
Abstract
Background:
Health care professionals (HCPs) are known to exhibit explicit and implicit biases toward individuals who use substances. However, it remains unclear whether these biases differ from those of the general population and, if so, when such differences emerge along the training continuum. This study examined whether implicit and explicit biases vary between the general population, health care learners (HCLs), and HCPs, and whether training and experience may modulate the congruence between these bias types.
Methods:
Participants included HCPs, HCLs, and members of the general populations recruited via crowdsourcing. All completed explicit bias instruments and an Implicit Association Test (IAT). Explicit bias scores underwent principal components analysis yielding 2 components: Prejudice (environmental biases) and Stigma Endorsement (personal negative attitudes). Component scores were compared across groups using one-way ANOVA. Fisher’s r-to-z transformations compared correlation coefficients between the 3 groups. Hierarchical multiple regression then examined explicit-implicit bias congruence while controlling for key covariates and profession, namely, medicine, nursing, paramedicine (ie, Emergency Medical Technicians, paramedics, and related roles).
Results:
The sample elicited moderate-to-strong negative biases overall. Groups did not significantly differ in explicit or implicit biases. However, HCPs exhibited significantly stronger correspondence between IAT and Prejudice scores (r = .38, P < .001) than HCLs (r = .10, P = .35) and the general population (r = .08, P = .23); the latter 2 groups did not significantly differ. This difference was maintained in the regression model controlling for key covariates.
Conclusions:
Although implicit and explicit bias toward individuals who use substances did not differ across HCP, HCL, and the general population, HCPs demonstrated significantly greater alignment of implicit and explicit bias scores. These findings suggest that training and professional experience may not be sufficient to reduce stigma toward this group. In fact, greater experience and environmental biases may be cyclically reinforced.
Highlights
Substance use bias was similar for health professionals/learners and the general public.
Perception, not endorsement of stigma, correlated with implicit bias.
This correlation was stronger for health professionals than for learners and the general public.
Introduction
Substance use disorders (SUDs) are chronic, relapsing conditions with serious personal and public health implications. 1 An estimated 40.3 million individuals in the United States are diagnosed with an SUD, yet only 6.5% receive treatment. 2 Even outside of the bounds of a diagnosable disorder, substance use is associated with significant health consequences, including overdose, injury, comorbid physical and mental health problems, and all-cause mortality, including suicide.3-5 Compounding these risks is persistent social stigma (ie, negative social attitudes) regarding substance use and the individuals who engage in it. Namely, individuals who use substances encounter disproportionate difficulties with housing, employment, and interpersonal relationships. 6 These effects are cyclical: Stigma reinforces barriers to care that then worsens outcomes; in turn, these negative outcomes reinforce stigma toward substance use.7,8
In addition to societal bias, individuals who use substances encounter significant stigma in health care settings. 9 A growing body of literature shows that health care professionals (HCPs) and learners (HCLs; we use this term to refer to individuals of all levels of training but not yet licensed or independently practicing [eg, medical or nursing students, residents, EMT trainees]) often hold negative attitudes toward those with SUDs.9-11 This stigma often manifests in clinical decision making, including diagnostic overshadowing, or the misattribution of symptoms to substance use.12,13 These biases may lead to suboptimal care, delayed treatment, and poorer health outcomes for individuals with SUDs due to inaccurate or inadequate treatment planning and/or reduced empathy.6,14,15 Determining how these attitudes develop and persist is essential to identifying and dismantling barriers to equitable care.
One avenue to understanding the development and continuance of these biases is to identify at which stage of professional development, if any, these biases may develop or diverge from the general population. Doing so is essential to determine how, or whether, clinical training exacerbates or reduces personally held negative attitudes. More specifically, it is presently unknown if stigma is intensified or reduced through exposure to patients, modeling from supervisors, or the demands of clinical practice. Pinpointing whether, when, and how these attitudes emerge or change can help identify the most effective intervention points.
Measurement of Stigma
Most available measures of stigma toward substance use focus on public stigma—the awareness of ambient biases toward a population—with fewer assessing stigma endorsement, or a personal endorsement of those attitudes. 16 Relatedly, implicit biases—measured via behavioral task instead of self-report—reflect the strength of automatic associations that mirror a blend of public stigma and stigma endorsement (eg, more quickly pairing substance-related terms with negative descriptors than positive).17,18 Explicit biases reflect consciously endorsed attitudes (eg, agreement with statements on a questionnaire describing individuals with SUDs as manipulative or unmotivated). 19 Explicit and implicit measures are thought to index different components of biases and, as such, do not always correspond; assessing both may provide a more comprehensive understanding of stigmatized attitudes within a population. 18 Most research on substance use–related stigma among health care workers has relied on self-reported explicit bias data, with providers often viewing patients with SUDs as manipulative, unmotivated, and morally deficient.9,10 Limited prior work with implicit biases in samples of HCPs and HCLs have demonstrated their advantages. For example, a recent pilot study of Canadian health care professionals and faculty demonstrated greater overall implicit than explicit biases toward individuals who use substances. 20 Among nurses working in addiction treatment settings, implicit bias scores were more predictive of intent to leave the profession than explicit measures. 21 In a sample of psychotherapists, explicit stigma predicted social distance, whereas implicit bias was stronger than explicit in predicting willingness to write clinical support letters for clients with SUDs. 22 No study has compared implicit biases of health care workers and the general public, nor has any compared stages of training such as students versus professionals. Therefore, it is unclear whether health care workers’ substance use–related biases differ from those of the general population. Some evidence suggests that individual implicit biases are more likely to change than systemic biases: They change to reflect systemic prejudices and not the other way around.23,24 As a result, implicit biases may better reflect the attitudes of groups than those of individuals.25,26 It has been hypothesized that this convergence may be particularly true in health care settings.27,28 However, this hypothesis has yet to be directly tested in the context of substance use.
Present Study
This study had 2 aims. First, we aimed to establish whether implicit and explicit biases differ across the general population, HCLs, and HCPs. The second aim was to determine whether congruence between implicit and explicit measures varies across these groups. We hypothesized that increased contact with individuals with SUDs, as well as greater levels of education and professional training and norms (eg, emphasizing nonjudgmental care) would result in lower explicit and implicit bias scores in HCL and HCPs than in the general population.29,30 We further hypothesized that the congruence between implicit and explicit measures (ie, the correlation between implicit and explicit bias scores) would be stronger for HCPs than for HCLs and that this stronger association would emerge independent of profession—medicine, nursing, or paramedicine (emergency medical services personnel, including Emergency Medical Technicians and paramedics) 31 —across the health care training continuum.
Methods
Study Design, Setting, and Recruitment
Participants were recruited from Prolific (www.prolific.com), a crowdsourcing platform that focuses on academic research. We recruited participants in 3 waves in February 2025: (a) a general population sample; (b) HCLs (based on previous screening surveys submitted to Prolific that they were current medical, nursing, or paramedical students); (c) HCPs (defined as licensed or license-eligible practitioners in these fields), based on responses to the same survey. Health care learners (HCLs) were defined as individuals currently engaged in training within a health care profession (eg, medical, nursing, or paramedical students or trainees), based on self-report. All participants were US residents. Paramedicine was included due to similar professional demands and previously documented patterns of bias. Group classification was determined by screening questions at the start of the study, and HCPs/HCLs then selected their profession from a list of 11 professions. Only those that selected medicine, nursing, and paramedicine were included. A priori power analyses suggested we needed approximately 80 to 90 participants per group to power medium effect sizes in the planned correlation and regression models; we exceeded this minimum to power smaller effect sizes. A total of 503 participants consented and began the study; 37 returned the study rather than completing it. Eighteen additional participants were removed for incomplete data or missing more than one attention check (eg, “select ‘strongly agree’”), leaving a final sample of 447. One included participant did not answer one item on the Perceived Stigma of Addiction Scale (PSAS); this datum was replaced using the mean of their remaining responses on the scale; there were no other missing data in the analytic sample.
Participants identifying as students and other trainees were classified as HCLs (n = 97), those identifying as professionals were categorized as HCPs (n = 105), and all others as general population (n = 245). One participant identified as a physician assistant and was retained in the HCP sample as a physician given broadly similar clinical roles and settings. Most HCPs were nurses (71%), whereas most of the HCLs were medical students (54%), a significant difference in distribution, χ2(3) = 19.27, P < .001, V = 0.31. Further descriptive statistics of this sample are presented in Table 1.
Demographic and Descriptive Statistics For Each Group and the Total Sample.
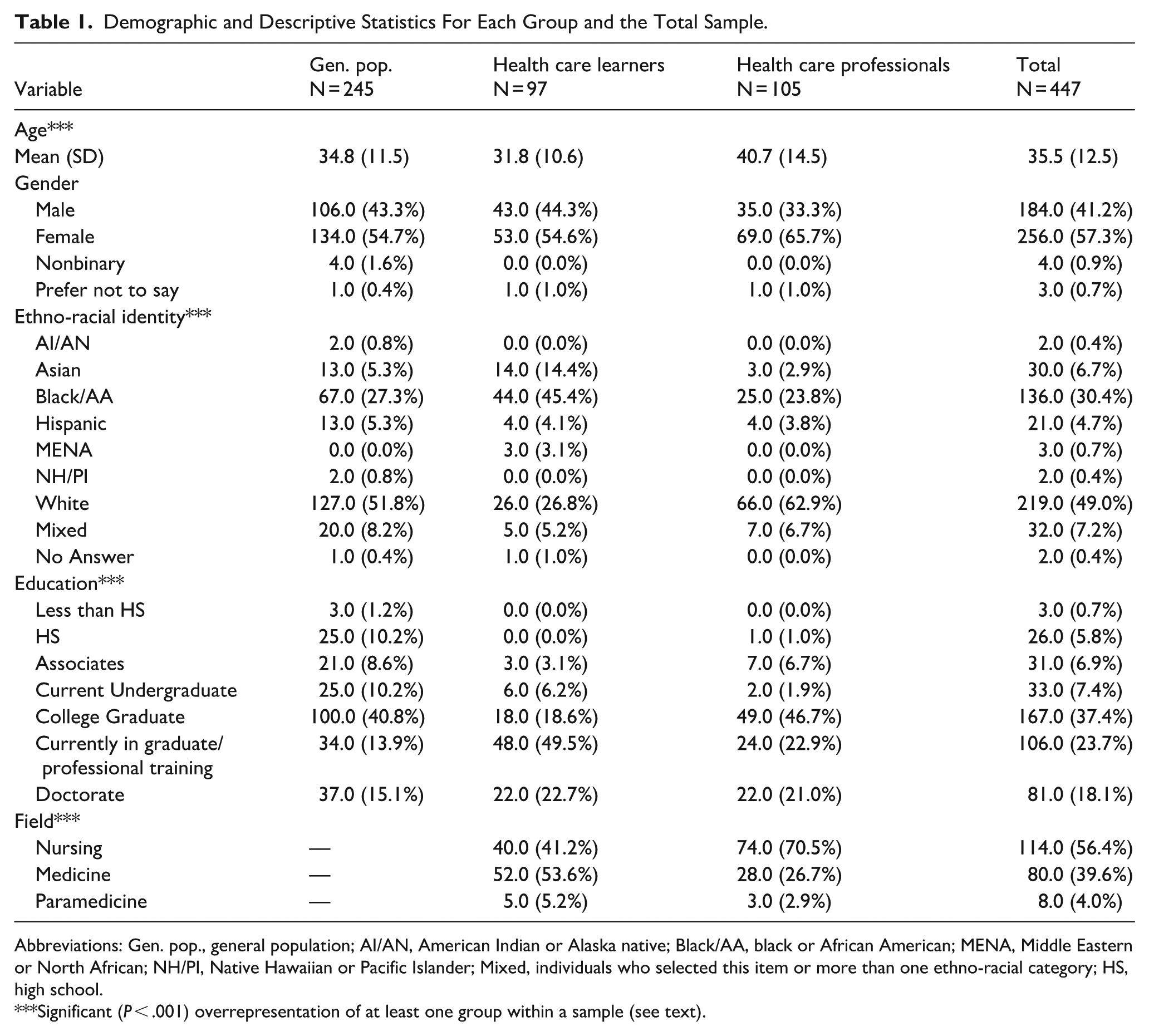
Abbreviations: Gen. pop., general population; AI/AN, American Indian or Alaska native; Black/AA, black or African American; MENA, Middle Eastern or North African; NH/PI, Native Hawaiian or Pacific Islander; Mixed, individuals who selected this item or more than one ethno-racial category; HS, high school.
Significant (P < .001) overrepresentation of at least one group within a sample (see text).
Implicit Measures
We generated an Implicit Association Task (IAT) using IATgen (www.iatgen.org), a free, web-based tool for generating in-line code to administer an IAT within Qualtrics. 32 The task followed the standard IAT structure and scoring algorithm. 17 Stimuli were adapted and supplemented from previous work.20,33 Description of stimuli and their limitations are presented in Supplemental Appendix 1. IATgen-generated D-scores were used as the dependent variable in all analyses. More positive D-scores indicate stronger negative implicit associations. The Spearman-Brown corrected split-half reliability was good (0.873).
Explicit Measures
Stigma Endorsement
The 10-item Attitudes Toward Injecting Drug Use (ATIDU) and the 4-item Perceived Controllability of Drug Use (PCDU) 34 were used to assess personal distaste to substance use. To match American English usage, we changed “injecting drug” to “injection drug.” Items were rated on a 5-point Likert scale from strongly disagree to strongly agree. Sample ATIDU items include “Injection drug use is just plain wrong,” whereas the PCDU items include “Injection drug users are responsible for their addiction.” Both scales showed acceptable internal consistency (ω > 0.66). Higher scores indicate greater negative attitudes toward (injection) drug use.
Public Stigma
We used the 8-item PSAS35,36 to measure public stigma. The PSAS asks respondents to rate agreement with statements about how often they believe stigmatizing views are expressed by others (eg, “Most people would willingly accept someone who has been treated for substance use”), using a 7-point Likert scale from strongly disagree to strongly agree. Internal consistency was good (ω = 0.82). Higher scores reflect greater perception of social stigma attitudes.
General (Traditional) Prejudice
The heroin item from the Attitudes Toward Mental Illness Questionnaire (AMIQ) 37 was included as a general assessment of attitudes toward this behavior. The item provides a brief vignette followed by 5 questions: “Pat has been injecting heroin daily for one year.” Questions combine elements of social distance, perceived consequences, and stereotyped expectations, for example, “Do you think that this would damage Pat’s career?” and “How likely do you think it would be for Pat to get in trouble with the law?” Items were scored on a 5-point scale and recoded from −2 to +2, depending on item wording, where higher scores reflect more positive or accepting attitudes. Internal consistency was acceptable on the measure (ω = 0.71).
Social Desirability
We included the 16-item Social Desirability Scale–17 (SDS-17) to assess the tendency to present oneself in an impossibly flattering light. 38 We presented items on a 5-point Likert scale ranging from strongly disagree to strongly agree. 39 Sample items include “I sometimes litter” and “In traffic, I am always polite and considerate of others.” Item 4 (regarding substance use) was omitted per the original author’s recommendation. The scale demonstrated good internal consistency in the present sample (ω = 0.84). Higher scores reflect greater social desirability bias.
Personal Substance Use History
To control for personal substance use, participants indicated lifetime use of the following: alcohol, tobacco, cannabis, cocaine, amphetamines, inhalants, sedatives, hallucinogens, opioids, and “other” based on the WHO ASSIST. 40 To index exposure to less common and more stigmatized substances, we summed endorsement of lifetime use of cocaine, amphetamines, inhalants, sedatives, hallucinogens, and opioids. We excluded alcohol, tobacco, cannabis, and “other” substances from this composite due to their higher prevalence and comparatively lower stigma. Fifteen respondents selected “other” substances: “N/A” or similar (n = 9; omitted), “DMT” (n = 1; recoded to “hallucinogen”), “medication for treatment” (n = 1; omitted), Tramol (n = 1; recoded to “opioid”), caffeine (n = 1; omitted), tranquilizers (n = 1; recoded to “sedatives”), and alcohol (n = 1; recoded to “alcohol”).
Procedures
After selecting the study and completing written informed consent, participants then completed the self-report questionnaires (in a randomized order), followed by the IAT, and then demographics. Data were collected January and February 2025 using Qualtrics (Qualtrics, Inc, Provo, UT, USA). The Institutional Review Board of Thomas Jefferson University reviewed and exempted these procedures (control # 21G.951).
Data Analysis
We first computed Pearson correlations across the full sample to examine associations among all variables. A one-sample t-test confirmed IAT D-scores differed from zero and provided an effect size estimate for the sample. To reduce dimensionality and simplify interpretation, we performed a principal components analysis (PCA) with Promax rotation on the ATIDU, PCDU, PSAS, and AMIQ-H scales. The PCA revealed 2 interpretable components: Component 1, comprising the ATIDU and the PCDU, reflected Stigma Endorsement; Component 2, comprising the PSAS and the AMIQ-H, reflected Prejudice (public stigma). Component scores were used in subsequent analyses. Next, group differences were assessed using 3 one-way ANOVA with group (general population, HCL, and HCP) as the independent variable and the IAT D-scores, Prejudice, and Stigma Endorsement entered as dependent variables. We conducted correlations within each of the 3 groups (general population, HCL, HCP) and compared the coefficients using Fisher’s r-to-z tests. Finally, we conducted a hierarchical multiple regression in 3 blocks with IAT D-scores as the dependent variable: (a) Prejudice, group (HCL, HCP), profession (medicine, nursing, paramedicine), SDS, age, and gender; (b) the Prejudice × Group interaction term; and (c) the Prejudice × Profession interaction. Block 1 tested the main association between Prejudice and IAT D-scores controlling for key covariates. Block 2 tested whether this association differed between HCLs and HCPs, and Block 3 tested whether the difference between HCL and HCP varied by profession. We conducted an identical model with Stigma Endorsement, though all results within that analysis were null (see Supplemental Appendix 2). The general population sample was omitted from the regression analyses to focus on training level and because profession was not applicable for this group.
Data and Code Availability
Data and IATgen code are available at https://osf.io/7xtbk/overview?view_only=4c04df9c5a6c45959575cabb6f656b78.
Results
Significant group differences emerged across age, gender, ethno-racial identity, education, and health care field composition (all Ps < .001). HCPs were older on average than HCLs and the general population. HCPs also included a higher proportion of women. Ethno-racial composition differed across groups, with the general population sample appearing more heterogeneous than either HCLs or HCPs; HCLs showed greater representation of black/African American participants, and HCPs showed greater representation of white participants. Differences in education level were consistent with expected training status across groups.
Alcohol, tobacco, and cannabis use were highly prevalent in the sample (89%, 53%, and 53%, respectively), whereas endorsement of other substances was comparatively less common (ranging from 8.5% to 29.5%, with most substances endorsed by fewer than 25% of the sample).
Descriptive statistics of questionnaire and IAT scores are presented in Table 2. The mean IAT D-score was 0.520 (SD = 0.451), reflecting moderate-to-strong negative biases toward individuals who use substances compared with those who do not. This score significantly differed from zero with a large effect size (t446 = 24.36; P < .001, d = 1.15). Table 3 presents correlations among all variables. Correlations were moderate to strong and in expected directions, supporting the use of the PCA described above. Results of one-way ANOVA indicated no significant group differences in component scores, IAT D-scores, or any questionnaire, all Fs < 1.0, Ps > .30.
Descriptive Statistics for Each Questionnaire (Mean [standard deviation]) for Each Scale for the General Population Sample, HCLs, HCPs, and the Whole Sample.
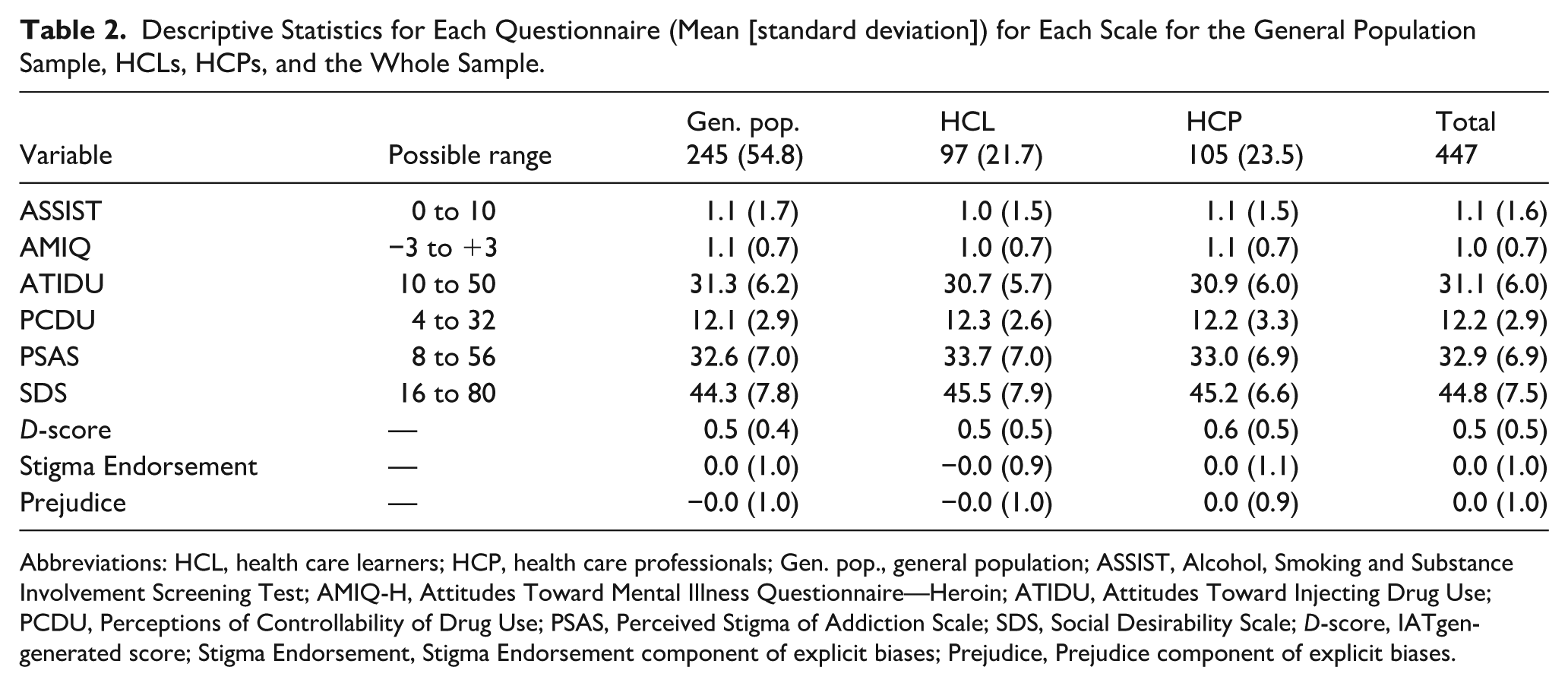
Abbreviations: HCL, health care learners; HCP, health care professionals; Gen. pop., general population; ASSIST, Alcohol, Smoking and Substance Involvement Screening Test; AMIQ-H, Attitudes Toward Mental Illness Questionnaire—Heroin; ATIDU, Attitudes Toward Injecting Drug Use; PCDU, Perceptions of Controllability of Drug Use; PSAS, Perceived Stigma of Addiction Scale; SDS, Social Desirability Scale; D-score, IATgen-generated score; Stigma Endorsement, Stigma Endorsement component of explicit biases; Prejudice, Prejudice component of explicit biases.
Pearson Correlations of the Main Variables of Interest for the Whole Sample.

Abbreviations: IAT, D-score of the Implicit Association Task; AMIQ, Attitudes Toward Mental Illness Questionnaire; PCDU, Perceived Controllability of Drug Use; PSAS, Perceived Stigma of Addiction Scale; SDS, Social Desirability Scale–17; ASSIST, World Health Organization Alcohol, Smoking, Substance Involvement Screening Test; Endorsement, Personal stigma endorsement component score; Prejudice, Prejudice component score.
P < .05, **P < .01, ***P < .001.
Comparing Congruence of Explicit and Implicit Bias
Prejudice scores were significantly correlated with D-scores in the full sample (r = .15, P = .002). At the subgroup level, this association was significant among HCPs (r = .38, P < .001) but not among HCLs (r = .10, P = .35) or the general population (r = .08, P = .23). Fisher’s r-to-z tests indicated that the correlation was significantly stronger for HCPs than for HCLs (P = .031) and the general population (P = .005), with no statistical difference between HCLs and the general population (P = .868).
Table 4 presents the regression results comparing the association of Prejudice and IAT D-scores between HCL and HCPs. As shown, in Block 1, the association between Prejudice and IAT was significant after controlling for key covariates. Adding the Prejudice × Group (HCL vs HCP) interaction in Block 2 significantly improved model fit. Simple effects analyses showed that Prejudice was positively associated with IAT D-scores significantly for HCPs but not HCLs. This pattern indicates greater congruence between explicit and implicit bias for HCPs than for HCLs, consistent with the correlation analyses above. Adding the Prejudice × Profession (nursing and paramedicine vs medicine) interaction in the third model did not improve model fit. Omitting the lone physician assistant did not alter the magnitude or statistical significance of these effects. Thus, the stronger Prejudice-IAT congruence observed among HCPs was not explained by specific professions within the HCP group, but by training status (professional vs learner).
Results of Hierarchical Regression.
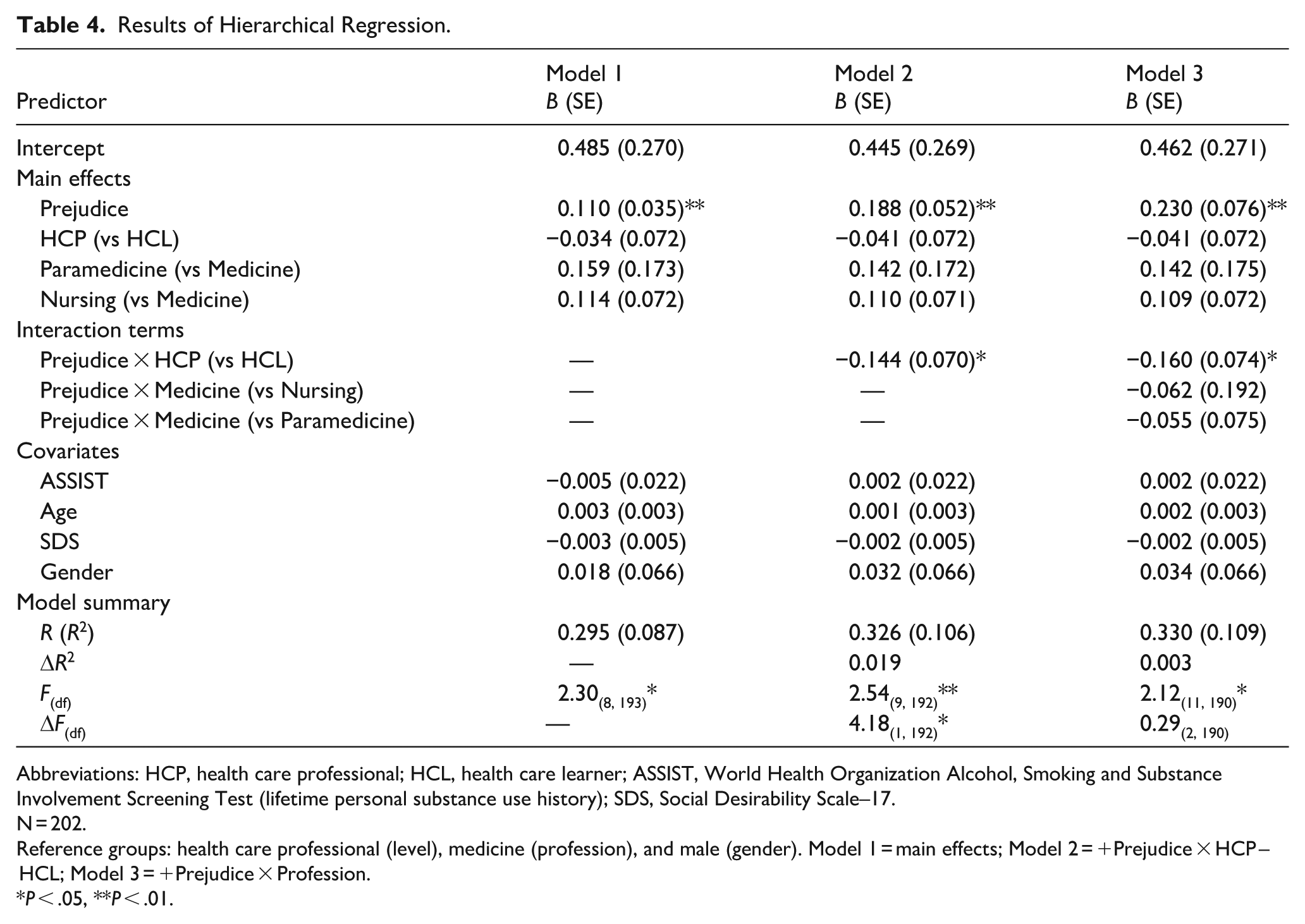
Abbreviations: HCP, health care professional; HCL, health care learner; ASSIST, World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (lifetime personal substance use history); SDS, Social Desirability Scale–17.
N = 202.
Reference groups: health care professional (level), medicine (profession), and male (gender). Model 1 = main effects; Model 2 = +Prejudice × HCP – HCL; Model 3 = +Prejudice × Profession.
P < .05, **P < .01.
Discussion
We had 2 central hypotheses in the present study. First, compared with the general population, we believed that HCL and HCP would report lower explicit and implicit bias related to individuals with SUDs. This hypothesis was not supported. Instead, HCP, HCL, and the general population reported statistically similar scores. Second, we hypothesized that the congruence (ie, correlation) between implicit and explicit scores would be significantly higher for HCPs than for HCLs, and both would report higher scores than the general population. This hypothesis had partial support: HCPs displayed significantly higher correspondence between implicit and explicit bias scores than the HCL and general population groups, but the HCL group did not significantly differ from the general population. Consistent with correlations, the difference between HCL and HCPs persisted independent of social desirability, personal substance use history, and profession (medicine, nursing, or paramedicine). Taken together, the results clarify how implicit and explicit biases toward individuals with SUDs vary across stages of professional training and highlight that, in many respects, HCLs and HCPs resemble the general population.
The first key finding of this study is that those working in health care—namely, medicine, nursing, and paramedicine—exhibited comparable levels of substance use–related biases to the general population. This is the first study to directly examine implicit and explicit biases in both HCLs and HCPs, as well as the first to compare these groups to a general sample. 9 These findings suggest that health care training and experience alone are unlikely to shift these biases. Individuals who pursue careers in health care are characterized by higher educational attainment and achievement, empathy, and other personality characteristics that could reduce biases toward individuals with SUDs and other stigmatized populations.41-44 Yet, in the present sample, these assumed traits did not influence responses on the explicit or implicit measures. Interestingly, although increased time and contact with stigmatized populations are key drivers of changes in explicit and implicit biases in health care professions,45,46 HCPs (who, by definition, have more experience) did not differ from learners or the general population. Taken together, these findings suggest that characteristics often associated with health care professionals—namely, empathy and education—may not translate to reduced stigma toward individuals with SUDs. Future work should directly measure both these traits and the type and quality of contact with individuals with SUDs to determine whether they, rather than training stage alone, shape bias.
The second key finding is that the congruence between implicit and explicit bias was stronger for HCPs than for HCLs even after controlling for key covariates. HCPs also exhibited significantly greater correlation coefficients than HCLs and the general population controlling for both SDS and personal substance use. These findings dovetail with previous work, suggesting that implicit attitudes and ambient environmental stigma are cyclically reinforced,23,24 which some suggest extends into health care settings. 28 In contrast, the Contact Hypothesis predicts that recurring contact—under supportive conditions—reduces prejudice by fostering empathy and humanization of stigmatized groups. 47 Although some evidence supports this effect among HCPs working with individuals with SUDs and other psychiatric disorders,30,46 the stronger Prejudice-IAT correspondence for HCPs than for HCLs suggests that, rather than buffering against stigma, continued involvement within health care environments—where negative stereotypes of people with SUDs are often institutionalized or normalized9,10—may strengthen the coupling of explicit and automatic biases. This convergence likely reflects professional context, exposure, and demand. Compared with HCLs, HCPs are more often witness to, or are required to make, clinical decisions involving individuals with SUDs in environments with embedded biases. Over time, these experiences may heighten awareness of ambient prejudice that eventually become aligned with their own implicit biases.
Finally, although perceived and personal stigma overlap, it is not clear why the Prejudice component corresponded to IAT scores but Stigma Endorsement did not.36,48 One likely explanation is that our questionnaires were specific to injection drug use (ie, the ATIDU and the PCDU) and may not have captured associations with the broader substance-related stimuli used in the present IAT. We selected these instruments for their psychometric strength 16 and previous evidence of correspondence with implicit measures.21,33 Despite growing recognition of the need to assess stigma toward SUDs, validated instruments of stigma endorsement remain scarce, often demonstrating poor psychometric properties, and a focus on specific substances rather than on substance use more generally. 16 Implicit measures and explicit measures capture complementary yet distinct components of these attitudes and both are necessary to fully elucidate the mechanisms that underlie stigma. 18
Limitations
Although this study provides insight into both explicit and implicit biases between HCLs and HCPs, there are some limitations that should be considered. First, we recruited from Prolific, which limited availability to those with access to that service. Professional status was self-reported, which could lead to inconsistencies in how subjects identified their roles. Further, we did not distinguish between stages of training or levels of professional experience, which should be considered in future work. It was also impossible to verify a participant’s profession, duration of training and/or professional service. Given the growing number and frequency of substance-related education and training HCLs, 49 and continuing education for HCPs, 50 future work should consider including exposure to such interventions to test their effectiveness and impact on bias. Additionally, though our explicit measures corresponded to some vignette-based measures in the AMIQ, 37 we did not assess how these biases relate to clinical judgment and behavior. The professional and sociodemographic representation across all groups was not as balanced as we had hoped. It was also beyond the scope of this study to consider sociodemographic variables (eg, race). Given the diversity within the samples, and the steadily diversifying health care field, 51 it is worth considering these important lived experiences in future work. Finally, the present study examined substance-use stigma broadly, which may mask meaningful differences in attitudes and associations across substances, routes of administration, and other contextual factors (eg, cannabis vs heroin; pills vs injections). Future work should examine these distinctions directly.
Conclusions and Clinical Implications
Despite increased attention to bias in health care education and training, these findings suggest that health care training and experience alone may not have been sufficient to differentiate groups in the present sample. 52 Many interventions feature contact with individuals who use substances, which shows some evidence of efficacy in health care settings.30,53 However, many of these interventions are brief (often single session workshops), heterogeneous in structure and targeted substance, and lack long-term follow-up.9,49 These findings highlight the importance of examining how training, exposure, and clinical context may relate to stigma, and suggest directions for future research and curriculum development. One potential implication is that structured opportunities to practice clinical decision making that integrates knowledge of substance use may be a useful direction for training and future research. Finally, the collection of explicit and implicit measures used in the present study could be useful for educators designing and evaluating anti-stigma curricula, though the development of additional explicit measures that are more targeted to health care learners might be useful to support evaluation of these curricula. Given that these data were cross-sectional, an important next step will be to collect longitudinal data to confirm whether, and how, the congruence of implicit and ambient biases influence one another over time.
Supplemental Material
sj-docx-1-saj-10.1177_29767342261456153 – Supplemental material for Implicit and Explicit Bias Toward Substance Use: A Cross-Sectional Study Comparing Health Care Professionals, Trainees, and the Public
Supplemental material, sj-docx-1-saj-10.1177_29767342261456153 for Implicit and Explicit Bias Toward Substance Use: A Cross-Sectional Study Comparing Health Care Professionals, Trainees, and the Public by Erik M. Benau and Jillian H. Zavodnick in Substance Use & Addiction Journal
Footnotes
Acknowledgements
The authors wish to acknowledge Rebecca Jaffe for her contribution to this work.
Ethical Considerations
This research was conducted ethically in accordance with the Declaration of Helsinki. The Institutional Review Board of Thomas Jefferson University reviewed these procedures and declared them exempt (control # 21G.951).
Consent to Participate
Participants provided written informed consent prior to participation.
Author Contributions
EMB contributed to conceptualization, formal analysis, investigation, methodology, project administration, validation, visualization, writing (original draft), and writing (review and editing). JHZ contributed to conceptualization, funding acquisition, investigation, methodology, project administration, and writing (review and editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based upon work supported by an Alliance for Academic Internal Medicine Innovation Grant, 2020-2021. The supporting organization had no further role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Zavodnick was a paid consultant for a medical education product, Osmosis, owned by Elsevier, until June 2025.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.