
Abstract
Background and Aims:
Decades of research have pointed to a negative association between religiosity and cannabis use. However, the complexity of the dimensions involved in cannabis consumption highlights the need to assess whether religious variables would still be considered protective factors if studies included the level of risk associated with cannabis use. This study examined the association between the strength of religious and atheist beliefs and cannabis use (vs nonuse), as well as the level of risk (low-risk use vs moderate/high-risk use) among participants who use cannabis.
Methods:
Data were collected from 5007 adults using an online questionnaire, of whom 1803 reported cannabis use. Cannabis use and its risk level were measured using the Alcohol, Smoking, and Substance Involvement Screening Test. Strength of religious and atheist belief was measured using the Centrality of Religiosity Scale (CRS-10BR), and the Dimensions of Secularity Scale.
Results:
Logistic regression analyses showed that having medium religiosity (aOR = 1.79; 95% CI = 1.43-2.25), low religiosity (aOR = 1.54; 95% CI = 1.04-2.28), medium/high atheism (aOR = 1.68; 95% CI = 1.27-2.23), or low atheism (aOR = 1.69; 95% CI = 1.18-2.44) was positively associated with cannabis use compared with having high religiosity. However, for moderate/high-risk cannabis use compared with low-risk use, the belief strength analyses were not significant. Regarding intrapersonal religious pluralism, there was no significant difference between non-plural and compatible plural, but being incompatible plural was positively associated with moderate/high-risk cannabis use (aOR = 1.71; 95% CI = 1.23-2.38).
Conclusions:
Cannabis use is negatively associated with high religiosity, while moderate/high-risk cannabis use was not associated with the strength of religious or atheist beliefs. The factors associated with cannabis use differed from those associated with moderate/high-risk cannabis use.
Highlights
High religiosity is negatively associated with cannabis use only when compared to people who do not use cannabis.
There are no differences between levels of religiosity and atheism and moderate/high-risk cannabis use vs. low-risk cannabis use.
Being plural incompatible is positively associated with cannabis use (vs. non-use) and moderate/high-risk cannabis use (vs. low-risk use).
Introduction
Cannabis is the most widely used illicit drug worldwide, reaching 4.6% of the global population. 1 The increase in cannabis use over the decades has been accompanied by research seeking to identify its associated factors.2-4 Among these, religious beliefs have been one of the most extensively studied variables. In general, research has pointed to a negative association between religiosity and cannabis use.5,6 These findings have been observed across different cultural contexts, including the United States,6-8 the United Kingdom, 9 Brazil,10,11 Switzerland, 12 South Africa, 13 and Lebanon. 14
However, much of the research investigating this relationship has been conducted with adolescents,5,8,15 most of whom are religious (ie, studies analyze levels of religiosity within predominantly religious samples).6,13,14 Furthermore, these studies tend to focus only on the dichotomy of use versus nonuse of cannabis.6,8 The complexity of the dimensions involved in cannabis consumption highlights the need to assess whether religious variables would still be considered protective factors if studies included the level of risk associated with cannabis use and focused on adult populations.
A review encompassing 83 studies analyzed the risk factors associated with the negative consequences of cannabis use. Of the 83 studies included in the review, none investigated religious variables. 16 Although a nationally representative study in the United States found a lower odds of cannabis use disorder among individuals who attended religious services, 17 some authors have discussed the limitations of research that considers only religious attendance. One such limitation is that the protective factors may not be inherently related to religiosity, but rather to social control and the selection of a social network that does not engage in drug use.18,19 In this context, other studies have also begun to question the supposed protective role of religiosity in various health outcomes,20-22 including substance use.23,24 One of the main distinctions in these studies on religiosity and health is the inclusion of atheists for comparison and, more importantly, the differentiation between nonreligious individuals and atheists. Those who identify as nonreligious are often grouped together with atheists.25,26 However, people without religion may still hold religious beliefs but do not belong to any formal religious affiliation—unlike atheists, who do not believe in a higher power or a deity. 27
This distinction, along with the inclusion of a substantial sample of atheists, has revealed a phenomenon that some authors refer to as the strength of belief. Findings from research on belief strength suggest that the protective role of religiosity in health outcomes may be related not to the content of belief itself, but to the conviction behind it, whether religious or atheist. In other words, individuals with high levels of religiosity may exhibit health outcomes similar to those of atheists.21,28-30 In the context of drug use, exploring this relationship is particularly important, as a body of literature has consistently emphasized the protective role of religiosity in reducing substance use.31-33 However, this consensus may be challenged by new research designs that include atheists for comparison and investigate other belief-related variables.
Addressing these gaps, the present study examines the strength of religious and atheist beliefs by analyzing the magnitude of these beliefs (ie, high, medium, and low levels of religiosity and atheism) as factors associated with cannabis use (vs nonuse) and, more importantly, investigates the level of risk (low-risk use vs moderate/high-risk use) among participants who report using cannabis. Additionally, this research includes the analysis of contextual religious variables, such as intrapersonal religious pluralism, which is particularly observed in the Brazilian population.
Method
The study included participants aged 18 and older from all regions of Brazil. Data collection was conducted through an online questionnaire hosted on the Google Forms platform. To recruit participants, the survey was widely disseminated between January 20, 2022, and February 19, 2022, across major digital communication channels commonly used by the Brazilian population, such as websites, Facebook, Instagram, Twitter, and WhatsApp. The advertising material for this study is available in Supplemental Material 1. The study followed the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies.
Instruments and Order of Questions
After providing informed consent to participate in the study, participants answered sociodemographic questions, including sex, age, sexual orientation/gender identity, marital status, and educational level. They then responded to questions regarding drug use, followed by questionnaires on religiosity and atheism. The belief-related questions were placed at the end of the questionnaire, considering that the order of questions in studies on religiosity and drug use can influence participants’ responses regarding their patterns of substance use. 34 All instruments are listed below.
Substance Use and Moderate/High-Risk Risk Patterns of Cannabis Consumption
To analyze patterns of cannabis use, we employed the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST), which has been validated for the Brazilian context. 35 This scale assesses the frequency, problems, and harms related to substance use over the past 3 months. Individuals who reported cannabis use within this period were classified as engaging in low-risk use (scores 0-3) or moderate/high-risk use (scores ≥4). These cutoffs are based on the validation of the Brazilian version of the ASSIST scale. We grouped the moderate use and the scores high-risk use into a single category to indicate moderate/high-risk cannabis use. For other substances such as alcohol, tobacco, cocaine, and psychedelics, participants were categorized based on use vs. nonuse in the past 3 months.
Intrapersonal Religious Pluralism
To measure intrapersonal religious pluralism, participants were asked the following question: “What is your belief/religion/religious or nonreligious position? (You can select more than one option).” This variable identified 3 categories of beliefs: “non-plural” (participants who selected only 1 affiliation); “incompatible plural” (participants who selected 2 or more incongruent options, such as atheist/evangelical); and “compatible plural” (participants who selected 2 or more options that are minimally equivalent or similar, such as Baptist/Presbyterian).
In grouping the incompatible plural category, both historical incompatibility between religions (ie, one religion did not derive from the other, for example, one being African and another Eastern) and theological incompatibility (ie, doctrinal principles are incompatible, such as one religion believing in reincarnation and another in resurrection) were considered. For the compatible plural category, historical compatibility was considered, whereby, despite theological differences, these tend to be minor (eg, the Presbyterian Church has theological differences from Methodist churches but shares historical proximity).
Strength of Religious and Atheistic Belief
Participants were asked the following question again: “What is your belief/religion/religious or non-religious position?” with the difference that now the participants were also told “In the previous question, you could select as many options as you wanted. Now, if you had to select only one option, the one that is most important to you, which would you choose?” Based on their responses, the sample was divided into religious individuals (those who identified as Catholic, evangelical, spiritist, umbanda practitioners, etc) and atheists (those who identified as atheists or agnostics). Agnostics were grouped together with atheists, according to the definition proposed by Bullivant (2013), which considers agnosticism a type of atheism. 36 Religious participants were classified into high, medium, and low religiosity according to the Centrality of Religiosity Scale (CRS-10BR). 37 This instrument, validated for the Brazilian population, measures the importance of religiosity in psychological and behavioral construction. The following CRS-10 parameters were applied: high religiosity (4.0-5.0); medium religiosity (2.1-3.9); low religiosity (1.0-2.0). 37
Atheists were classified as having high or medium/low atheism according to the Dimensions of Secularity Scale (DoS), also validated for the Brazilian context. 38 The atheism factor consists of 5 statements rated on a six-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). High atheism was defined by scores from 21 to 30, medium atheism by scores from 11 to 20, and low atheism by scores from 5 to 10. However, since the number of atheists scoring low on the atheism scale was notably small (N = 26), the medium and low atheism groups were combined.
We also analyzed continuous scores of secular philosophical orientations from the DoS scale, namely, humanism (ie, interest in global and humanitarian issues), scientism (ie, belief in the ability of science to solve the world’s problems), and personal responsibility (ie, the extent to which an individual takes responsibility for their personal choices). Additionally, participants were asked whether they follow any religious or atheist pages on social media.
Statistical Analysis
To analyze the association between the strength of religious or atheistic beliefs and cannabis use, binary logistic regression models were employed. Chi-squared tests were used to compare sociodemographic differences between cannabis use and nonuse, and differences between low-risk cannabis use and moderate/high-risk cannabis use. All analyses were conducted using the JAMOVI software (https://www.jamovi.org), version 2.7.5. Prior to these analyses, multicollinearity among variables was assessed using tolerance values (>0.8) and variance inflation factor (VIF). 39 First, we analyzed the full sample with the dependent variable being cannabis use in the past 3 months versus nonuse. Subsequently, regression analyses were performed on the subsample of participants who reported cannabis use in the past 3 months. In this case, the dependent variable was low-risk cannabis use versus moderate/high-risk cannabis use. In model 1, substance use variables in the past 3 months (alcohol, tobacco, cocaine, and psychedelics) were included. Model 2 incorporated all variables related to the strength of religiosity and atheism (strength of belief, religious pluralism, following atheist pages, following religious pages, scientism, humanism, and personal responsibility). All models were adjusted for sociodemographic variables (sex, age, sexual orientation/gender identity, educational level, and marital status). Model fit quality was assessed by comparing the full model with a model including only sociodemographic variables, using the likelihood ratio test and McFadden’s pseudo-R2. The log-likelihood ratio chi-squared test yielded significant results for both the full sample (N = 5007) (χ2[24] = 1791, P < .001) and the subsample of people who use cannabis (N = 1803) (χ2[24] = 189, P < .001), suggesting that models including all predictor variables provided a better fit than those with sociodemographic variables alone. McDonald’s omega reliability coefficients for this study were 0.84 for the DoS scale and 0.93 for the CRS-10 scale.
Results
A total of 5007 individuals participated in the study. Of these, 1803 reported cannabis use, with the majority engaging in moderate/high-risk cannabis use (N = 1396; 77.4%). Table 1 presents the characteristics of the participant sample comparing cannabis use versus nonuse and low-risk versus moderate/high-risk cannabis use.
Sample Characteristics.
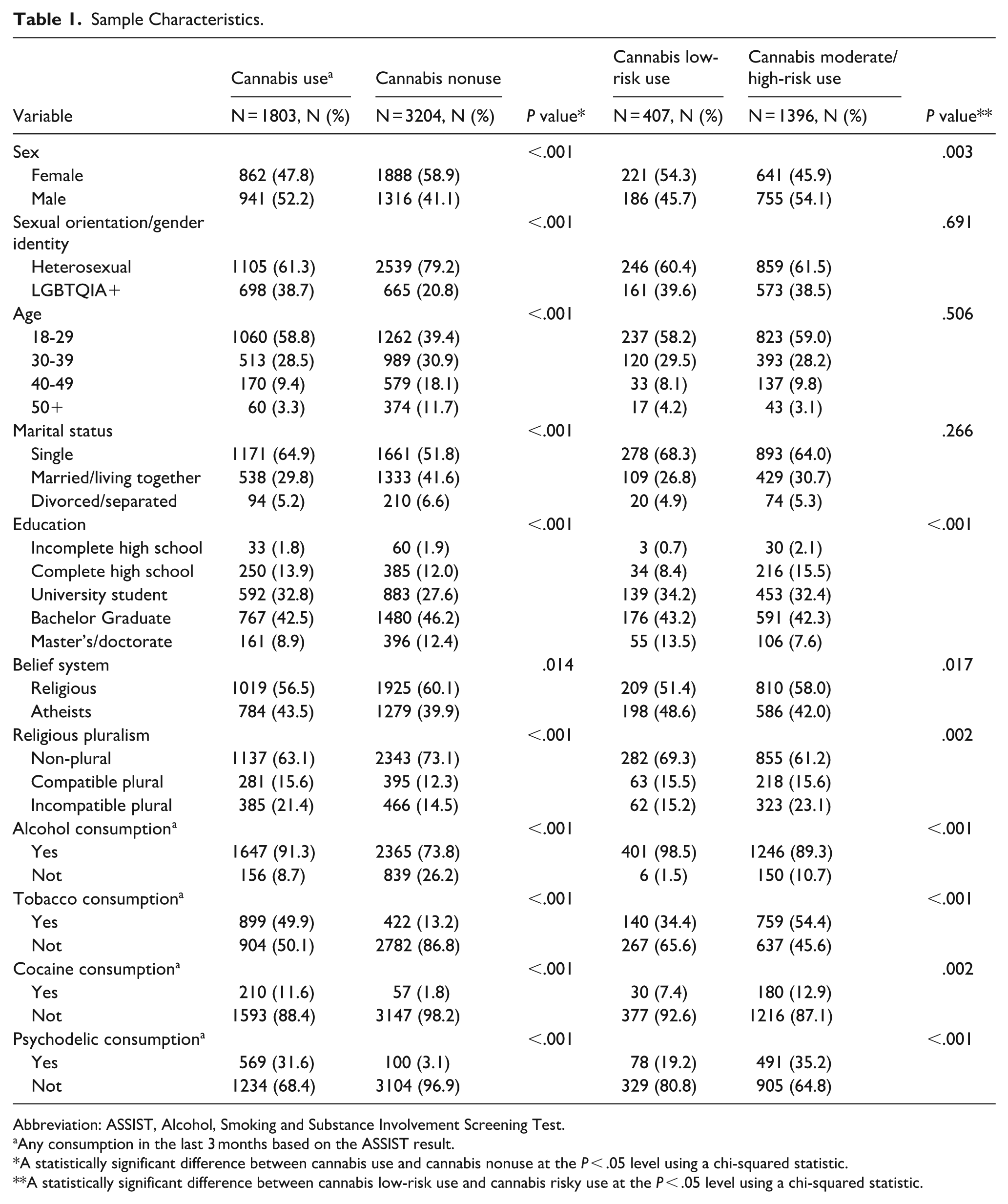
Abbreviation: ASSIST, Alcohol, Smoking and Substance Involvement Screening Test.
Any consumption in the last 3 months based on the ASSIST result.
A statistically significant difference between cannabis use and cannabis nonuse at the P < .05 level using a chi-squared statistic.
A statistically significant difference between cannabis low-risk use and cannabis risky use at the P < .05 level using a chi-squared statistic.
Associations With Cannabis Use Versus Nonuse
Logistic regression results for association between cannabis use versus nonuse are presented in Table 2. In model 1, logistic regression analyses showed that the substances most strongly associated with cannabis use were tobacco (aOR = 4.23; 95% CI = 3.61-4.97), and psychedelics (aOR = 10.14; 95% CI = 7.92-12.99). Alcohol and cocaine use were also positively associated with cannabis use, as shown in Table 2. In model 2, when variables related to religiosity were included, although explanatory power was lower, it was still significant. Having medium religiosity (aOR = 1.79; 95% CI = 1.43-2.25) and low religiosity (aOR = 1.54; 95% CI = 1.04-2.28) was positively associated with cannabis use compared with having high religiosity. Similarly, having medium/high atheism (aOR = 1.68; 95% CI = 1.27-2.23) or low atheism (aOR = 1.69; 95% CI = 1.18-2.44) was positively associated with cannabis use compared with individuals with high religiosity. Regarding intrapersonal religious pluralism, there was no significant difference between non-plural and compatible plural, but being incompatible plural was positively associated with cannabis use. Religious variables improved the explanatory power (pseudo-R2) of cannabis use in model 2.
Binomial Logistic Regression Models For Cannabis Use (vs Nonuse) and Moderate/High-Risk Cannabis Use (vs Low-Risk Use).
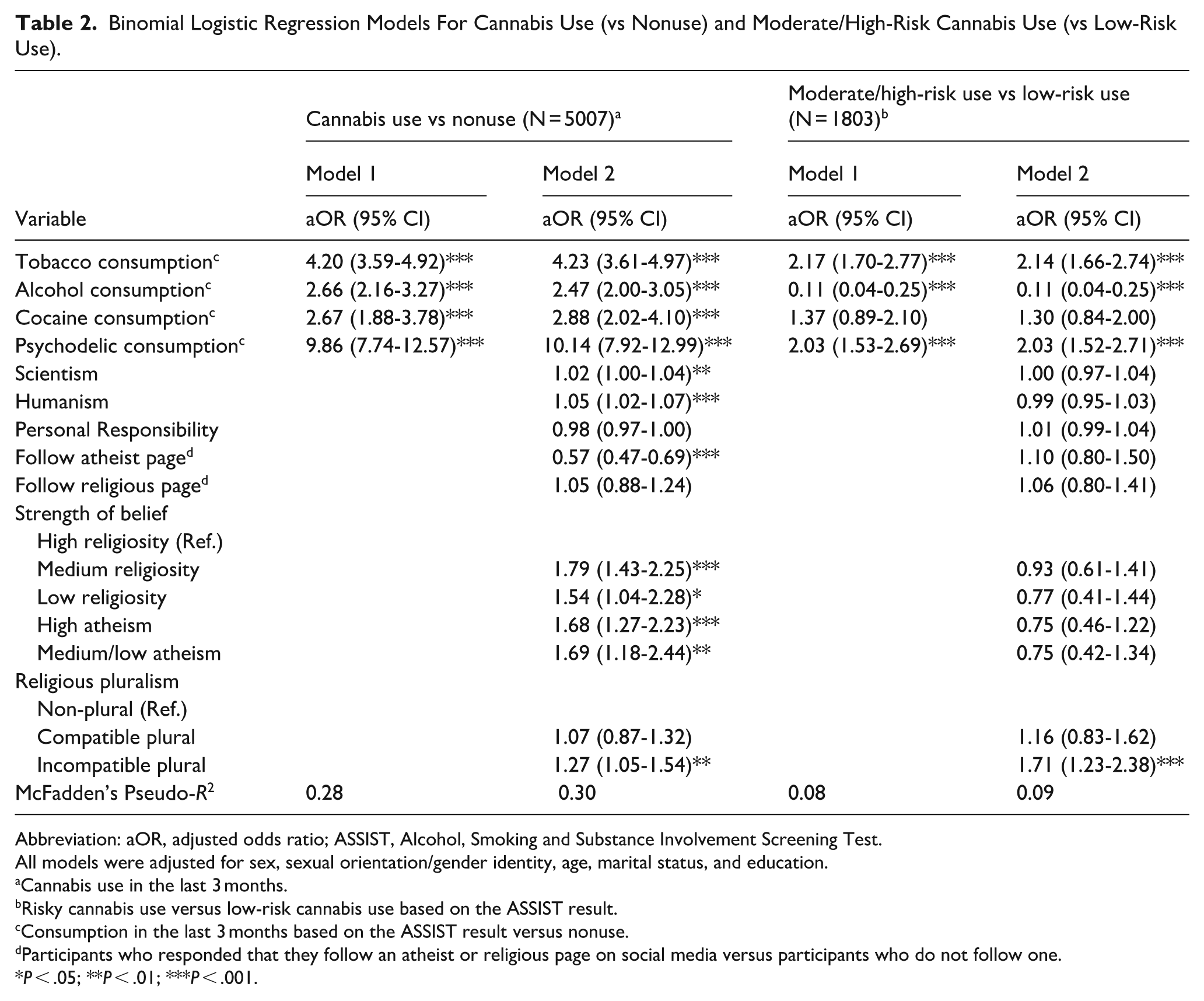
Abbreviation: aOR, adjusted odds ratio; ASSIST, Alcohol, Smoking and Substance Involvement Screening Test.
All models were adjusted for sex, sexual orientation/gender identity, age, marital status, and education.
Cannabis use in the last 3 months. b Risky cannabis use versus low-risk cannabis use based on the ASSIST result. c Consumption in the last 3 months based on the ASSIST result versus nonuse. d Participants who responded that they follow an atheist or religious page on social media versus participants who do not follow one.
P < .05; **P < .01; ***P < .001.
Associations With Moderate/High-Risk Cannabis Use Versus Low-Risk Use
Logistic regression analyses that examined only cannabis use (comparing moderate/high-risk cannabis use vs low-risk cannabis use) showed lower explanatory power. Models 1 and 2 indicated a weak fit, based on McFadden’s pseudo-R2 values (0.08 in model 1; 0.09 in model 2). Tobacco use (aOR = 2.14; 95% CI = 1.66-2.74) and psychedelics use (aOR = 2.03; 95% CI = 1.52-2.71) were positively associated with moderate/high-risk cannabis use, while alcohol use was negatively associated with moderate/high-risk cannabis use (aOR = 0.11; 95% CI = 0.04-0.25). In model 2, when variables related to religiosity were included, no variable was significant except for intrapersonal religious pluralism, which was positively associated with moderate/high-risk cannabis use compared with non-plural individuals (aOR = 1.71; 95% CI = 1.23-2.38).
Discussion
The present study investigated whether different levels of religiosity and atheism were associated with cannabis use (vs nonuse) and moderate/high-risk cannabis use (vs low-risk use). Our results indicated 2 distinct scenarios. First, high religiosity was negatively associated with cannabis use, when compared to medium and low religiosity and high and medium/low atheism. Second, when examining the risk level among participants who used cannabis, no significant differences were found between high religiosity compared with low or medium religiosity, as well as high and medium/low atheism. Intrapersonal religious pluralism was significant in both analyses, showing that being incompatible plural was positively associated with cannabis use and moderate/high-risk use compared with non-plural individuals. However, the variables with the greatest weight associated with cannabis use and moderate/high-risk use were the use of other drugs.
These results indicate that religiosity was only negatively associated with cannabis use when the level of religiosity is high. This suggests that merely identifying as religious is not, in itself, associated with lower cannabis use, nor are different levels of atheism. The findings of this research, while corroborating some studies,40,41 highlight the need to distinguish which forms of religiosity are associated with reduced use. This association appears to apply only to the initial stages of cannabis use and not among individuals who are already using. This distinction is particularly important given that decades of literature have emphasized a negative association between religiosity and drug use,2,42 often without making such distinctions.
Our study did not support previous research on the strength of religious and atheistic beliefs that found similar health outcomes among individuals with high religiosity and those who are atheist.20,28,43 Analysis of cannabis use (or nonuse) showed that high religiosity was negatively associated with cannabis use when compared to all other levels of religious and atheistic belief. Conversely, following an atheist page on social media was associated with lower odds of cannabis use, while following a religious page was not a significant predictor. Although seemingly counterintuitive, these results may suggest that in a predominantly religious country like Brazil, engagement with atheist pages may serve as a form of group affiliation. This type of group engagement is often difficult to measure within atheist populations. The negative association between group engagement in religious activities and drug use is already well documented in the literature.25,44,45 However, future research could further explore how group engagement may manifest in atheist populations. Similarly, a positive, although very small, association between secular philosophical orientations such as scientism and humanism and cannabis use.
The only religious variable that was significant in both analyses was intrapersonal religious pluralism, which was positively associated with cannabis use (and nonuse) and moderate/high-risk (vs low-risk) cannabis use when comparing samples of non-plural individuals. In other words, individuals who reported having conflicting belief systems, such as identifying simultaneously as evangelical, atheist, and umbandist, were more likely to engage in risky cannabis use. Thus, the combination of beliefs with divergent values and premises appears to be a more important variable in cannabis use risk patterns than the strength of either religious or atheistic beliefs. Future studies could examine whether holding incompatible beliefs increases the likelihood of experiencing spiritual struggles, a variable that has been positively associated with drug use.46-48 Our findings suggest that analyzing religious variables adapted to specific cultural contexts may provide a more accurate understanding of the role of belief systems in cannabis use. This approach could also be extended to the study of other substances. Although the impact of incoherent beliefs has only been observed in Brazilian studies,24,27 it may also be present in other settings. Moreover, the way religious affiliation questions are typically formulated, often allowing for only a single response, may fail to capture these nuances, which reflect current shifts in religious landscapes. Therefore, examining the unique characteristics of belief systems within each studied context may enhance our understanding of the contemporary dimensions of belief and their relationship to cannabis and other substance use.
It is important to note that among individuals who were already using cannabis, the strength of religious and atheistic beliefs was not significantly associated with risky use. This suggests that belief-related variables lose their significance when the level of risk is analyzed rather than mere use. In general, the variables included in the models carried less explanatory weight when predicting risk level compared to when they were used to predict cannabis use versus nonuse. This difference is particularly evident in the model fit, as indicated by the pseudo-R2 values. For cannabis use, the model accounted for 30% of the variance in the dependent variable, whereas for risky use, the model explained only 9%. These findings indicate that the variables associated with risky cannabis use may differ from those associated solely with use.
Although the present study included a sample of 5007 individuals, of whom 1803 reported cannabis use, there are some limitations to consider. As a nonrepresentative sample of the Brazilian population, participants tended to have a high level of education, and 36% reported cannabis use in the past 3 months. This percentage is considerably higher than that found in the most recent national drug survey. 49 On the other hand, the substantial number of people who use cannabis, along with a notable proportion of atheists (who are typically underrepresented in research on religiosity and health), provided a unique opportunity to examine the role of both religious and atheistic belief strength. The findings suggest that belief strength plays a relatively small role in the factors associated with cannabis use. More importantly, they highlight that the factors associated with moderate/high-risk cannabis use appear to be distinct and remain insufficiently understood.
Conclusion
In our study, having a high level of religiosity was negatively associated with cannabis use. However, levels of religiosity and atheism were not significant variables when analyses compared moderate/high-risk versus low-risk cannabis use. Intrapersonal religious pluralism, a variable that measures belonging to 2 or more religions simultaneously, showed that being incompatible plural was positively associated with cannabis use (vs nonuse) and moderate/high-risk cannabis use (vs low-risk use). These results point to the importance of analyzing this variable in future research on the relationship between religiosity and drug use. Furthermore, the strength of belief, commonly observed in health-related studies, was not corroborated in the present study, since only high religiosity showed a negative association with cannabis use. Finally, the explanatory power of the regression models was high for cannabis use (vs nonuse), but low for moderate/high-risk use (vs low risk), indicating that other dimensions should be explored in future research to better understand the factors associated with different levels of risk in cannabis consumption.
Supplemental Material
sj-docx-1-saj-10.1177_29767342261456138 – Supplemental material for Cannabis Use Patterns and the Strength of Belief: Challenging the Religious-Atheist Division
Supplemental material, sj-docx-1-saj-10.1177_29767342261456138 for Cannabis Use Patterns and the Strength of Belief: Challenging the Religious-Atheist Division by Camila Chagas, Leonardo Breno Martins, Tassiane Cristine Santos de Paula, Wellington Zangari and José Carlos Fernandes Galduróz in Substance Use & Addiction Journal
Footnotes
Acknowledgements
We used ChatGPT (GPT-5.3) only for English grammatical revision.
Ethical Considerations
This study was approved by the Ethics and Research Committee of the Federal University of São Paulo. Project No. 0931/2020.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Contributions
CC Conceptualization, statistical analysis, writing original draft, and review. LBM Writing, review, and editing. TCSP Statistical analysis and review. WZ Review and editing. JCFG Conceptualization, review, and writing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by grant from the São Paulo Research Foundation (FAPESP); C.C. (PhD scholarship—2020/10234-2).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.