
Abstract
Background:
Xylazine has emerged in the unregulated drug supply and is associated with heavy sedation and severe skin wounds. This study uses dried blood spot (DBS) testing to examine xylazine exposure among a community-based sample of people who use drugs in Rhode Island.
Methods:
We conducted a secondary analysis of 234 people who use drugs enrolled in a clinical trial with DBS samples from October 2020 to December 2023. Participants completed interviews at multiple visits (baseline, 6, and 12 months); DBS samples were tested at 1 or more of those time points. Samples were tested for xylazine, fentanyl, and fentanyl analogs. We compared baseline sociodemographic and drug use characteristics of participants with and without detectable xylazine at any time point using descriptive statistics.
Results:
We found that 69 (29%) participants had detectable fentanyl at 1 or more time points, and among those, 27 (39%) had detectable xylazine. Detection of xylazine was associated with younger age, non-Hispanic white race, and prior-month homelessness (all P < .05). Among 397 DBS samples, 97 (24%) had detectable fentanyl and 32 (8%) had detectable xylazine. Among samples with detectable fentanyl, xylazine positivity was 24%, 21%, and 80% in years 2021, 2022, and 2023, respectively.
Conclusion:
DBS testing identified moderate levels of xylazine exposure among a sample of people who use drugs in Rhode Island during the observation period. Findings underscore the need for targeted xylazine education and harm reduction strategies focused on people who use fentanyl and unregulated opioids.
Highlights
12% of participants tested positive for xylazine using DBS testing.
Those testing positive for xylazine were more likely younger, non-Hispanic white, homeless.
Xylazine was strongly associated with fentanyl use and preference for fentanyl.
Among samples with detectable fentanyl, xylazine detection greatly increased in 2023.
Introduction
Over the past decade, continual changes in the unregulated drug supply have exacerbated drug-related morbidity and mortality.1,2 Non-pharmaceutical fentanyl now dominates the unregulated opioid supply, 3 and overdoses involving both stimulants and opioids (primarily fentanyl) characterize the “fourth wave” of the epidemic.3-6 Xylazine, a veterinary tranquilizer, first emerged in the Puerto Rican drug market in 2001; 7 however, more recently, xylazine has emerged as a novel substance detected alongside fentanyl in overdose postmortem toxicologies8-11 and in public health–based surveillance of unregulated drug supplies in the continental United States.12,13 First emerging in the Northeast, xylazine was present in 34% of overdose deaths in Philadelphia in 2022 14 and approximately 9% of overdose deaths in Massachusetts in 2023. 15 Between May 2022 and December 2023, a community-based drug-checking study known as testRI 16 found xylazine in 44% of drug residue samples tested in Rhode Island; in every case, xylazine was detected alongside fentanyl.17,18 Although the drug supply in the Northeastern United States shows a higher prevalence of xylazine than other regions, 19 xylazine emerged on the West Coast in early 2023, with 29% of samples from a community-based drug-checking program in Los Angeles County showing concentrations of the substance by 2025. 20
Xylazine’s emergence is thought to be a result of the substance extending the “legs” (ie, duration) of drug effects and enhancing its euphoric effects. 12 However, other factors likely contribute to xylazine’s presence in the drug supply, including economic considerations such as cost, accessibility, and reduction in the availability of fentanyl. 21 Research has documented numerous adverse experiences with xylazine, including heavy and prolonged sedation,11,22,23 with increased risks of violence and victimization; 22 blackouts and amnesia;11,22 parasomnia; 22 acute skin and soft tissue infections;11,22,23 and symptoms of xylazine withdrawal, including anxiety and body aches. 23 Despite the documented adverse effects of xylazine exposure and numerous research publications about xylazine, scarce research has examined the emergence of xylazine in unregulated drug supplies in New England.
Several approaches have been employed to document trends in xylazine presence, including direct testing of drug samples (eg, community-based drug-checking programs), 16 testing urine samples obtained from clinical settings,24,25 and postmortem toxicology. 10 Other chemical analyses could complement these approaches, particularly when drug-checking infrastructure or access to clinical care is limited.
The present study uses dried blood spot (DBS) testing, a collection method that affords greater sample stability, easier transport, and more feasible collection than traditional venipuncture-based blood sampling for subsequent centralized laboratory testing.26,27 We examined the presence of xylazine in DBS samples that were collected among people who use drugs in Rhode Island from October 2020 through December 2023. 28 The objectives of this research were to: (1) identify participants’ sociodemographic and drug use pattern correlates of exposure to xylazine and (2) document changes in the prevalence of xylazine in DBS samples over the course of the observation period.
Methods
Setting and Data Collection
The parent study (ie, Rhode Island Prescription and Illicit Drug Study [RAPIDS]), described previously, 28 compared a fentanyl test strip and behavioral intervention to standard overdose education among people who use drugs; the primary aim of the parent study was to assess the efficacy of the intervention in reducing rates of overdose among people who use drugs. In this RAPIDS substudy, we collected DBS via capillary fingerstick to identify novel substances (eg, xylazine, emergent fentanyl analogs) that were not captured by the drug detection procedures used in the parent study. DBS was proposed as a “toxico-surveillance system” to characterize the changing drug supply over the study follow-up. Rhode Island residents were eligible if (a) they were aged 18 to 65 years; (b) they were able to complete interviews in English; (c) they were able to provide informed consent; and (d) they reported past 30-day substance use (ie, unregulated stimulants or opioids, prescription medications purchased extramedically, or any past-month injection drug use [IDU]). Participants were recruited using a combination of strategies, including internet-based advertising and marketing on state-wide public transit. Baseline and follow-up visits were completed from September 2020 to May 2024; DBS samples were collected from October 2020 through December 2023.
At baseline and 5 follow-up visits (1, 2, 3, 6, and 12 months post-baseline), participants completed a standardized, interviewer-administered questionnaire that elicited sociodemographic information, drug use patterns, and clinical characteristics. The primary outcome of the RAPIDS parent clinical trial was a composite measure of self-reported overdose in the previous month at 6 and 12-month follow-up visits; secondary outcomes included fatal and nonfatal overdose from postmortem investigation and hospitalization or emergency medical service utilization, respectively. At 3 study visits (ie, baseline, 6, and 12 months), fingerstick DBS samples were collected from consenting participants at fixed study sites. Thus, participants could have up to 3 DBS samples collected throughout the study period. Consent for DBS collection was obtained separately from consent for the main study assessments; therefore, only those participants who consented to DBS collection contributed DBS samples.
DBS Analysis
Collected DBS were dried overnight and stored at −80°C until processing. DBS samples with at least 1 visible blood spot were tested in the Brown University Health Toxicology laboratory for the presence of xylazine and fentanyl (Table S1) via Liquid Chromatography Quadrupole Time-of-Flight Mass Spectrometry (LC-QTOF-MS) on a Sciex X500R QTOF platform. Fentanyl products detected included analogs (para-fluorofentanyl, acetylfentanyl), metabolites (norfentanyl), or precursors (4-ANPP, NPP, phenethyl 4-ANPP, despropionyl para-fluorofentanyl) (Table S1). The DBS samples were analyzed using an untargeted acquisition method capable of detecting a wide range of substances; however, this investigation focused solely on xylazine and fentanyl because they were most relevant to the primary outcomes of the parent study (Table S1). DBS samples were routinely batched, stored, and sent to an off-site laboratory for analysis. Samples were then processed and analyzed at the collaborating laboratory, with results transmitted back to the study investigators approximately annually. At the consenting stage, participants were informed that the results would not be relayed back to them, given substantial delays in sample collection, transfer, and analysis. This secondary analysis includes RAPIDS participants who provided consent for the collection of DBS and provided ≥1 DBS sample (Figure S1). Table S2 presents baseline distributions of eligible participants and the broader RAPIDS cohort. We did not collect information on who was offered DBS testing, although it varied by survey administration site capabilities.
Measures
The primary outcome was whether participants had detectable xylazine at any time point (ie, baseline, 6, 12 months). Individual-level exposures assessed at baseline included participants’ self-reported sociodemographic characteristics (eg, age, sex at birth, gender identity, sexual orientation, race/ethnicity, homelessness status, monthly income, and history of incarceration), drug use patterns (regular use of unregulated drugs [ie, at least weekly in the prior month], IDU, sharing of syringes or supplies, drug selling history, overdose history), fentanyl-specific characteristics (regular fentanyl use, preference for fentanyl), and clinical characteristics (use of opioid agonist therapy [OAT], diagnosed depression, anxiety, and bipolar disorder).
Statistical Analysis
Results are stratified by the detection of xylazine in DBS at any time point (yes vs no). Groups were compared using Wilcoxon rank sum tests, Chi-squared tests, or Fisher’s exact tests as applicable. P-values ≤ .05 were considered statistically significant. A two-paneled histogram presents quarterly xylazine test positivity: One panel displays the proportion of samples with detectable xylazine, and the other shows the proportion among fentanyl-positive samples. Ethics approval was obtained from the Brown University Institutional Review Board.
Results
Sociodemographics
Among 503 RAPIDS participants, 264 (52%) were enrolled during the DBS sample collection period (October 2020 to December 2023) and consented to DBS testing (Figure S1). Almost half (234 participants, 47%) of the total sample provided 397 DBS samples over the 3 study visits: 121 (52%) participants provided 1 sample, 63 (27%) provided 2, and 50 (21%) provided 3 (Figure S1). The median age at enrollment was 44 years, 34% were assigned female at birth, 96% were cisgender, and 18% identified as non-Hispanic black (Table 1).
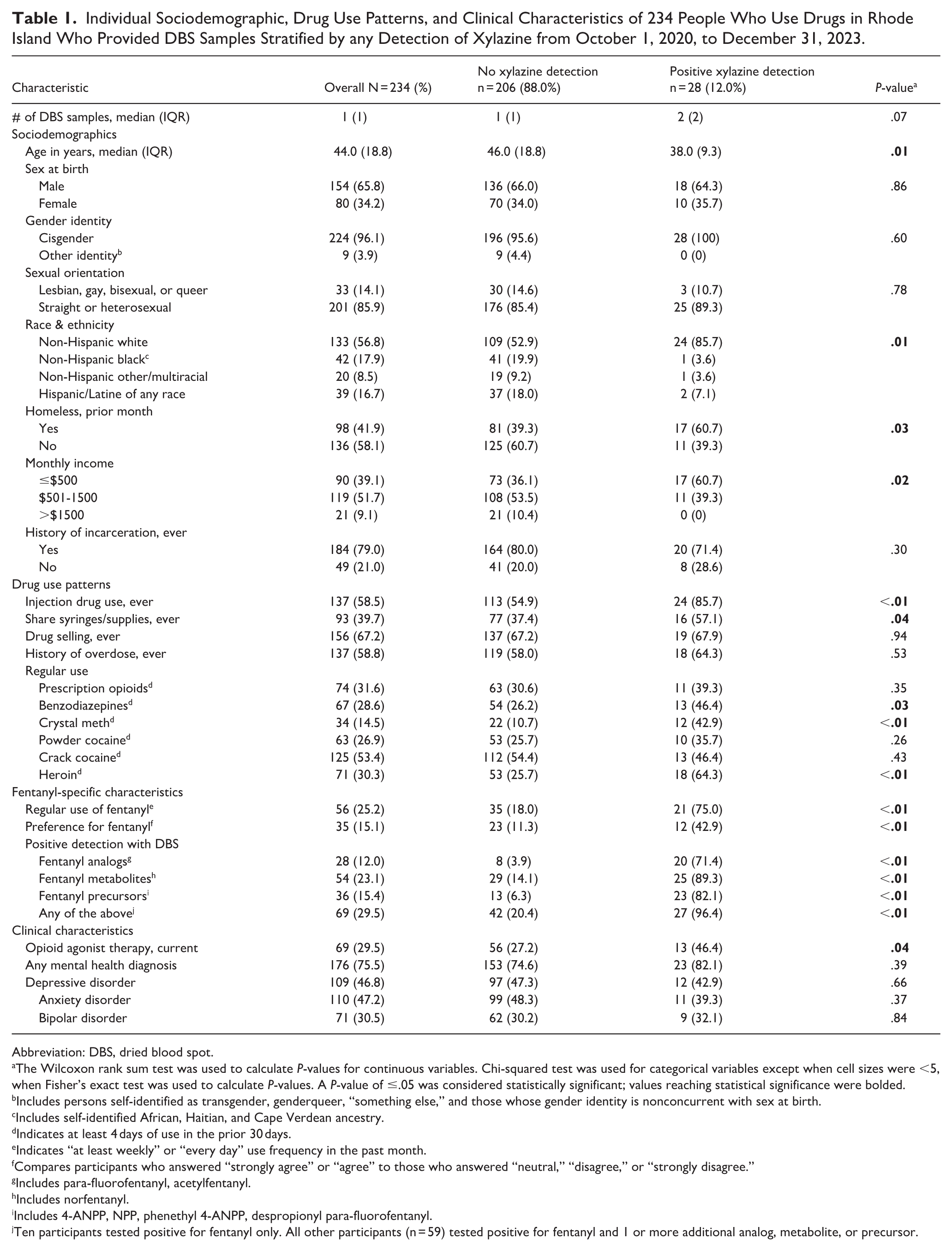
Individual Sociodemographic, Drug Use Patterns, and Clinical Characteristics of 234 People Who Use Drugs in Rhode Island Who Provided DBS Samples Stratified by any Detection of Xylazine from October 1, 2020, to December 31, 2023.
Abbreviation: DBS, dried blood spot.
The Wilcoxon rank sum test was used to calculate P-values for continuous variables. Chi-squared test was used for categorical variables except when cell sizes were <5, when Fisher’s exact test was used to calculate P-values. A P-value of ≤.05 was considered statistically significant; values reaching statistical significance were bolded; bIncludes persons self-identified as transgender, genderqueer, “something else,” and those whose gender identity is nonconcurrent with sex at birth; cIncludes self-identified African, Haitian, and Cape Verdean ancestry; dIndicates at least 4 days of use in the prior 30 days; eIndicates “at least weekly” or “every day” use frequency in the past month; fCompares participants who answered “strongly agree” or “agree” to those who answered “neutral,” “disagree,” or “strongly disagree.”; gIncludes para-fluorofentanyl, acetylfentanyl; hIncludes norfentanyl; iIncludes 4-ANPP, NPP, phenethyl 4-ANPP, despropionyl para-fluorofentanyl; jTen participants tested positive for fentanyl only. All other participants (n = 59) tested positive for fentanyl and 1 or more additional analog, metabolite, or precursor.
Twelve percent (n = 28) of participants had detectable xylazine through DBS testing during at least 1 study visit (Table 1). Among those with detectable xylazine during at least 1 study visit, 24 (86%) had 1 positive sample, 4 (14%) had 2, and none had 3.
Participants with detectable xylazine at any time point were 8 years younger at baseline than those who did not have detectable xylazine (P = .01). A significantly higher proportion of those with detectable xylazine were also non-Hispanic white, homeless in the prior month, and earned <$500 per month (all P < .05).
Drug Use Patterns
Over half (58%) of participants had ever injected drugs, and 40% had ever shared syringes/supplies. Both practices were more prevalent among those with positive xylazine results (P < .01 and P = .04, respectively). Those with detectable xylazine during the study period were also more likely to report regular use of benzodiazepines, crystal methamphetamine, heroin, and fentanyl (all P < .05).
Fentanyl-Specific Characteristics
At baseline, 25% of participants reported regular use of fentanyl in the prior month, and 15% reported preferring fentanyl over other drugs. Thirty percentage of participants tested positive for a fentanyl analog, metabolite, or precursor at least once during follow-up. All fentanyl-specific characteristics differed by the detection of xylazine in DBS, with those who tested positive for xylazine being more likely to use, prefer, and test positive for fentanyl (all P = .01). Among those with xylazine detected, 96% (n = 27) also had fentanyl detected.
Clinical Characteristics
Those engaged in OAT at baseline were significantly more likely to have xylazine detected (46% with detectable xylazine versus 27% without, P = .04). There were no significant differences in mental health diagnoses.
Detection of Xylazine Over Time
We present DBS sample results as a two-panel histogram, ranging from October 2020 through the end of December 2023, by quarter; Figure 1 shows results out of the total number of samples tested (Panel 1A, N = 397) and results among samples with fentanyl detected (Panel 1B, N = 97). Thirty-two of 397 DBS samples tested positive for xylazine over the study period, for an overall test positivity rate of 8%. Xylazine was detected in 6% and 5% of samples in 2021 and 2022, respectively, and increased precipitously to 21% of samples (12 of the 57 samples tested) in 2023 (Figure 1A). When restricting the sample to only those testing positive for fentanyl, xylazine positivity was 24%, 21%, and 80% in years 2021, 2022, and 2023, respectively (Figure 1B). All samples with fentanyl detected in the final 3 quarters of 2023 (n = 5) also contained xylazine. Lastly, we present the proportion of individuals with positive DBS sample results over time (Figure S2). There were 28 individuals who tested positive for xylazine at some point during study follow-up, with 9 participants testing positive in 2023.
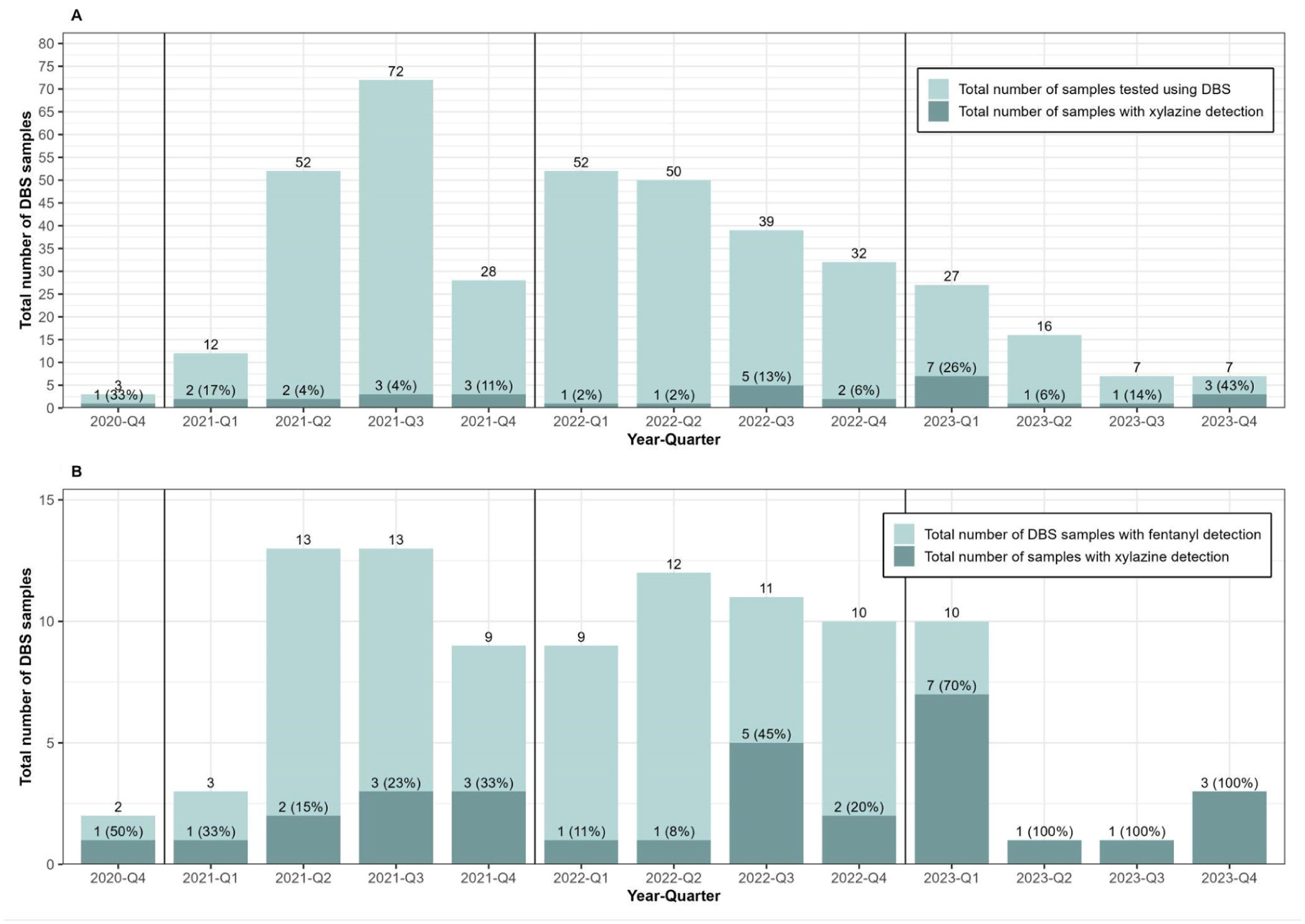
Two-panel histogram of xylazine detection out of the total number of samples tested using DBS (Figure 1A, N = 397, 32 samples with xylazine detected) and the total number of samples tested using DBS with fentanyl detection (Figure 1B, N = 97, 31 samples with both xylazine and fentanyl detected) from October 1, 2020, to December 31, 2023, among a sample of people who use drugs in Rhode Island. DBS, dried blood spot.
Discussion
Using DBS testing, this study documented moderate levels of xylazine exposure in a community-recruited sample of people who use drugs in RI. We found that 69 (29%) participants had detectable fentanyl, and among those, 27 (39%) had detectable xylazine. Participants exposed to xylazine tended to be younger, non-Hispanic white, homeless, and earn less money per month. They also tended to report IDU and sharing of supplies/syringes, among other drug use–related factors. There were some differences in self-reported regular use of fentanyl at baseline (25%) and positive detection of fentanyl at some point over the study period (30%); these differences may reflect unrecognized fentanyl exposure, differing recall periods, or variations in fentanyl use (eg, discontinued fentanyl use after baseline exposure and assessment). Finally, we identified an approximately four-fold increase in test positivity in 2023 compared with that in 2021 and 2022, contributing to the literature documenting the proliferation of xylazine in the drug supply in RI.
DBS was a feasible method of sample testing and could be added to the existing tools for chemical analysis in clinical and/or community-based settings, as it does not require venous access, phlebotomy, or access to medical or health care settings. 29 In light of the high prevalence of the co-occurrence of xylazine with fentanyl and the elevated presence of xylazine among those engaged in OAT, informative and educational harm reduction programming should be offered in settings that serve those who use unregulated opioids (eg, syringe service programs, OAT programs) in preventing or treating adverse reactions from xylazine (eg, skin wounds).
Our findings validate prior work in Rhode Island. Notably, a project called testRI collected drug samples from community members, used comprehensive toxicology testing via LC-QTOF-MS, and reported back to the community via plain language reports,13,17 integration with existing public dashboards, 30 and peer-reviewed research. 18 From May 2022 through January 2023, testRI documented that among samples with detectable fentanyl, 62% had detectable xylazine. 18 Our study results show a very high co-occurrence of xylazine and fentanyl (aligned with testRI findings), with only 1 sample with detectable xylazine not also having detectable fentanyl, although fentanyl may have been present at levels below detection due to differences in the detection window for xylazine and fentanyl. Several factors may explain the differences between our results and those from testRI. Xylazine presence may be overrepresented in drug-checking service surveillance systems, as people may be more likely to submit samples that produced unusual effects. Recent pharmacokinetic research suggests that blood testing would adequately afford detection of xylazine alongside fentanyl,31,32 so the difference in results may be due to sampling bias or differences in populations. For these reasons, it is imperative to monitor changes to the ever-shifting drug supply using comprehensive, multi-modality methods. Our research suggests that DBS may add to the robustness of existing drug-checking and xylazine surveillance systems in clinical and community-based settings.
This analysis is subject to some limitations. We did not quantify the concentration of xylazine in a given sample, which has been identified as an important area of ongoing and future research. 20 RAPIDS participants may differ from other populations of people who use drugs, and results from this study may not be generalizable to other contexts. Results may not be generalizable to non-English-speaking people in the United States, including those of Hispanic/Latino ethnicity. Also, the number of DBS samples tested in 2023 was fewer than those tested in previous years; it is unclear if this difference would skew results and, if so, in what direction. Lastly, those who agreed to DBS testing differed by some sociodemographic and substance use–related characteristics (less likely to be homeless and less likely to regularly use fentanyl) compared with the broader RAPIDS cohort, since only participants recruited through a fixed study site were eligible to provide DBS samples (Supplemental Table 1). Despite these limitations, our study contributes meaningfully to the growing body of evidence documenting the presence of xylazine in unregulated drug supplies and characterizing those most likely to test positive for xylazine.
Conclusions
DBS may be a useful tool to add to surveillance testing, especially in the context of an unregulated and rapidly changing drug market and fentanyl use. Given the heightened prevalence of co-occurring xylazine and fentanyl exposure among participants engaged with OAT in this study, our findings support expanding interventions that mitigate the effects of xylazine exposure (eg, drug checking, wound care) within the service settings that reach people who use fentanyl, such as syringe service programs and OAT programs.
Supplemental Material
sj-docx-1-saj-10.1177_29767342261450958 – Supplemental material for Documenting the Emergence of Xylazine Among People Who Use Drugs in Rhode Island: An Analysis of Dried Blood Apot Samples
Supplemental material, sj-docx-1-saj-10.1177_29767342261450958 for Documenting the Emergence of Xylazine Among People Who Use Drugs in Rhode Island: An Analysis of Dried Blood Apot Samples by Leah C. Shaw, Carolyn J. Park, Jason A. Scott, Mary C. Figgatt, Jacqueline E. Goldman, Brendan Jacka, Brandon D. L. Marshall, Adina Badea and Alexandria Macmadu in Substance Use & Addiction Journal
Footnotes
Acknowledgements
The authors would like to acknowledge the RAPIDS participants for their interest and participation in the study. Additionally, the authors would like to thank their RAPIDS researchers, students, and staff, both past and present, including Andrew Gould, Carolyn Park, Cathy Lenox, Esha Sridhar, Esther Moon, Evelyn Lai, Julia Trombley, Michael Tan, Roxxanne Newman, Sari Greene, Tania Lobo Paz, and Tayla Giguere.
ORCID iDs
Ethical Considerations
Ethics approval was obtained from the Brown University Institutional Review Board.
Consent to Participate
Verbal consent was obtained at the start of pre-screening for eligibility, and e-signed written informed consent was obtained at the start of baseline assessment for eligible participants. All participants were offered a copy of the e-signed informed consent via e-mail. All participants were given detailed explanations of their rights as human subjects.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The RAPIDS project is supported by the US National Institute on Drug Abuse [R01-DA0347975] and an administrative supplement [R01-DA047975-02S1]. Dr. Macmadu is supported by the Center for Biomedical Research Excellence (COBRE) on Opioids and Overdose at the Rhode Island Hospital, funded by the National Institute of General Medical Sciences [P20-GM125507], and the Collaborative Justice-Involved Research and Training (CJRT) Program on Substance Use and HIV at Brown University Health, funded by the National Institute on Drug Abuse [R25-DA037190].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Reasonable requests for data will be considered by the corresponding author. De-identified data may be provided as long as there are continued protections for anonymity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.