
Abstract
Background:
Hospitalization presents a critical juncture to engage patients with opioid use disorder, but safety net hospitals are less likely to offer transitional opioid programs (TOPs), which initiate treatment and connect patients to care after discharge. This study explored determinants of TOP adoption in 4 diverse safety net health systems.
Methods:
We interviewed key participants affiliated with safety net health systems and partner community-based organizations about TOPs within their organization. We used inductive coding informed by grounded theory to identify emerging themes related to TOP implementation and thematic analysis to compare determinants across health systems. A deductive approach was then used to map data that aligned with an existing TOP typology to document the presence of specific programs and promote comparison in implementation progress across sites. Throughout the iterative process, we developed analytic themes related to the extent to which TOPs were integrated into each health system. Finally, determinants were mapped to Consolidated Framework for Implementation Science Research domains.
Results:
Determinants spanned inner and outer setting domains and shaped the presence of TOPs and their integration into routine health system operations. The number and types of care transition models varied across organizations. We grouped health systems into 2 patterns, foundational and embedded, reflecting differences in how their TOPs were organized and supported. Reimbursement rates, inefficient organizational functioning, and stigma hindered TOPs at all phases of implementation, while organizational champions were key facilitators. Foundational programs experienced severe staffing shortages and low organizational support. Embedded programs were distinguished by grant-writing staff and more supportive outer contexts.
Conclusions:
This study highlights the challenges and opportunities faced by safety net health systems in implementing TOPs. The findings emphasize the need for tailored implementation strategies that address the unique barriers and leverage facilitators within resource-constrained settings, particularly at different phases of implementation.
Keywords
Highlights
Safety net health systems experienced barriers and facilitators to the implementation of transitional opioid programs (TOPs) differently based on size, regional location, organizational context, and implementation phase.
Organizations with a comprehensive menu of TOPs may lose evidence-based interventions or struggle to scale them without implementation support.
Organizations with fewer TOPs may need more support to implement TOPs successfully in the face of inner and outer setting challenges.
Implementation support is critical at all phases of implementation for TOPs in safety net hospitals.
Introduction
Individuals with opioid use disorder (OUD) are at elevated risk of not only overdose-related mortality, but significant morbidities, including overdose 1 and infectious disease related to injection drug use2,3 that result in hospitalization. Hospitalization is a critical window to initiate treatment, as fewer than 30% of patients hospitalized for injection drug use–related infections are on medications for OUD (MOUD). 4 There are also persistent socioeconomic and racial/ethnic disparities in access to MOUD5-7; hospitalization is an opportunity to expand access to evidence-based care for people with OUD.
To initiate care, some hospitals have established transitional opioid programs (TOPs), 8 which are comprehensive addiction treatment models that initiate care during a hospital stay and extend treatment post-discharge through coordinated referrals. 9 TOPs focus on assessment, initiation of MOUD, patient education, care coordination, and linkage after discharge rather than functioning as residential step-down programs. 8 TOP service eligibility varies across health systems, but generally includes patients hospitalized with OUD, or OUD complications such as injection-related infections.8,10 There is no standard definition of a TOP, but a recent systematic review 9 identified 7 components that are often part of TOPs: (1) Protocol Implementation; (2) Screening, Brief Intervention, and Referral to Treatment (SBIRT); (3) Pharmacotherapy; (4) Addiction Consult Services; (5) Intensive Case Management; (6) Recovery Coaching; and (7) Patient Navigation. TOPs have demonstrated success in reducing hospital visits and readmission rates for patients with OUD, 11 retaining patients on MOUD after discharge, 12 and reducing opioid-related morbidity and mortality. 13
Despite their demonstrated effectiveness, TOPs are not uniformly available in hospitals, especially in safety net settings. Common barriers to TOP adoption include unstable funding, 14 understaffing, 15 stigma, 16 and a lack of standardized workflows. 17 TOPs are most often in large, academic medical centers.18,19 Safety net hospital organizations have smaller operating margins and resource constraints, which make TOPs more challenging to implement.20,21 TOP adoption has been frequently studied in high resource and urban settings, but less is known about the implementation of TOPs in safety net hospital settings.14,22-25 Safety net hospital organizations are an essential setting to embed services for OUD because they disproportionately serve minoritized patients and people with Medicaid insurance.26-28 Low TOP adoption within safety net settings exacerbates disparities in MOUD access5,29,30 and access to community-based addiction treatment post-discharge.31,32
To better understand implementation gaps within safety net hospitals, this study explored the extent to which there are unique determinants of TOP implementation in these settings. In addition, building on the Exploration, Preparation, Implementation, and Sustainment (EPIS) framework, 33 which characterizes aspects of the implementation process, we assessed whether determinants of TOPs varied across safety net health systems in different phases of implementation. This study contributes to the development of tailored implementation strategies that may enhance the adoption and long-term sustainment of TOPs in resource-limited settings.
Methods
Conceptual Framework
This study was informed by 2 implementation science frameworks: EPIS and the Consolidated Framework for Implementation Science Research (CFIR). EPIS provides a conceptual structure for understanding how determinants operate across different implementation phases, highlighting the importance of tailoring support for different stages of the implementation process. 33 EPIS guided our comparison of TOP determinants across health systems in different phases of implementation. CFIR, a related framework, offers a commonly used taxonomy of determinants across multiple domains, 34 helping to situate our findings within the existing implementation science literature. Together, these frameworks informed how we conceptualized and interpreted variation in determinants across 4 safety net health systems.
Study Population
Qualitative interviews were conducted via Zoom with key participants affiliated with 4 safety net health systems in New York City (System A), Chicago (System C), and 2 rural regions of Ohio (Systems B and D). Given significant variation in safety net hospital definition, 35 we defined safety net hospitals as hospitals that are either included in America’s Essential Hospitals, an organization of urban and rural safety net health systems 36 or were categorized as a critical access hospital, a designation used for extremely small rural hospitals, by the American Hospital Association. 37 Health systems were selected based on diversity in size (small <100 beds, medium = 100-499 beds, and large >500 beds) as defined by the American Hospital Association. 38 We also included health systems in both urban and rural locations, a mix of private nonprofit and public hospital systems, and we included organizations with a varying amount of implemented TOPs. We selected interprofessional health system staff using a purposive sampling approach, 39 prioritizing roles with first-hand knowledge about TOPs. Participants included hospital staff, upper management, and clinicians working in the emergency department or in more specialized behavioral health or addiction medicine roles. Participants were also recruited from community-based organizations (CBOs) that partnered with health systems for treatment or harm reduction. After conducting interviews with health system–based informants, we utilized a snowball sampling approach, 40 asking participants to provider contacts (names and e-mail addresses) at partner CBOs. We contacted all informants by e-mail to request participation and continued recruiting until theoretical saturation was reached.
Data Collection
Trained interviewers (C.F., A.Y.L., J.E.C., B.F., Z.L.) conducted in-depth, semi-structured interviews. The interview guide was created by the study team and assessed barriers to TOP implementation common in the literature14-17 and identified in preliminary studies by the study team using a national sample of safety net hospitals. 41 Topics covered included the history of TOP implementation in the organization, barriers, and facilitators unique to the health system, organizational support for TOPs, and the role that external partnerships with CBOs play in implementation. Each interview was conducted via Zoom by at least 2 members of the study team using a standardized interview guide. A modified version of the interview guide was used with community partners that focused on their relationship with the participating health system. Interviews lasted between 30 and 60 minutes and were audio-recorded. Participants were compensated with a $50 Amazon gift card. All participants provided verbal informed consent prior to participation, and all study procedures were reviewed and approved by the Ohio University Institutional Review Board.
Analytic Approach
Audio files were professionally transcribed and analyzed using the web-based data analysis software, Dedoose Version 9.0 (SocioCultural Research Consultants, LLC). 42 We used an iterative, team-based approach that combined inductive constructivist grounded theory 43 techniques with theoretically informed comparative analysis. Two experienced qualitative analysts (C.F., Z.L.) conducted open coding to develop an initial codebook, which was refined through additional coding. To ensure intercoder reliability, C.F. and Z.L. independently coded randomly selected transcripts and reviewed the codebook to address any inconsistencies in coding and use of the codebook. Once coding inconsistences were resolved, all transcripts were individually coded line-by-line. The analysts used a 3-part process: creating initial codes, establishing relationships between codes, and constructing themes related to the determinants of TOP implementation. During this phase, themes related to the determinants of TOP implementation emerged organically through participants’ descriptions of organizational practices. Using thematic analysis, we examined how these determinants manifested across health systems and compared patterns across sites. Determinants that appeared across multiple systems were grouped as common, while those present in only 1 system were grouped as unique. This step was informed by EPIS, which helped to sensitize our analysis to variation in implementation determinants across different implementation phases, such as health systems that were in the early phases of adopting TOPs and those that had a more robust set of longstanding TOPs in place. 33
Following the inductive coding process, we used a deductive approach to group qualitative data that aligned with 7 components from an existing TOP typology. 9 This step helped us to contextualize how the TOPs at each health system was compared with previously documented TOP models. Specifically, we assessed the extent to which each site had implemented different TOP components and used the 7 categories as sensitizing concepts 43 to promote comparison in implementation progress across the 4 sites. Throughout this iterative process, we developed analytic themes related to the extent to which TOPs were integrated into each organization. These patterns emerged inductively but were interpreted using the EPIS framework. Finally, determinants were mapped to CFIR domains to better understand the different implementation contexts in which determinants operated and must be addressed. CFIR mapping occurred after primary themes were already established to help situate findings within the broader implementation science literature. Consistent with CFIR, determinants of TOP implementation were organized by outer and inner setting domains (see Table S2). The outer setting refers to macro-level environments, such as policies, cultural attitudes, or economic factors that shape implementation. The inner setting refers to specific organizational environment where implementation occurs and reflects characteristics of the implementing organization such as available resources and culture. A Consolidated Criteria for Reporting Qualitative Research (COREQ) 44 checklist is available for this study (see Table S1).
Results
Participant Characteristics
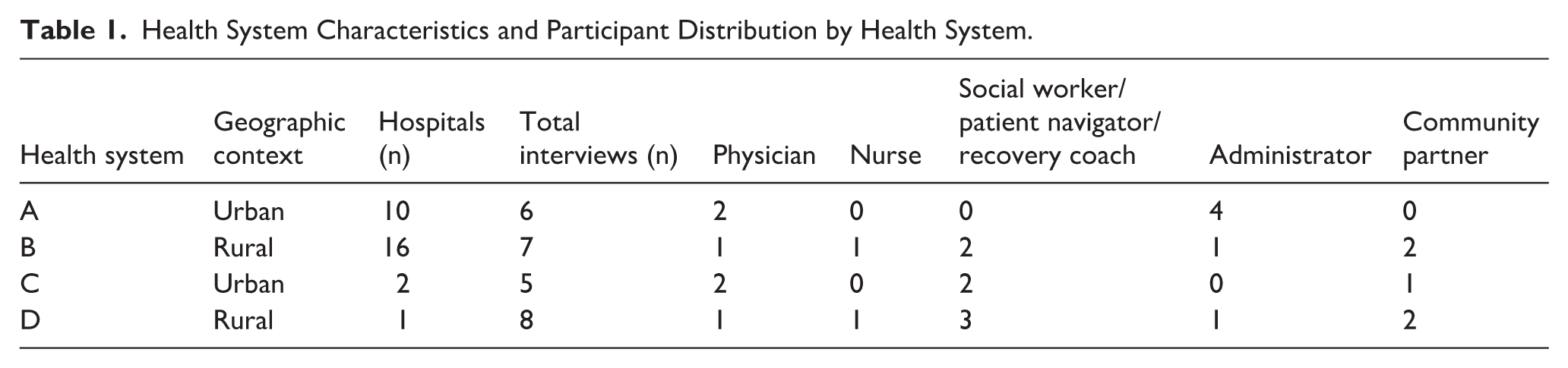
Twenty-six participants (Table 1) affiliated with 4 safety net health systems and partner CBOs participated in in-depth interviews. Approximately 19% of participants were from CBOs (n = 5) and 81% (n = 21) were health system employees. Among the health system staff, 6 participants were physicians, 7 were social workers, patient navigators, or recovery coaches, 2 were nurses, and 5 held primarily administrative roles. Among community partners, 2 worked for county mental health and addiction boards, 2 held leadership positions at local substance use treatment organizations, and 1 was a county health commissioner. Approximately 69% of participants (n = 18) identified as female and 31% identified as male. Most participants (65%, n = 17) held leadership roles within hospitals. Roughly 58% of participants (n = 15) worked in rural regions.
Health System Characteristics and Participant Distribution by Health System.
TOP Components and Implementation Patterns
The presence and types of care transition models varied widely across safety net health systems (Table 2). The only TOP component adopted across all 4 health systems was SBIRT.
Hospital-Based Transitional Opioid Programs by Health System.
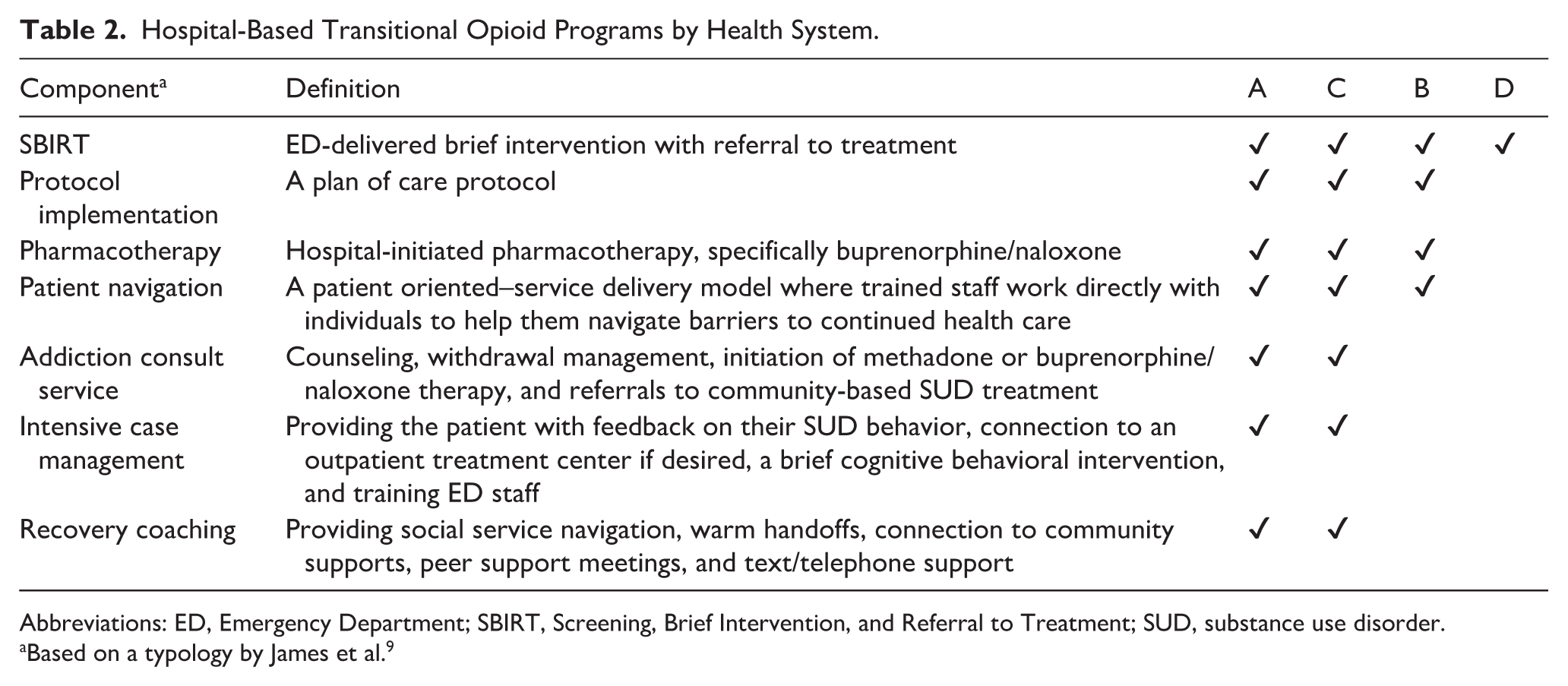
Abbreviations: ED, Emergency Department; SBIRT, Screening, Brief Intervention, and Referral to Treatment; SUD, substance use disorder.
Based on a typology by James et al. 9
Cross-site comparison provided additional context about the TOPs at each health system and revealed 2 distinct patterns, in how TOPS were organized and supported. Health Systems B and D were in the foundational pattern, characterized by gaps in basic addiction treatment infrastructure, limited human resources, and low organizational support for TOPs. These systems relied heavily on limited, often individual-driven efforts, and addiction treatment was not widely integrated into the organization. Health Systems A and C were in the embedded pattern, characterized by the presence of basic addiction treatment infrastructure, which was supplemented by more dedicated resources and supportive local political environments which helped them to adequately fund and expand their TOPs (Table 3). Determinants across these 2 patterns spanned inner and outer setting constructs but most fell within the inner setting domain.
Quotes Illustrating Differences in Determinants Among Safety Net Health Systems in the Foundational versus Embedded Pattern for TOPs.
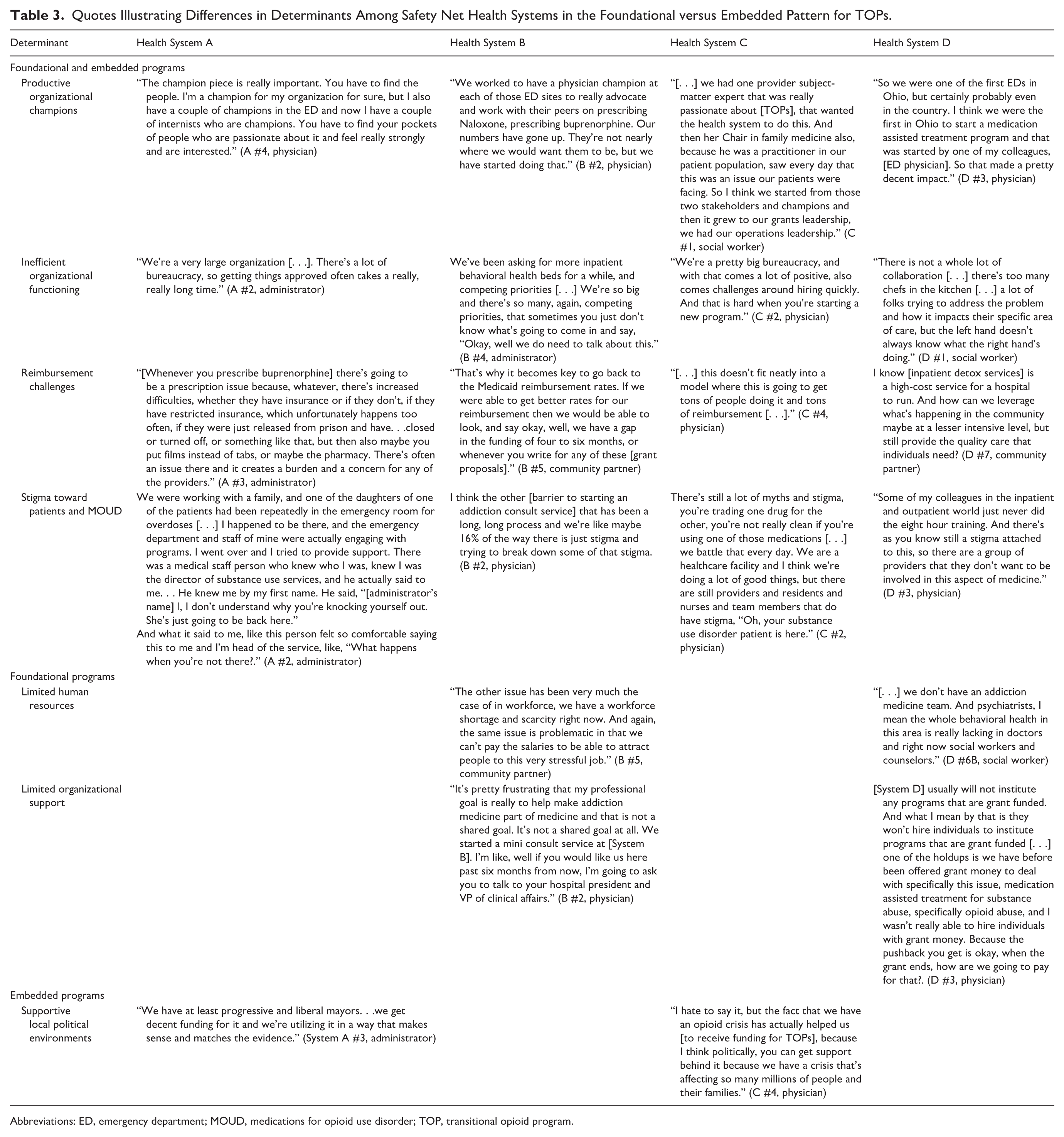
Abbreviations: ED, emergency department; MOUD, medications for opioid use disorder; TOP, transitional opioid program.
Determinants of TOP Adoption That Are Common to Both Foundational and Embedded Implementation Patterns
Productive Organizational Champions
Organizational champions were key facilitators to TOP adoption at organizations in both implementation patterns. Health systems in the embedded pattern had well-organized staff champions which they credited for TOP implementation success. Clinical champions often partnered with grant-writing staff to identify and capture alternative funding sources for TOPs. An emergency medicine physician described what it took to receive an innovative grant that allowed their organization to offer an ED-based fentanyl screening program that automatically notifies recovery coaches: She wrote these grants for the system, so I think actually someone in a system like ours recognizing these opportunities were out there. The fentanyl thing, we just dreamed that idea up, so they went for it. . . The other people that are key. . .it’s also the whole grants management team. . . (System C #4, physician)
Organizations in the foundational pattern had fewer staff champions and champions often worked alone or with little support from leadership. However, the champions’ work remained critical. Two patient navigators at Health System B were determined to prove to organizational leaders that reduced ED admissions save money. One of them explained this perspective: Our positions, we don’t bring any money in. As of right now, the way to help revenue would be to keep people from coming back through the ED to reduce those frequent visits. . .helping them find housing, hooking them up with agencies. . .We give homeless referrals, food. . . tonight we’re going to a counseling meeting in [redacted] to let them know what we do. . . (System B #1, patient navigator)
Organizational champions were critical in both implementation patterns and helped to address funding limitations as safety net health systems worked to implement TOPs.
Poor Organizational Functioning
Despite successfully adopting TOPS, organizations in the embedded pattern were prone to work infrastructure barriers related to their size. Centralization of processes, including the need for many “sign offs,” and delayed approval for existing TOPs made it challenging to implement new programs, especially when the implementation of TOPs required interorganizational collaboration. A director of a substance use disorder division at System A described how centralization impacted the implementation of a much-needed program, and how it differed from their time at a smaller organization: We instituted a withdrawal program in 2020, and it required getting DEA (Drug Enforcement Administration) approvals, utilizing certain medications. . . So in addition to all the hospital approvals, there’s pharmacy committees at the central office. There’s the Department of Health. . .It’s been over two years, and we still have not gotten the final approval on something that should have taken a few months. . .I think at a smaller organization with less centralization. . .once you got approval. . .that was pretty much it. (System A #2, administrator)
At organizations in the foundational pattern, informants similarly described poor organizational functioning as a daily challenge. Respondents faced organizational barriers when hiring new staff or sharing data between providers. A behavioral health services manager at System D explained how bureaucracy and a lack of collaboration made it difficult to access the data necessary for estimating the impact of services: “The data sharing. . .And then the follow-up. . .nobody wants to share follow up information. Even just numbers, basic numbers. . .” (System D #6B, social worker). Long wait times for new hires and programs to be approved plagued organizations in both patterns of implementation, but organizations in the embedded pattern managed to implement TOPs despite organizational complexity.
Reimbursement Challenges
Inadequate reimbursement rates were a critical barrier to TOP implementation within safety net health systems in all patterns of implementation. A CBO leader and partner of System B shared their perspective: The current trajectory for our area is very much along the lines for the state in that overdose deaths are absolutely problematic. . .I think the issues deal a lot with funding. The support services that people need to decrease overdose deaths aren’t properly funded. The Medicaid reimbursement rates are inadequate and most of the people in our area have Medicaid. (System B #5, community partner)
Respondents described “working against” the fee for service model, which still predominates. An emergency department director at System C felt that in the absence of adequate reimbursement rates, having a supportive community and strong public health system was imperative. One solution, the director offered, was “baking in” funding for TOPs at the local and organizational levels: We cannot rely on soft money to do this. These things have to be baked into the way we do it. If we expect pharma and reimbursement to pay for this, it’s just not going to happen. I think government does have to step in and pay for it. . .the people that need it are not the people with a lot of resources. The recovery coaches. . .there’s never going to be a good fee for service on that. This is where public health has to be funded and empowered. . . (System C #4, physician)
At System A, a number of TOPs were internally funded by the organization. Reimbursement rates were not a significant issue because the organization had dedicated funding to TOPs, as 1 participant explained: Yeah, we’re not grant-dependent at all, and this is all programmatic that’s embedded within the funding for [System A] and our usual salaries. . .we don’t have to worry that it’s going to go away at any time. (Healthy System A #5, physician)
Although 1 health system managed to implement TOPs using internal programmatic funding, inadequate reimbursement caused implementation challenges for TOPS at safety net health systems that aligned with both patterns of implementation. In the absence of adequate reimbursement rates, other sources of funding were critical to implement and sustain TOPs.
Stigma Toward Patients With OUD and MOUD
Across patterns of implementation, participants felt that many of the challenges they faced implementing TOPs were a result of multifaceted stigma. Within each organization, the respondents stated that only some providers were interested in treating patients with OUD. A physician at System B shared that patients with behavioral health and substance use disorders were seen as “expensive,” “difficult to manage,” or “unfixable.” An administrator working in a behavioral health office at System A explained that despite operating robust TOPs, stigma played a major role in keeping addiction care somewhat fragmented: . . .the ideal would be if each hospital had an addiction department that was a little broader in it’s purview and wasn’t just considered this outpatient thing. . .we used to have inpatient detoxes at six or seven of our sites which are no longer in existence. . .my understanding is those were fairly distinct units. . .so there hasn’t been necessarily a larger vision for an addiction department. I think it probably has also something to do with not just stigma of this patient population, but stigma of this genre of medicine in a certain way being A, shunted off to a basement space traditionally or B, well even behavioral health is, there’s a stigma around that . . . (System A #6, administrator)
Respondents also described stigma outside of organizational walls, including at local pharmacies. Some pharmacies would not cooperate with filling MOUD prescriptions. Even when organizations in the embedded pattern were able to initiate medication in the hospital, access was perceived to be limited due to stigma among pharmacists. As part of their role at System C, a recovery coach had to help patients navigate stigmatizing attitudes at local pharmacies: Some of those conversations I used to have with the pharmacist when we’re trying to get to the root of why the patient couldn’t pick up, I feel like it was stigma based. The language that was used. The, hmm, you could just go to another Walgreens, no sense of urgency that you have this patient in front of you, and they need their medication now. (System C #3, recovery coach)
Organizations in the foundational pattern described similar experiences of stigma from local pharmacies, which was particularly challenging for rural communities with limited options. A respondent from System B described this frustrating experience: “the local pharmacies kind of make up their own rules about that. They’re not state rules, but they will tell you, oh, we’re at capacity for our buprenorphine patients. . .” (System B #2, physician). Negative attitudes toward patients with OUD within the organization and negative perceptions of MOUD in the broader community hindered TOP implementation and sustainability for organizations across implementation patterns.
Determinants of TOP Adoption That Are Unique to the Foundational Pattern
Limited Human Resources
Participants from organizations in the foundational pattern noted that recruiting and maintaining adequate staff for TOPs was difficult. Without sufficient internal funding, organizations relied on grants to hire crucial staff, such as ED-based social workers, leading to inconsistent staffing. The ED director at System D explained: One of the concerns with grant money is it will only go so far. . .that social worker we have, we probably need multiple social workers. And right now that’s one of the holdups is we can’t afford a second or third or a fourth person. . .even with grant money, they won’t let me hire someone because. . .if the grant money goes away, we’re stuck with this full-time equivalent person. (System D #3, physician)
Even if funding was sufficient, organizations in the foundational pattern also faced challenges recruiting other key positions, such as full-time addiction medicine specialists and psychiatrists, which were essential for developing and maintaining TOPs. For example, a unit director at System B explained: We just expanded our behavioral health ED and bedside consults there a little bit ago. . .We couldn’t hire people to live in those areas, and you can’t hire a full-time addiction person to live in [redacted] County to see one patient a week. (System B #4, administrator)
Insufficient funding and inconsistent staffing of TOPs weakened the ability of organizations in the foundational pattern to offer even the most basic evidence-based resources like take-home naloxone. An addiction medicine specialist at System B described the lack of funding and staffing: When we look at the naloxone prescribing, it peaked, but when we had to let people go, we see those numbers trending back down. And so it’s just unfortunate that to be honest, navigators aren’t very expensive from a health system perspective, but we don’t seem to have the drive to pay for them. (System B #2, physician)
Human resource challenges were not actively cited as an acute barrier by organizations in the embedded pattern.
Limited Organizational Support
There was limited support for expanding TOPs at organizations in the foundational pattern. Since these organizations already experienced resource deficits, TOPs were threatened by competing priorities. Limited organizational support for TOPs impeded efforts to obtain funding for new and existing TOPs, or for nonclinical staff that served in peer support or SUD navigator roles. A unit director at System B explained: They [peers and navigators] are very helpful to the attendings, and the non-behavioral health substance use disorder clinicians in the ED are thrilled to have that support. But it doesn’t always translate to FTEs on the budget. . . (System B #4, administrator)
The ED director at System D described the difficulty prioritizing OUD treatment: “Everyone’s fighting for those few dollars and looking at this population, they’re unfortunately usually not at the top of that conversation” (System D #3, physician). Limited organizational support for TOPs was unique to organizations in the foundational pattern and threatened sustainment of existing TOPs.
Determinants of TOP Adoption That Are Unique to the Embedded Implementation Pattern
Supportive Local Political Environments
Organizations in the embedded pattern felt supported by their communities and local government organizations as they were in cities and states with funding allocated for substance use treatment. An administrator at System A explained: . . .given the funding we received. . .to kind of pilot, but it was larger than a pilot because it was giving us money to do six of them, we used that money and the political moment to strong arm all of the hospitals into creating these programs. From a central office perspective, we very much created a support system to do that and several administrators to work and build those programs. (System A #6, administrator)
Similarly, the respondents from System C felt that local political support for opioid treatment resources and programs was high. As 1 physician described: We did work with policy makers and government, and I think that those conversations were critical. I think that the governmental folks we spoke to were very sympathetic, and then kind of walking them through the language of what we needed fixed to get our work done was really key. Also, focusing them so that they would appropriate funds in the right direction. (System C #4, physician)
Local economic and political conditions were a facilitator of TOP implementation and expansion for organizations in the embedded pattern, but organizations in the foundation pattern were not supported by these same conditions.
Discussion
Safety net health systems face complex challenges as they disproportionately care for uninsured patients and those covered by public insurance. 35 Interviews with key informants provided insight into TOP implementation across 4 safety net health systems. Two distinct implementation patterns emerged that demonstrated meaningful variation in how TOPs were organized and supported; foundational programs, characterized by gaps in basic addiction treatment infrastructure, struggled to implement and sustain TOPs, while embedded programs harnessed dedicated resources to strengthen and enhance existing programs. Although TOP components varied across the 4 systems, implementation was shaped less by program components and more by inner setting conditions. Informants described a range of determinants, which were largely organizational in nature, highlighting the inner setting context as a key driver of TOP implementation among safety net health systems.
Across implementation patterns, shared barriers included inner setting factors such as multifaceted stigma and complex organizational processes that prevented adoption. We found that even health systems with robust TOPs still cited stigma as a barrier to maintaining or expanding these programs. At foundational programs, stigma was pronounced at the community level, as well as among organizational leaders and individual clinicians. Negative attitudes limited the number of clinicians willing to support TOPs, which worsened workforce challenges. Within embedded programs, stigma was felt most acutely among individual clinicians, which threatened long-term stability of TOPs. Other inner setting barriers were unique to organizations in the foundational pattern. For example, severe internal resource deficits and critical staffing shortages made it difficult to prepare for and implement TOPs. These barriers sometimes led to inconsistent service availability for TOPs, further limiting their integration into health system operations.
While these barriers overlap with barriers identified in other hospital settings, they are likely exacerbated in rural safety net settings and may help explain disparities in TOP access within safety net hospitals as compared to other hospital settings in the United States 41 and within rural communities. 19 The literature consistently highlights stigma14,45 and unstable funding streams, 46 which were evident across the health systems in our sample, but studies focused on safety net settings document barriers that exacerbate these challenges, such as staffing shortages, workload burden, constrained referral networks.15,16 In the context of constrained resources and nimble staffing models characteristic of safety net settings, it is unsurprising that organizational champions emerged as a crucial inner setting determinant for all safety net health systems. At embedded programs, champions were essential to seeking supplemental funding to implement and sustain TOPs and worked to address stigma within the organization. At foundational programs, champions worked to implement basic addiction treatment infrastructure, such as SBIRT and naloxone distribution, but struggled to build additional TOPs without better funding, adequate staff, and organizational support. Previous studies have also identified organizational champions as especially important for reducing stigma related to addiction treatment within hospital settings.14,47,48
The fact that safety net healthy systems have diverse implementation challenges is important for designing and testing implementation strategies to support access to TOPs. Importantly, our findings suggest that determinants of TOP adoption in safety net settings may be concentrated within the inner setting. External policies and incentives within the outer setting (eg, local political context, external funding sources) influenced TOP implementation, and even proved helpful for embedded programs, but these factors were still mediated by inefficient organizational functioning and internal stigma. Safety net organizations who have already implemented a comprehensive menu of TOPs may be at risk of losing evidence-based interventions or may face challenges without implementation support. 49 Organizations with fewer TOPs need more targeted support in the face of outer context factors such as limited community support and workforce shortages. These organizations may benefit from strategies focused on the pre-implementation phase. 50
Implementation support should be tailored to the diverse organizational contexts of safety net health systems, but TOPs at all phases of implementation could benefit from improved reimbursement rates for OUD treatment.51,52 In resource-constrained settings, inadequate funding for addiction treatment makes it challenging to adopt and sustain TOPs. Especially in the context of stigma, greater financial incentives for offering evidence-based TOPs may improve implementation and sustainment. Stigma reduction at the organizational level and strategies specifically focused on leadership engagement are also important at all phases of implementation. For less developed programs, policies that provide funding for dedicated addiction medicine staff may help to address barriers related to staffing and service availability. Participants also described challenges recruiting staff to work in rural areas. Incorporating telehealth may address this barrier by enabling psychiatry and addiction medicine providers to offer substance use disorder services remotely, 53 expanding the number of providers who can potentially support TOP implementation in areas where recruiting local staff is difficult. Embedded programs had successfully adopted TOPs in part because they were able to leverage their existing human and material resources to obtain grant funding to maintain service continuity. Continued local and state funding mechanisms would help to sustain TOPs at these organizations. Smaller, rural hospitals would benefit the most from increased reimbursement rates and targeted policies to support TOP access.
Qualitative interviews provided rich data on experiences implementing TOPs within safety net organizations. However, our study does not include the perspectives of safety net organizations in the Southern or Western regions of the United States, and our study design does not allow for generalization of these findings to all safety net organizations in the United States. Future studies should assess whether similar determinants of TOP implementation translate to other safety net organizations. We conducted in-depth interviews with hospital administrators, clinicians, staff, and CBOs, but did not include patients with OUD in interviews. Future studies should consider end users as research participants to better understand patient experiences and access barriers within safety net hospitals. Our study identified important determinants of TOP adoption across different safety net settings, which is a critical first step to designing tailored implementation support. Future work should test the impact of implementation strategies on TOP adoption and reach within safety net health systems.
Conclusion
Fewer settings are more important than hospitals to engage patients with OUD and facilitate linkages to care.3,4,8,11,32,47,54-57 Our findings suggest that safety net health systems experience implementation barriers and facilitators differently based on their size, regional location, and stage of implementation. To improve access to these evidence-based programs for OUD, implementation strategies are necessary at all phases of implementation, to support successful adoption of programs and to sustain and scale-up programs already in place.
Supplemental Material
sj-docx-1-saj-10.1177_29767342261451111 – Supplemental material for Determinants of Implementation and Sustainability of Transitional Opioid Programs Within Rural and Urban Safety Net Hospitals
Supplemental material, sj-docx-1-saj-10.1177_29767342261451111 for Determinants of Implementation and Sustainability of Transitional Opioid Programs Within Rural and Urban Safety Net Hospitals by Cheyenne Fenstemaker, Alden Yuanhong Lai, Ji Eun Chang, José A. Pagán, Zoe Lindenfeld, Cory E. Cronin and Berkeley Franz in Substance Use & Addiction Journal
Supplemental Material
sj-docx-2-saj-10.1177_29767342261451111 – Supplemental material for Determinants of Implementation and Sustainability of Transitional Opioid Programs Within Rural and Urban Safety Net Hospitals
Supplemental material, sj-docx-2-saj-10.1177_29767342261451111 for Determinants of Implementation and Sustainability of Transitional Opioid Programs Within Rural and Urban Safety Net Hospitals by Cheyenne Fenstemaker, Alden Yuanhong Lai, Ji Eun Chang, José A. Pagán, Zoe Lindenfeld, Cory E. Cronin and Berkeley Franz in Substance Use & Addiction Journal
Footnotes
Ethical Considerations
All study procedures were reviewed and approved by the Ohio University Institutional Review Board.
Consent to Participate
All participants provided verbal informed consent prior to participation.
Author Contributions
All authors study design and conceptualization. CF, AYL, JAP, JEC, CEC, and BF original draft, reviewing, editing. AYL, BF, CF, and ZL methodology. CF and ZL formal data analysis. CF and BF led the manuscript writing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Clinical Trial Planning Grant from the National Institute on Drug Abuse (grant R34DA055228).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
R34 DA057160/DA/NIDA NIH HHS/United States.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.