
Abstract
Background:
Stimulant use disorder (StUD), particularly involving cocaine and amphetamines, is associated with significant cognitive impairments that impede recovery and increase relapse risk. Atomoxetine, a selective norepinephrine reuptake inhibitor, has been proposed as a potential treatment given its role in enhancing executive function and its established efficacy in attention-deficit/hyperactivity disorder (ADHD). This systematic review aimed to evaluate the efficacy, cognitive, and mood effects of atomoxetine compared with placebo in individuals with StUD.
Methods:
A comprehensive literature search of PubMed, Cochrane CENTRAL, and Embase databases was conducted to identify randomized controlled trials (RCTs) evaluating atomoxetine for StUD. Eligible studies compared atomoxetine with placebo and assessed outcomes related to cognition (attention and response inhibition), stimulant use or abstinence, mood symptoms, and safety. Data were extracted and synthesized qualitatively due to methodological heterogeneity across studies.
Results:
Nine RCTs met the inclusion criteria. Findings on cognitive outcomes were inconsistent: Some studies reported improvements in attentional bias and inhibitory control, while others showed no significant effects. Atomoxetine did not significantly reduce stimulant use, craving, or sustain abstinence compared with placebo. Limited mood-related benefits were observed, particularly among male participants, although results were variable. Across studies, atomoxetine was well tolerated, with most adverse events mild and transient.
Conclusion:
Despite a compelling neurobiological rationale and evidence of modest cognitive and mood benefits, atomoxetine has not demonstrated consistent efficacy as a monotherapy for StUD. Its favorable safety profile may warrant further investigation in carefully defined populations, such as individuals with comorbid ADHD or in combination with behavioral interventions.
Keywords
Highlights
This systematic review synthesized evidence from 9 randomized controlled trials evaluating atomoxetine for stimulant use disorder (StUD).
Atomoxetine showed inconsistent effects on cognition, with occasional improvements in attentional bias and response inhibition.
No significant reductions in stimulant use, craving, or sustained abstinence were observed compared with those in placebo.
Mood-related benefits appeared in limited subgroups (notably males), but findings were variable.
Atomoxetine demonstrated a favorable safety profile, with adverse events generally mild and transient.
Current evidence does not support atomoxetine as an effective monotherapy for StUD, although further research is warranted in individuals with comorbid attention-deficit/hyperactivity disorder or in combination with behavioral interventions.
Introduction
Stimulant use disorders (StUD), particularly involving cocaine and amphetamine-type stimulants, remain a major global health challenge. Globally, approximately 0.4% of the population uses cocaine and 0.7% uses amphetamine-type stimulants, with dependence affecting 16% and 11% of people who use cocaine and amphetamine, respectively. 1 In 2010, an estimated 6.9 million people were dependent on cocaine and 17.2 million on amphetamines worldwide, with substantial regional variation: Over half of the global burden of amphetamine dependence occurs in Asia, while nearly half of cocaine dependence is concentrated in the Americas. 2 Mortality and morbidity patterns differ by substance; cocaine is more strongly associated with acute cardiovascular complications, whereas methamphetamine carries a greater risk of psychiatric comorbidity, including psychosis, depression, and suicidality.1,3-5 Injection use of stimulants further increases the risk of infectious disease transmission, particularly HIV and hepatitis C.1,6
The overall disease burden of StUD is considerable. According to a report from CDC’s State Unintentional Drug Overdose Reporting System data, drug overdose deaths involving stimulants have increased substantially in the United States since 2011. 7 The number of overdose deaths involving cocaine increased from 4681 in 2011 to 29 449 in 2023, while deaths involving psychostimulants with abuse potential increased from 2266 to 34 855 during the same period. 7 From January 2021 to June 2024, stimulants were involved in 59.0% of all US overdose deaths, with 43.1% co-involving stimulants and opioids and 15.9% involving stimulants without opioid co-involvement. These trends underscore the growing public health impact of StUDs. 7
Despite this burden, there are currently no FDA-approved pharmacological treatments for StUD. Psychosocial interventions, particularly contingency management (CM), represent the standard of care. CM has consistently demonstrated effectiveness in promoting abstinence and treatment engagement, although its long-term impact diminishes after discontinuation. 8 Cognitive-behavioral therapy (CBT), the Community Reinforcement Approach, and the Matrix Model are also recommended as adjunctive approaches, but none has achieved the robust efficacy of CM. 8 Pharmacological interventions, including bupropion, modafinil, topiramate, and prescription stimulants, have been tested in randomized trials, yet systematic reviews conclude that evidence for their effectiveness is limited or inconsistent. Thus, the treatment landscape remains dominated by psychosocial approaches, with a clear need for novel pharmacotherapies. 8
One mechanism central to stimulant addiction is cognitive dysfunction, particularly deficits in attention and inhibitory control. Individuals with StUD demonstrate persistent impairments across multiple domains, including working memory, decision-making, processing speed, and learning efficiency, but deficits in attentional bias and response inhibition are especially pronounced. 9 These impairments correlate with treatment dropout, heightened craving, and increased relapse risk. 9 Neuroimaging studies support a model of prefrontal cortical dysfunction, with hypofrontality and impaired activation in regions such as the anterior cingulate cortex and right middle frontal gyrus during inhibitory control tasks. Such deficits are observed both during early abstinence and after prolonged abstinence, suggesting trait-like features that contribute to chronic relapse vulnerability. 9 Likewise, mood dysregulation is increasingly recognized as an important component of StUD. Acute stimulant exposure enhances dopaminergic transmission within mesocorticolimbic reward pathways, reinforcing drug-taking behavior. With repeated exposure, neuroadaptations within this circuitry are associated with diminished responsiveness to natural rewards and the emergence of negative affective states during withdrawal. Symptoms such as anhedonia, irritability, and dysphoria are therefore linked to craving and relapse vulnerability. 10
Given the centrality of cognitive dysfunction in StUD, noradrenergic modulation has emerged as a potential therapeutic strategy. Atomoxetine, a selective norepinephrine reuptake inhibitor approved for attention-deficit/hyperactivity disorder (ADHD), enhances prefrontal cortical functioning and indirectly increases dopaminergic signaling in the prefrontal cortex. 9 Unlike stimulant medications, it does not directly increase dopamine in reward-related striatal regions, conferring lower abuse potential. 9 Preclinical studies indicate that atomoxetine may reduce stimulant self-administration and relapse-like behaviors, and preliminary human studies suggest possible improvements in response inhibition, decisional impulsivity, and attentional bias to drug cues.11,12 However, evidence across clinical trials remains limited and inconsistent, highlighting the need for a systematic evaluation.
The role of comorbid ADHD further complicates this landscape. ADHD prevalence among stimulant-using populations is estimated at 20% to 30%, 13 and this comorbidity is associated with earlier onset, greater severity, and increased relapse risk. 13 Although stimulant medications remain effective for ADHD in these populations, concerns regarding misuse and diversion are prominent. Atomoxetine, with its lower abuse liability, is often preferred, although its effects on addictive behaviors are less clear. 13 Evidence suggests atomoxetine may improve ADHD symptoms in individuals with comorbid StUD, but its efficacy for reducing stimulant use or craving in those without ADHD remains unproven. 13
In light of these considerations, a systematic review focused specifically on atomoxetine for StUD is warranted. Prior reviews have examined atomoxetine primarily within ADHD populations, with less emphasis on its potential role in addressing the cognitive dysfunction and relapse vulnerability characteristic of StUD.14-17 Accordingly, this review evaluates atomoxetine across 3 prespecified, clinically relevant domains: (i) stimulant use and abstinence as primary indicators of efficacy; (ii) cognitive outcomes as mechanistically relevant intermediate targets; and (iii) mood outcomes, given atomoxetine’s noradrenergic profile and the high prevalence of affective comorbidity in this population.
Methods
Study Design
This systematic review was conducted according to the Cochrane Handbook for Systematic Reviews and Interventions and is reported following the updated Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 18
Search Strategy
We conducted a comprehensive search of PubMed/MEDLINE, Cochrane CENTRAL, and Embase databases from inception to May 2025. The search strategy included combinations of the following terms: (“atomoxetine” OR “selective norepinephrine reuptake inhibitor”) AND (“cocaine use disorder” OR “amphetamine use disorder” OR “stimulant use disorder”) AND (“attention” OR “response inhibition” OR “executive function” OR “cognition” OR “abstinence” OR “urine drug test” OR “depression symptoms”). Additionally, reference lists of eligible articles were manually screened to identify any relevant studies that may have been missed.
Studies were eligible for inclusion if they aligned with our eligibility criteria: (1) randomized controlled trials (RCTs); (2) comparing atomoxetine versus placebo; (3) enrolling patients reported with stimulant dependence; and (4) reporting outcomes related to cognition, attention, response inhibition, drug use/abstinence, or mood symptoms in patients reported with stimulant dependence. No language restrictions were applied. We excluded studies that met any of the following criteria: (1) lack of a control group; (2) observational design; or (3) overlapping patient populations.
Study Selection
Two reviewers (M.R.A. and D.C.G.) independently screened titles and abstracts from the initial search to identify potentially eligible studies. In the second phase, full texts of selected studies were assessed against the predefined inclusion and exclusion criteria. Disagreements during screening or eligibility assessment were resolved through discussion, and a third reviewer (A.T.) was consulted when necessary.
Data Extraction
Two authors (R.S. and S.S.P.) independently extracted data from each included study, collecting information on study design, sample size, participant characteristics, intervention details (dose and duration of atomoxetine), outcomes assessed, and main findings. A third author (D.B.) verified all extracted data, and any discrepancies were resolved by consensus.
Summary Measures and Statistical Analysis
Outcomes were prespecified and grouped into 3 domains: (1) stimulant use and abstinence outcomes; (2) cognitive outcomes related to attention and inhibitory control; and (3) mood-related outcomes. We planned to conduct a meta-analysis only for outcomes that satisfied additional eligibility criteria: (i) reporting in at least 3 independent studies; (ii) use of comparable methodologies; and (iii) expression using the same or sufficiently similar units of measurement or effect estimates, thereby avoiding the need for statistical conversion. For continuous outcomes, we planned to extract or calculate mean differences (MD) with corresponding standard deviations (SD), and for dichotomous outcomes, relative risks with SD. Outcomes not meeting these criteria were synthesized narratively. None of the outcomes met the criteria for quantitative synthesis; therefore, a meta-analysis was not performed. Planned pooled analyses would have been conducted using R Studio (Posit, Boston) (version 4.5.1), with statistical significance defined as P < .05, and heterogeneity assessed using the I2 statistic.
Results
Baseline Study Characteristics
As shown in Figure 1, the database search identified 168 records. After the removal of duplicates and application of inclusion and exclusion criteria, 10 articles were retrieved for full-text review. Of these, 9 RCTs including 427 participants fulfilled all inclusion criteria and were included in the review, comprising both parallel-group, randomized controlled trials and randomized, double-blind crossover trials.19-28 Baseline study characteristics are summarized in Table 1.
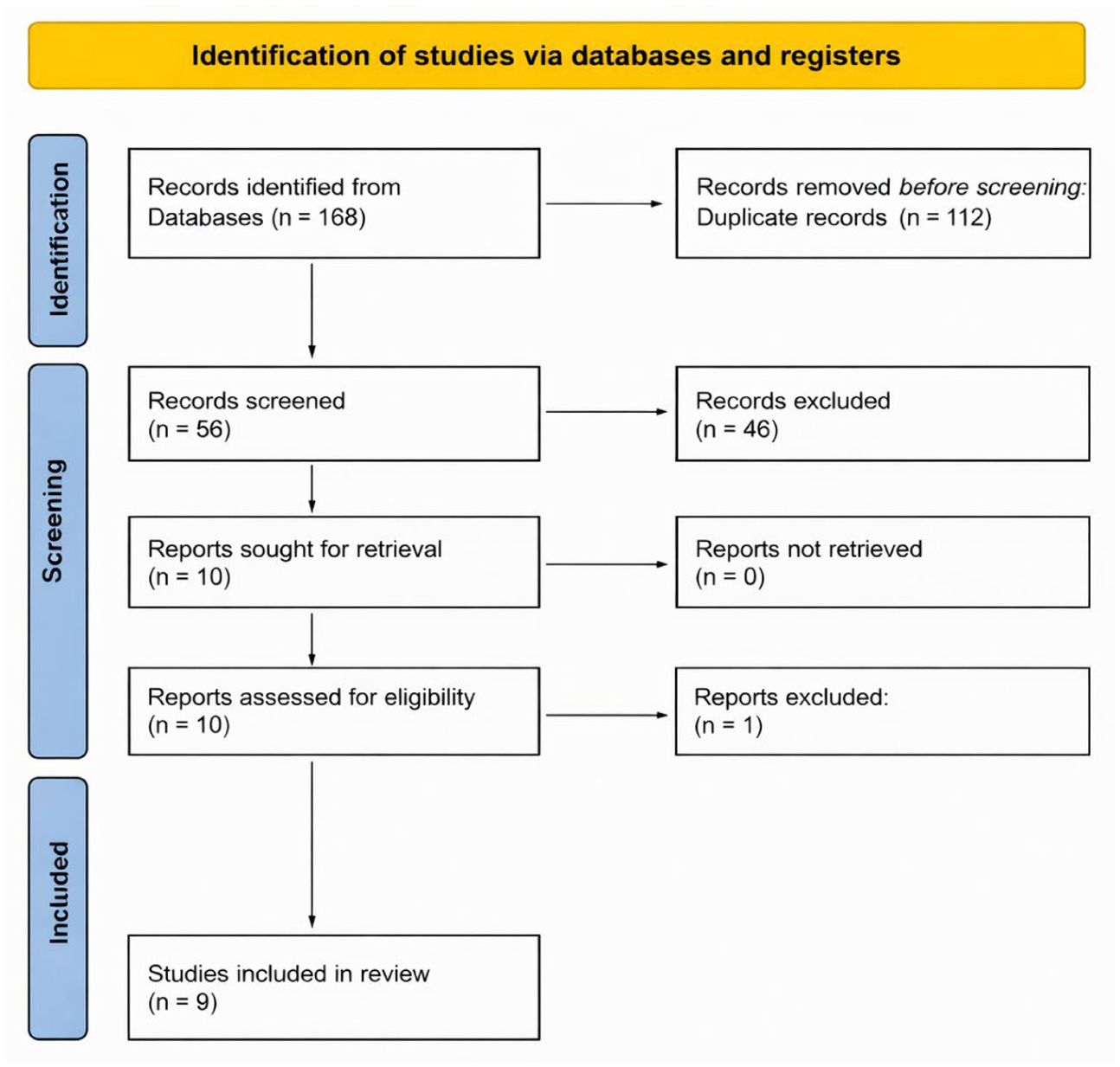
PRISMA diagram.
Characteristics of Included Randomized Controlled Trials Evaluating Atomoxetine in Stimulant Use Disorders.
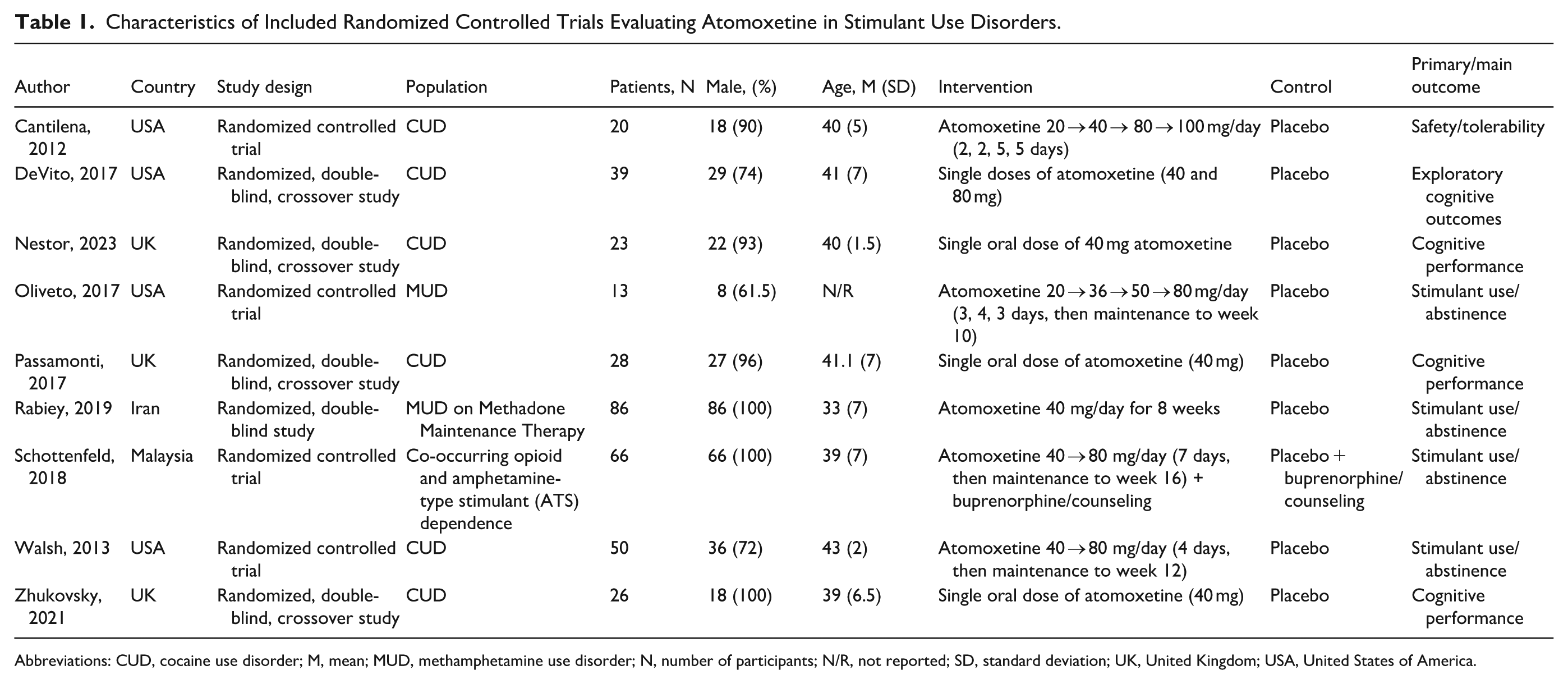
Abbreviations: CUD, cocaine use disorder; M, mean; MUD, methamphetamine use disorder; N, number of participants; N/R, not reported; SD, standard deviation; UK, United Kingdom; USA, United States of America.
Most trials were conducted in the United States,19-22,24 with additional studies from the United Kingdom,26-28 Iran, 23 and Malaysia. 25 Sample sizes ranged from 13 patients 22 to 86 patients. 23 Across studies, participants were predominantly male, with proportions ranging from 61.5% participants 22 to 100% in Rabiey (2019), Schottenfeld (2018), and Zhukovsky (2021).
With respect to study populations, 6 trials investigated individuals with cocaine use disorder,19-21,24,26-28 2 examined those with methamphetamine use disorder,22,23 and 1 included participants with amphetamine-type stimulant (ATS) and opioid use disorders treated with buprenorphine. 25 Placebo was used as the control condition in all studies; Schottenfeld (2018) was the only trial to employ an active comparator consisting of buprenorphine plus counseling.
Intervention duration varied. Four trials were single-session studies,20-21,26,27,28 whereas others lasted 8, 23 10, 22 12, 24 14, 19 and 16 weeks. 25 Crossover trials typically administered a single oral dose of atomoxetine (40-80 mg), while most longitudinal trials employed titrated regimens. Atomoxetine was titrated from 40–80 mg/day over 12 weeks in Walsh (2013) and 16 weeks in Schottenfeld (2018), 20–80 mg/day over 10 weeks in Oliveto (2017), and 20–100 mg/day over 14 weeks in Cantilena (2012).
Outcome Assessment
Table 2 summarizes the outcomes reported across studies, including abstinence/drug use, mood, cognition, safety, and adverse effects. In most studies, abstinence/drug use22-25 or cognitive performance26-28 were the primary outcomes. No outcome fulfilled the prespecified criteria for quantitative synthesis (ie, reporting by at least 3 independent studies with comparable methodology and measurement). Accordingly, results are presented narratively.
Clinical, Cognitive, and Safety Outcomes of Randomized Controlled Trials of Atomoxetine in Stimulant Use Disorders.
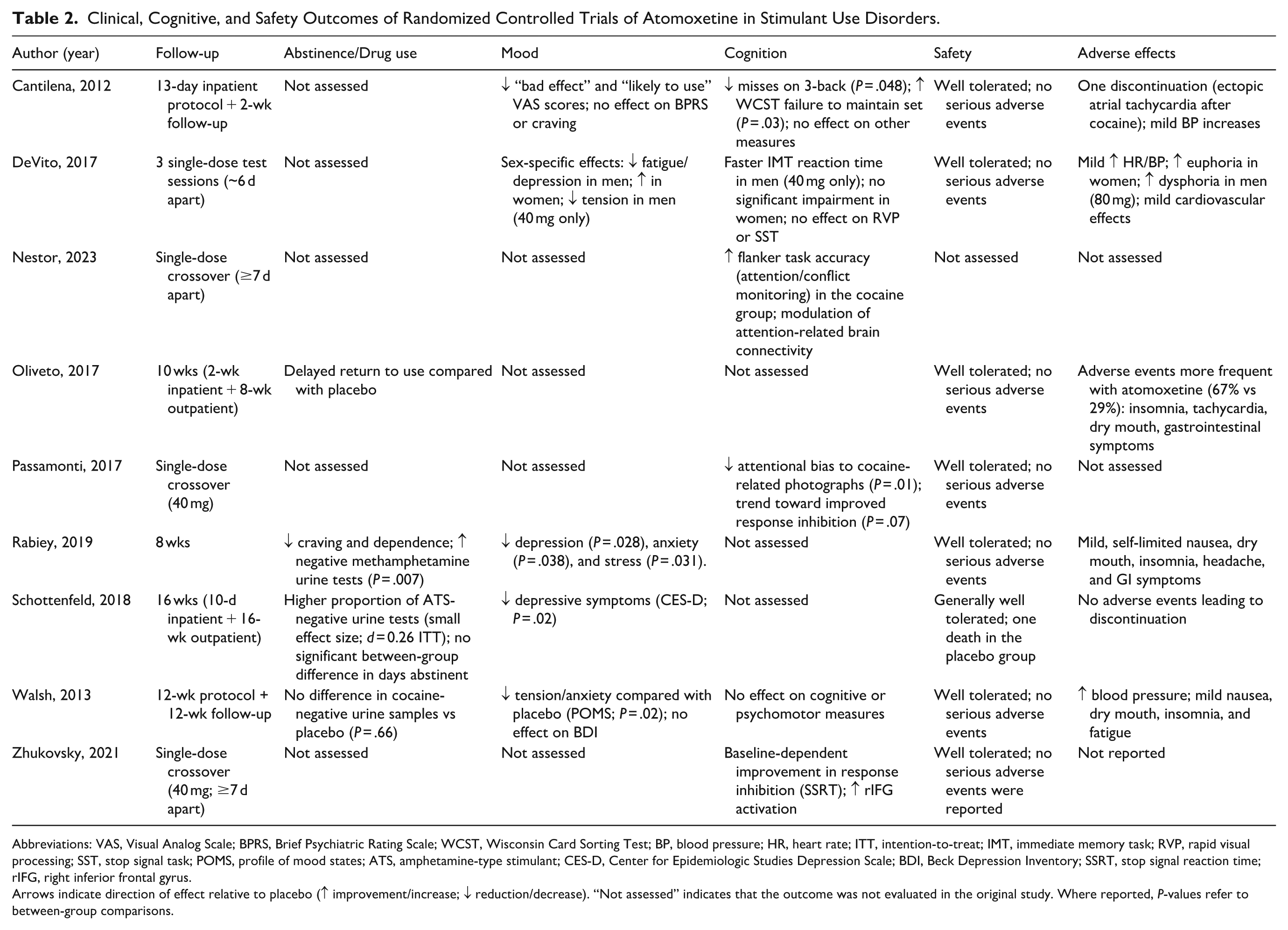
Abbreviations: VAS, Visual Analog Scale; BPRS, Brief Psychiatric Rating Scale; WCST, Wisconsin Card Sorting Test; BP, blood pressure; HR, heart rate; ITT, intention-to-treat; IMT, immediate memory task; RVP, rapid visual processing; SST, stop signal task; POMS, profile of mood states; ATS, amphetamine-type stimulant; CES-D, Center for Epidemiologic Studies Depression Scale; BDI, Beck Depression Inventory; SSRT, stop signal reaction time; rIFG, right inferior frontal gyrus.
Arrows indicate direction of effect relative to placebo (↑ improvement/increase; ↓ reduction/decrease). “Not assessed” indicates that the outcome was not evaluated in the original study. Where reported, P-values refer to between-group comparisons.
Abstinence and Drug Use Outcomes
Four of the 9 included RCTs reported outcomes related to stimulant use, abstinence, or return to use. Findings were heterogeneous. Rabiey et al (2019) reported that atomoxetine significantly reduced methamphetamine craving and dependence, with a higher proportion of negative urine tests compared with placebo (P = .007). Schottenfeld et al (2018) observed a higher proportion of ATS-negative urine tests during weeks 9 to 16, although between-group differences in abstinent days were not statistically significant. Oliveto (2017) found a longer median time to return to use in the atomoxetine group. By contrast, Walsh et al (2013) found no significant difference in cocaine-negative urine samples between groups. The remaining 5 studies did not assess abstinence or return-to-use outcomes.
Mood Outcomes
Mood-related outcomes were reported in 5 of the 9 included trials, with effects varying across studies and, in some cases, by sex. DeVito (2017) reported sex-specific effects favoring men for fatigue (P = .013) and depression (P = .045), with sex-by-dose interactions for tension at 40 mg (P = .040) and fatigue (P = .030). Rabiey et al (2019) found significant reductions in depression (P = .028), anxiety (P = .038), and stress (P = .031) scores (Depression, Anxiety and Stress Scale) in the atomoxetine group compared with placebo. Schottenfeld et al (2018) observed reductions in Center for Epidemiologic Studies Depression Scale scores over time (P = .02), with greater reductions in the atomoxetine group. Walsh et al (2013) reported reduced tension and anxiety in the atomoxetine group compared with placebo (Profile of Mood States interaction P = .02), while no differences were observed on the Beck Depression Inventory. Cantilena (2012) reported reductions in VAS-rated “bad effect” (P = .003) and “likely to use” (P = .03), without significant effects on standardized mood scales. Several studies22,26-28 did not evaluate mood outcomes.
Cognitive Outcomes
Cognitive outcomes were assessed in 6 of the 9 included trials, with effects differing across tasks and study designs. DeVito (2017) reported modest improvement in immediate memory task (IMT) discriminability that did not survive correction, and no changes in rapid visual processing or stop signal tasks; a dose-by-sex interaction was observed for IMT reaction time (P = .026), with improvement in men at 40 mg only. Passamonti (2017) found reduced attentional bias to cocaine-related photographs (P = .01) and a near-significant trend toward improved response inhibition (P = .07). Zhukovsky (2021) reported baseline-dependent improvement in stop-signal reaction time accompanied by increased inferior frontal gyrus activation, without a significant overall drug effect at the group level. Cantilena (2012) observed fewer misses on a 3-back task (P = .048) but no differences in hits or commission errors; on the Wisconsin Card Sorting Test, the atomoxetine group demonstrated greater difficulty maintaining set (P = .03). Nestor (2023) found improved flanker task accuracy in the cocaine group and modulation of functional connectivity during task performance. Walsh et al (2013) reported no significant effects on cognitive or psychomotor measures. Rabiey (2019), Oliveto (2017), and Schottenfeld (2018) did not assess cognition.
Safety and Adverse Effects
Atomoxetine was generally well tolerated, and no study reported serious adverse events directly attributable to the medication. Rabiey et al (2019) and Schottenfeld et al (2018) reported no serious adverse events, with the latter noting one unrelated death in the placebo group. Walsh et al (2013) and Zhukovsky (2021) similarly reported no serious adverse events, although modest increases in blood pressure were reported in some studies.19-21,24 DeVito (2017) documented dose-related increases in heart rate and blood pressure, as well as sex-specific subjective effects, including increased euphoria in women and increased dysphoria at higher doses in men. Cantilena (2012) found small but statistically significant hemodynamic changes without serious clinical consequences. Oliveto (2017) documented a higher frequency of adverse events in the atomoxetine group than in placebo (67% vs 29%), although these were predominantly mild and transient, including insomnia, tachycardia, dry mouth, and gastrointestinal symptoms. Regarding sleep adverse events, some studies reported insomnia.22-24 Passamonti (2017) reported no adverse events, and Nestor (2023) did not provide formal safety data.
Other Findings
Several additional results were noted. DeVito (2017) identified sex differences in both subjective and cognitive responses. Passamonti (2017) reported that longer cocaine use duration was associated with smaller reductions in attentional bias. Zhukovsky (2021) found that atomoxetine blood levels correlated positively with right inferior frontal gyrus activation during successful stopping. Cantilena (2012) confirmed the safety and psychological detectability of submaximal intravenous cocaine doses as part of pharmacological validation.
Discussion
This systematic review evaluated atomoxetine for StUD, prioritizing stimulant use and abstinence as primary efficacy outcomes while also examining cognitive and mood effects as intermediate targets relevant to relapse vulnerability and treatment engagement. Although atomoxetine is an established treatment for ADHD and has a compelling theoretical rationale for StUD, through modulation of noradrenergic signaling and enhancement of prefrontal executive control, the available clinical evidence does not support its effectiveness in reducing stimulant use.9,29 RCTs have generally failed to demonstrate consistent benefits over placebo with respect to consumption, craving, or sustained abstinence. Modest improvements in mood, particularly among male participants, have been reported but were neither robust nor consistent across studies. Evidence of cognitive enhancement (including improvements in attentional bias, response inhibition, and reaction time) has also been observed; however, variability in cognitive measures limited comparability between trials.
Stimulant use or abstinence was most often the primary endpoint in the included studies. In several trials, cognitive and mood outcomes were secondary or exploratory endpoints, and multiple comparisons were often conducted without formal adjustment, increasing the risk that isolated positive findings reflect chance rather than robust effects. Overall, atomoxetine was well tolerated, with adverse events typically mild and transient, but its clinical utility for StUD remains unsubstantiated. When considered against the broader pharmacotherapy landscape for StUD, the evidence summarized here suggests that atomoxetine does not represent a promising candidate for further standalone investigation.
Defining clinical effectiveness in StUD warrants careful consideration. In the context of StUD, the ultimate therapeutic goal is typically sustained abstinence or a clinically meaningful reduction in stimulant use, given the strong association between continued use and adverse medical, psychiatric, and social outcomes. Accordingly, outcomes such as abstinence rates, frequency of use, and objective toxicology measures are often prioritized as primary indicators of treatment efficacy in clinical trials and guidelines. However, intermediate outcomes, such as reductions in craving, improvements in cognitive control, or mood stabilization, may still carry clinical relevance, particularly if they contribute to treatment engagement, retention, or reduced relapse severity. In the present review, atomoxetine demonstrated modest and inconsistent effects on some intermediate domains (eg, cognition and mood), but these did not translate into reliable reductions in stimulant use or sustained abstinence. As such, while certain changes may be clinically meaningful at an individual level, the absence of consistent effects on use-related endpoints limits the interpretation of atomoxetine as an effective treatment for StUD at the population level.
These findings align with the broader pharmacotherapy literature, where no single agent has demonstrated reliable, generalizable efficacy for StUD. Trials of psychostimulant agonists such as methylphenidate and dextroamphetamine have shown some promise, particularly in cocaine use disorder, but results have been inconsistent.30,31 Similarly, other agents, including modafinil, bupropion, and topiramate for cocaine-type, have produced modest or subgroup-specific effects, yet meta-analyses converge on the conclusion that no pharmacological treatment currently provides dependable benefit.32,33 Within this context, atomoxetine exemplifies a recurring pattern in which agents with strong mechanistic rationale fail to translate into clinical effectiveness. By contrast, behavioral interventions, most notably CM and CBT, remain the most consistently supported treatments for StUD.34,35
Notably, the neurobiological rationale for evaluating atomoxetine derives from converging evidence that chronic stimulant exposure disrupts dopamine and norepinephrine signaling within mesocorticolimbic circuits, thereby impairing executive control and promoting compulsive drug-seeking.36-38 Preclinical studies further indicate that norepinephrine transporter inhibition enhances prefrontal cortical regulation of behavior and reduces stimulant self-administration in animal models.11,39 The high prevalence of comorbid ADHD, affecting up to one third of individuals with StUD, 40 provides an additional rationale, given atomoxetine’s established efficacy as a non-stimulant ADHD therapy. 41 However, despite a compelling mechanistic rationale, the existing randomized trials, although few and heterogeneous, have not shown consistent or clinically meaningful benefit. This limits the strength of the current evidence base to justify continued independent investigation of atomoxetine as a monotherapy for StUD. This conclusion does not preclude further investigation in narrowly defined contexts, such as individuals with comorbid ADHD or as an adjunct to CM, but it does argue against prioritizing atomoxetine as a broadly promising pharmacologic candidate.
The limited clinical effects observed may reflect the core pathology of stimulant addiction, which involves profound dysfunction in reward and motivational systems, particularly dopaminergic circuitry in the mesolimbic pathway. Enhancing executive control alone may be insufficient to counteract compulsive reward-seeking. In contrast, ADHD medications such as methylphenidate and dextroamphetamine act directly on dopaminergic signaling, increasing extracellular dopamine within mesolimbic circuits through transporter blockade and, in the case of amphetamines, vesicular release. This mechanism is particularly relevant given consistent imaging evidence of reduced striatal dopamine release, transporter availability, and D2/D3 receptor binding among those who use stimulants.42,43 By partially restoring dopaminergic tone, stimulant agonists may more directly address the hypodopaminergic state underlying compulsive drug-seeking. Clinical trials of sustained-release dextroamphetamine and high-dose methylphenidate in cocaine use disorder have reported reductions in cocaine-positive urine samples and craving, although these effects remain inconsistent across studies.42,44,45 Reviews and guidelines similarly conclude that psychostimulant agonist therapy can benefit certain subgroups (such as those with comorbid ADHD or heavier baseline use) but is not yet a broadly reliable treatment.8,46 This contrast underscores the limitation of atomoxetine: While it engages executive-control circuits via noradrenergic modulation, its effects may be insufficient unless reward-related and motivation-related dopaminergic dysfunctions are also targeted.
For instance, a meta-analysis of in vivo imaging studies found consistent and pronounced deficits in dopamine release, transporter availability, and D2/D3 receptor binding among stimulant users compared with those among controls, reflecting a broadly downregulated dopaminergic system. 44 Neurobiological models further suggest that when reward and habit circuits dominate motivational drive, improvements in top-down control may be overwhelmed. 45 Supporting this, animal studies of working-memory training have shown increased markers of prefrontal plasticity (eg, Brain-Derived Neurotrophic Factor) without reductions in drug self-administration or cue-induced seeking. 47 Thus, while atomoxetine engages noradrenergic and executive-control pathways, these effects may be insufficient unless reward-related and motivation-related dysfunctions are also addressed.
This underscores a broader recognition that single-agent pharmacotherapies may be insufficient to address the complex pathophysiology of StUD. 48 Emerging evidence supports the integration of pharmacological agents with behavioral interventions, such as CM, to enhance treatment outcomes. 48 For instance, combining atomoxetine with CM could potentially leverage its effects on executive control and motivation, thereby improving treatment adherence and reducing stimulant use. This approach aligns with the shift toward multimodal treatment strategies that consider the complex interplay of biological, psychological, and social factors in substance use disorders. 49 If atomoxetine is studied further, such research should be restricted to adequately powered trials in clinically or mechanistically stratified populations where a clear rationale exists, given the lack of consistent benefit observed in broader stimulant-using samples.
It is also important to note that atomoxetine was generally well tolerated in the included trials, with adverse events typically mild and transient. However, its lack of demonstrated efficacy for stimulant use disorder raises important ethical and practical considerations. 8 In individuals with comorbid ADHD and StUD, atomoxetine may still represent a reasonable treatment option for managing ADHD symptoms. 13 Still, it should not be prescribed with the expectation of reducing stimulant use. Unjustified prescribing risks exposing patients to unnecessary costs and potential side effects, while diverting attention from interventions with established benefit, such as CM and CBT.34,35 Given the clinical vulnerability of this population, characterized by high return to use risk, comorbidity, and limited access to effective care, research findings must be communicated with caution, and therapeutic recommendations should remain firmly grounded in evidence. 8
Another key limitation relates to dosing. While established titration strategies exist for ADHD, no comparable guidelines are available for StUD, and existing trials provide no evidence that higher doses improve outcomes. 50 The same challenge applies to other off-label agents, such as methylphenidate and dextroamphetamine, where dosing practices are largely borrowed from ADHD treatment. At present, there is no indication that dosing strategies in StUD differ from those in ADHD, and no data suggest that nonstandard dosing yields superior results.50-52 This lack of dosing guidance further limits the interpretation of atomoxetine’s efficacy in this context.
An additional consideration concerns the time course of atomoxetine’s therapeutic response. Evidence from ADHD populations indicates that although symptomatic improvements can begin within 1 to 2 weeks of initiation, maximal efficacy is generally not achieved until at least 6 to 12 weeks of continuous treatment, with incremental gains continuing up to 24 weeks or longer in some patients.14,53-55 Pooled analyses further demonstrate that both effect sizes and responder rates increase over time, with substantially stronger outcomes observed during 12 to 24 weeks compared with earlier assessments. 55 This gradual, time-dependent trajectory suggests that short trial durations, commonly less than 12 weeks in the StUD literature, may underestimate atomoxetine’s potential benefits. Thus, insufficient treatment exposure could plausibly contribute to the negative or inconclusive findings reported to date.
This review represents the first systematic evaluation of atomoxetine for StUD and should be interpreted within the constraints of a preliminary evidence base. The small number of trials, modest sample sizes, short treatment durations, and high attrition rates limit confidence in the findings. Heterogeneity in stimulant type (cocaine versus amphetamine) and comorbidity profiles, particularly the lack of systematic assessment or stratification by ADHD, further constrained synthesis and limits the ability to disentangle effects on StUD from potential benefits related to untreated or unmeasured ADHD. Most studies were also underpowered to explore subgroup effects, and none were designed to prospectively test whether outcomes differed as a function of comorbid ADHD. These limitations preclude firm conclusions regarding efficacy and constrain the interpretation of the existing evidence.
This should be considered in the perspective that clinical trials for StUD face persistent challenges that limit their interpretability. High attrition, often exceeding 50%, undermines internal validity and generalizability. Outcome measurement is complicated by reliance on self-reports, which are susceptible to underreporting due to social desirability, and by heterogeneity in endpoints, including inconsistent definitions of abstinence and craving. 56 Short trial durations relative to the chronic course of addiction further restrict evaluation of sustained effects. Improvement in the evidence base can be improved by standardized outcomes, extended follow-up, and employing multisite designs to enhance reliability, comparability, and generalizability.
Future research should prioritize adequately powered RCTs incorporating adaptive trial designs to address retention challenges, such as employing multisite designs to enhance reliability, comparability, and generalizability. Precision medicine approaches, including treatment matching by clinical or neurocognitive profiles, may help identify responsive subgroups. Integrating mechanistic assessments, including neuroimaging and biomarker analyses, may further clarify whether noradrenergic modulation has therapeutic potential within the broader context of StUD.
Conclusion
Atomoxetine has not demonstrated consistent efficacy in reducing stimulant use, although modest and inconsistent cognitive and mood effects were observed. Although atomoxetine is generally well tolerated and may remain appropriate for treating comorbid ADHD, current data do not support its use or prioritization as a stand-alone treatment for StUD.
Footnotes
Ethical Considerations
This article does not contain any studies with human participants or animals performed by any of the authors.
Author Contributions
Conceptualization: DB, TM, HO; Methodology: DB, NP, AG, TM, HO.; Data curation: DB, MPE, VA, BP, EC.; Formal analysis: DCG, VR, LCH, IRZ, VGS.; Software: VR, LCH, IRZ, VGS.; Writing (original draft): DB, MLS.; Writing (review & editing): DB, NP, AG, DBK, RERF.; Supervision: DBK, RERF.; Project administration: DB, NP, AG.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.