
Abstract
Objective:
The aim of this study is to examine the associations between smoking self-efficacy, health anxiety, and women’s awareness of third-hand smoke (THS).
Methods:
This descriptive, cross-sectional study was conducted in Türkiye between June and July 2025 through an online survey with 335 women aged ≥18 years. Data were collected using a Descriptive Information Form, the Third-hand Smoke Awareness Scale, the Smoking Self-Efficacy Scale, and the Health Anxiety Inventory. Data were analyzed using descriptive statistics, Mann–Whitney U, Kruskal–Wallis, Spearman’s correlation, multiple linear regression, and mediation analysis.
Results:
A total of 335 women were included in the study (mean age: 34.67 ± 12.31 years). Significant differences in THS awareness, smoking self-efficacy, and health anxiety were observed across several sociodemographic and behavioral variables. Higher educational level was associated with greater THS awareness, while participants with children and those whose partners smoked had lower awareness levels (P < .05). Smoking self-efficacy was higher among nonsmokers and individuals with higher education, whereas health anxiety was higher among smokers and those exposed to smoking in their environment (P < .05). Spearman’s correlation analysis revealed weak but significant associations, including a negative correlation between number of children and THS awareness (ρ = −.213, P < .01), and a positive correlation between THS awareness and smoking self-efficacy (ρ = .154, P < .05). Multiple linear regression analysis showed that the model explained a small proportion of variance (R2 = .06). Only the number of children was significantly associated with THS awareness (β = −.16, P = .02), while smoking self-efficacy and health anxiety were not significant predictors. Mediation analysis indicated that smoking self-efficacy did not mediate the relationship between THS awareness and health anxiety (P > .05).
Conclusion:
THS awareness was associated with several sociodemographic and behavioral factors; however, smoking self-efficacy and health anxiety were not significant predictors in the adjusted model. These findings suggest that awareness alone may be insufficient and that broader contextual and individual factors should be considered in strategies aimed at reducing tobacco exposure.
Highlights
This study examined the associations between women’s thirdhand smoke awareness, smoking self-efficacy, and health anxiety.
Higher thirdhand smoke awareness was associated with greater smoking self-efficacy among women.
Educational level and family-related characteristics significantly influenced women’s awareness of thirdhand smoke, whereas health anxiety showed no significant effect.
Introduction
Exposure to tobacco smoke is categorized as active, passive (secondhand), and third-hand smoke (THS). In particular, THS residue poses numerous health risks and is considered a significant environmental threat. 1 THS is defined as tobacco smoke pollutants that remain on surfaces after tobacco has been smoked. It forms when chemicals from tobacco combustion accumulate on textiles, furniture, and wall surfaces, and are later re-emitted into the environment through air, dust, or clothing. 2 THS can enter the human body through inhalation, skin contact, or ingestion—even in environments where active or passive smoking is not present—posing a significant health risk, especially for vulnerable groups such as children, the elderly, and pregnant women. 3
Despite growing evidence on the health risks of THS, public awareness of this concept remains limited in many populations. Studies conducted in different countries indicate that a considerable proportion of individuals have never heard of THS, even though they may recognize the harmful effects of tobacco smoke residues. For example, a meta-analysis reported that approximately 80% of individuals recognize THS as harmful, although awareness varies substantially across populations. 4 In Türkiye, awareness appears to be considerably lower; several studies have reported that the majority of participants had never heard the term “third-hand smoke,” with rates reaching 84% to 89% in some samples.5,6 Recent studies conducted both in Türkiye and internationally have shown that awareness of THS remains limited, even among younger and more educated segments of the population.5,7
The health effects of THS exposure have been linked to respiratory diseases, weakened immune function, behavioral developmental problems, and certain types of cancer. 1 However, low public awareness in this area hinders the development of individual and societal behaviors aimed at preventing THS exposure. Raising awareness is not solely dependent on information; it is also directly related to psychosocial factors that influence individuals’ health behaviors. 8 One of the primary psychosocial factors in this context is self-efficacy. According to Bandura’s social cognitive theory, self-efficacy refers to an individual’s belief in their capacity to successfully perform a specific behavior. 9 In particular, women’s ability to make active decisions—such as protecting their children in smoking environments or setting boundaries with a smoking partner—is closely related to their level of self-efficacy. Women, particularly during pregnancy, represent a highly vulnerable group in terms of exposure to tobacco smoke. Toxic cigarette residues can cross the placenta and adversely affect fetal development. Prenatal exposure to tobacco smoke has been shown to be associated with adverse outcomes such as low birth weight, premature birth, and fetal growth restriction. 10 Therefore, pregnant women’s awareness and behavioral self-efficacy regarding cigarette smoke exposure play a crucial role in protecting both maternal and infant health.
Self-efficacy refers to an individual’s belief in their ability to perform behaviors necessary to achieve a desired outcome. 9 Individuals with higher smoking cessation self-efficacy are generally more likely to attempt and maintain smoking cessation, whereas lower levels may hinder engagement in protective health behaviors. Health anxiety, on the other hand, reflects the degree of concern individuals experience regarding potential health threats and may influence how seriously they perceive environmental health risks. 11 Although self-efficacy does not directly determine individuals’ awareness of environmental risks such as THS, it may influence the likelihood that individuals translate perceived risks into preventive behaviors. In the context of tobacco exposure, individuals with higher self-efficacy may therefore be more likely to adopt protective actions—such as establishing smoke-free home rules or limiting exposure to tobacco smoke—once they recognize the potential risks.
Psychological factors can play a significant role in shaping individuals’ awareness of environmental health risks such as THS and their behavioral responses. Individuals with a high level of health self-efficacy are more likely to engage in protective behaviors, avoid exposure to tobacco smoke, and implement smoke-free environment rules in their homes.9,12 Self-efficacy may influence how women perceive the risks associated with THS and whether they take action to protect themselves and their families from exposure. Understanding the psychological determinants of THS awareness may therefore contribute to the development of more effective public health interventions aimed at reducing environmental tobacco exposure. In this context, examining women’s awareness of THS is particularly important for understanding the risks they may encounter both within the home environment and at the individual behavioral level. Furthermore, the relationship between THS awareness and smoking self-efficacy and health anxiety represents a critical gap in the literature, particularly from the perspective of psychosocial factors and behavioral interventions.
THS has emerged as a significant public health issue in recent years. Residual tobacco smoke in the environment can cause more harmful health effects for women and children, who spend the most time indoors and are therefore exposed for longer periods. 13 Despite growing scientific evidence regarding potential health risks, public awareness of THS remains limited in many populations. 14 It can be argued that increased awareness among women would contribute to the health of the entire family, particularly children. Therefore, understanding the factors associated with THS awareness is important for developing effective public health interventions aimed at reducing environmental tobacco exposure.
The aim of this study is to examine women’s awareness of THS exposure and its associations with smoking self-efficacy, health anxiety, and selected sociodemographic and smoking-related variables in Türkiye. In this study, the THS awareness total score is treated as the outcome variable, while smoking self-efficacy and health anxiety are considered the main predictor variables. Age, number of children, smoking status, and partner’s smoking status are included as additional covariates.
The main research question of this study is: Which sociodemographic, smoking-related, and psychological variables are associated with women’s awareness of third-hand smoke exposure?
Method
This descriptive and cross-sectional study was conducted in Türkiye via an online survey between June and July 2025. The target population consisted of women aged 18 years and older who were literate in Turkish and used at least one social media platform. A convenience sampling method was used in this study. Participants were recruited online through the researchers’ social media platforms, and women who met the inclusion criteria and volunteered to participate were included in the study. The study included women from different regions of Türkiye.
The sample size was calculated a priori using the standard formula for estimating a single population proportion. 15 The calculation was based on a 95% confidence level (Z = 1.96), a margin of error of 0.03, and an expected prevalence of THS exposure (P = .478), informed by prior literature Guan et al and used as an input parameter. 16
The minimum required sample size was estimated as 207 participants. To enhance the robustness of the findings and improve the stability of multivariable regression analyses, the final sample size was increased to 335 participants.
Study Model
A conceptual model of the study variables is presented in Figure 1. In this model, the THS awareness total score was defined as the outcome variable, while age, number of children, smoking self-efficacy, health anxiety, smoking status, and partner’s smoking status were included as predictor variables.
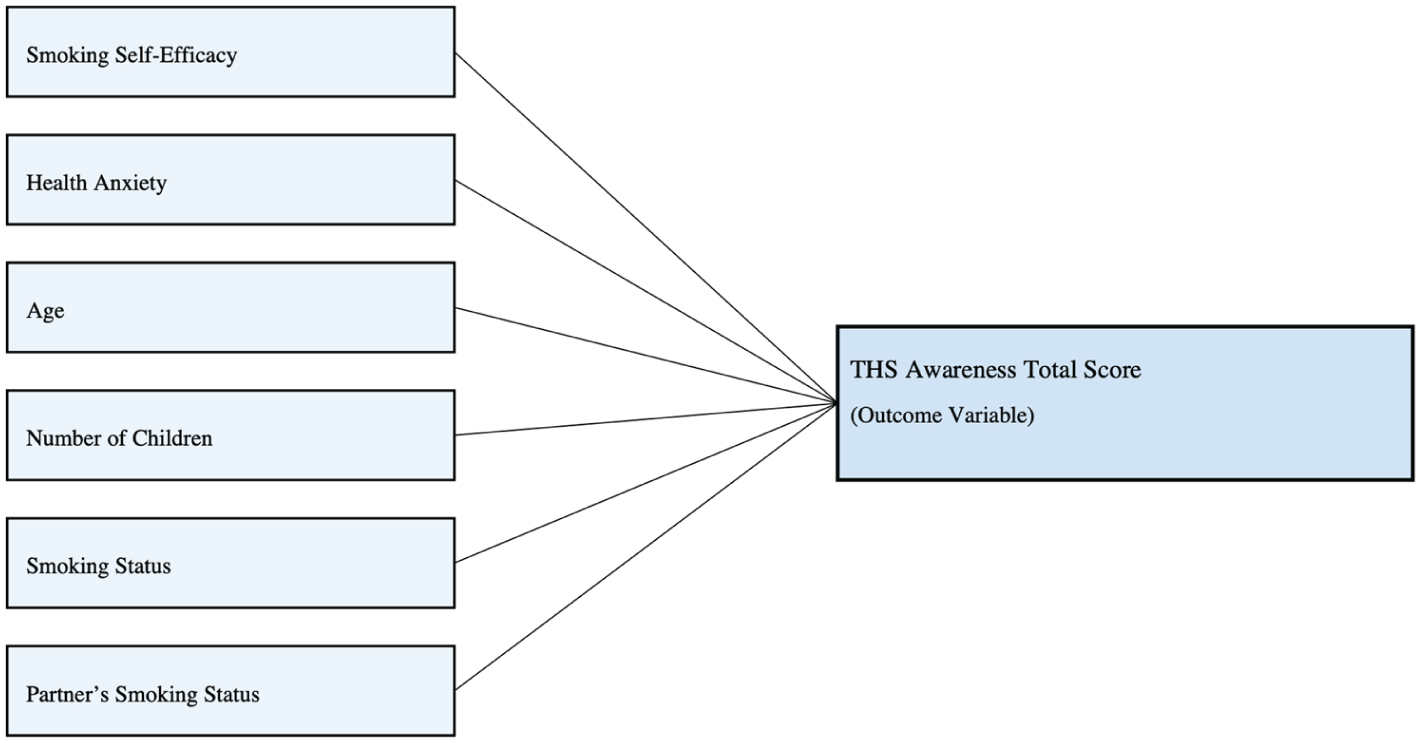
Conceptual model of the study variables.
Inclusion and Exclusion Criteria
The inclusion criteria for the study were being a woman, being 18 years of age or older, being able to speak, read, and write in Turkish, using at least one social media platform, and agreeing to participate voluntarily in the study. The exclusion criteria were being younger than 18 years of age, not being able to read and write in Turkish, not using social media, declining to participate voluntarily, or submitting an incomplete questionnaire.
Data Collection and Instruments
The research data were collected online using a Google Forms questionnaire between June and July 2025. Participants were invited to the study through the researchers’ social media platforms, including LinkedIn, Instagram, Facebook, and WhatsApp. After accessing the study link, participants were first presented with brief information about the study and an electronic informed consent form. Those who agreed to participate voluntarily proceeded to complete the Turkish version of the questionnaire. Women younger than 18 years of age and those who did not complete all items in the questionnaire (n = 24) were excluded from the study.
The online questionnaire consisted of the Descriptive Information Form, the Third-hand Smoke Awareness Scale (THSAS), the Smoking Self-Efficacy Scale (SSES), and the Health Anxiety Inventory (HAI). The Descriptive Information Form was developed by the researchers to obtain data on the participants’ sociodemographic and smoking-related characteristics. It included items on age, marital status, educational level, income status, employment status, parental status, number of children, smoking status, partner’s smoking status, and feelings and thoughts about smoking in the environment. Smoking status was assessed using the self-report item “Do you smoke?” and responses were categorized as “I’ve never smoked,” “Every day,” “Occasionally,” and “I quit.” In the regression analysis, smoking status was entered as a categorical variable.
Third-Hand Smoke Awareness Scale
The THSAS was developed by Haardörfer et al, and its Turkish validity and reliability study was conducted by Önal et al.17,18 The 9-item scale consists of 2 dimensions: health effects and environmental persistence. It is scored on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). The scale has a Cronbach’s alpha value of .71, with a minimum total score of 9 and a maximum total score of 45. 16 Higher total scores indicate greater awareness of THS. According to the exploratory factor analysis results reported by Önal et al, the rotated factor loadings of the items in the health effects subdimension ranged from 0.537 to 0.698, while those in the environmental persistence subdimension ranged from 0.512 to 0.829. 18 The scale uses a 5-point Likert-type response format, with total scores ranging from 9 to 45. There are no reverse-coded items. Higher total scores indicate greater awareness of THS. The Cronbach’s alpha reliability coefficient of the scale was reported as .712. 18 In the present study, the internal consistency of the scale was assessed using Cronbach’s alpha coefficient, which was calculated as .82 (α = .820, 95% CI [0.79, 0.85]). This result indicates that the scale demonstrates a good level of internal consistency and reliability.
Smoking Self-Efficacy Scale
The SSES, which reflects an individual’s confidence in not returning to a risky behavior after facing challenging situations, was developed by Velicer et al. Its Turkish adaptation was carried out by Erol. The Cronbach’s alpha coefficients for the Turkish version were reported as .74 for Negative Affect and Positive Social Situations, .57 for Habitual Temptation, and .67 for Weight Control. Higher scores on the scale indicate a stronger ability to resist returning to the previous behavior despite intense pressure from encouraging situations. The scale consists of 8 items rated on a 5-point Likert-type scale, with total scores ranging from 8 to 40. The scale includes 4 subdimensions: Negative Affect, which reflects the ability to refrain from smoking despite experiencing negative emotions (items 1 and 5); Positive Social Situations, which measures the ability to resist smoking in the presence of encouraging factors (items 2 and 6); Habitual Temptation, which reflects the capacity to maintain change even when smoking is habitual (items 3 and 7); and Weight Control, which indicates the ability to refrain from smoking due to concerns about weight (items 4 and 8).19,20 In the present study, Cronbach’s alpha for the scale was .964 (95% CI [0.96, 0.97]), indicating very high internal consistency. At the same time, this coefficient may also suggest a high degree of inter-item similarity, and thus should be interpreted cautiously.
Health Anxiety Inventory (Short Version)
The HAI, developed by Salkovskis et al, 21 is an 18-item self-report scale used to measure health anxiety. Higher scores on the scale indicate higher levels of health anxiety. The reliability and validity study for the Turkish version was conducted by Aydemir et al. 22 The first 14 items of the scale represent the main body dimension, while the remaining 4 items form an additional subscale related to the negative consequences of illness. The Cronbach’s alpha reliability coefficient of the scale was reported as .918. 22 In the present study, the internal consistency of the scale was assessed with a Cronbach’s alpha coefficient of .86 (α = .861, 95% CI [0.84, 0.89]). This result indicates that the inventory has a high level of internal consistency and reliability.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics. Descriptive statistics for continuous variables were presented as mean, standard deviation, minimum, and maximum values, whereas categorical variables were summarized using frequencies and percentages.
The distribution of THSAS, SSES, and HAI total scores was assessed using the Shapiro–Wilk test. As the data did not meet the assumption of normality, nonparametric tests were used for group comparisons.
Comparisons involving 3 or more groups were conducted using the Kruskal–Wallis test. When significant, post hoc pairwise comparisons were performed using Dunn’s test with Bonferroni correction. Comparisons between 2 groups were performed using the Mann–Whitney U test.
Correlation analyses were conducted using Spearman’s rank correlation coefficient. Total scale scores were used in the analyses instead of subdimension scores to ensure a more parsimonious model and to avoid redundancy due to high intercorrelations among subdimensions.
The analytical framework of the study was structured with THS awareness total score as the dependent variable. Smoking self-efficacy and health anxiety were included as the main independent variables, while age, number of children, smoking status, and partner’s smoking status were entered as covariates. A multiple linear regression analysis was conducted as the main multivariable model to identify factors associated with THS awareness total score.
In addition, a mediation analysis was performed to examine whether smoking self-efficacy mediated the relationship between THS awareness and health anxiety. A P value of less than .05 was considered statistically significant.
Ethical Approval
Ethical approval for the study was obtained (Date: June 27, 2025, Number: 952164). The study was also conducted in accordance with the principles of the Declaration of Helsinki.
Results
Participants had a mean age of 34.67 ± 12.31 years (range: 18-71), and the mean number of children was 1.49 ± 1.89 (range: 0-7). Most participants were married (56.1%), had a university degree or higher (51.9%), were unemployed (63.0%), and reported having children (57.9%). Regarding smoking status, 46.9% had never smoked, while 25.7% reported smoking every day (Table 1).
Demographic Characteristics of the Participants.

Abbreviation: SD, standard deviation.
Continuous variables are presented as mean ± standard deviation and minimum-maximum values; categorical variables are presented as frequencies and percentages.
Since multiple options could be selected.
Table 2 presents the comparisons of THSAS, SSES, and HAI scores according to women’s sociodemographic characteristics.
Comparison of THSAS, SSES, and HAI Scores According to Women’s Sociodemographic Characteristics.

Abbreviations: SD, standard deviation; THSAS, Third-hand Smoke Awareness Scale; SSES, Smoking Self-Efficacy Scale; HAI, Health Anxiety Inventory.
Multiple responses were allowed.
P < .01.
No statistically significant difference was observed in THSAS or HAI scores according to marital status (P > .05). However, SSES scores differed significantly (P < .001, η2 = .038). Post hoc analysis with Bonferroni-adjusted Dunn test indicated that divorced participants had significantly higher SSES scores compared to both single and married participants, while no difference was found between single and married groups.
Educational level was significantly associated with all 3 scales. THSAS scores showed a strong difference (H = 62.66, P < .001, η2 = .178), indicating a moderate-to-large effect size. Post hoc comparisons (Dunn–Bonferroni) revealed that participants with higher education levels had significantly higher THS awareness, particularly those with university education compared to lower education groups.
SSES scores also differed significantly by educational level (P = .013, η2 = .026), although the effect size was small. HAI scores showed a significant difference as well (P = .007, η2 = .030), with higher anxiety levels observed in lower educational groups.
No significant differences were observed in THSAS, SSES, or HAI scores according to income status (P > .05).
THSAS scores differed significantly by employment status (P = .025, rrb = .146), with employed participants reporting higher awareness levels. SSES scores also showed a significant difference (P < .001, rrb = −.242), indicating lower self-efficacy among employed individuals. No significant difference was observed in HAI scores (P = .076).
Participants with children had significantly lower THSAS scores compared to those without children (P = .006, rrb = .177). No significant differences were observed in SSES or HAI scores.
Smoking status was not associated with THSAS scores (P = .353). However, non-smokers had significantly higher SSES scores (P < .001, rrb = −.849) and lower HAI scores (P = .005, rrb = .179) compared to smokers.
Participants whose partners smoked had significantly lower THSAS (P = .007, rrb = −.174) and SSES scores (P < .001, rrb = −.353), and higher HAI scores (P = .038, rrb = .133).
Participants who reported being annoyed by smoking in their environment had higher SSES scores (P < .001, rrb = .323), although no difference was observed in THSAS or HAI scores. Participants who stated that they “do not care” about smoking had significantly lower THSAS (P = .004, rrb = −.246) and SSES scores (P < .001, rrb = −.309). Perceiving smoking as harmful was associated with higher THSAS (P = .035, rrb = .133) and SSES scores (P < .001, rrb = .337). Similarly, participants who believed that smoking harms both their own and their children’s health had significantly higher SSES scores (P < .001, rrb = .319) and lower HAI scores (P = .018, rrb = −.163; Tables 3 and 4).
Spearman Correlations Among Age, Number of Children, THS Awareness, Smoking Self-Efficacy, and Health Anxiety Variables.

Abbreviation: THSAS, Third-hand Smoke Awareness Scale; SSES, Smoking Self-Efficacy Scale; HAI, Health Anxiety Inventory.
Spearman’s rho coefficients are reported.
P < .05. **P < .01.
Multiple Linear Regression Analysis of Factors Associated with THSAS Total Score.

Abbreviations: THSAS, Third-hand Smoke Awareness Scale; SSES, Smoking Self-Efficacy Scale; HAI, Health Anxiety Inventory; SE, standard error.
Dependent variable: THSAS total score. Model fit: R = .25, R2 = .06, adjusted R2 = .04, RMSE = 5.17, F(6, 310) = 3.30, P = .004. Standardized coefficients (β) are reported for continuous predictors only; categorical variables are presented as unstandardized coefficients.
P < .05.
Spearman’s correlation analysis revealed a strong positive association between age and number of children (ρ = .699, P < .01). Age was weakly and negatively correlated with THS awareness (THSAS) scores (ρ = −.152, P < .05), while no significant associations were observed between age and SSES or HAI scores (P > .05).
The number of children was negatively correlated with THSAS (ρ = −.213, P < .01) and SSES scores (ρ = −.135, P < .05), indicating that higher parity was associated with lower awareness and self-efficacy levels. No significant relationship was found with HAI scores. A weak positive correlation was observed between THSAS and SSES scores (ρ = .154, P < .05), suggesting that higher awareness was associated with higher smoking self-efficacy.
In contrast, SSES scores were weakly and negatively correlated with HAI scores (ρ = −.155, P < .05), indicating that higher self-efficacy was associated with lower health anxiety. No significant correlation was found between THSAS and HAI scores.
A multiple linear regression analysis was conducted to examine factors associated with THSAS total score. The overall model was statistically significant (F[6, 310] = 3.30, P = .004), explaining a small proportion of the variance (R = .25, R2 = .06, adjusted R2 = .04).
Among the predictors, only the number of children was significantly associated with THSAS total score. Specifically, a higher number of children was associated with lower THSAS scores (B = −0.68, β = −.16, t = −2.34, P = .02). Age, smoking self-efficacy, health anxiety, smoking status, and partner’s smoking status were not significantly associated with THSAS total score (P > .05).
A mediation analysis was conducted to examine whether smoking self-efficacy mediated the relationship between THS awareness and health anxiety. THS awareness was significantly associated with smoking self-efficacy (β = .23, P = .015). However, smoking self-efficacy was not significantly associated with health anxiety (β = −.09, P = .076), and the indirect effect was not statistically significant (estimate = −0.02, SE = 0.01, Z = −1.43, P = .152, 95% CI [−0.05, 0.01]).
The direct effect of THS awareness on health anxiety was also not significant (estimate = 0.05, P = .557). These findings indicate that smoking self-efficacy did not mediate the relationship between THS awareness and health anxiety.
Discussion
The findings of this study indicate that several sociodemographic and behavioral factors are associated with variations in THS awareness, smoking self-efficacy, and health anxiety.
Educational level emerged as one of the most influential variables. Higher education was associated with significantly greater THS awareness, accompanied by a moderate-to-large effect size. This pattern is consistent with previous research indicating that individuals with higher education levels tend to have greater awareness of tobacco-related harms and environmental exposure risks.23,24 Education may enhance individuals’ access to health-related information and their capacity to interpret the risks of THS exposure. In parallel, lower educational levels were associated with higher health anxiety, which may reflect increased uncertainty or limited access to accurate health information among less educated groups. Similar associations between tobacco exposure and anxiety-related outcomes have been reported in prior studies. 25
Smoking self-efficacy demonstrated distinct group differences across several variables. Divorced individuals exhibited higher self-efficacy compared to both single and married participants, which may indicate differences in life experience, autonomy, or coping strategies. Additionally, individuals with higher education levels reported greater self-efficacy, supporting the notion that education contributes not only to awareness but also to confidence in health-related behaviors. Previous studies have similarly highlighted the role of self-efficacy in shaping smoking-related behaviors and cessation outcomes.26-29
Behavioral factors were also strongly associated with outcomes. Nonsmokers had significantly higher self-efficacy and lower health anxiety compared to smokers, suggesting that smoking behavior is closely linked with both psychological confidence and perceived health risk. This finding is in line with studies demonstrating associations between tobacco use and mental health outcomes such as anxiety and depression.30,31 Similarly, individuals whose partners smoked reported lower THS awareness and self-efficacy, alongside higher health anxiety. This finding highlights the influence of the immediate social environment and aligns with previous research emphasizing the role of household and family context in tobacco exposure and awareness.32-34
Family-related factors also played a role. Participants with children had lower THS awareness, which may be related to competing responsibilities or reduced engagement with health information. In contrast, a higher number of children was associated with lower awareness in multivariable analysis, reinforcing the potential impact of family burden on health-related knowledge and behaviors. Previous studies have also shown that family dynamics and caregiving responsibilities can influence exposure to tobacco-related risks and preventive behaviors.32,33
Perceptions and attitudes toward smoking were consistently associated with outcomes. Individuals who perceived smoking as harmful demonstrated higher awareness and self-efficacy, while those who reported indifference (“do not care”) exhibited lower awareness and self-efficacy. These findings are consistent with prior evidence suggesting that risk perception and cognitive appraisal play a central role in shaping tobacco-related awareness and behavior.35,36
Behavioral factors were also strongly associated with outcomes. Nonsmokers had significantly higher self-efficacy and lower health anxiety compared to smokers, suggesting that smoking behavior is closely linked with both psychological confidence and perceived health risk.
In addition, sociocultural context may play a role in shaping smoking-related behaviors. In Türkiye, smoking prevalence has been reported to be higher among men than women, and tobacco use among women may be influenced by gender-related social norms and stigma. 37 These sociocultural dynamics may affect both smoking behaviors and perceptions related to tobacco exposure.
Overall, these results indicate that THS awareness and related psychosocial factors are shaped by a combination of educational, behavioral, and contextual influences. However, given the modest effect sizes observed in several analyses, these associations should be interpreted cautiously and considered within a broader socio-environmental context.
The correlation findings suggest that age and family-related factors are modestly associated with THS awareness and smoking self-efficacy. The negative association between number of children and both awareness and self-efficacy may indicate that increasing caregiving responsibilities limit individuals’ engagement with health information and preventive behaviors. Similar findings have been reported in studies showing that family environment and parental roles influence tobacco exposure and awareness patterns.34,38
The positive relationship between THS awareness and smoking self-efficacy suggests that individuals who are more aware of the harms of tobacco exposure may also feel more confident in managing or avoiding such risks. This is consistent with previous research emphasizing the role of awareness and behavioral beliefs in shaping tobacco-related avoidance behaviors.35,39
In contrast, the negative association between self-efficacy and health anxiety indicates that greater perceived control over smoking-related behaviors may be linked to lower anxiety levels. Prior literature also suggests that perceptions and beliefs about tobacco exposure are closely linked to psychological and behavioral responses. 8
However, given that all correlations were weak in magnitude, these relationships should be interpreted with caution and considered as indicative rather than strong predictors.
The regression analysis indicated that the overall model explained only a small proportion of the variance in THS awareness, suggesting that awareness is likely influenced by a broader set of unmeasured contextual and structural factors, such as public health messaging, social norms, and environmental exposure patterns. This finding indicates that approximately 95.8% of the variance in THS awareness is explained by factors beyond the scope of this study, such as public health policies, media influences, and sociocultural norms. Previous studies have similarly emphasized that THS awareness and beliefs are shaped by multiple individual and environmental determinants rather than a limited set of predictors.16,38,40
Within the model, the number of children emerged as the only significant predictor, with higher numbers of children associated with lower THS awareness. This finding may reflect the potential impact of increased caregiving responsibilities, which could limit individuals’ time and capacity to access or process health-related information. Family-based studies also indicate that parental roles and household dynamics play a key role in shaping tobacco exposure awareness and related behaviors.41,42
In contrast, age, smoking self-efficacy, health anxiety, and smoking-related variables were not significantly associated with THS awareness after adjustment. This suggests that the apparent relationships observed in univariate analyses may be attenuated when considered alongside other variables, highlighting the multifactorial nature of awareness. Prior research has similarly shown that awareness and behavior are influenced by complex interactions between cognitive, behavioral, and environmental factors.35,43
The mediation analysis further demonstrated that smoking self-efficacy did not mediate the relationship between THS awareness and health anxiety. Although THS awareness was positively associated with self-efficacy, self-efficacy was not significantly related to health anxiety, and the indirect effect was not significant. While self-efficacy is widely recognized as a key factor in smoking behavior change and prevention,44,45 its role in linking awareness to psychological outcomes such as anxiety appears to be limited in this context. Intervention-based studies suggest that self-efficacy may be more responsive to targeted education and behavioral interventions rather than general awareness alone. 46
Overall, these findings suggest that while individual-level cognitive factors such as self-efficacy are related to awareness, they may not be sufficient to explain psychological outcomes such as health anxiety. Instead, other psychosocial or environmental mechanisms may play a more prominent role, and future research should explore these pathways in more comprehensive models. Additionally, growing evidence indicates that the health impacts of tobacco smoke exposure, including THS, are complex and extend beyond awareness alone, involving behavioral, environmental, and physiological dimensions. 47
Limitation
This study has some limitations. First, the cross-sectional design does not allow conclusions regarding temporal changes, long-term patterns, or causal relationships in women’s awareness of THS exposure. Second, the use of online self-report data may have introduced recall bias and social desirability bias. Third, the use of convenience sampling may limit the generalizability of the findings. In addition, multiple statistical comparisons were conducted, and therefore the possibility of type I error cannot be fully excluded despite efforts to interpret the findings cautiously. Another limitation is that some subgroup sizes were relatively small, which may have reduced the stability of subgroup comparisons. Finally, pregnancy status was not assessed, although it may be relevant in studies focusing on tobacco-related exposure awareness among women. In addition, the item assessing feelings and thoughts about smoking in the environment allowed multiple responses; therefore, each response option was analyzed separately as a binary variable, which may have limited the interpretability of comparisons related to this item. Participants were recruited through social media platforms, women with lower levels of internet or social media use may have been underrepresented, particularly in older age groups. Therefore, the findings may not fully represent the broader population of women in Türkiye.
Conclusion
This study demonstrated that THS awareness is associated with several sociodemographic and behavioral factors. While smoking self-efficacy and health anxiety showed relationships with certain variables, they were not significantly associated with THS awareness in the adjusted model.
The findings suggest that awareness alone may not be sufficient to influence behavior, and that multiple contextual and individual factors should be considered. Women may represent a particularly important group in this context, given their roles in family health and caregiving.
Factors such as partner smoking status, number of children, and caregiving responsibilities may be associated with women’s health-related decisions. Therefore, intervention strategies should not only focus on increasing awareness but also consider broader contextual influences. Overall, tailored approaches that address both individual and environmental factors may contribute to reducing tobacco exposure, including secondhand and THS.
Footnotes
Acknowledgements
We would like to thank all the women who participated in this study.
Ethical Considerations a
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Dicle University XXX in June 2025 (Protocol No: E-52857131-050.04-747827).
Consent to Participate
Informed consent was obtained electronically from all participants prior to their participation in the study. Participation was voluntary, and participants were informed about the purpose of the study, confidentiality of the data, and their right to withdraw at any time without penalty.
Authors contribution
EYA Conceptualization, Methodology, Data curation, Investigation, Writing – original draft, Writing – review and editing. ZO Formal analysis, Data analysis, Writing – original draft, Writing – review and editing. ÖT Writing – original draft, Writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are not publicly available due to privacy restrictions. The raw de-identified data may be made available upon reasonable request from the corresponding authors.