
Abstract
Background:
Undergraduate medical education is increasingly incorporating harm reduction (HR). Assessments of HR curricula have focused on skills like overdose reversal. The literature lacks evaluations of curricula that more broadly teach HR-based physician-patient communication.
Methods:
From academic years 2022 to 2024, a Harvard Medical School student working group collaborated with faculty to take a quality improvement approach to incorporating HR into the substance use interview curriculum. We implemented two Plan-Do-Study-Act cycles. We measured the effectiveness of HR education in the 2023 Substance Use interview session by surveying students on a 5-point Likert scale (ranging from 1 = strongly disagree to 5 = strongly agree). We also conducted a focus group with four students to provide qualitative insights into the curriculum’s impact and areas for improvement. We thematically analyzed the focus group session based on Borkan’s Immersion/Crystallization methodology.
Results:
Thirty-three students completed the pre-survey and post-survey (19.4% response rate). In the survey, self-reported HR understanding improved, from mean 3.6 on the Likert scale to 4.2 (P < .001). Students strongly agreed with being interested in harm reduction before and after the session (mean pre-survey score: 4.3). In the focus group, students identified patient stories as helpful for improving understanding of HR communication. They expressed difficulty understanding the relationship between HR and abstinence-based approaches like Alcoholics Anonymous and recommended more diverse patient perspectives during the session and more HR exposure throughout medical school.
Conclusion:
A half-day session on the substance use interview showed promise for teaching HR communication principles. For future HR communication curricula, our results favor retaining an emphasis on patient narratives and ensuring representation of diverse patients. Future research can assess whether harm reduction education translates into improved patient care.
Keywords
Highlights
A quality improvement model helped integrate harm reduction into medical school curriculum.
Revised curriculum about the substance use interview was associated with a trend toward improved understanding of harm reduction.
Students perceived patient stories to be effective for learning harm reduction communication.
Introduction
Harm reduction (HR) is an approach to health care that seeks to minimize detrimental effects of behaviors to both individuals and their communities. Facing the HIV epidemic, stigma, and criminalization, people who use substances themselves were the earliest to promote harm reduction as a pragmatic and compassionate approach to substance use. 1 HR seeks to minimize harmful effects from substance use and to promote safer outcomes, without requiring abstinence to access care and services. A growing number of medical schools have started incorporating HR into their curricula.2-7 Yet, the most recent AAMC survey on Addiction Medicine, Substance Use, and Pain Management in Medical School Curricula did not ask institutions about HR education. 8 A recent scoping review and a national survey found that existing HR curricula tend to focus on basic knowledge about substance use and preliminary clinical skills (e.g., recognizing and treating overdose and withdrawal), rather than on HR theory and communication.4,5 That observation applies to the overdose prevention module at our own institution. 7 HR principles, such as respecting patient autonomy, provide physicians with enduring approaches for partnering with patients, even as the drug supply and relevant clinical skills rapidly evolve. What is lacking in the literature is evaluation of a curricular initiative to prepare students with a broader HR approach for communicating with patients about substance use, with emphasis on substance use history taking and clinical interviewing.
In our quality improvement initiative at Harvard Medical School (HMS), a group of medical students collaborated with faculty to incorporate HR principles into the curriculum for first-year students. At HMS, the Practice of Medicine course includes an Interviewing and Communication Skills (ICS) component, which instructs first-year students on the patient interview, including a half-day session devoted to substance use. This quality improvement project sought to increase students’ understanding of HR and their readiness to apply HR principles during patient interviews.
Methods
Context
During the 2022 ICS Substance Use session, HR was a peripheral topic, mentioned by an optional reading and by one panelist physician. By contrast, both the preparatory materials and discussion groups featured members from Alcoholics Anonymous (AA), which has historically promoted abstinence-based recovery and discouraged HR practices. 9 After participating in the session, student authors N.S. and E.L. wished to provide feedback in favor of integrating HR as a core component of the ICS Substance Use curriculum. They organized a meeting with classmates who had backgrounds in substance use care to request their suggestions. Classmates’ experiences included working at harm reduction organizations, working for Hepatitis C prevention programs, working in public health, and volunteering with unhoused individuals. This student working group generated a list of recommendations for the curriculum. N.S. and E.L. then sent these recommendations to faculty authors B.W. and D.K., who proposed working together on revising the 2023 session.
Quality Improvement Design
Our SMART goal was to improve students’ self-reported interest in and readiness to use harm reduction in patient communication after a 1-day session, as measured by changes in Likert scores before and after the session (see Evaluation). Figure 1 summarizes how Plan-Do-Study-Act (PDSA) cycles, a common framework for QI, informed the curriculum revision. In 2022, the “plan” stage was carried out by ICS faculty. The 2022 “study” stage was initiated by a student working group that identified a gap in HR content. For the “act” stage, students shared these findings, and faculty directors invited collaboration on planning the 2023 curriculum. For the 2023 “plan” stage, students and faculty together revised the preparatory materials and in-person content. Changes included making HR the guiding principle for the Substance Use session, encouraging students to attend peer support groups that emphasize HR principles (e.g., SMART Recovery https://smartrecovery.org/about) for the prework assignment, adding a podcast about patient and provider experiences with HR to the preparatory materials, 10 and adding an HR specialist to the panel of addiction providers during the in-person session. Table 1 details changes made to the 2023 ICS Guide. The 2023 “do” stage consisted of required curriculum for 170 first-year medical and dental students, including preparatory materials and a 4-hour in-person session. The “study” stage for the 2023 curriculum is described below in the remainder of the Methods section.
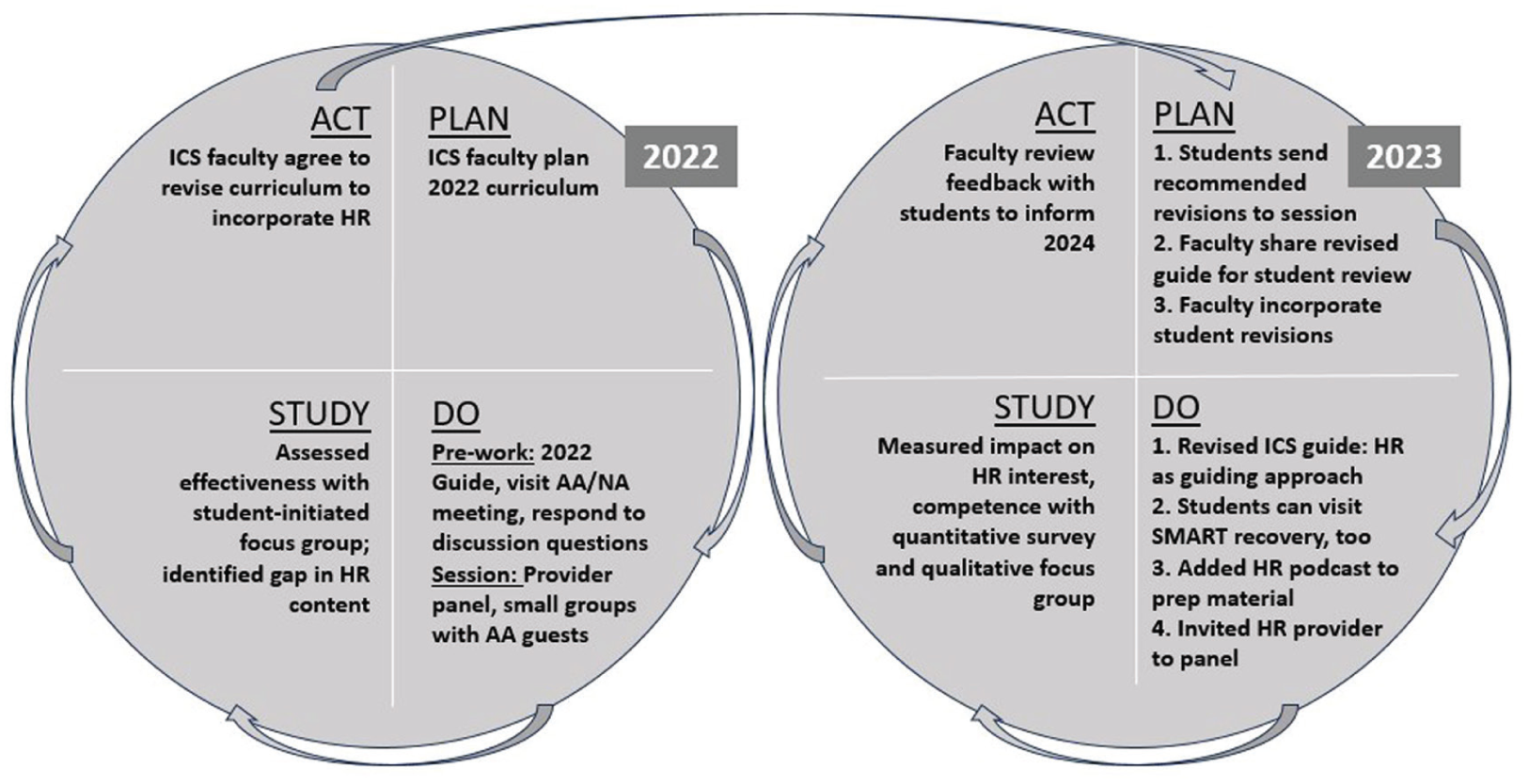
Two Plan-Do-Study-Act Cycles for Quality Improvement of ICS: Substance Use Session.
Examples of Incorporation of Harm Reduction Into the ICS Guide.

Abbreviations: ICS, Interviewing and Communication Skills; AA, Alcoholics Anonymous; HR, harm reduction.
Study Instruments
We collected quantitative and qualitative data to evaluate the revised curriculum’s impact. Survey development was guided by the QI SMART goal and the course learning objectives. The survey aimed to measure students’ attitudes, understanding, and confidence in applying HR principles during patient communication. Items were drafted by the author group, reviewed for clarity by faculty directors, and further refined with feedback from Dr. Hilary Connery, an addiction psychiatrist not involved in the course’s instruction. Due to time constraints, formal pilot testing was not conducted. Instead, the author team conducted an internal review of the survey to ensure it was easy to complete and protected anonymity. The pre-survey and post-survey were collected via Qualtrics.
Both the pre-survey and post-survey contained the items “I have a good understanding of what harm reduction is and the strategies it employs,” “I am interested in harm reduction to inform my clinical work with substance use disorder,” and “I worry that some harm reduction interventions may be harmful for patient care.” Students rated these items using a five-point Likert scale, from strongly disagree (1) to strongly agree (5). Additionally, the post-survey asked students to rank the following session components from least beneficial (1) to most beneficial (5):
“Materials on Canvas and readings for the session” [preparatory readings, podcast, and ICS Guide] (Note: Canvas refers to the course website)
“Attending meeting of AA or other organization”
“Session with the entire class and speakers” [panel discussion]
“ICS tutorial discussion” [discussion with faculty]
“Discussion with speaker visiting ICS group” [speaker with substance use disorder]
The focus group guide consisted of six structured questions. The questions were designed to help elucidate how the curriculum affected students’ learning about harm reduction, what worked well, and what could be improved in the future. Supplemental Appendix 1 contains the survey questions and the focus group guide.
Ethical Considerations and Institutional Review
The Harvard Longwood Campus Institutional Review Board reviewed the QI project and deemed it exempt from full IRB review because it consisted of a curriculum improvement evaluation rather than generalizable research.
To maintain the anonymity of survey responses, students used unique labels for responding to the survey. Students generated these labels based on their hometown and phone number. Focus group facilitators verbally shared information with participants about the focus group’s purpose, voluntary nature, and data security plan. After this, focus group participants provided verbal informed consent. Participation was voluntary and had no impact on course grades or academic standing.
All data were stored securely on institutional servers, accessible only to members of the research team. During transcription of qualitative data, any potentially identifying information was removed to protect participant confidentiality.
Administration and Analysis of Surveys
The pre-survey was available at two time points. First, a link was posted on the course website before the session. Second, course faculty posted a QR code in the amphitheater for five minutes at the beginning of the in-person session. The post-survey was available on the course website as part of the post-session reflection materials. Additionally, course faculty reminded students via e-mail to complete these items by the end of the day.
Likert score means were compared using Wilcoxon rank-sum to measure effect size (R version 4.3.2). This statistical test was selected because we compared non-paired aggregate mean scores, rather than comparing individual students’ pre-post scores. Students were not compensated for participation in the survey or focus group.
Administration and Analysis of Focus Group
Focus group recruitment took place through an e-mail from course faculty and an amphitheater announcement. A convenience sample of four students volunteered to participate the day after the session. Participants provided verbal consent to the recording and analysis of their responses for quality improvement and research. Authors S.I. and I.B., classmates of the focus group participants, facilitated the 45-minute session. Aware of potential social desirability bias, the facilitators emphasized creating a safe space for critique by explicitly mentioning that critical feedback was welcomed and valued. To further mitigate biases, the focus group was conducted as a structured interview with facilitators refraining from contributing to the discussion.
Author N.S. transcribed the recording verbatim. Authors N.S. and S.I. conducted a thematic analysis. The analysis was conducted from a constructivist epistemological stance, acknowledging that students’ perceptions of the HR curriculum are defined through prior individual experiences, social contexts, and exposure to substance use topics. They used Borkan’s Immersion/Crystallization method of analysis, which entails each analyst immersing herself in the text and identifying ideas that crystallize related to the question under study. 14 The analysis used inductive coding, meaning that each analyst labeled the transcript with themes that emerged based on the content of the text, rather than based on a predetermined theoretical framework. These codes (i.e., labels) were organized in a spreadsheet, which also listed supporting quotations. The analysts compared their independent conclusions and arrived at a consensus set of themes. Reflexivity was an active practice in our analysis. We considered the positionality of the two medical student researchers conducting the analysis. One researcher was involved in the design of the curriculum under study, and the second participated in the curriculum but was not involved in its development. These roles can influence data interpretation, such as dampening sensitivity to critical feedback. To help address this, the analysts independently coded the transcripts and then discussed discrepancies until consensus was reached.
Results
Quantitative Results
Of the 170 students who participated in the session, 33 (19.4%) completed both the pre-survey and post-survey. Data were analyzed as pre-aggregate and post-aggregate. Understanding of HR improved following the session, with the pre-survey mean Likert score of 3.58 rising to 4.15 on the post-survey (P < .001; Cohen’s d 0.97). Students’ agreement with the statement “I am interested in using harm reduction” did not change significantly after the session, with a pre-survey mean of 4.36 and a post-survey mean of 4.33 (P = .76). Concern that HR interventions can be harmful decreased from a pre-survey mean of 3.12 to a post-survey mean of 2.70, with the difference approaching statistical significance (P = .071) and demonstrating a moderate effect size (Cohen’s d = −0.47) (Table 2).
Pre-survey and Post-Survey Results Regarding Student Attitudes Via Likert Scale.
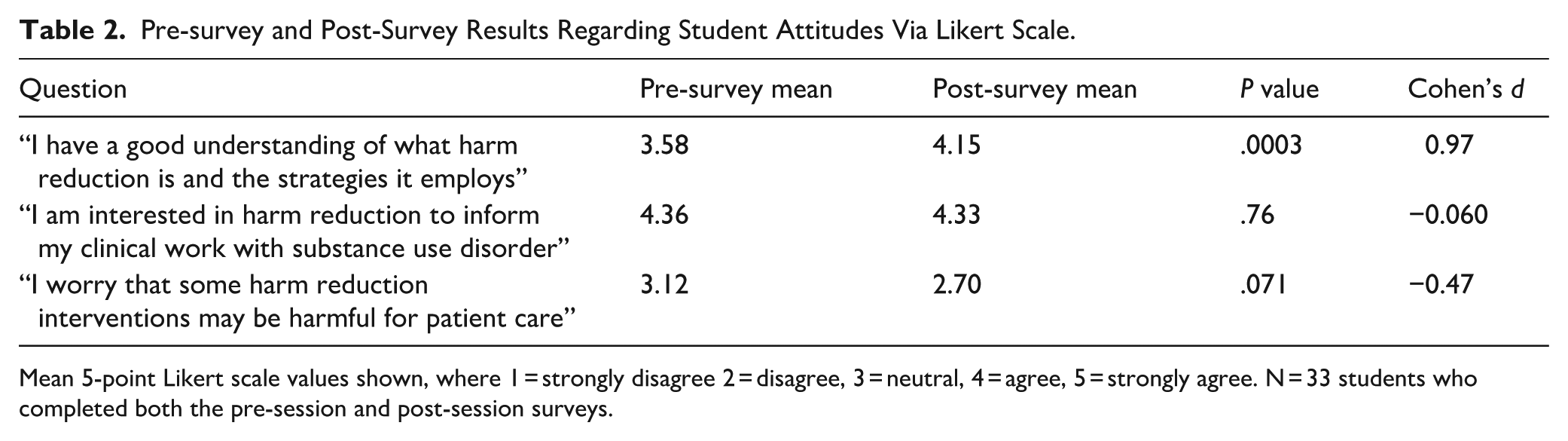
Mean 5-point Likert scale values shown, where 1 = strongly disagree 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree. N = 33 students who completed both the pre-session and post-session surveys.
Students rated the materials on the course website (preparatory readings, podcast, and ICS guide) as most beneficial with a mean score of 4.09, whereas small group discussion with an AA member was seen as less beneficial with a mean score of 1.82. The other components were viewed more neutrally (Table 3).
Survey Results on Helpfulness of Five Curriculum Components.
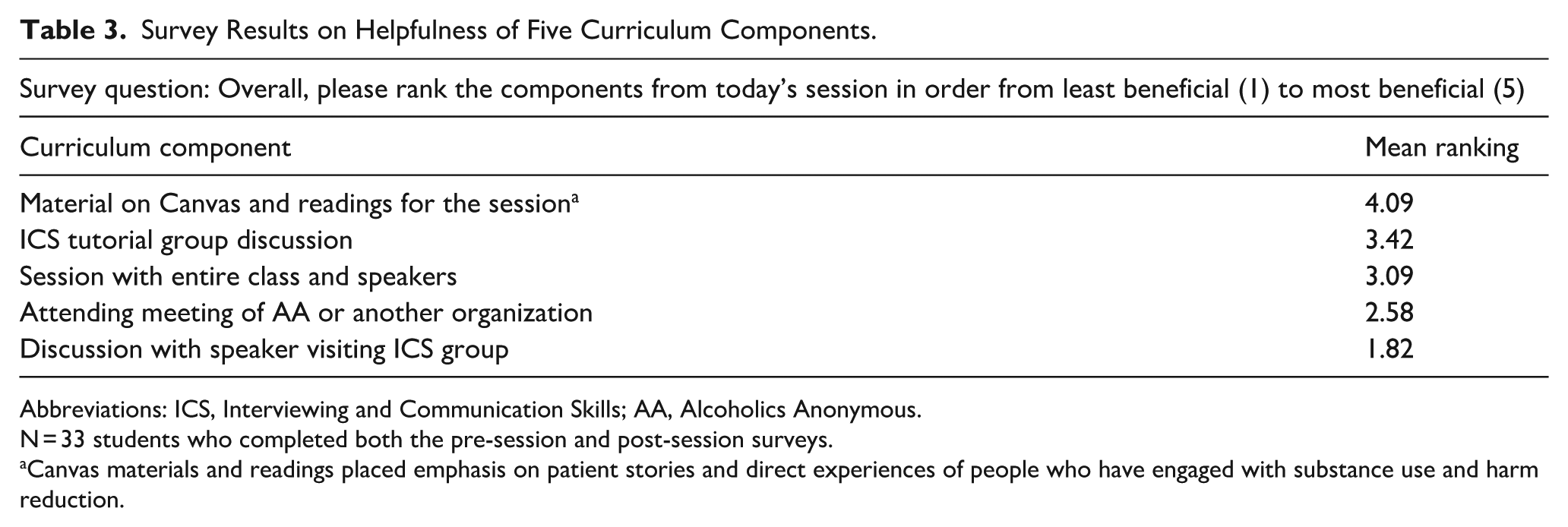
Abbreviations: ICS, Interviewing and Communication Skills; AA, Alcoholics Anonymous.
N = 33 students who completed both the pre-session and post-session surveys.
Canvas materials and readings placed emphasis on patient stories and direct experiences of people who have engaged with substance use and harm reduction.
Qualitative Results
Focus Group Participants
The four focus group students entered the ICS session with pre-existing HR interest. Their confidence in incorporating HR into clinical practice ranged from “something I’ve been very interested in but didn’t know a lot about” to “interested in engaging with harm reduction with any patient.”
Theme 1: Improved Understanding
Students expressed that the ICS session helped improve their understanding of the philosophy behind HR. They described that the emphasis on HR had the effect of “changing the end goal or what we define as success for our patients,” with success now expanding beyond abstinence to include helping patients stay safe and engaged in care:
“Why wouldn’t you get incremental gains in terms of substance use rather than saying [abstinence] is the absolute goal? That really doesn’t work all the time. With our own personal goals, we can see something as too big to achieve and never really strive to get there.”
“It’s more about what the person wants and how they want to get to that point, not what you want for them.”
The session also addressed misconceptions: “Often when we talk to patients or physicians about it, they’d say, ‘Oh I’m worried this is going to cause increased addiction.’. . .It’s cool to see the studies that people presented [supporting HR].”
Theme 2: Increased Interest
Students described that the session increased their interest in incorporating HR into clinical practice. The visit from an HR program director was particularly influential: “That was sort of a different direction than what I’d thought about in the past, which was if I had a patient who had a substance use disorder in any way, how I would engage with harm reduction with them, versus [this new direction focused on] how to use harm reduction to invite more people into clinical care.”
The session especially motivated interest in addressing existing, sometimes subtle barriers to accessing substance use and HR services. They named barriers ranging from delays in dosing methadone in the emergency room to difficulty climbing stairs to get to a bridge clinic.
Theme 3: Patient and Provider Narratives Facilitate Understanding of HR
In the qualitative analysis, too, students identified that the most beneficial components of the session were the stories of real patients and providers navigating substance use and HR.
These stories helped dispel stereotypes: “I personally had some perceptions of what someone with a substance use disorder looks like. I guess I always thought that people with a substance use disorder at an extreme level are not able to keep working. We saw directly that [the patient who visited our small group] was able to continue functioning. It really widened my eyes that people can cope and how difficult it is to identify it in a patient.”
The real-life story in the podcast helped demonstrate a provider speaking with a HR approach: “There was no part of her that was like, ‘You should use less. You shouldn’t use.’. . .If that was even the tiniest bit in her intonation even, there’s a lot of people who would not call.”
Theme 4: Confusion About Relationship Between Abstinence-Based Approaches and Harm Reduction
The curricular components that students described as less helpful—the focus on AA in both prework and small groups, as well as the facilitation of small group discussions—contributed to ambiguity about the relationship between HR and abstinence.
One student summarized: “There was a little bit of confusion created around how to talk about harm reduction in and of itself versus a means to an end of eventual abstinence.”
Students had concerns that AA was overrepresented, given that AA was central to the prework and to the small group 1:1 visits: “I feel like that barrier [to decreasing the stigma around active use and harm reduction] was still not broken by having the patient advocate speakers be all people from Alcoholics Anonymous or other organizations who are all practicing abstinence.”
The other component that students asked to improve was facilitation of the small groups. Students expressed concern that the preparatory discussion questions and the small group discussions framed HR’s utility as open to debate: “We’d just learned about harm reduction and then it was like, ‘Okay you just learned about this thing. What do you think? Is it good?’ I felt like that was a little weird because it’s not like we learn about Tamoxifen and then the homework question is like, ‘We learned about this, and it’s evidence-based. But what do you think personally? Is this a good treatment?’”
Theme 5: More Diversity and Exposure
Students asked for a greater diversity of experience to be represented in the ICS Substance Use session.
“Maybe hearing from a patient or a person who is utilizing those sorts of resources would be great. I also feel like that would be a really valuable way to address the stigma.”
“Diversity based on class, race and ethnicity, cultural background, immigration status, I don’t think was ever mentioned throughout the entirety of the curriculum. . .When someone has a substance use problem and they’re in a high economic status, the way that they’re treated is very very different.”
Overall, students desired more HR exposure throughout their medical education: “I think it would still be hard to get in a conversation with someone who’s pretty anti-harm reduction. I’ve had a lot of conversations like that, and that’s really hard. But I think it also comes with being exposed to it more in the curriculum.”
Discussion
This QI initiative explored the integration of HR principles into HMS’s preclinical curriculum through a PDSA approach. While previous efforts have incorporated HR into medical education, they have primarily focused on substance use knowledge and skills like overdose reversal, withdrawal management, and screening.1,2,4-7 Adding to these efforts, our initiative emphasizes instilling harm reduction principles and developing students’ clinical communication skills. These are foundational steps for effective SUD care, in accordance with Smith et al.’s Harm Reduction Educational Spectrum. 5
Our quantitative evaluation suggests that students developed improved understanding of HR as a guiding principle. Interest in incorporating HR into future clinical practice started and ended high. There was also no statistically significant change in student perception that HR is potentially harmful to patients. The HR preparatory materials and readings were rated most beneficial. These results indicate early progress toward our SMART goal of increasing HR understanding, but not for increasing interest in incorporating HR, given that students’ interest was already high at baseline. The qualitative results provided more insight into the quantitative trends. The focus group conveyed that patient and provider narratives were helpful components of the session for improving understanding of HR and decreasing stigma toward substance use, consistent with previous literature reviews that find patient stories are effective tools for reducing stigma. 13 Reviewing the QI results, in particular the themes from the qualitative analysis, led study authors to identify concrete ideas for continuing to strengthen the HR curriculum in ICS and subsequent courses at HMS:
Reposition AA as one of many ways to find recovery (as opposed to primarily featuring AA during the session); continue to include voices from AA as a common tool for recovery while balancing the AA perspective with guests who take a HR approach.
Invite guests who currently use substances and HR services.
Deepen engagement (via preparatory materials and invited guests) with opportunities to address racial disparities in substance use outcomes through HR, a recommendation echoed by Smith et al. 5
Equip small-group facilitators with deeper understanding of HR, for example, through a preparatory session for faculty, in order to help address confusion about the relationship between HR and abstinence.
Revisit HR in the curriculum longitudinally.
Limitations
Selection bias may have influenced our qualitative findings, as the focus group consisted only of students already interested in HR. Additionally, the low post-survey response rate (19.4%) raises concerns about whether respondents represented the larger student body, as respondents may have had a particular interest in the topic. The survey instrument also had design limitations. For example, item 1 (“I have a good understanding of what harm reduction is and the strategies it employs”) is double-barreled, which may have reduced response validity. Future iterations should separate these components into distinct items. Furthermore, the survey was not formally validated through a piloting stage, limiting confidence in its reliability and validity. Finally, with only one focus group of 4 participants, thematic saturation was not achieved. While the themes identified provide valuable insights, they may not represent the full range of student perspectives across the cohort.
Conclusion
This study is one of the first in the literature to take a quality improvement approach to implementing and evaluating a curriculum focused on HR communication skills. Future directions for the HMS curriculum include implementing and assessing recommendations that emerged from this study, such as continuing to amplify patient and provider narratives and enhancing teaching about HR as a critical health equity tool. Further quality improvement and research initiatives should seek to evaluate how the integration of HR into medical education ultimately affects clinical care and patient outcomes.
Supplemental Material
sj-docx-1-saj-10.1177_29767342261452657 – Supplemental material for Quality Improvement Initiative to Prepare Medical Students With Harm Reduction Principles for Substance Use Care
Supplemental material, sj-docx-1-saj-10.1177_29767342261452657 for Quality Improvement Initiative to Prepare Medical Students With Harm Reduction Principles for Substance Use Care by Natalie Swartz, Ethan Lowder, Sabina Iqbal, Irving Barrera, Shahin Saberi, William Oles, Beverly Woo, David Krieger and Hilary Smith Connery in Substance Use & Addiction Journal
Footnotes
Acknowledgements
This study does not add further acknowledgments.
Ethical Considerations
The Harvard Longwood Campus Institutional Review Board found this research to be exempt from review (no. IRB24-1549) on November 18, 2024, with the need for written consent waived.
Consent to Participate
Informed consent was obtained verbally before participation in the focus group.
Consent for Publication
Not applicable; this submission does not contain identifying information or material related to study participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data from this study are available to review upon contacting corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.