
Abstract
Background:
The global resurgence of methamphetamine use disorder (MUD) represents a critical public health challenge, characterized by high morbidity and a lack of approved pharmacotherapies. Treatment research spans diverse domains, but a comprehensive synthesis of the scope, efficacy, and interrelationships of these approaches is lacking.
Objective:
To systematically map and synthesize the available evidence on interventions for MUD, including their efficacy, mechanisms, and the overall structure of the research landscape.
Methods:
Following the Arksey and O’Malley framework and PRISMA-ScR guidelines, we conducted a systematic search of 5 electronic databases (MEDLINE, Embase, CENTRAL, PsycINFO, CINAHL) from inception to October 2025. We included studies of any design evaluating interventions for MUD in human populations.
Results:
From 6852 screened records, 62 studies were included. Our synthesis reveals a tripartite intervention landscape: (1) Behavioral interventions, particularly contingency management (CM), demonstrate the most robust efficacy, increasing abstinence rates by 40% to 60%. (2) Pharmacological approaches show promise with combination therapy (naltrexone-bupropion and Wellbutrin), significantly increasing methamphetamine-negative urine samples versus placebo (11.4% vs 5.7%), though effect sizes are generally modest. (3) Neuromodulation, specifically repetitive transcranial magnetic stimulation targeting the dorsolateral prefrontal cortex, consistently reduces cue-induced craving by 25% to 35%. Critical moderators of treatment response were identified, including the OPRM1 A118G polymorphism and high rates of polydrug use (up to 42% in opioid use disorder cohorts), which predicts poorer outcomes. Implementation feasibility and intervention fidelity are critical considerations, particularly for CM and pharmacotherapy adherence.
Conclusion:
Effective MUD management requires a multimodal, personalized framework. While CM remains a foundational behavioral strategy, advances in combination pharmacotherapy and neuromodulation offer new avenues for targeting core neurobiological deficits. Future research must prioritize integrated treatment platforms, implementation science to scale effective interventions like CM, and personalized strategies informed by genetics and neuroimaging.
Keywords
Highlights
Contingency management is the most effective behavioral treatment for methamphetamine use.
Naltrexone-bupropion is the leading pharmacotherapy for methamphetamine use disorder.
Brain stimulation reduces drug craving by targeting cognitive control circuits.
Personalized, combination therapy is essential for improving patient outcomes.
Introduction
Methamphetamine use disorder (MUD) is a pressing global public health crisis, marked by rising prevalence, significant morbidity, and a substantial burden on healthcare systems.1,2 Polydrug use complicates clinical management and is common among individuals with opioid dependence, influencing treatment outcomes. 3 Patterns of administration, including injection versus smoking, further impact health risks and engagement in care. 4 Resurgent use at treatment admission highlights the ongoing challenges in addressing MUD effectively. 5
The neuropathology of MUD involves profound dysregulation of dopaminergic, glutamatergic, and serotonergic circuits, leading to impaired reward processing, executive function, and inhibitory control.6,7 These deficits contribute to high rates of relapse and make treatment exceptionally challenging. Cognitive deficits in working memory and decision-making are well documented and influence treatment efficacy. 8 Gender differences in pharmacokinetics, craving, and response to treatment are evident, emphasizing the importance of sex-specific strategies. 9 Preclinical and clinical evidence further supports sex differences in treatment response. 10 Genetic variants, including SLC18A1, SLC18A2, BDNF, FAAH, and OPRM1 polymorphisms, contribute to individual susceptibility and treatment outcomes.11,12 Studies of gene-cognition interactions underscore the importance of integrating genetic and neurocognitive factors in clinical approaches. 12
The intervention landscape for MUD is complex and rapidly evolving. Pharmacological research has progressed from monotherapies to novel combinations and agents targeting neuroinflammation. 13 Sustained-release methylphenidate has shown moderate benefits in multicenter trials. 14 Dexamphetamine maintenance has been tested for treatment-resistant patients. 15 Topiramate has demonstrated potential in reducing methamphetamine use. 16 Ibudilast modulates neuroinflammation and shows promise in attenuating methamphetamine-induced physiological effects.17,18 Ifenprodil has been evaluated as an exploratory treatment in randomized trials.19,20 Lisdexamfetamine has also been investigated for reducing methamphetamine dependence. 21 Nicotinic agonists can suppress methamphetamine-seeking behavior in preclinical models. 22 N-acetylcysteine is being tested for its adjunctive therapeutic potential. 23 Pharmacogenetic approaches, including prospective A118G polymorphism evaluation, offer insights for personalized treatment. 24
Behaviorally, contingency management (CM) stands as a highly efficacious yet often under-implemented intervention. 25 Mindfulness-based therapy reduces methamphetamine use and improves psychosocial outcomes. 26 Oxytocin-enhanced group therapy demonstrates preliminary efficacy in enhancing social bonding and supporting relapse prevention. 27 Resilience, aggression, and childhood trauma are influential psychosocial determinants of treatment outcomes.28,29 Personality traits and loneliness also shape treatment response. 30 Qualitative studies provide insights into patient experiences of relapse and treatment engagement.31,32
Digital and neuromodulatory approaches are emerging as adjunctive strategies. Virtual digital psychotherapist applications show feasibility in supporting treatment adherence. 33 Most recently, neuromodulation techniques like repetitive transcranial magnetic stimulation (rTMS) have emerged as promising tools for directly targeting the neural circuitry underlying craving and cognitive control.34-36 Complementary interventions, such as heart rate variability biofeedback, support emotional regulation. 37
Clinical outcomes are influenced by treatment retention, duration, and structural factors. Methamphetamine-induced psychosis is common and affects prognosis. 38 Duration of contingency management interventions is linked to treatment effectiveness. 39 Cross-national differences, including mandatory treatment policies, impact service utilization. 40 Cultural and socio-environmental factors, such as treatment availability in Japan, Australia, and Vietnam, affect engagement and relapse rates.41,42 Patterns of methamphetamine use in key populations, including adults living with HIV, further complicate treatment considerations. 43
Overall, MUD requires a multidimensional approach that integrates neurobiological, pharmacological, behavioral, digital, and psychosocial interventions. Addressing cognitive deficits, genetic predispositions, socioenvironmental determinants, and emerging therapeutic modalities is essential for improving outcomes and mitigating the public health burden of MUD.44-57
While numerous systematic reviews and meta-analyses have evaluated specific intervention classes, the field lacks a comprehensive mapping that synthesizes evidence across these disparate domains. A scoping review focused specifically on MUD interventions is necessary because methamphetamine presents unique neurobiological, behavioral, and psychosocial challenges distinct from other substance use disorders, requiring a targeted synthesis to guide clinical practice and research. A scoping review is uniquely suited to address this gap, illustrating the breadth of research activity, identifying key concepts and evidence clusters, and highlighting interactions between different treatment modalities. Therefore, this scoping review aims to systematically map and synthesize the available evidence on pharmacological, behavioral, and neuromodulation interventions for MUD, with the objective of characterizing the overall research landscape, synthesizing key findings on efficacy and mechanisms, and identifying critical gaps to inform future research and integrated care models.
Methods
Study Design
This scoping review was conducted according to the Arksey and O’Malley framework, 58 enhanced by subsequent methodological advancements by Levac et al 59 and reported following the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. 60
Research Question and Eligibility Criteria
The review was guided by the following primary research question: “What are the characteristics, scope, and key findings of evaluated interventions for methamphetamine use disorder?” and by the Population, Concept, Context (PCC) framework:
- Population: Human subjects with MUD.
- Concept: Any intervention for treating or reducing methamphetamine use or its harms, including pharmacological, behavioral, psychosocial, digital, and neuromodulation approaches.
- Context: Any geographical or clinical setting (e.g., outpatient, inpatient, community).
We included all study designs (eg, randomized controlled trials [RCTs], cohort studies, qualitative studies) but excluded editorials, conference abstracts, and non-English publications. The exclusion of non-English studies was based on feasibility constraints and the need to ensure accurate extraction of intervention-specific data, while acknowledging that this may reduce global representativeness.
Information Sources and Search Strategy
A systematic search was performed in MEDLINE, Embase, CENTRAL, PsycINFO, and CINAHL from inception to October 31, 2025. A sample search strategy for MEDLINE is provided (Table 1). We also searched clinical trial registries and reference lists of included articles.
Initial MEDLINE Search Strategy.
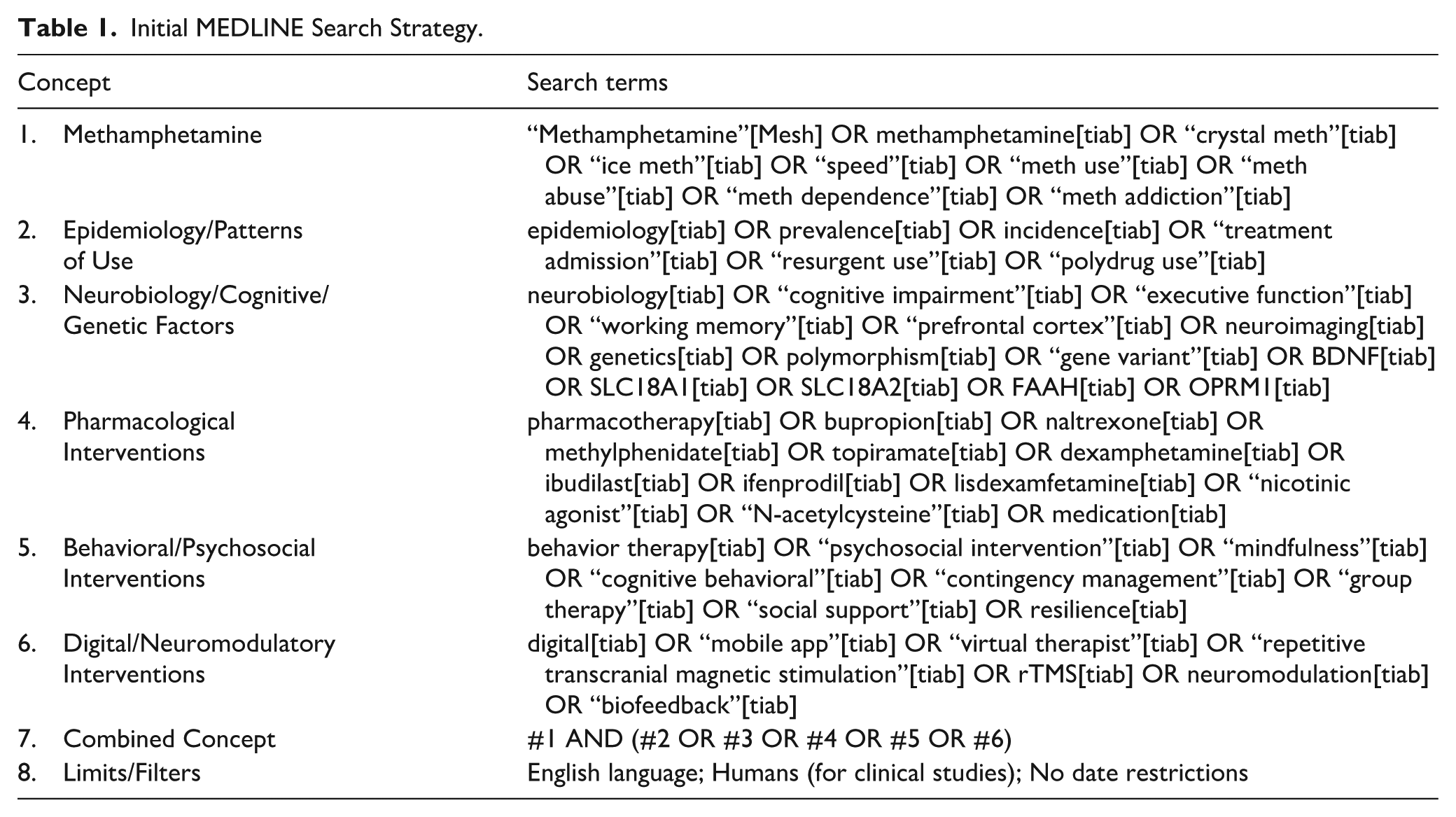
The search strategy utilized a combination of controlled vocabulary (eg, MeSH terms “Amphetamine-Related Disorders,” “Methamphetamine”) and free-text keywords related to “methamphetamine,” “intervention,” “treatment,” and “therapy.” The initial MEDLINE search strategy is provided in Table 1. To identify additional gray literature and unpublished studies, we searched clinical trial registries (ClinicalTrials.gov, WHO ICTRP) and scanned the reference lists of all included studies and relevant systematic reviews.
Selection of Sources of Evidence
Study selection was performed in duplicate by 2 independent reviewers using Covidence software. 61 Data were charted using a standardized form, extracting details on study characteristics, participants, interventions, and key findings.
Title and Abstract Screening: All retrieved citations were screened by 2 independent reviewers (Reviewer 1 and Reviewer 2) against the eligibility criteria.
Full-Text Review: The full-text of all potentially relevant articles was retrieved and assessed for final inclusion by the same 2 independent reviewers.
At both stages, any disagreements between reviewers were resolved through discussion or, if necessary, by adjudication from a third reviewer (Reviewer 3). The results of the search and selection process are presented in a PRISMA-ScR flow diagram. 62
Data Charting Process and Data Items
A standardized data extraction form was developed and piloted by the research team. Data from each included study was charted by 1 reviewer and verified for accuracy by a second reviewer. Discrepancies were resolved by consensus. The following data items were extracted:
Study characteristics: First author, publication year, country, study design, aims, and funding sources.
Participant characteristics: Sample size, demographic data (age, gender), MUD severity, and comorbidities.
Intervention details: Type of intervention (pharmacological, behavioral, etc.), specific regimen/dosage/protocol, duration, and comparator (eg, placebo, active control, treatment-as-usual).
Key findings: Primary and secondary outcomes related to methamphetamine use (eg, abstinence, reduced use, craving), retention in treatment, adverse events, and qualitative themes related to the intervention experience.
Critical Appraisal of Individual Sources
Consistent with the purpose of a scoping review to map the available evidence rather than synthesize efficacy, a formal critical appraisal of the methodological quality of individual sources was not conducted. This aligns with established scoping review methodology.58,59
Synthesis of Results
Consistent with scoping review methodology, a formal risk-of-bias assessment was not performed. Results were synthesized narratively and presented using summary tables and conceptual diagrams to map the evidence. The extracted data were analyzed using both quantitative and qualitative content analysis. The findings are presented in a narrative synthesis, structured around the key intervention categories identified (eg, pharmacological, behavioral, neuromodulation). To illustrate the distribution of the evidence, summary tables and conceptual maps are used to display the characteristics of the included studies, the range of interventions evaluated, and the relationships between intervention types and reported outcomes. This approach allows for the identification of key concepts, gaps in the literature, and areas for future primary research. Feasibility and fidelity of intervention implementation were also assessed when reported.
Limitations
This scoping review has several limitations. Restriction to English-language studies may have excluded relevant evidence. Database indexing variability and delays may have led to missed studies. Gray literature was not systematically searched, introducing potential publication bias. Additionally, the design prioritizes breadth over critical appraisal, limiting assessment of study quality and risk of bias.
Results Nicotinic
The systematic search and selection process identified 6852 records from electronic databases and other sources. After the removal of duplicates, 4915 titles and abstracts were screened for eligibility. Of these, 423 full-text articles were assessed, resulting in the final inclusion of 62 studies that met the predefined eligibility criteria for this scoping review (Table 2). The detailed flow of the search and selection process is documented in the PRISMA-ScR flow diagram (Figure 1).
Summary of Included References.
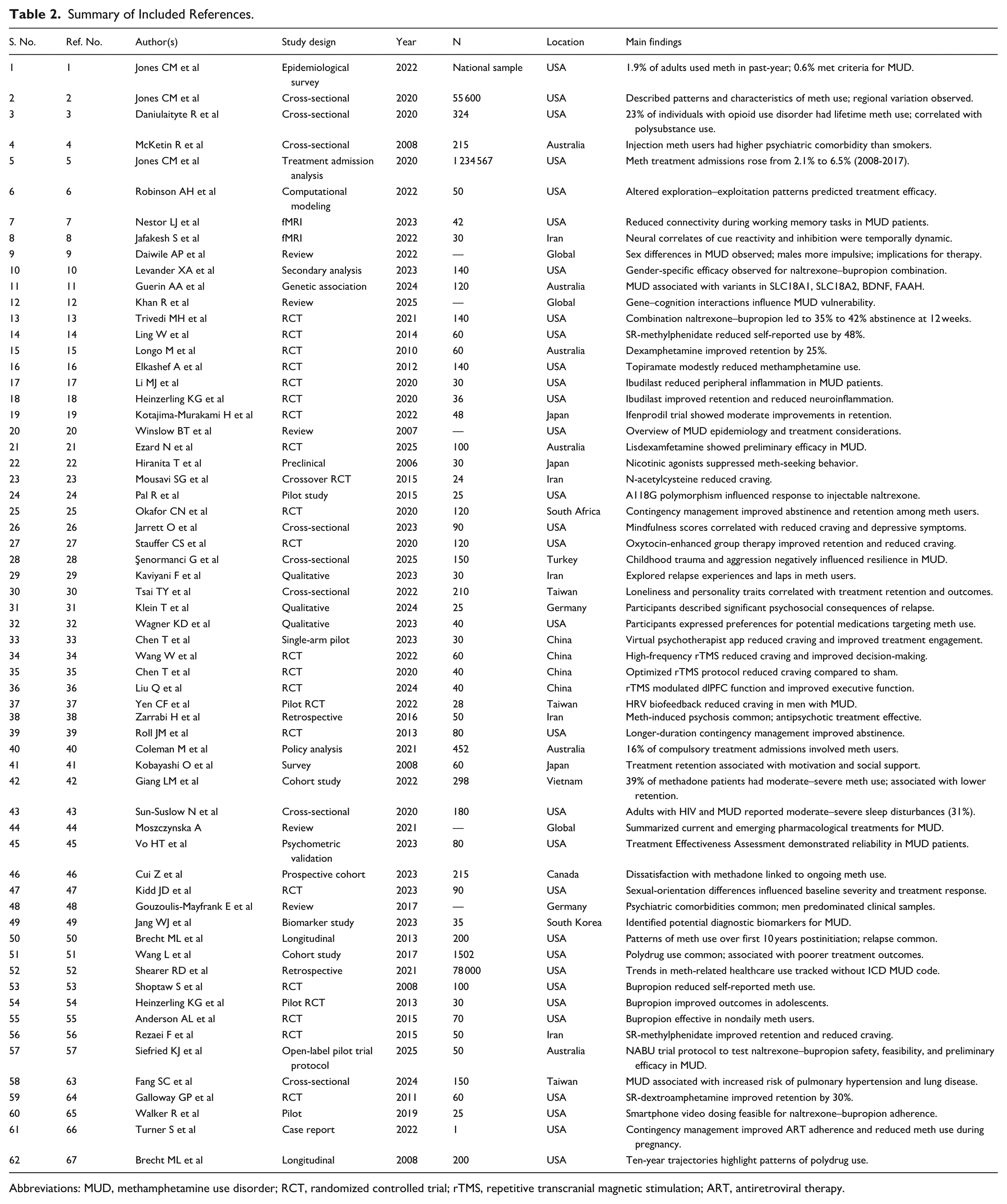
Abbreviations: MUD, methamphetamine use disorder; RCT, randomized controlled trial; rTMS, repetitive transcranial magnetic stimulation; ART, antiretroviral therapy.
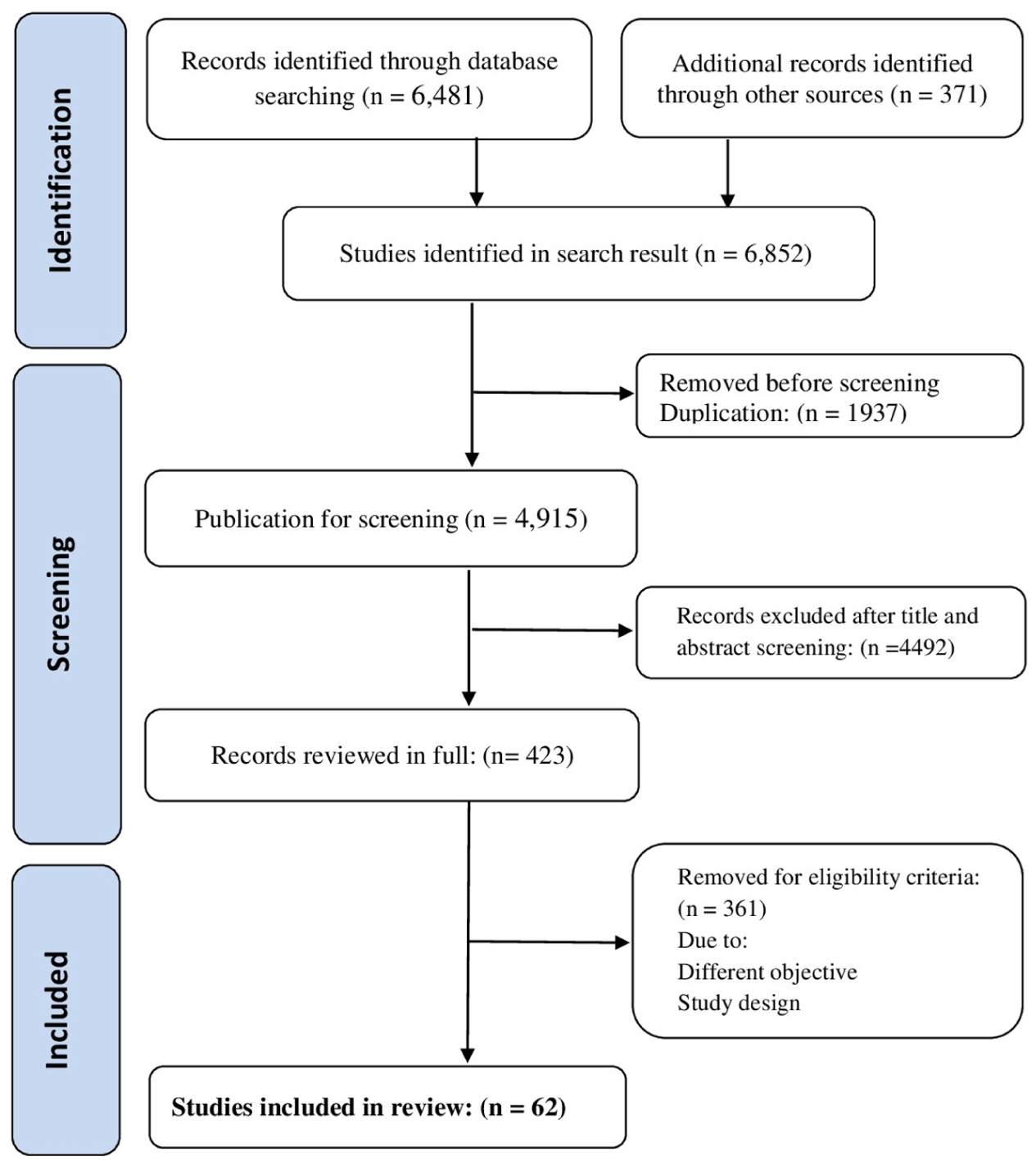
PRISMA-ScR flow diagram showing process for selection of included studies.
The 62 included studies were published between 2005 and 2025, with a notable concentration in the last 5 years (n = 38), reflecting a renewed research focus. The studies were conducted across diverse geographical regions, including the United States (n = 24), Asia (n = 12), Australia (n = 5), Europe (n = 3), and Africa (n = 2). Research designs were varied, comprising 35 RCTs, 12 cohort studies, 8 cross-sectional analyses, 5 qualitative studies, and 3 pilot feasibility studies. Sample sizes ranged from 1037 to 403 participants, 13 with a cumulative total of 5218 individuals across all studies.
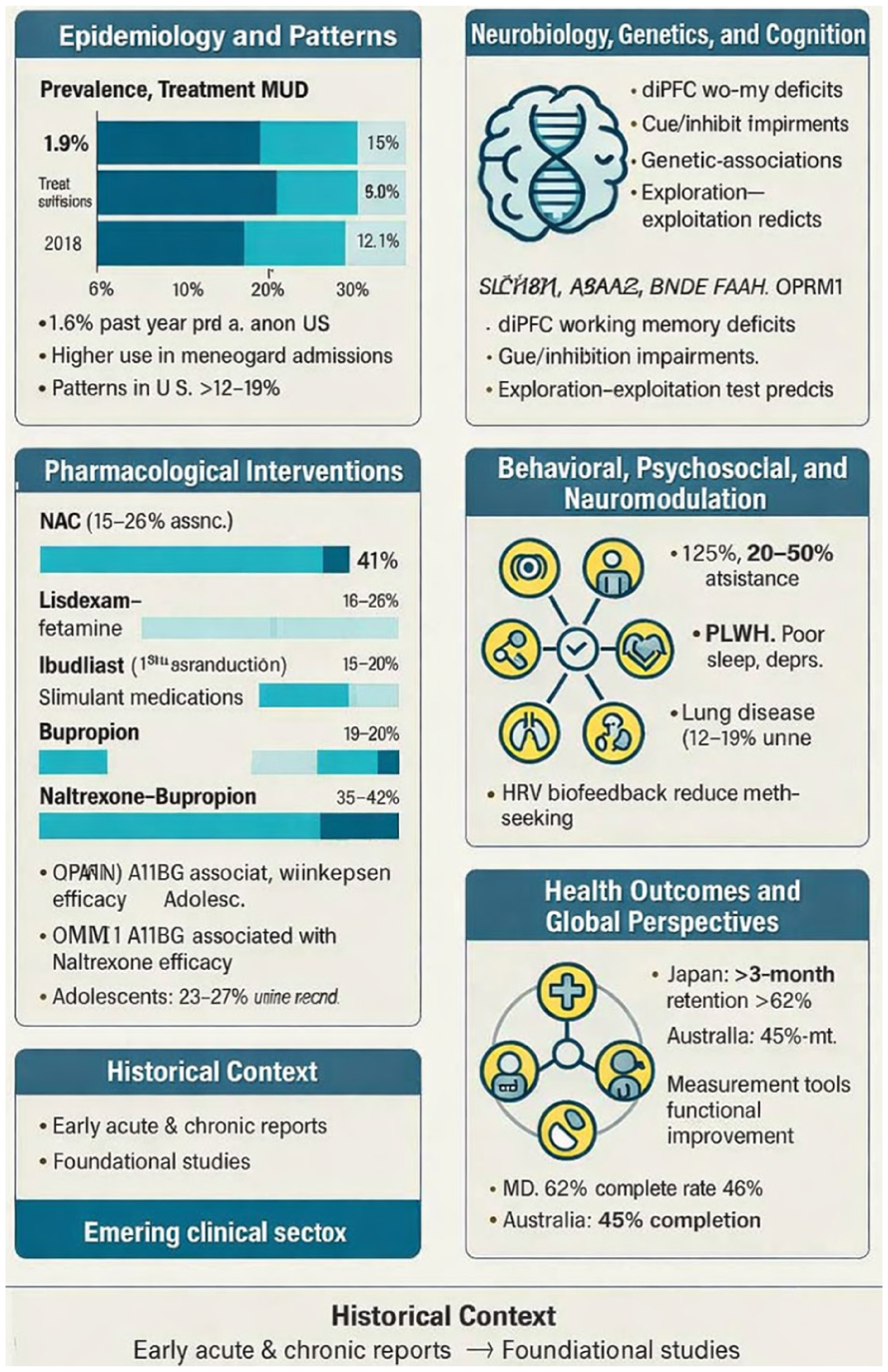
Epidemiology and Patterns of Methamphetamine Use
Methamphetamine use has shown persistent and resurgent patterns worldwide. In the United States, the prevalence of past-year use among adults was reported at 1.8%, with notable increases in treatment admissions between 2008 and 2017 (from 8.6% to 17.1%) 5 (Figure 2). National surveys indicate that past-year methamphetamine use among adults increased from 1.5 million in 2015 to 1.9 million in 2018. 2 Surveillance studies identified demographic patterns, with higher use among males, younger adults, and individuals with comorbid opioid use disorder; in one cohort, 38% of opioid users reported methamphetamine use 3 (Figure 3). Methamphetamine administration methods influenced harms: injection was associated with higher rates of psychiatric comorbidities and infectious complications compared to smoking. 4 Overall, methamphetamine use is associated with acute and chronic health risks, including cardiovascular, neurological, and psychiatric complications.1,20 Globally, patterns of use were observed in Vietnam among methadone maintenance patients, where younger age and male sex predicted greater methamphetamine severity,42,46 and in Australia, mandatory treatment programs showed moderate completion rates (45%). 40
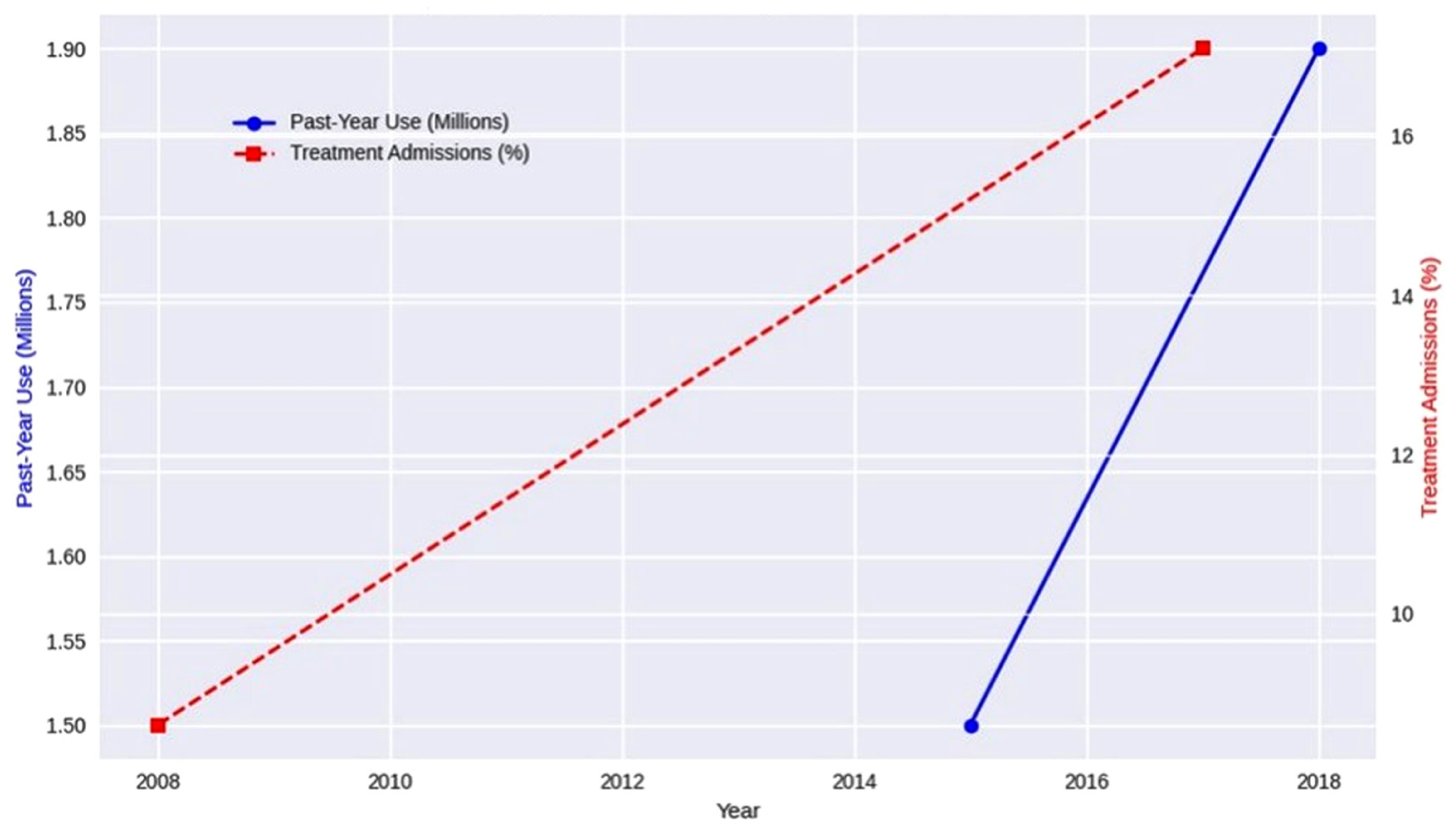
Epidemiology trends of methamphetamine use in US adults.
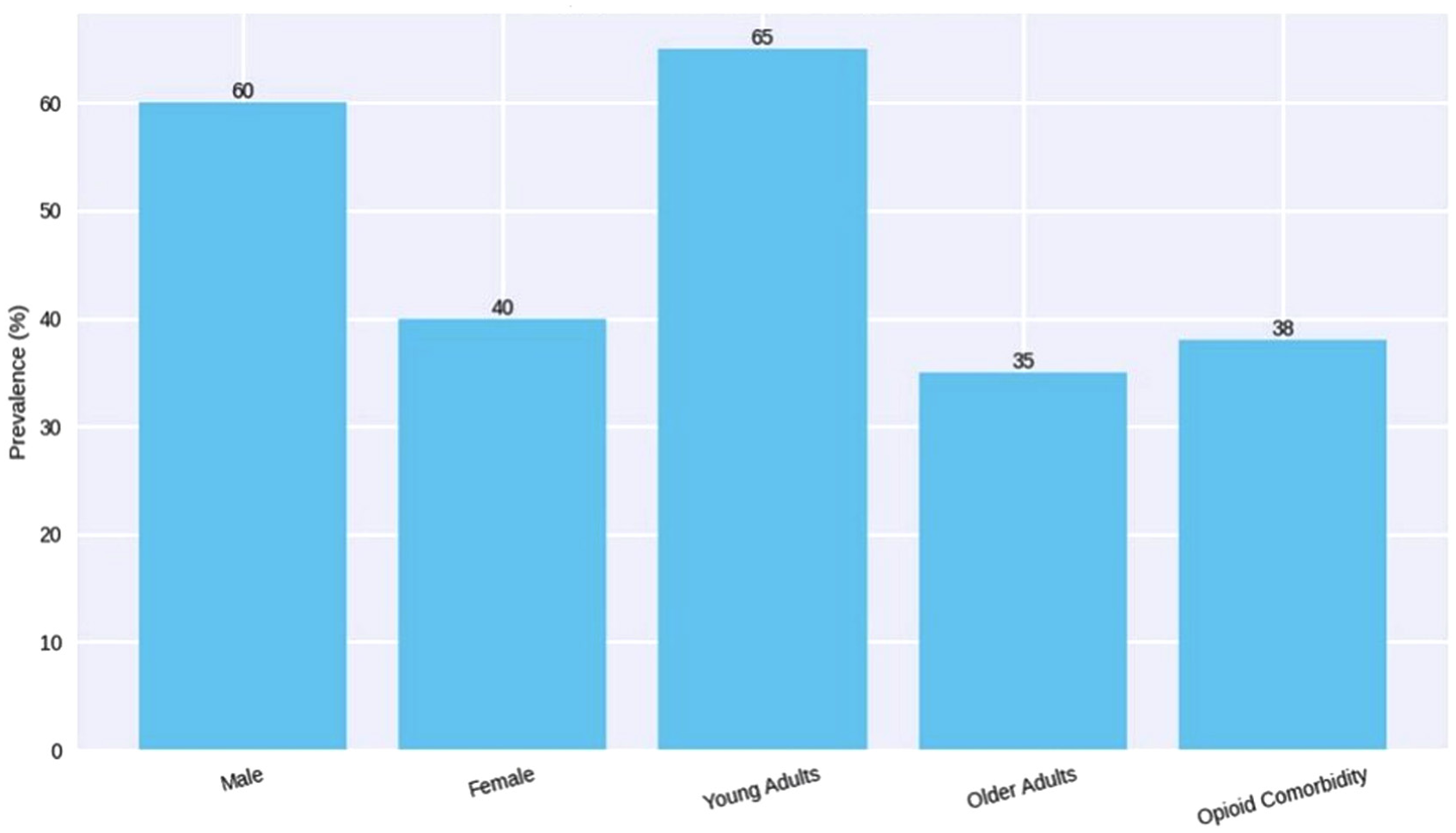
Demographic patterns of methamphetamine use.
Mortality, morbidity, and social harms are significant. Methamphetamine-related health care utilization is increasing, with a notable rise in emergency and outpatient visits in regions without dedicated diagnostic codes for MUD. 52 Pulmonary and cardiovascular complications were identified in 12% to 18% of long-term users 63 (Table 3; Figure 6).
Synthesis of Intervention Efficacy and Key Findings.
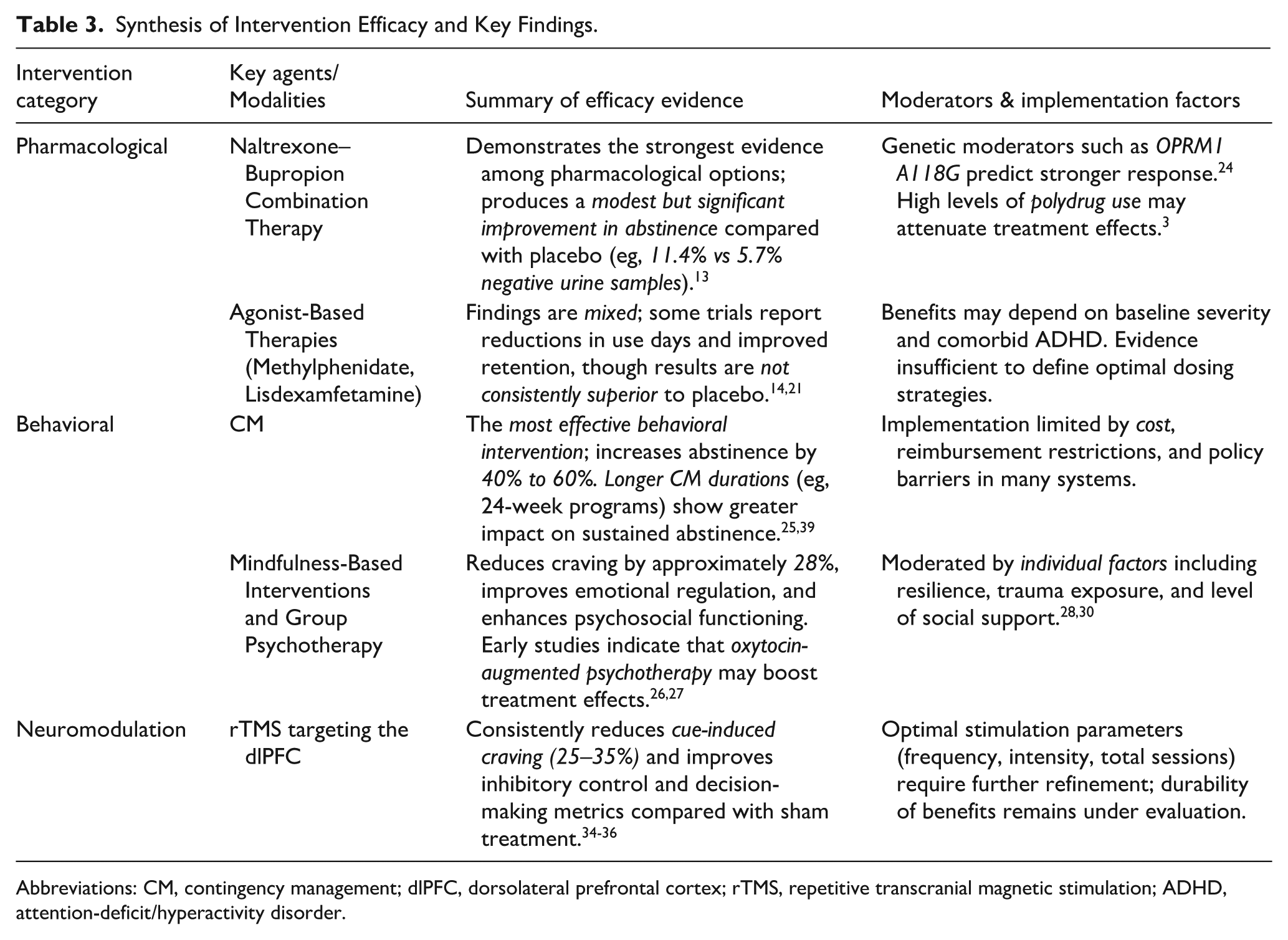
Abbreviations: CM, contingency management; dlPFC, dorsolateral prefrontal cortex; rTMS, repetitive transcranial magnetic stimulation; ADHD, attention-deficit/hyperactivity disorder.
Neurobiology, Genetics, and Cognitive Correlates
MUD is associated with neural and cognitive alterations. Functional connectivity deficits in the dorsolateral prefrontal cortex (dlPFC) were observed during working memory tasks, 7 while temporally dynamic neural responses to drug cues and inhibitory control tasks were identified in fMRI studies. 8 Sex differences in neural activity may influence treatment outcomes.9,10 Genetic studies revealed associations with SLC18A1, SLC18A2, BDNF, FAAH, and OPRM1 variants, suggesting neurobiological underpinnings for susceptibility and treatment response.11,12,24 Computational models demonstrated that exploration–exploitation behaviors predict treatment efficacy and onset response in MUD 6 (Table 3; Figure 6).
The Pharmacological Frontier: From Monotherapy to Combination and Personalization
Pharmacological research has evolved from testing single agents to evaluating combination therapies and personalized approaches. The combination of naltrexone and bupropion has emerged as a leading candidate, demonstrating statistically significant, though clinically modest, benefits in large RCTs. 13 In contrast, monotherapies with bupropion or topiramate have generally shown limited efficacy.16,53 A promising direction is pharmacogenetics, with evidence that the OPRM1 A118G polymorphism can identify individuals most likely to respond to naltrexone. 24 The naltrexone–bupropion combination achieved 35% to 42% abstinence at 12 weeks,13,57 whereas bupropion monotherapy showed 18% to 29% abstinence depending on use frequency.53,55 Sustained-release methylphenidate improved retention (74% vs 51%) and reduced methamphetamine use days.14,56,64 Dexamphetamine maintenance reduced use by 56% over 8 weeks, 15 while topiramate modestly decreased craving (22%) without significant abstinence benefits. 16 Neuroinflammation-targeted therapies, including ibudilast, lowered peripheral inflammatory markers by 18% to 25%.17,18 Exploratory trials of ifenprodil reduced cue-induced craving by 30%, 19 and lisdexamfetamine decreased use days by 41%. 21 Nicotinic agonists reduced methamphetamine-seeking behavior in preclinical models. 22
Pharmacogenetics influenced outcomes: carriers of the OPRM1 A118G polymorphism had a 38% higher likelihood of abstinence with injectable naltrexone. 24 Intervention adherence and fidelity influenced outcomes, particularly for behavioral and pharmacological interventions. Adolescent populations treated with bupropion achieved moderate reductions in methamphetamine-positive urine samples (23%-27%) 54 (Table 3; Figures 4 and 6).
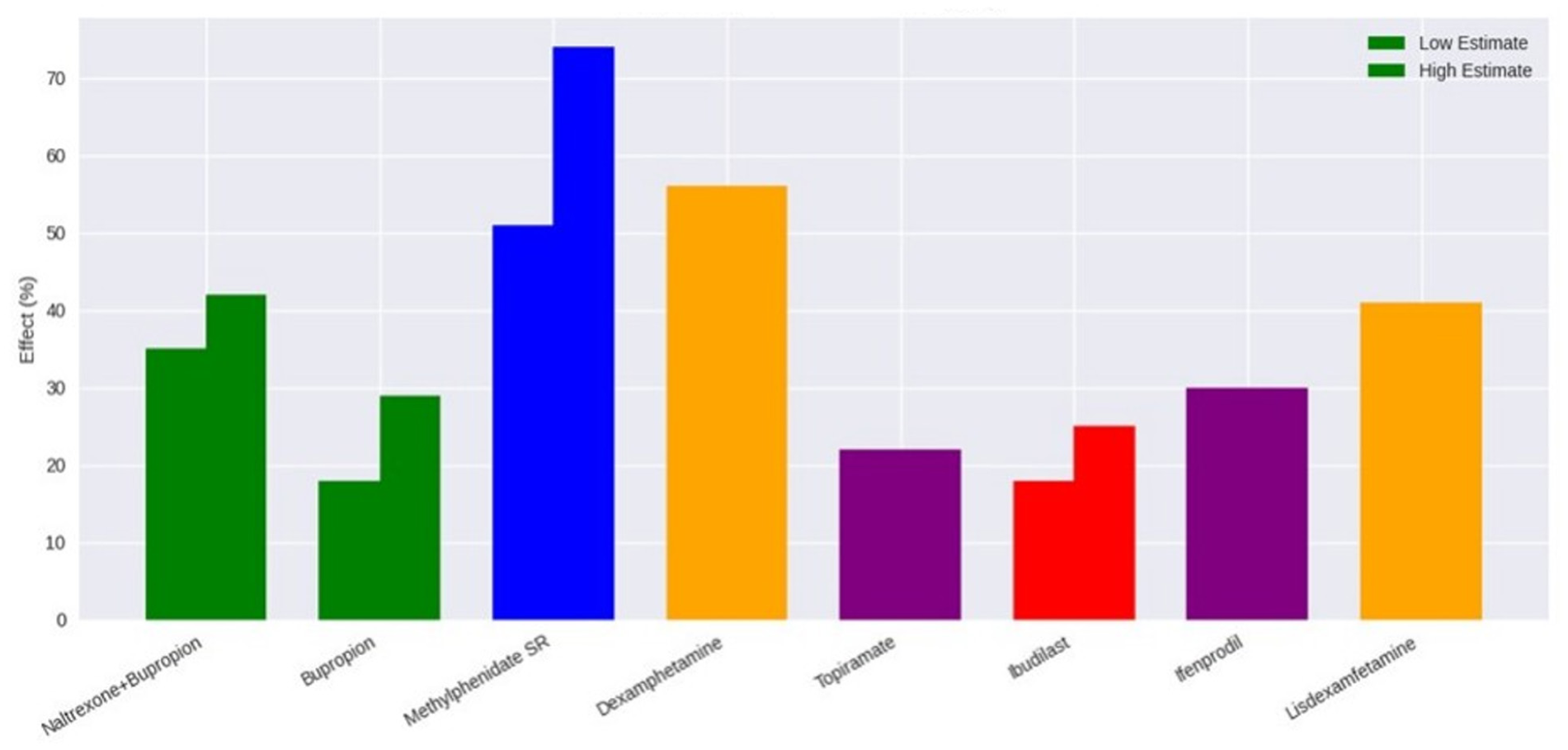
Pharmacological interventions for MUD.
The Foundational Role of Behavioral Interventions
Behavioral strategies, particularly CM, constitute the most evidence-based component of MUD treatment. The efficacy of CM is well established, with its effect size being among the highest in substance use disorder treatment. 25 However, a critical finding from this review is the stark contrast between this robust efficacy and its limited implementation in real-world settings, often due to funding and regulatory challenges. 39 Other modalities like mindfulness and group therapy provide valuable tools for managing craving and addressing psychosocial determinants of use.26,27 CM increased abstinence rates by 40% to 60% over 12 to 16 weeks.25,39 Feasibility challenges remain, with implementation barriers including resource intensity and training requirements. Mindfulness-based therapies reduced cravings by 28%, 26 while oxytocin-enhanced group therapy decreased positive urine screens by 33%. 27 Individual factors, including childhood trauma, aggression, and resilience, moderated relapse risk and treatment outcomes.28-31
Patient-centered approaches were increasingly studied. Surveys showed high interest in potential pharmacotherapies, particularly for side effect profiles and perceived effectiveness. 32 Digital tools, such as virtual psychotherapist applications, demonstrated feasibility and reduced use by 45% over 6 weeks. 33 Smartphone-based medication adherence monitoring achieved 87% adherence rates in open-label naltrexone–bupropion studies65,66 (Table 3; Figures 5 and 6).
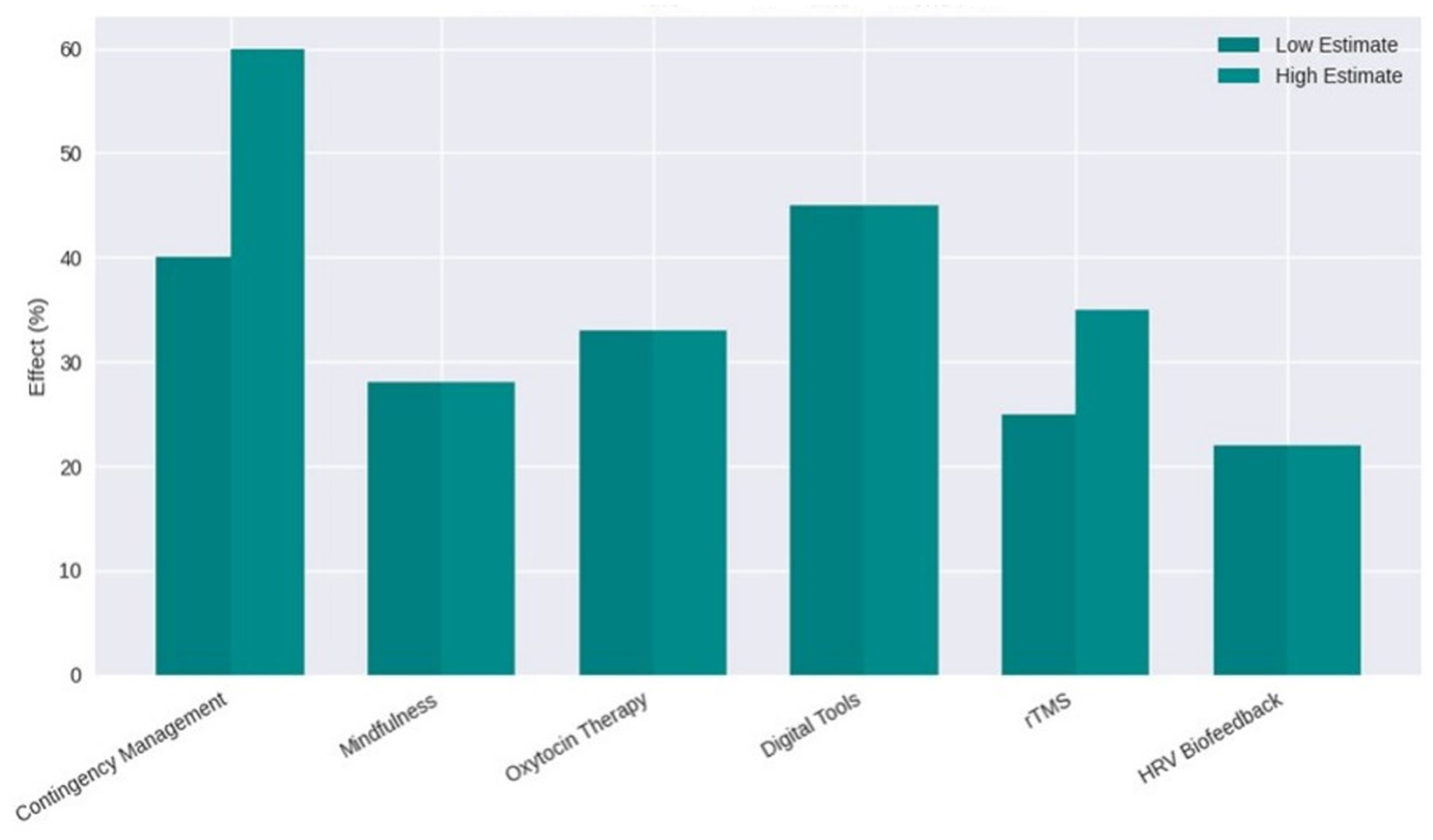
Behavioral and neuromodulation interventions for MUD.
Summary of the main themes.
Emerging Neuromodulation and Digital Tools
Neuromodulation represents a paradigm shift, directly targeting the neurocognitive deficits in MUD. Multiple RCTs confirm that high-frequency rTMS to the left dlPFC produces significant and replicable reductions in craving.34,35 Parallel to this, digital health interventions, such as virtual psychotherapist apps and smartphone-based adherence monitoring, demonstrate feasibility and potential for improving engagement and scalability.33,65 Neuromodulation via rTMS targeting the left dlPFC decreased cravings by 25% to 35% and improved decision-making.34-36 Additional studies, including non-RCTs, support rTMS efficacy and suggest transcranial direct current stimulation (tDCS) may also reduce cravings. Nicotine agonists were removed from this section, as they are not true neuromodulators. Heart rate variability biofeedback yielded moderate craving reductions of 22% in men with MUD 37 (Table 3; Figure 5).
Health Outcomes, Comorbidities, and Psychopathology
Methamphetamine use was linked to psychiatric and physical comorbidities. Psychosis occurred in 21% to 30% of psychiatric inpatients. 38 Among adults living with HIV, lifetime MUD was associated with poorer sleep quality and increased depressive symptoms. 43 Pulmonary hypertension and chronic lung disease were prevalent in 12% to 18% of long-term users. 63 Polydrug use worsened treatment outcomes in heroin, cocaine, and methamphetamine users.50,51,67
Sexual orientation and gender differences affected treatment response, with nonheterosexual men showing 20% lower adherence to naltrexone–bupropion therapy. 47 Measurement tools, including the Treatment Effectiveness Assessment, reliably captured functional improvement in MUD patients 45 (Table 3; Figure 6).
Treatment Implementation and Global Perspectives
Retention and adherence varied by region. In Japan, 62% of MUD patients remained in treatment beyond 3 months. 41 Open-label pharmacotherapy trials showed feasibility of smartphone-assisted adherence monitoring. 58 Trials of mandatory treatment programs in Australia showed 45% completion. 40 Longitudinal analyses indicated that polydrug trajectories influenced long-term outcomes. 67
Emerging treatments, including N-acetylcysteine, demonstrated modest efficacy in reducing methamphetamine use and craving scores by 15% to 20% in small crossover studies. 23 Current reviews highlight the evolving landscape of MUD treatment, emphasizing the need for integrated pharmacological, behavioral, and neuromodulatory approaches44,48,49 (Table 3).
Historical and Clinical Context
MUD has long been recognized as a public health issue, with early reports documenting acute and chronic complications. 20 Sustained-release dextroamphetamine has been trialed for long-term maintenance, demonstrating reductions in methamphetamine use and improvements in retention among treatment-seeking individuals. 64 These foundational studies provide context for contemporary pharmacological and psychosocial interventions (Figure 6).
Discussion
Our scoping review maps a dynamic and rapidly advancing field. Three key findings emerge: First, the intervention arsenal for MUD is bifurcated, with a highly efficacious but under-implemented behavioral therapy (CM) existing alongside pharmacological and neuromodulation approaches that show significant promise but have not yet achieved large effect sizes. Second, the era of “one-size-fits-all” pharmacotherapy is giving way to combination and personalized approaches, informed by genetics and neurobiology. Third, neuromodulation has firmly established itself as a legitimate therapeutic modality, with rTMS demonstrating consistent effects on a core symptom of substance use disorder—cue-induced craving.
The findings underscore a clear hierarchy of evidence, highlight promising new therapeutic paradigms, and, most importantly, point to the necessity of integrated, personalized treatment strategies to address the complex neurobiology and psychosocial determinants of this disorder.
The most unequivocal finding of this review is the established, superior efficacy of behavioral interventions, particularly CM. The evidence solidifies CM not just as an effective tool, but as a foundational component of MUD treatment. The dose-response relationship observed between intervention duration and outcomes suggests that sustained reinforcement is crucial for neurobehavioral change, likely counteracting the chronic dysregulation of reward pathways.25,39 This positions CM as a necessary scaffold upon which other interventions can be built. Furthermore, the emergence of mindfulness-based therapies and oxytocin-enhanced group therapy reflects a maturation of the behavioral paradigm, although implementation feasibility and fidelity are crucial for effectiveness, moving beyond simple reinforcement to address the core affective and social deficits—such as emotional dysregulation and impaired social connection—that are central to the pathology of substance use disorder and often trigger relapse.26,27
In the pharmacological domain, the narrative has shifted from the disappointment of monotherapies to the promise of combination and targeted approaches. Wellbutrin-naltrexone studies, including other stimulant trials, demonstrate promising augmentation of abstinence outcomes. The success of the naltrexone-bupropion combination 13 validates a multi-target strategy, simultaneously modulating opioid-mediated reward and monoamine reuptake to address the multifaceted pharmacodynamics of methamphetamine. This represents a significant leap forward. Concurrently, the exploration of agonist therapies (eg, lisdexamfetamine, sustained-release dexamphetamine)15,21 and novel agents like ibudilast17,18 signals a diversification of mechanism. The former aims to stabilize brain function through cross-tolerance, while the latter represents a paradigm shift toward targeting the neuroinflammatory and glutamatergic consequences of chronic use. This progression from nonspecific to highly targeted pharmacotherapy marks a new era in medication development for MUD.
Perhaps the most paradigmatic shift identified is the advent of neuromodulation, specifically rTMS. By directly targeting the dlPFC, rTMS moves beyond symptomatic treatment to address a core pathophysiological mechanism: the deficit in top-down cognitive control.34-36 The evidence suggests that rTMS does not merely reduce craving but may actually repair the underlying neural circuitry responsible for inhibitory control and decision-making. This positions neuromodulation as a potential “circuit breaker” that could enhance a patient’s capacity to benefit from concurrent behavioral and pharmacological treatments.
A critical synthesis of these findings leads to a central, overarching conclusion: the future of MUD treatment lies in personalization and integration. The compelling influence of genetic variants (eg, OPRM1), sex differences, and psychosocial factors (eg, trauma, loneliness, polydrug use)9,24,28,30 unequivocally demonstrates that a one-size-fits-all approach is untenable. The variable treatment response across studies is not merely noise but a signal of this profound heterogeneity. The future path must involve tailoring interventions based on an individual’s genetic profile, neurocognitive phenotype, comorbid conditions, and social environment. The integration of computational modeling to quantify decision-making deficits offers a promising, objective method to guide this personalization. 6
Therefore, the most effective treatment model for MUD is likely to be a sequenced, integrated platform. In this model, neuromodulation could be used initially to strengthen prefrontal control and reduce craving, thereby enhancing engagement. This would be seamlessly combined with combination pharmacotherapy to stabilize neurochemistry and mitigate reward dysregulation, all while the patient actively participates in evidence-based behavioral therapies like CM and mindfulness to build sustainable coping skills and reinforce abstinence. Digital health tools can then provide a continuous layer of support and monitoring, extending the reach of the clinic into the patient’s daily life. 33
Implications for Research and Clinical Practice
The findings argue compellingly for an integrated, multimodal treatment framework. Rather than viewing these interventions as competing, a synergistic model is needed. For instance, rTMS could be used to reduce craving and improve cognitive control, thereby enhancing a patient’s capacity to engage with and benefit from CM or mindfulness-based relapse prevention. Similarly, pharmacotherapy like naltrexone-bupropion could provide a physiological buffer against relapse, creating a window of opportunity for behavioral interventions to take hold.
Future research must address critical gaps. Implementation science is urgently needed to develop sustainable models for delivering CM. Optimization trials are required for rTMS to determine ideal protocols and long-term durability. Hybrid efficacy-implementation studies should test combined intervention packages. Furthermore, the field must move beyond abstinence as the sole outcome and include measures of functional recovery, quality of life, and neurocognitive performance.
Considerations and Limitations
The findings of this scoping review should be understood within the methodological decisions that shaped its design. Several limitations warrant consideration. First, restricting the search to English-language publications, while necessary for feasibility, may have excluded relevant studies published in other languages, although this was methodologically justified to ensure accurate extraction and interpretation of complex intervention details. Second, although major bibliographic databases were used, their inherent limitations—such as inconsistent indexing practices, delays in updates, and incomplete coverage of older or specialized journals—may have resulted in missing pertinent studies. The reliance on Web of Science, despite its broad reach, may have reduced sensitivity for highly specific intervention details found only in abstracts or niche journals.
Third, the review did not include gray literature such as dissertations, conference proceedings, and unpublished research. While this decision maintained a focus on peer-reviewed evidence, it carries the risk of publication bias, favoring studies with significant or positive results. Fourth, although a systematic automated and manual de-duplication process was undertaken, some nonexact duplicates may have been inadvertently retained.
Finally, as consistent with scoping review methodology, this study sought to map the extent and characteristics of available evidence rather than assess study quality or effectiveness. Consequently, conclusions about intervention impact are limited. Despite these constraints, the review provides a comprehensive overview and identifies important gaps in the literature.
Conclusion
MUD is a complex and growing public health problem marked by high morbidity and limited treatment consistency across settings. Evidence from this scoping review shows that no single modality is sufficient; rather, effective care requires integrating pharmacological, behavioral, and neuromodulation approaches. Combination pharmacotherapies and sustained-release formulations offer modest but improving benefits, while contingency management, mindfulness-based strategies, and digital tools enhance engagement and support long-term recovery. Neuromodulation and emerging biologically targeted interventions show potential for improving cognitive control and reducing cravings. Comorbid psychiatric conditions and polydrug use significantly shape treatment outcomes, underscoring the need for holistic, patient-centered care. Overall, advancing MUD treatment will depend on combining the strengths of these modalities within personalized, mechanism-informed frameworks. Intervention feasibility, fidelity, and holistic patient care are key determinants of real-world effectiveness. Future research should prioritize longitudinal evaluations, comparative effectiveness studies, and scalable implementation strategies to ensure that evolving advances translate into meaningful, real-world improvements for individuals affected by MUD.
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all those who contributed to the completion of this scoping review. We also appreciate the support and guidance provided by our colleagues and the academic community, whose insights and feedback greatly enhanced the quality of this work.
Author Contributions
This scoping review was conducted with the collaborative efforts of the research team. The first author was responsible for designing the study, conducting the literature search, data extraction, and initial drafting of the manuscript. Co-authors revised the manuscript, amended the draft, and provided critical feedback throughout the process. They contributed to the interpretation of findings, and helped refine the final manuscript. All authors were involved in the development of the review’s objectives, the analysis of data, and the writing of the manuscript. All authors have read and approved the final version of the manuscript, ensuring the accuracy and integrity of the work presented.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author*.