is to explore the use of artificial intelligence (AI) to enhance simulation by offering scenarios. Chatbots can be integrated into nursing education to assist nursing students with challenging conversations they may have with their patients. 38 The use of AI is being integrated into virtual reality and augmented reality to develop immersive virtual simulation experiences. 39 This technology has the potential to simulate settings that are difficult to access in the real world. Nursing students could practice skills in AI-enhanced virtual environments, which are challenging to access in traditional educational and clinical settings. 40
Conclusion
This study described the KSAs of undergraduate nursing students in 2 academic institutions in the Midwest by administering the MAADUP and the PC-DDPPQ alongside qualitative interviews. The findings indicated that nursing students have limited knowledge, moderate levels of stigma, and varied skill sets when caring for women with PSU and their infants. Nursing curricula should consider including broader coverage of PSU using various educational strategies (ie, simulation; AI) which incorporate the lived experiences of women with PSU.
Supplemental Material
sj-docx-1-saj-10.1177_29767342261422047 – Supplemental material for Nursing Students’ Knowledge, Attitudes, and Skills Related to Perinatal Substance Use
Supplemental material, sj-docx-1-saj-10.1177_29767342261422047 for Nursing Students’ Knowledge, Attitudes, and Skills Related to Perinatal Substance Use by Kalyn M. Renbarger, Jeri M. Antilla, Rachel Tiefel, Zachary Hass and Clayton J. Shuman in Substance Use & Addiction Journal
Footnotes
Author Contributions
KMR: Writing—review & editing, Writing—original draft, Visualization, Validation, Software, Resources, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. JMA: Writing—review & editing, Validation, Investigation, Data curation, Formal analysis. RT: Writing—review & editing, Validation, Methodology, Investigation, Formal analysis, Data curation. ZH: Writing—review and editing, Writing—original draft, Validation, Methodology, Data curation. CS: Writing—review & editing, Writing- original draft, Visualization, Resources, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization, Mentoring.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by Sigma Theta Tau Rho Chapter (Research Project Grant). Dr. Clayton J. Shuman is supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under award number K08HD105986.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.