
Abstract
Background:
Health and mental health systems are increasingly employing community health workers and peer support specialists to expand service reach and effectiveness, yet role definitions and competency standards vary widely. Little is known about how to train or prepare these professionals to collaborate with health care teams, engage peers and community members, and address complex health and mental health needs. Tobacco use remains a leading cause of illness and death in the United States and disproportionately impacts people with low incomes and people with mental health conditions, including substance use disorders. Support for Tobacco Recovery Training (STaRT) was developed to provide brief but comprehensive training to support engagement in evidence-based tobacco treatment. This study describes STaRT’s development and evaluates knowledge, reach, and satisfaction among graduates during its first 2 years.
Methods:
We developed STaRT using a community-engaged process with peer specialists, behavioral health professionals, and academic partners. The final program includes 8 self-paced online modules emphasizing recovery-oriented language, communication strategies, evidence-based treatment, and resource navigation. We collected demographics and a knowledge assessment at baseline, and a post-knowledge assessment and evaluation upon training completion. We used descriptive statistics to summarize demographics and evaluation items and a choropleth map of trainees demonstrates reach. We evaluated change in knowledge using a paired samples t-test.
Results:
From November 2023 through October 2025, 256 trainees graduated from STaRT. Trainees were primarily women (83%) and worked across diverse settings, including public health, mental health, community health, and social service settings. Mean knowledge scores increased from 83% to 97% (P < .01). Trainees represented 46/105 counties, with reach ranging from 1 to 43 graduates/100 000 population. Program satisfaction was high (mean 4.6/5).
Conclusions:
STaRT is a feasible, scalable, and peer-informed training model that improves knowledge and expands the tobacco recovery workforce. Findings suggest strong potential for implementation and adaptation beyond Kansas.
Highlights
Community health workers and peer support specialists need knowledge and skills to be effective.
Support for Tobacco Recovery Training engaged a diverse workforce and achieved statewide reach.
Trainees reported high satisfaction and showed gains in tobacco recovery knowledge.
This adaptable model can expand reach and impact of the tobacco recovery workforce.
Introduction
Tobacco use continues to be the leading cause of preventable death and disease worldwide, attributing to more than 480 000 deaths each year. 1 Tobacco use is associated with 30% of all cancers and 80% of lung cancers.2,3 In 2022, nearly 20% of adults in the United States used tobacco products. 4 Studies estimate that anywhere from half to 68% of adults who use tobacco want to stop; about half of those make an attempt, but fewer than 10% are successful.5,6 Evidence-based treatment strategies including counseling and pharmacotherapy are effective for tobacco use disorder; however, few individuals who want to stop receive these treatments.5,7
The reach of tobacco treatment and recovery can be increased through equipping peer support specialists, community health workers (CHWs), and other health care workers with the skills needed to assist peers/clients with tobacco recovery. CHW and peer support specialist roles are grounded in person-centered approaches and represent distinct but complementary models. Peer support specialists draw on their lived experiences with substance use or mental health conditions to provide recovery-oriented support, whereas CHWs typically serve as trusted community members who facilitate access to care, deliver health education, and connect individuals to resources. Both roles can leverage shared understanding and community trust to foster engagement, reduce stigma, and support behavior change. This combination of experiential and community-based support can help address barriers that traditional cessation programs often overlook, such as lack of motivation and limited access to culturally or contextually relevant support. Peers and CHWs can normalize the challenges of treating tobacco use, celebrate small successes, and offer practical strategies to navigate triggers and relapse risks.8,9
A growing body of evidence demonstrates that peer support can increase attempts to stop smoking10,11 and results in successful cessation10,12-15 or reduction in the number of cigarettes smoked per day.10,11,15 Additionally, peer-to-peer communication has been shown to empower individuals to feel comfortable talking to their health care provider about tobacco use 11 and improve self-efficacy related to managing health. 16
Despite evidence for the effectiveness of peer support in tobacco recovery, little is known about how peer support providers and CHWs are trained to deliver tobacco cessation and recovery. Tobacco treatment education programs, such as tobacco treatment specialist (TTS) trainings, have demonstrated effectiveness in increasing knowledge and skills related to tobacco treatment. 17 These programs are typically designed for health care providers and are often time-intensive and costly. Moreover, the content is often heavily theoretical, which may not be appropriately tailored to the needs or scope of peer supporters and CHWs.
Support for Tobacco Recovery Training (STaRT) was developed in collaboration with a training development workgroup including peer support specialists, TTSs, tobacco researchers and educators in academic medical centers, program officers at the departments of health, and advocates for mental health services. The STaRT program was designed to equip health and social service professionals, such as CHWs, peer coaches, substance use counselors, health and wellness coordinators, health care navigators and athletic trainers to address stigma and effectively support tobacco recovery. The content emphasizes effective communication about tobacco recovery, recognizing tobacco use disorder as both a mental health and substance use condition, facilitating nonconfrontational conversations, and highlighting recovery benefits. The program underscores the importance of celebrating incremental successes, clarifying provider roles, using evidence-based treatment approaches, understanding health impacts associated with e-cigarette use, and applying evidence-based recovery strategies. This paper describes the development of STaRT and evaluates the knowledge, reach, and satisfaction of graduates participating in the first 2 years of the program.
Methods
Program Development
Over a 2-year period, the STaRT Training Development Workgroup collaborated to design the training and develop materials. This group included State of Kansas Certified Peer Specialists from a local health department who had participated in TTS trainings, individuals from a local mental health department, the National Alliance on Mental Illness (NAMI), the Kansas Department of Aging and Disability Services (KDADS), experts in peer training at the Wichita State University, and the University of Kansas Medical Center. Wichita State University’s Community Engagement Institute, with expertise in technical assistance, also contributed to the development process. Collectively, this group represented academic researchers, experts on health and mental health/substance use, individuals with lived experience, and instructional technology experts.
At the first workgroup meeting, the group determined the core knowledge and skills to be included in STaRT, reviewed existing materials and resources, and determined what, if any, new materials needed to be developed. They also discussed the appropriate format and platform for the training, developed evaluation questions, and developed a format to provide recognition for completing the training.
After the preliminary format and content had been developed, we piloted the training with a group of peer specialists during a 3-hour virtual meeting conducted via Zoom. During this session, trainees completed the course in real-time and then members of the training team solicited input on the content and format. The peer specialists’ feedback was incorporated into the final program.
Design and Content
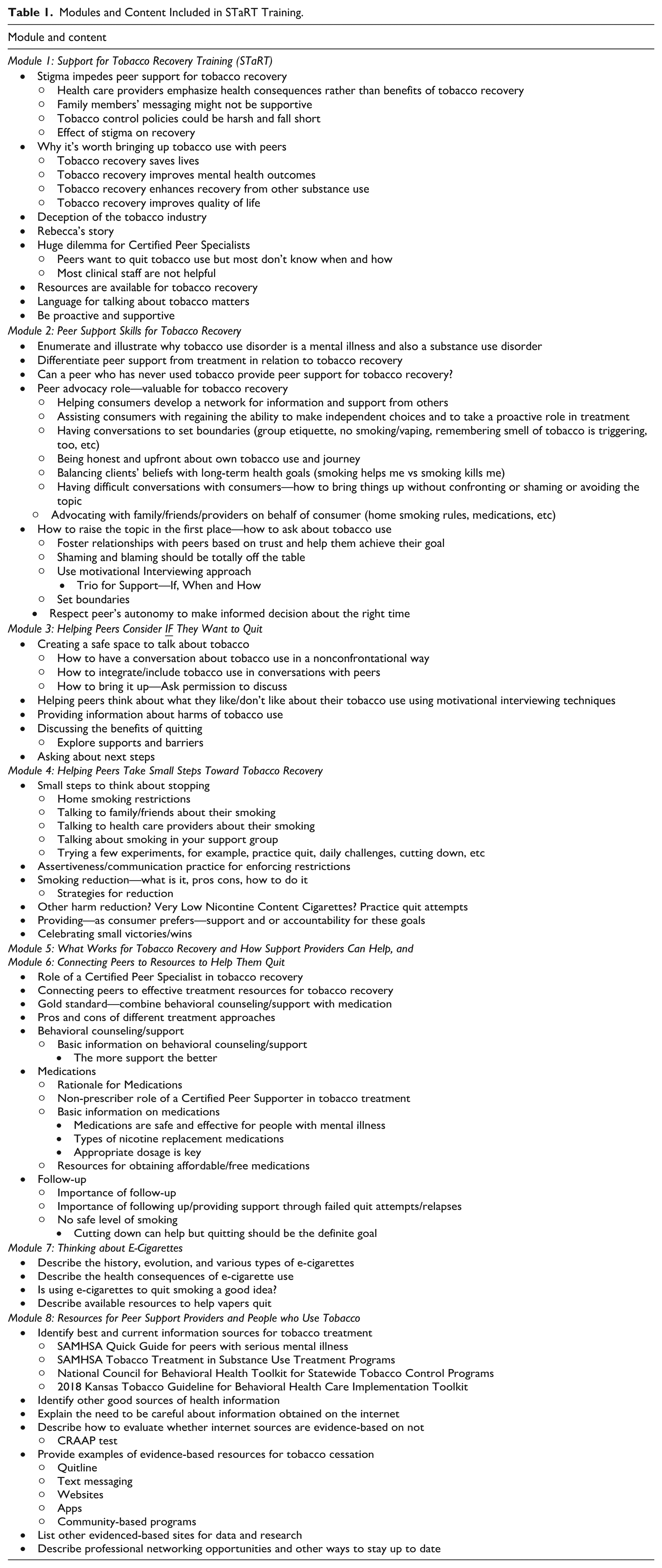
The final STaRT curriculum evolved into a self-paced, asynchronous training, including 8 modules that are completed online. Each module is designed to be completed in 15 to 20 minutes. Modules include video testimonials, links to resources, and materials that can be printed. There is a short quiz after each module to reinforce learning. Trainees must score 100% on the quiz before proceeding to the next module. Trainees are given 60 days to complete all 8 modules (see Table 1 for a list of modules and content). Although the course content can be completed in approximately 3 hours in a single sitting, the program was intentionally divided into eight 20 to 30-minute modules and delivered over a 60-day period. This structure provides flexibility for working professionals with completing professional responsibilities and reflects evidence-based principles of adult learning, particularly distributed practice, which enhances long-term retention and application compared with single session instruction.18-22 Trainees receive a certificate upon completion of the training. The cost to complete the course is $100; trainees providing support to clients in the state of Kansas were eligible to receive a scholarship from the State Health Department to cover the cost of the training.
Modules and Content Included in STaRT Training.
Introductory Lecture
The course begins with a brief video that introduces the instructors and overviews what to expect from the training.
Module 1: Support for Tobacco Recovery Training
The intent of Module 1 is to show CHWs and peer supporters the importance of their addressing tobacco use and how they can address it in an empathetic, nonconfrontational way. This module addresses input from peer specialists that they fear damaging their relationship with the people they want to help if they try to address clients’ tobacco use.
This module examines stigma surrounding tobacco use, explores the role of peers and health care providers in addressing it, and underscores the importance of delivering consistent, supportive messages across helping roles. It introduces key language that will be used throughout the training. For example, instead of framing the process as “quitting” or “smoking cessation,” which implies an immediate on/off switch, the training emphasizes the concept of “recovery,” similar to other substance use disorders. The training also emphasizes the term “tobacco use disorder” rather than “tobacco addiction,” as it is the correct medical terminology. Similarly, individuals are referred to as “someone who smokes or uses tobacco” instead of “smoker,” reflecting that tobacco use is a behavior, not an inherent identity.
Module 2: Peer Support Skills and Tobacco
Module 2 differentiates tobacco treatment from tobacco recovery and illustrates how CHWs and peer specialists can make unique and unprecedented contributions to the recovery process due to their personal experiences and relationships with their clients. This module addresses input from peer training specialists that the peer role is distinct from other roles in treatment teams. For example, a treatment provider may prescribe a medication; the peer support provider or CHW can support clients in obtaining the prescription and discussing its effectiveness. The training highlights similarities between tobacco use and other mental health conditions and offers guidance on applying existing skills to support tobacco recovery. Finally, it provides advice on initiating conversations about tobacco recovery in ways that minimize stigma and shame.
Module 3: Helping Peers Consider IF They Want to Quit
The intent of Module 3 is to demonstrate creating a safe space for discussing tobacco use. This module addresses concerns identified during development regarding the potential for the typical directive approach to undermine the CHW or peer relationship with the people they support. It emphasizes ensuring the peer remains in control of when and how they want to address their tobacco use. Additionally, the module provides information on the harms of tobacco use, highlights the benefits of recovery, and guides peers in exploring potential next steps.
Module 4: Helping Peers Take Small Steps Toward Tobacco Recovery
Module 4 trains participants in strategies to meet their patients and clients “where they are,” facilitating progress toward tobacco recovery. This module acknowledges that many individuals are ambivalent about stopping tobacco use and that tobacco use is a chronic, relapsing condition 23 that often requires multiple attempts and strategies to achieve complete remission (cessation). This module focuses on incremental steps toward recovery. It includes topics such as moving beyond all-or-nothing mindset, celebrating small steps toward recovery, and considering tobacco reduction goals as a step toward tobacco recovery.
Module 5: What Works for Tobacco Recovery and How Support Providers Can Help
The goal of Module 5 is to provide education on evidence-based tobacco treatment and effective approaches to support motivation for stopping tobacco use. This module addresses published reports and work group concerns that behavioral health professionals may lack training in evidence-based care of tobacco use disorder. 24 The module provides information related to effective forms of behavioral support such as brief counseling, telephone, and text messaging. It also outlines medications available to support recovery, along with their benefits and risks.
Module 6: Connecting Peers to Resources for Tobacco Recovery
The intent of Module 6 is to highlight free, readily available ways to access medications and counseling for tobacco use. This module addresses concerns raised during development regarding the affordability and accessibility of cessation medications and behavioral support. It informs trainees regarding Medicaid and insurance coverage and further provides information on connecting those in their recovery journey to free and/or low-cost resources.
Module 7: Thinking About E-Cigarettes
The focus of Module 7 is to clarify misconceptions regarding e-cigarettes and to consider appropriate strategies to address their use. This module describes the types of electronic devices currently available and how they have changed over time, current evidence regarding the health effects of e-cigarettes, how effective they are in helping people stop cigarette use, and how to support individuals who want to stop or reduce e-cigarette use.
Module 8: Resources for Peer Support Providers and People Who Use Tobacco
The intent of Module 8 is to empower trainees to keep current with changes in tobacco use, e-cigarette technology, evidence-based treatments, and resources available for training and supporting recovery. This module recognizes the evolving nature of tobacco use and highlights the importance of being a knowledgeable resource for those they support, along with other health care providers with whom they work. It provides education on how to determine whether or not sources are evidence-based. Additionally, it includes tools and resources that peers can utilize in helping others and offer to individuals during their recovery journey.
Instructor Qualifications and Training Team
The STaRT training team consists of 2 PhD/MD-level academic researchers and certified tobacco treatment trainers with decades of experience in tobacco cessation research and education, a peer support specialist, and a tobacco treatment training coordinator. The recorded videos are delivered by the PhD/MDs with excerpts from a TTS trained peer support specialist who shares her experiences in providing tobacco recovery support. The tobacco treatment training coordinator helps with recruitment, follow-up of trainees, and other logistical support involved in the day-to-day activities of the project.
Participant Recruitment and Selection
Training participants were recruited using a wide range of methods. These included flyers distributed at conference meetings and community events, social media posts (LinkedIn), targeted email and listservs, word of mouth, and email advertisements through the state health department.
Funding and Support
The development of STaRT was funded through the Kansas Health Foundation’s Tobacco and Behavioral Health Initiative, Phase 2, which focused on increasing the number and location of TTSs and increasing demand for quality improvement and evidence-based practices. The Kansas Department of Health and Environment provided funding for scholarships for trainees working with clients in the state of Kansas.
Evaluation Methods
Measures
At enrollment, participants were asked to provide the following demographic information: age, gender, race, highest level of education completed and work setting, including type of setting and county. The county in which participants worked were coded as metropolitan or nonmetropolitan according to 2023 Rural Urban Continuum Codes. Additionally, they completed a baseline 10-item knowledge assessment consisting of multiple-choice and true/false questions. A knowledge score was calculated as the percentage of questions answered correctly.
Upon completion of the program, trainees were asked to complete the knowledge assessment again. They were also asked to evaluate their satisfaction with the program. They were asked to provide an overall rating of the course on a 5-point Likert scale from 1 (poor) to 5 (excellent). They were also asked to provide their level of agreement with 13 statements related to the curriculum (1, strongly disagree to 5, strongly agree) and how well the course met 8 learning objectives (1, poorly to 5, extremely well).
Statistical Analyses
Baseline demographics and program assessment questions were evaluated using basic descriptive statistics (frequencies and percentages for categorical variables; means and standard deviations for continuous variables). Change in the assessment score from baseline to post-training was evaluated using a paired samples t-test. Reach was calculated as the ratio of STaRT graduates in each county in Kansas to the total county population. Counties were categorized into quartiles based on reach, and results were visualized using a choropleth map. The mean reach by metropolitan status was calculated and compared using an independent samples t-test. All analyses were conducted using SAS Version 9.4 (SAS Institute, Inc, Cary, NC, USA), and maps were generated using ArcGIS Pro Version 3.1 (Esri Inc, Redlands, CA, USA). The institutional review board at our institution approved the evaluation of this training.
Results
Demographics
From November 2023 to October 2025, a total of 256 trainees graduated from STaRT. The mean age of graduates was 41.5 (SD 12.9) years. Most trainees self-reported their gender as woman (n = 213, 83.2%) and their race as white (n = 183, 71.5%). Most trainees worked in the state of Kansas (n = 233, 91.0%). The highest level of education reported varied, with the most frequent response being a bachelor’s degree (n = 81, 31.6%), followed by a master’s degree (n = 66, 25.8%), and an associate’s degree (n = 48, 18.8%). Trainees came from a variety of work settings, including, but not limited to, public health agencies (n = 71, 27.7%), mental health clinics (n = 54, 21.1%), community health centers (n = 35, 13.7%), social service agencies (n = 31, 12.1%), and substance use facilities (n = 27, 10.6%). About 80% of trainees received a scholarship to cover the cost of the training. See Table 2 for trainee demographics.
Demographics of N = 256 Graduates of the STaRT Program From November 2023 Through October 2025.
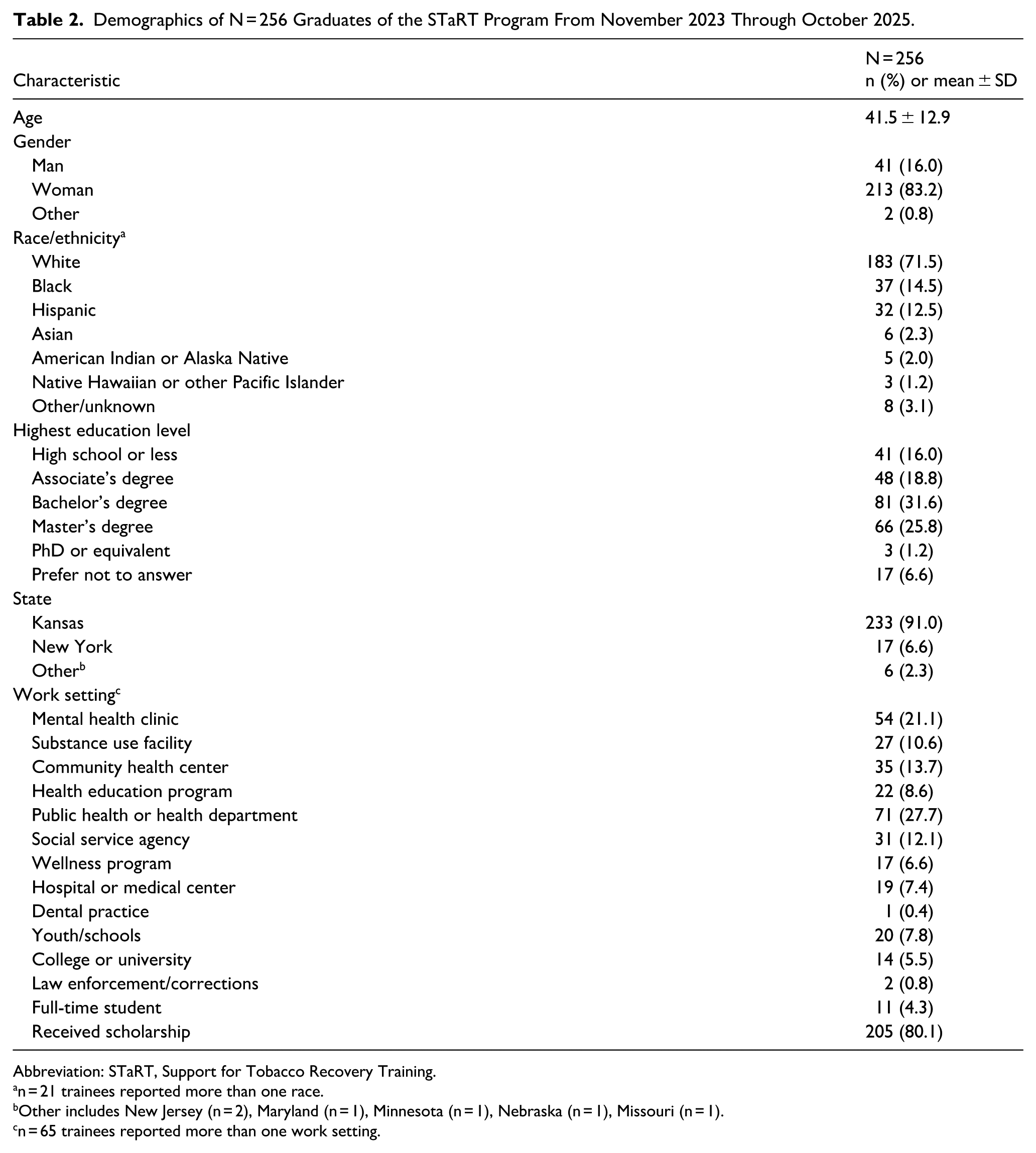
Abbreviation: STaRT, Support for Tobacco Recovery Training.
n = 21 trainees reported more than one race. b Other includes New Jersey (n = 2), Maryland (n = 1), Minnesota (n = 1), Nebraska (n = 1), Missouri (n = 1). c n = 65 trainees reported more than one work setting.
Reach
Figure 1 demonstrates the reach of the training within the state of Kansas. Trainees came from 46 of the 105 counties in Kansas, with the number of trainees per 100 000 population in counties reached ranging from 1 to 43. Trainees were distributed throughout all geographic regions of the state, with a mean reach of 9.0 (SD 9.8) in counties classified as metropolitan and 7.0 (SD 14.3) in counties classified as nonmetropolitan (P = .5762).
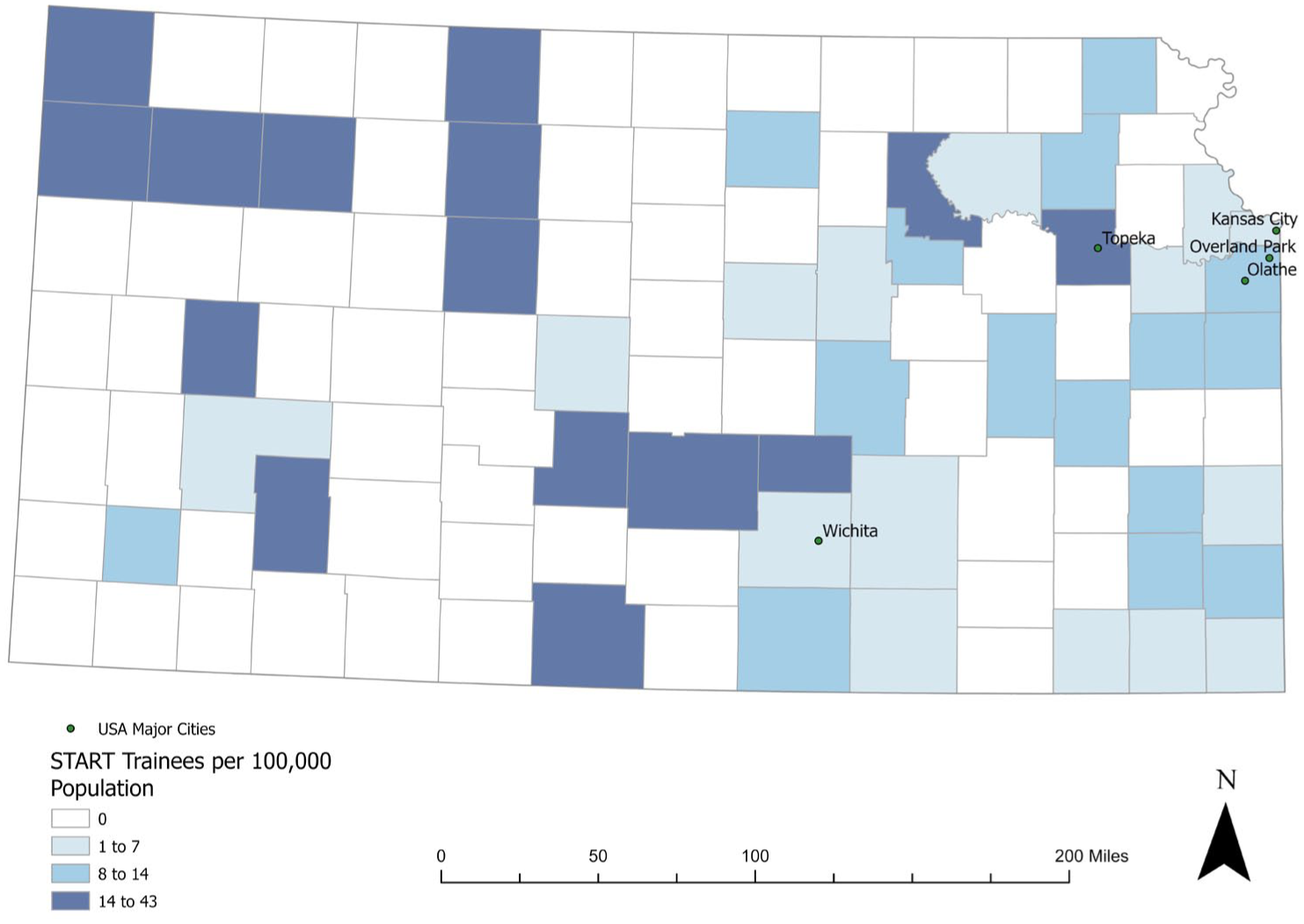
Density of STaRT Trainees per 100 000 population by county of employment, state of Kansas, November 2023 to October 2025.
Knowledge and Evaluation
Knowledge scores improved from baseline to posttest (83% [SD 11.9] to 97% [SD 5.8], P < .01). A total of 200 (78%) graduates completed the course evaluation. The mean satisfaction with the overall training was 4.6 (SD 0.59). Curriculum evaluation ratings were also very high, ranging from a mean of 4.1 to 4.6. The lowest ratings were related to the technology and online platform used for the training. Mean scores for how well the course met learning objectives ranged from 4.4 to 4.6. Table 3 includes scores for each evaluation item.
Trainee Feedback From the Course Evaluation Survey (N = 200 [78%] Trainees).
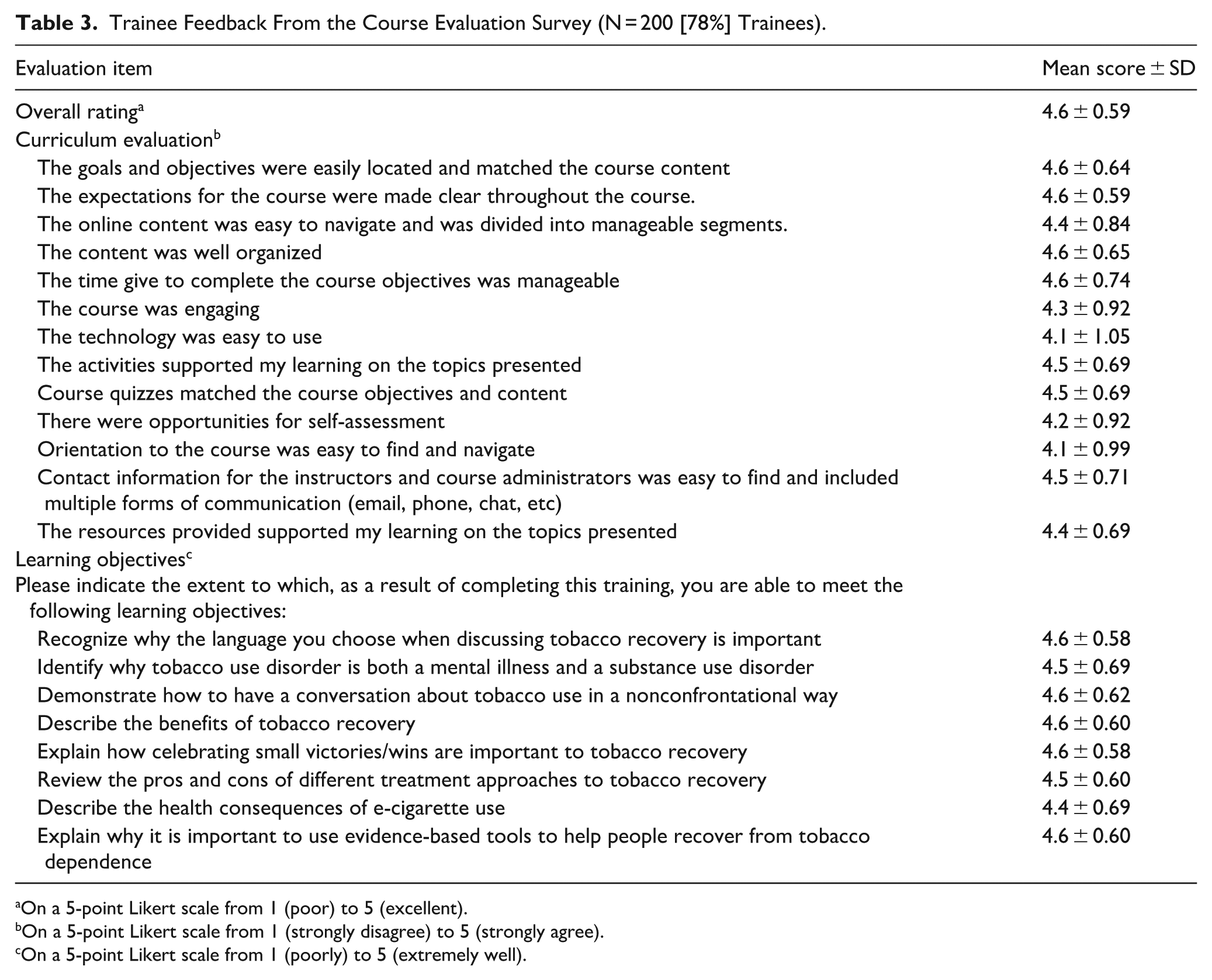
On a 5-point Likert scale from 1 (poor) to 5 (excellent). b On a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). c On a 5-point Likert scale from 1 (poorly) to 5 (extremely well).
Discussion
STaRT was designed using a community-engaged process to build capacity among peer support specialists, CHWs, and other professionals to integrate tobacco recovery principles into their practice. In its first 2 years, STaRT engaged a diverse workforce, achieved broad geographic reach within the state, and was highly rated by trainees across multiple domains of learning and satisfaction. Importantly, the course cost was $100, and 80% of participants received scholarships, increasing the program’s accessibility. Despite a fairly high level of knowledge at baseline, trainees demonstrated improved knowledge upon completion of the training.
The program also demonstrated broad geographic reach across the state of Kansas and even reached trainees from other states. However, despite this broad reach, there are still gaps in the tobacco recovery workforce in our state, demonstrating room for growth of the program.
Evaluations of the program reflected high levels of satisfaction and perceived learning across nearly all dimensions. The mean overall course rating was 4.6 out of 5, indicating a strong endorsement of the program. Trainees rated the curriculum very highly. They overwhelmingly agreed that the course was well organized, that the content matched the course goals and objectives, that expectations for the course were clear, that content was divided into manageable segments, and that time to complete the course was appropriate. The lowest rated items were related to the ease of use of the technology and course navigation. Though these items were still rated highly (4.1/5), they identify opportunities for modest improvement in the user experience. When STaRT was initially launched, our university-based training platform required an extensive onboarding process, including assignment of a university email address for trainee access. Later, the platform was updated to eliminate this requirement, substantially simplifying the login process.
Ratings for how well the course met learning objectives were uniformly high, with mean scores ranging from 4.4 to 4.6 on a 5-point scale. Trainees reported the greatest gains in their ability to use recovery-oriented language, discuss tobacco use nonconfrontationally, and explain why tobacco use disorder is both a mental health condition and a substance use disorder. These findings suggest that STaRT improved both knowledge and confidence in addressing tobacco recovery. These findings align with findings of other online tobacco treatment programs that demonstrate improved knowledge and self-efficacy related to tobacco treatment. 25
An important consideration is the role of peers with lived experience of tobacco use in delivering tobacco recovery support. Engaging individuals in recovery in work that involves exposure to others’ tobacco use may raise concerns about cue-induced cravings or relapse. However, it is important to note that most STaRT participants are already employed in peer support or behavioral health roles in which they routinely work with individuals who use tobacco. As such, the program does not newly introduce trainees to this environment but instead provides training to support work they are already performing. The STaRT curriculum reinforces the application of peer support principles, including self-awareness, boundary setting, and use of lived experience in a safe and intentional manner. It also encouraged trainees to monitor their own recovery status and seek support when needed. In this way, the training is intended to better equip trainees to navigate potential triggers and may serve as a protective factor rather than increasing risk.
There are several important limitations to consider related to the evaluation of STaRT. First, we did not have a control group that did not receive training, so it cannot be stated that knowledge improvement was directly related to the training. In addition, the knowledge assessment items were developed specifically for this training and aligned with course content and learning objectives. While this supports strong content relevance, the assessment tool has not undergone formal psychometric evaluation. Future work should include evaluation of the reliability and validity of these measures. Further, the knowledge gain represents an immediate improvement; it is unknown whether this is sustained long-term. Additionally, because the evaluations were completed by 78% of graduates, response bias is possible, as those who were highly satisfied with the program may have been more likely to respond than those less satisfied with the training. Also of note, the recruitment methods used for the program may introduce selection bias. Participants were recruited through channels such as conference outreach, social media, and word of mouth, which are likely to engage individuals who are already highly motivated or interested in tobacco treatment. As a result, the sample may not be representative of the broader workforce, and the observed improvements in knowledge and level of satisfaction may reflect trainees’ preexisting motivation or engagement rather than training alone. Further, although most participants (80%) received scholarships to cover the cost of training, a small proportion paid the registration fee ($100). While this cost is substantially lower than that of many tobacco treatment trainings, it is possible that cost may have influenced participation for some individuals. Finally, outcomes such as change in clinical practice, client engagement, or organizational policies were not measured. Future evaluations should be conducted to understand the sustained impact of the training on workforce and client outcomes.
Despite these limitations, these findings have important implications. Early results from STaRT provide evidence that an online, asynchronous, peer-informed training model can effectively strengthen the tobacco recovery workforce. Indeed, STaRT has been integrated into a university degree program in our state and is now a required component of an Addictions Treatment course, with scholarships provided to complete the training. Additionally, a Spanish-language version of the STaRT program has recently been launched, including culturally relevant content developed in collaboration with our university’s JUNTOS Center for Advancing Latino Health. Addressing the challenge of identifying an online platform that meets institutional requirements while remaining accessible and user-friendly is critical to enabling program growth. This advancement has facilitated expansion across the state and positions STaRT for broader dissemination at the national and international levels. Future efforts will focus on further language adaptations and the incorporation of culturally tailored content to support diverse populations. In this context, we also note that the term “tobacco” as used in this evaluation primarily reflects products most prevalent in the United States, particularly combustible cigarettes and e-cigarettes. However, patterns of tobacco product use vary globally. For example, in some countries, including Norway, noncombustible products such as snus are widely used and may be perceived differently in terms of risk. Future iterations of STaRT will consider expanding content to address a broader range of tobacco products to enhance relevance for international audiences.
Conclusions
The early success of STaRT in improving knowledge, achieving broad reach, and generating strong participant satisfaction demonstrates the potential for a scalable model for strengthening the tobacco recovery workforce in Kansas and beyond. There is a need for continued education and integration of programs like STaRT into workforce training.
Footnotes
Acknowledgements
We wish to thank the training development workgroup and collaborators who provided feedback at various stages of the curriculum development. These include Bob Tryanski, Lisa Cyrus, Dee Vernberg, Laura McCulloch, Asley Grill, Nicole Passafume, Rick Cagan, Carrie Billbe, Teresa Cornejo, Danny Barrera, Hope Krebill, Karla Van Goethem, Lety Sarmiento, Mariana Ramirez, Mariana Hildreth, Paula Cupertino, Francisco Cartujano, Arlette Chavez, Doug Adams, Matthew Schrock, Kim Jordan, Sheri Hall, Darla Denton, Andy Brown, Regina Anderson, Clint Sturky, Mary Greiner, and Allen Davis. ChatGPT was used for language polishing, and the authors verified the accuracy, validity, and appropriateness of all content generated by artificial intelligence.
Ethical Considerations
This work was approved as a quality improvement initiative by our institutional review board.
Author Contributions
Sharon Fitzgerald Wolff: conceptualization, data curation, formal analysis, methodology, validation, visualization, writing—original draft, and writing—review & editing.
Tresza D. Hutcheson: data curation, methodology, project administration, supervision, validation, writing—original draft, and writing—review & editing.
MeLinda Lair: investigation, project administration, supervision, validation, writing—review & editing.
Kimber P. Richter: conceptualization, data curation, investigation, methodology, project administration, funding acquisition, resources, software, supervision, validation, writing—original draft, and writing—review & editing.
Babalola Faseru: conceptualization, data curation, investigation, methodology, project administration, funding acquisition, resources, software, supervision, validation, writing—original draft, and writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The STaRT program was funded by the Kansas Health Foundation (Grant number: 201601004). The Kansas Department of Health and Environment provided funding for trainee scholarships.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
A de-identified dataset will be made available upon request.