
Abstract
Buprenorphine and other medications for opioid use disorder are recommended as standard of care and associated with positive health and addiction-related outcomes. Although observational research suggests at least 180 days of continuous buprenorphine therapy as a measure of treatment quality, more than 50% of patients discontinue before this time period. The drivers of early discontinuation have not been well studied. Prior research, largely utilizing retrospective administrative data, has identified demographic and clinical correlates of discontinuation, including polysubstance use, younger age, minoritized race or ethnicity, male birth sex, higher pain interference and low buprenorphine dose, but why or how such factors are linked with early discontinuation remains unknown. This prospective cohort study will use a convergent parallel mixed methods design to obtain administrative, quantitative survey and qualitative interview data addressing early buprenorphine discontinuation. We will enroll a national sample of N = 965 veterans initiating buprenorphine, stratifying recruitment by sex, race/ethnicity and rurality and collect longitudinal quantitative surveys at baseline, 6 and 12 months to identify modifiable barriers to treatment retention and learn about participant experiences sustaining versus discontinuing buprenorphine. Electronic health record data supplemented by medical record review will identify provider- and system-level factors associated with early discontinuation. Qualitative interviews with a subset of discontinuing participants and their buprenorphine-prescribing clinicians will identify motivations for, and experiences with, discontinuation and contextualize results from surveys and medical record review. This study will provide key information from which to develop interventions targeting the modifiable causes of early buprenorphine discontinuation.
Highlights
Half of patients discontinue buprenorphine early in treatment.
Mechanisms underlying discontinuation are not well understood.
This study will collect surveys, administrative records and interviews (patients and providers).
Results will enable development of interventions targeting early buprenorphine discontinuation.
Background/Rationale
Problem
Opioid use disorder (OUD) remains a public health crisis in the U.S. Although drug-related overdose deaths declined for the first time in a decade in 2023, nearly 80 000 Americans died from an opioid-related overdose in that year. 1 Patients receiving care within the US Department of Veterans Affairs (VA) have been heavily affected by the opioid crisis, with rates of opioid-related mortality increasing by approximately 50% from 2010 to 2019. 2
Medications are considered first-line treatment for OUD and contribute to a 50% reduction in 12-month mortality risk. 3 Among medications for OUD (MOUD), buprenorphine has considerable advantages, which have contributed to significant growth in use.4,5 While methadone prescribing is restricted to licensed opioid treatment programs, buprenorphine can be prescribed in any clinical setting, which both increases access and potentially reduces treatment stigma. It also carries a lower risk of overdose and has a milder side effect profile. 6 Within the VA, more than 80% of patients who receive MOUD are prescribed buprenorphine.7,8
For those initiating buprenorphine, the National Quality Forum designates 180 days of continuous pharmacotherapy as a measure of treatment quality, 9 and clinical guidance recommends maintaining treatment “for as long as it provides a benefit.” 10 This guidance reflects a robust body of research demonstrating that longer periods of treatment are associated with improved clinical outcomes, including lower risk of all-cause inpatient and emergency department use, overdose events and mortality.11-13 For instance, a recent retrospective cohort study, comprising all VA patients engaged in MOUD treatment between 2010 and 2020, found that mortality benefits of MOUD retention continue to accrue through at least 4 years of treatment. 14 Despite the benefits of sustained treatment, early discontinuation is common, with studies showing only 22% to 55% of patients retained in buprenorphine treatment for at least 6 months.15-17
Key Knowledge Gaps
Knowledge of why patients discontinue buprenorphine early in treatment is limited. Prior research, largely utilizing retrospective administrative data, has identified socio-demographic and clinical predictors of discontinuation among U.S. samples. Participant characteristics associated with early discontinuation include younger age, male birth sex, minoritized race/ethnicity, polysubstance use, homeless status, lower buprenorphine dose during treatment and higher baseline pain interference.18-22 While clinical and socio-demographic characteristics associated with early discontinuation have been identified, we lack understanding of the mechanisms through which these characteristics are linked with early discontinuation, which limits the development of interventions to support retention.
Unmet social needs, disproportionately experienced by patients experiencing higher rates of early discontinuation, may be 1 mechanism through which sociodemographic characteristics are linked with early discontinuation. Unmet social needs can be understood as the individual-level manifestation of systemic disadvantages experienced by groups. Group-level differences, which may result from social, economic and political factors that differentially shape life conditions and experiences, are commonly referred to as the social determinants or drivers of health. 23 Few studies have examined the role of unmet social needs in continuity of OUD treatment. One study, utilizing the Veterans Aging Cohort Study, a national observational cohort of VA patients diagnosed with HIV and a group of matched HIV-negative controls, found that patients with a history of homelessness had a significantly lower rate of 12-month buprenorphine retention than those without such history. 21 Another study, conducted within 22 opioid treatment programs, identified significantly greater patient retention in methadone treatment in programs offering transportation services. 24 More broadly, whether higher burden of social needs may partially explain the relationship between patient socio-demographic characteristics and retention in treatment has not been explored.
Evidence is also emerging regarding health system and provider-level factors (eg, clinical approaches) that may be associated with early discontinuation,25,26 although broader replication of findings is needed and questions remain. Two studies conducted within individual states (Michigan and North Carolina) found that providers utilizing “high-threshold” buprenorphine treatment practices increased the likelihood of treatment discontinuation.25,26 High-threshold practices are those that have strict criteria for program entry and require compliance with rules and regulations for treatment continuity. 27 For instance, a study of 377 Michigan prescribers, which assessed the impact of high-threshold requirements on patient retention in treatment, found that patients whose providers required counseling as a condition of treatment were 33% more likely to terminate buprenorphine treatment, while patients whose providers required a urine drug test at each clinical visit were 38% more likely to terminate treatment. 26 Whether the relationship between high-threshold practices and early discontinuation is evident within a large national VA sample remains unknown.
Finally, we lack understanding of patient–provider dynamics that may be influential in discontinuation decisions. 28 For instance, the use of shared decision-making within OUD treatment has increasingly been advocated as a key indicator of OUD treatment quality, 29 and has been shown to reduce opioid misuse via bolstering trust in one’s prescribing provider. 30 However, evidence demonstrating improvements in key patient outcomes such as retention in MOUD associated with the use of shared decision-making is lacking. 31
Objective/Rationale
To advance scientific understanding of modifiable factors impacting buprenorphine discontinuation within the VA and inform strategies clinicians and health systems can utilize to support retention in treatment, we will enroll a national sample of VA patients initiating buprenorphine and follow them for 12 months via longitudinal surveys, administrative record review and interviews with patients and prescribing providers.
Methods/Study Design
Study Design
This prospective cohort study will utilize a convergent parallel mixed-methods design. The study will enroll a national sample of N = 965 veterans initiating buprenorphine and administer quantitative surveys at baseline, 6 and 12 months to obtain patient-reported data unavailable in administrative records. Administrative data supplemented by medical record review will identify provider- and system-level factors associated with early discontinuation. Qualitative interviews with a subset of discontinuing participants, and their buprenorphine-prescribing providers, will identify motivations for, and experiences with, discontinuation and contextualize results from survey and medical record review (Figure 1).
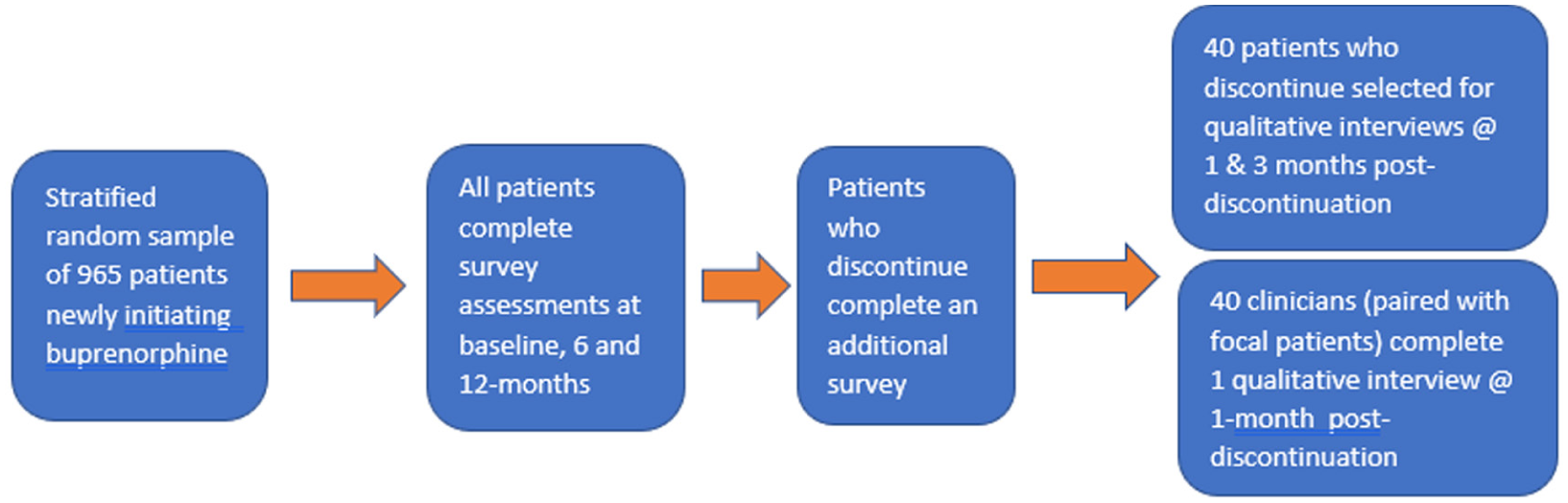
Study sample and processes.
The conceptual model guiding our study (Figure 2) reflects a multi-level understanding of decision-making to hypothesize factors at the patient, provider and system levels that may contribute to a decision to discontinue buprenorphine, with the understanding that decision-making within each level is grounded in a broader social and community context. 32 The model is informed by the Outcomes from Addressing Social Determinants of Health in Systems framework, 33 which details the pathways through which unmet social needs may lead to challenges with medication and appointment adherence, and thereby influence clinical outcomes.
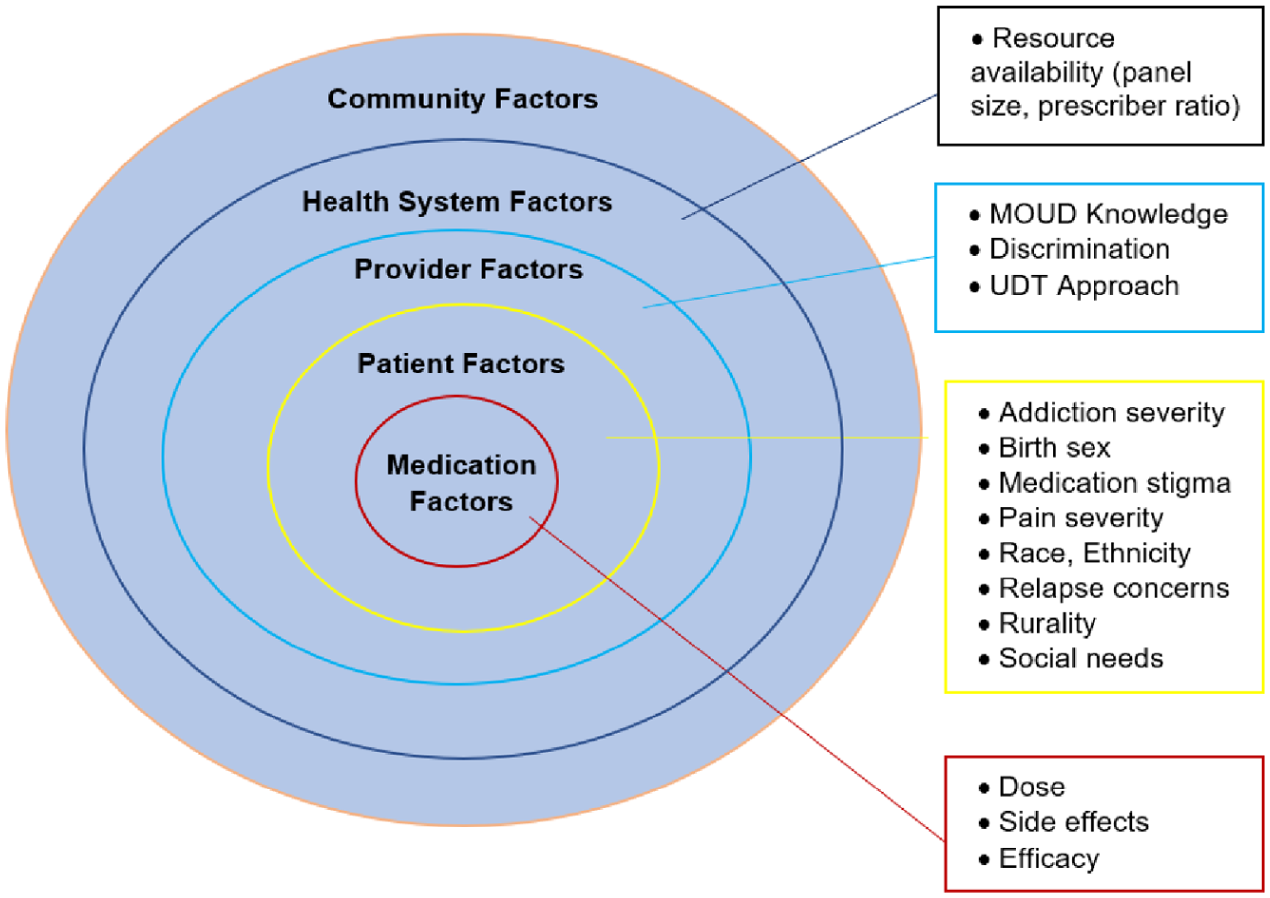
Multi-level factors affecting buprenorphine discontinuation.
Survey Recruitment and Data Collection
The VA Corporate Data Warehouse (CDW), a national repository of data populated from VA electronic health records, will be used to identify all veterans nationally who initiate a new prescription of buprenorphine for OUD. Eligibility criteria include veterans who are (1) diagnosed with OUD; (2) newly initiating buprenorphine, with new initiation defined as receiving a new prescription in the prior 2 weeks, and no buprenorphine treatment within VA or in the community in the 60-day period preceding the new prescription; (3) the ability to speak and read English; and (4) reliable access to a landline or mobile telephone. Buprenorphine treatment will be identified through pharmacy fill data and confirmed via self-report.
Eligibility will be confirmed by chart review. We will mail eligible veterans a letter inviting them to participate within 4 weeks of the initial prescription. Interested veterans may call a study number and complete screening over the phone with a research staff member. Study staff will also reach out to eligible veterans 2 weeks after the initial outreach letter is sent. Eligible veterans will complete informed consent over the phone during the screening visit. We aim to enroll eligible veterans within 6 weeks of medication initiation.
Patient surveys administered at baseline, 6 and 12 months will measure participants’ social needs, medication stigma and perceived discrimination in health care as primary predictors of early buprenorphine discontinuation. We will also collect measures of medication side effects, mental health stigma and comorbidity including symptoms and severity, substance use, pain and quality of life. See Table 1 for a list of survey measures.
Quantitative Study Instruments.
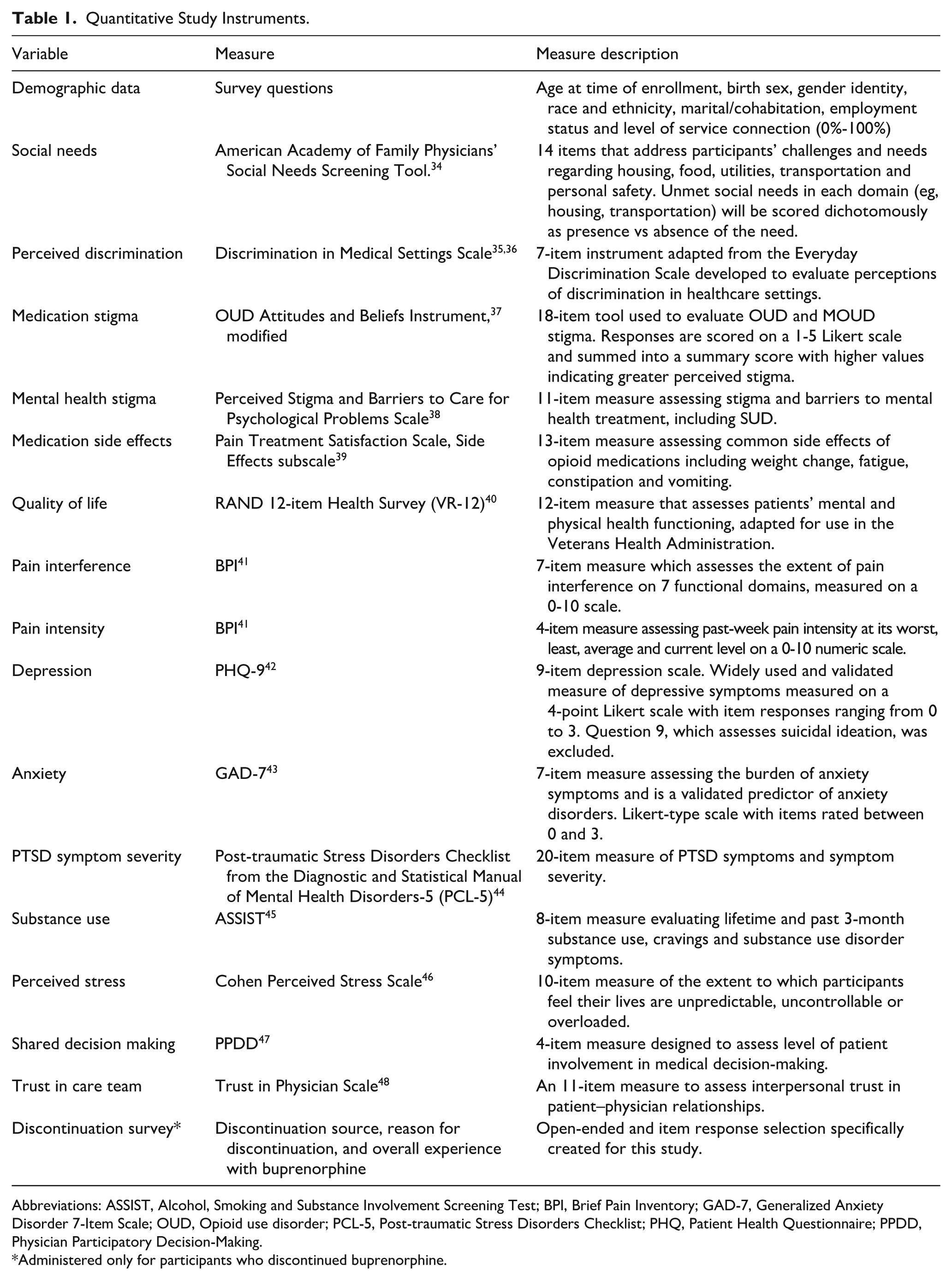
Abbreviations: ASSIST, Alcohol, Smoking and Substance Involvement Screening Test; BPI, Brief Pain Inventory; GAD-7, Generalized Anxiety Disorder 7-Item Scale; OUD, Opioid use disorder; PCL-5, Post-traumatic Stress Disorders Checklist; PHQ, Patient Health Questionnaire; PPDD, Physician Participatory Decision-Making.
Administered only for participants who discontinued buprenorphine.
Data extracted from the CDW will include buprenorphine discontinuation, which will be identified by >30 days without filling a buprenorphine prescription past the prescription end-date of a patient’s last buprenorphine fill. We will also extract patient-level data on buprenorphine dose, medical comorbidity, UDT frequency, and mental health and SUD diagnoses and treatment utilization. Provider-level data will include clinical specialty and percentage of panel prescribed buprenorphine. System-level data will include prescriber panel size and ratio of patients diagnosed with OUD to clinicians eligible to prescribe buprenorphine at the facility level.
Among participants who discontinue before 12 months, we will administer a short survey that will collect information about the reason for discontinuation and overall experience with buprenorphine.
Interview Recruitment and Data Collection
We will conduct interviews with a subsample of 40 participants who have participated in the survey component of the study. Participants will complete 2 interviews each; the first will be administered following discontinuation and the second approximately 3 months later. The initial participant interview will assess perceptions of, and experiences with, buprenorphine discontinuation. Interviews will examine how and through what mechanisms patient, provider and system factors are linked with early discontinuation, and patient perspectives of the barriers and facilitators to retention in treatment. The second patient interview will probe ongoing quality of life, social needs and substance use outcomes and investigate barriers and facilitators to treatment reengagement. To ensure variation in interviews, we will prioritize participants who collectively report diverse reasons for buprenorphine discontinuation in survey response.
We will conduct a single interview with the patient’s buprenorphine-prescribing clinician for a total of 40 provider interviews. The provider interview will uncover clinician perspectives on the motivation for, and process of, discontinuation for their patient, which will allow us to identify areas of concordance and discordance between patient and provider narratives.
Data Analysis
Quantitative Analyses
We will describe the study cohort’s sociodemographic, health and healthcare utilization characteristics, both with and without survey weighting. Inverse probability weighting will be used to account for the stratified sampling design and survey non-response weighting. We will use mixed-effects logistic regression models to evaluate the association between potentially modifiable patient-, provider- and system-level factors at baseline and buprenorphine discontinuation within 12 months. All models will be clustered for provider and site at baseline and potential confounders will be chosen a priori using Directed Acyclic Graphs; this causal model approach helps specify the most parsimonious models and avoids adjustment for variables that are on the causal pathway. 49 Models will also be run with a secondary outcome, buprenorphine discontinuation at 6 months, to identify factors associated with shorter-term discontinuation. Additional analyses restricted to participants who discontinue buprenorphine will quantify discontinuation characteristics, such as source (ie, patient vs provider), reasons for, and whether it was perceived as voluntary or occurred through a shared decision-making process. Analyses will provide important descriptive information regarding buprenorphine discontinuation and causal inference of potentially modifiable factors to reduce early buprenorphine discontinuation among VA patients.
Qualitative Analyses
The analytic team will use a mixed inductive-deductive approach to analyze qualitative interview data. Two members of the research team will independently free-code interviews. Members of the study team will then meet to identify discrepancies in coding, come to consensus and build a final codebook. All transcripts will be coded by a primary coder and secondary reviewer. Following coding of each transcript, primary coders will develop memos summarizing key findings and insights obtained from interviews. A random sample of coded transcripts will be reviewed on an ongoing basis to ensure coding consistency. Guided by the Team’s memos, we will select codes descriptive of important explanatory categories. Participant quotations associated with these codes will then be compared both within and across interviews to identify dimensions of categories and concepts within the data. Through this analytic process, we will develop primary themes addressing our research questions.
Summary
This prospective cohort investigation will utilize quantitative and qualitative data collection methods to enhance understanding of patient- and provider-level factors and patient–provider dynamics associated with early buprenorphine discontinuation. Data obtained from this study has the potential to improve clinical care and inform the development of implementation strategies that aim to enhance treatment retention among veterans with OUD.
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board at the VA Portland Health Care System.
Consent for Publication
All authors reviewed this article prior to submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the US Department of Veterans Affairs Health Systems Research (I01HX003745), the VA Office of Rural Health Career Development Award (#04269), and resources from the VA Health Systems Research-funded Center to Improve Veteran Involvement in Care (CIVIC) at the VA Portland Health Care System (CIN 13-404). Dr. Lovejoy received support from the VA Office of Rural Health during the conduct of this work (NOMAD PROG-0000095).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available, due to the study being in the recruitment phase, but will be available from the corresponding author on reasonable request after study completion.*