
Abstract
Background:
Depression and anxiety are highly prevalent among individuals with opioid use disorder (OUD), and antidepressants are frequently prescribed in conjunction with medication for opioid use disorder. However, the relationship between specific antidepressants and continued illicit opioid use during buprenorphine-based treatment remains insufficiently characterized. This exploratory analysis aimed to investigate the association between prescribed antidepressants and illicit opioid use among adults with OUD receiving buprenorphine/naloxone.
Methods:
This sub-analysis included 92 participants from a randomized controlled trial of 141 adults with OUD treated with buprenorphine/naloxone over 16 weeks in an outpatient setting. Participants were eligible if they received at least one antidepressant for a minimum duration of 10 days. Depressive and anxiety symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9) and the Generalized Anxiety Disorder-7 (GAD-7), respectively. The primary outcome was the proportion of urine drug screens positive for illicit opioids. Point-biserial correlation analyses were conducted to examine associations between individual antidepressants and illicit opioid use. Antidepressants demonstrating significant associations were subsequently included in multivariable linear regression models adjusted for age, treatment allocation group, and buprenorphine elimination rate constant. Interaction effects were also examined.
Results:
The mean (SD) PHQ-9 score was 10.0 (5.4), and the median (IQR) GAD-7 score was 5.5 (2.0-13.75). Escitalopram 10 mg was the only antidepressant significantly associated with illicit opioid use, demonstrating a negative correlation (rpb = −.28). Multivariable regression analyses indicated that escitalopram exposure and older age were independently associated with a lower proportion of opioid-positive urine tests. A statistically significant interaction between escitalopram exposure and age was observed.
Conclusions:
Exposure to escitalopram 10 mg was associated with reduced illicit opioid use among individuals receiving buprenorphine/naloxone, with the magnitude of this association modified by age. Further large-scale prospective studies are warranted to confirm these findings and to elucidate the underlying mechanisms.
Keywords
Highlights
Escitalopram 10mg is the only antidepressant found as a potential predictor of lower illicit opioid use among adults with opioid use disorder (OUD), and mood disorders (depression and anxiety) receiving buprenorphine/naloxone. Age and escitalopram demonstrated significant interaction on rate of illicit opioid use.
The rate of prescribing antidepressants was higher than reported in previous studies.
Findings suggest the need for larger prospective studies to develop integrated treatment protocols for adults with co-occurring OUD, and mood disorders (depression and anxiety) receiving MOUDs.
Introduction
Many adults (75%) with opioid use disorder (OUD) presenting to specialized substance use disorder (SUD) treatment facilities have at least one co-occurring psychiatric disorder. 1 The most reported are major depressive disorder (MDD) and anxiety disorders, particularly post-traumatic stress disorder (PTSD).1-4 These psychiatric comorbidities pose significant challenges to the diagnosis, treatment, and recovery of individuals with OUD and are associated with worse clinical outcomes, underscoring the need for patient-centered integrated treatment.5-7
A growing body of literature demonstrates a strong relationship between opioid use, anxiety, and depression.4,8,9 This relationship is described as bidirectional in a systematic review by Rogers et al. 8 In contrast, a systematic review and a meta-analysis of longitudinal prescription opioid use showed an increased risk of developing anxiety (adjusted effect size 1.40 [95% CI 1.2-1.8]) but not depression (adjusted effect size 1.18 [95% CI 0.98-1.41]). 10
Conversely, the impact of depression on illicit opioid use in adults receiving buprenorphine-based treatment is equivocal. A literature review by Ghabrash et al 10 found that while some studies suggest that depression may hinder long-term remission, other studies suggest that depressive symptoms may predict reductions in illicit opioid use during treatment. Elarabi et al 11 reported no significant association between baseline depression and anxiety, and illicit opioid use among individuals receiving buprenorphine/naloxone over 16 weeks of outpatient treatment.
Antidepressants are the most prescribed class of psychotropics in adults with OUD receiving medications for opioid use disorder (MOUD) at a rate of 35.4%. 12 Despite this, limited data exist on the impact of antidepressants on the rate of illicit opioid use among patients receiving MOUD. In contrast, the effect of antidepressants on enhancing retention while receiving buprenorphine treatment was not consistent across studies.13-15 While a population-based cohort study by Zhang et al 15 reported that the initiation of antidepressant therapy during buprenorphine treatment was associated with improved treatment retention, other studies suggest that initiating antidepressants prior to buprenorphine was associated with lower retention outcomes. 11
This paper reports on a sub-analysis of the Suboxone Treatment and Recovery Trial (STAR-T), a randomised controlled trial of 141 adults with OUD receiving buprenorphine/naloxone film (BUP/NX-F) that evaluated the effect of Incentivised Adherence and Abstinence Monitoring (IAAM; experimental) on illicit opioid use and treatment retention.16,17 Results from STAR-T demonstrated that IAAM significantly reduced illicit opioid use compared with treatment-as-usual (control). Further analyses identified older age and lower buprenorphine elimination rate constant (BUP EL.R) to be significantly associated with lower rates of illicit opioid use. Other clinical variables, for example, opioid type and pattern of illicit opioid use, polysubstance use, duration of opioid use, addiction severity, sleep disorders, impulsiveness, and personality traits, were not significantly associated with illicit opioid use in this cohort.16,18
This study aimed to explore the correlation between prescribed antidepressants and illicit opioid use in adults receiving buprenorphine/naloxone. The null hypothesis for this analysis is that exposure to antidepressants has no correlation with illicit opioid use.
Methods
Study Design
This study is a sub-analysis of the Suboxone Treatment and Recovery Trial (STAR-T), a 16-week pragmatic, two-arm, parallel randomized controlled trial involving 141 adults with OUD receiving BUP/NX-F.
Adults diagnosed with OUD were admitted to a 4-week inpatient program at a specialized SUD treatment service and evaluated for enrolment in the trial. 17 At intake, participants were evaluated for multiple psychopathologies, including mood disorders, impulsiveness, personality disorders, quality of sleep, and addiction severity. 17
Patients were eligible if they were ≥18 years old, voluntarily seeking treatment, and residents of the UAE with stable accommodation. Patients were excluded if they: (i) reported daily benzodiazepine use exceeding 20 mg diazepam equivalent in the past 30 days; (ii) were pregnant or planning to become pregnant; (iii) had known naloxone or buprenorphine hypersensitivity; (iv) presented with signs of hepatic impairment, defined as elevation of liver function tests to 3 times the upper limit of normal; (v) reported a suicide attempt in the past 12 months; (vi) reported involvement with the criminal justice system likely to result in arrest and incarceration; (vii) presented with uncontrolled severe mental or physical illness judged to compromise safety; or (viii) demonstrated cognitive impairment marked by a score of <17 on the Mini-Mental State Examination.
Induction and stabilization on BUP/NX-F were completed during the 4-week inpatient care. At the end of the inpatient program, 141 participants were randomized on a 1:1 basis to receive 16 weeks of outpatient treatment: (i) Incentivised Adherence and Abstinence Monitoring, delivered as medication management integrated with Therapeutic Drug Monitoring (TDM) (n = 70; experimental group), or (ii) treatment-as-usual (n = 71; control group). Participants in the experimental group received up to 4 weeks of stepped unsupervised BUP/NX-F doses contingent on adherence determined by TDM and abstinence according to urine drug tests. In contrast, participants in the control group received up to 2 weeks of unsupervised BUP/NX-F doses contingent on abstinence from illicit opioid use assessed by urine drug tests.
The primary outcome for STAR-T was illicit opioid use, measured as the proportion of urine tests positive for illicit opioids relative to the total number of tests performed. The secondary outcome was retention in treatment, measured by completion of the 16-week study period without interruption, with interruption defined as missing 3 consecutive appointments at the outpatient clinic. The present sub-analysis investigates the correlation between prescribed antidepressants and the primary outcome. Data for this sub-analysis were retrieved from the electronic health records of the STAR-T participants.
Participants were included in the analysis if they received at least one antidepressant. Alternatively, participants were excluded if they: (i) were receiving antidepressants at the time of admission; (ii) were prescribed antidepressants during the study for a period of less than 10 days; or (iii) failed to refill the antidepressant prescriptions during the 16-week follow-up period.
Tools
Patient Health Questionnaire
The Patient Health Questionnaire (PHQ-9) 19 is a validated self-administered nine-item instrument used to assess the severity of depressive symptoms over the preceding 2 weeks. Each item is rated on a 4-point Likert scale ranging from 0 (“not at all”) to 3 (“nearly every day”), yielding a total score between 0 and 27, with higher scores indicating greater depression severity. A cutoff score of ≥10 is commonly used to indicate moderate depression warranting pharmacological treatment, with reported sensitivity and specificity of 88%. 19 The PHQ-9 has demonstrated high internal consistency (Cronbach’s α = .89). 19 In this cohort, the Tunisian Arabic version was used, demonstrating good reliability (Cronbach’s α = .857) and sensitivity and specificity of 86.2% and 83.8%, respectively. 20
Generalised Anxiety Disorder 7-item Scale
The Generalised Anxiety Disorder 7-item Scale (GAD-7) 21 is a validated self-administered seven-item instrument assessing anxiety symptoms over the preceding 2 weeks. Items are scored from 0 to 3, yielding a total score ranging from 0 to 21. Standard cutoffs of 5, 10, and 15 represent mild, moderate, and severe anxiety, respectively. At a cutoff score of 10, sensitivity and specificity are reported as 89% and 82%, respectively. 21 The scale demonstrates strong internal consistency (Cronbach’s α = .89). 21 The Tunisian Arabic version used in this cohort demonstrated acceptable reliability (Cronbach’s α = .76). 22
Outcome Measures and Procedures
The primary outcome was defined as the proportion (%) of confirmed positive urine tests for illicit opioids from the total number of urine tests conducted per participant over the 16-week study period. This measure provides a longitudinal and quantitative assessment of illicit opioid use, capturing both frequency and persistence of use during treatment.
Procedures
At each follow-up visit, participants underwent urine drug screening (UDS) for illicit opioid use using Clinical Laboratory Improvement Amendments (CLIA)-approved point-of-care tests. To ensure high diagnostic accuracy and minimize false-positive results, all samples that tested positive on initial screening were subjected to confirmatory analysis using Gas Chromatography–Tandem Mass Spectrometry (GC–MS/MS), the gold standard for confirmatory tests. Only samples that were confirmed positive by GC–MS/MS were reported positive for illicit opioid use. This two-step testing approach (immunoassay screening followed by GC–MS/MS confirmation) reduces the risk of misclassification bias and reinforces the validity of the outcome measurement. Adherence to antidepressant treatment was monitored by pharmacy prescription refills.
The PHQ-9 and GAD-7 were administered at intake, and at 4, 8, 12, and 16 weeks thereafter. Adherence to antidepressants was confirmed by pharmacy dispensing records.
Statistical Analysis
Descriptive statistics were performed for baseline participant characteristics and prescribed antidepressants. A bivariate analysis using point-biserial correlation was conducted to examine the correlation between exposure to each antidepressant and the proportion of urine positive tests for illicit opioid use.
Antidepressants demonstrating statistically significant correlations were added to a multivariate linear regression model including age, study group allocation, and buprenorphine elimination rate constant. These variables were reported to demonstrate significant correlation with illicit opioid use in this cohort. The regression model was further updated for the interaction of variables showing significant association with the primary outcome. The regression model results were reported as follows: unstandardized beta coefficient, standard error, standardized beta coefficient, P-value, and 95% confidence interval.
All statistical tests were two-tailed, with a significance threshold of P < .05, performed using IBM SPSS Statistics, Version 25.0 (IBM Corp, Armonk, NY, USA).
Ethical Statement
The STAR-T 18 was conducted in accordance with the International Conference on Harmonisation Good Clinical Practice guidelines and the Declaration of Helsinki. Ethics approval was obtained from an Institutional Review Board (details blinded for peer review). The trial was registered with ISRCTN (ISRCTN41645723). All participants provided written informed consent, and data were managed in accordance with established governance protocols.
Results
Participants’ Characteristics
Ninety-two (n = 92, 65.2%) of the 141 participants in the primary study were included in this analysis. Table 1 presents the characteristics of the sample. The mean (SD) PHQ-9 score was 10.0 (5.4), suggesting moderate depression, and the median (IQR) GAD-7 score was 5.5 (2.0-13.75), suggesting mild anxiety. Mirtazapine 30 mg was the most prescribed antidepressant (n = 54, 58.7%), followed by clomipramine 50 mg (n = 30, 32.6%), and escitalopram 10 mg (n = 26, 28.2%).
Baseline Characteristics of Participants Included in the Sub-Analysis (N = 92).
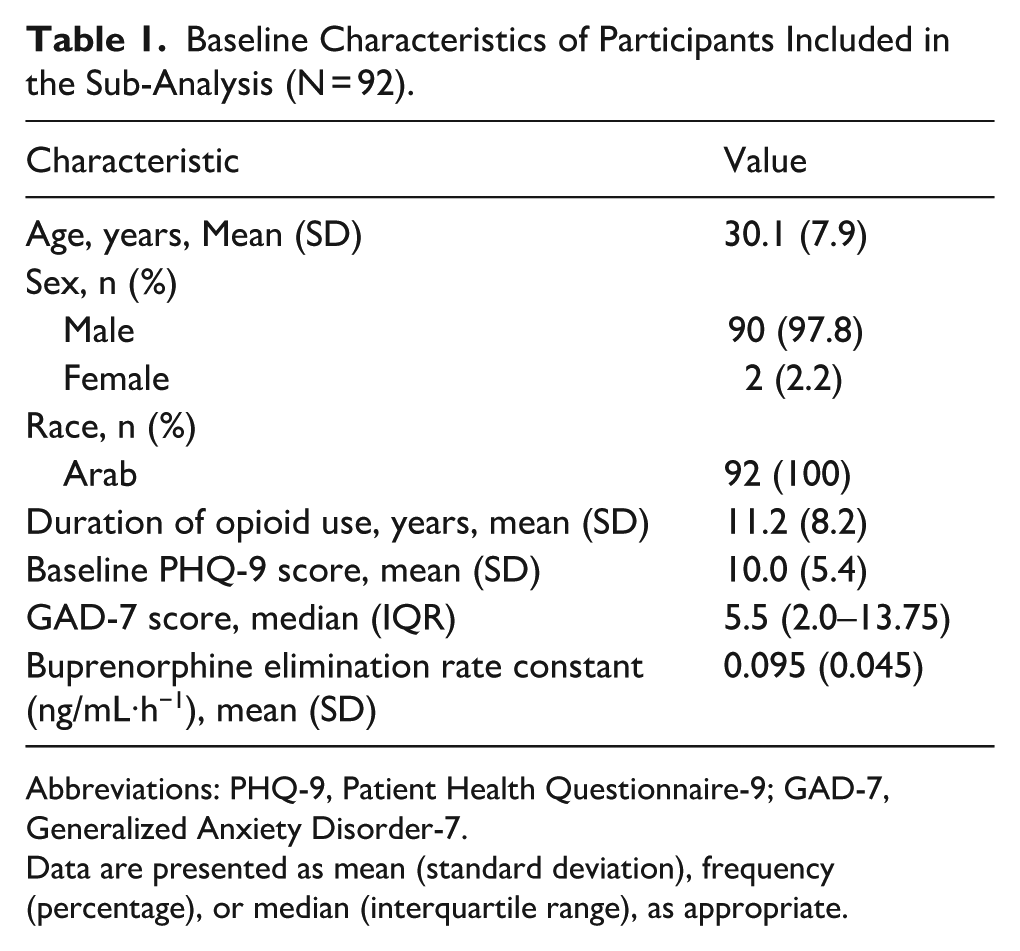
Abbreviations: PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalized Anxiety Disorder-7.
Data are presented as mean (standard deviation), frequency (percentage), or median (interquartile range), as appropriate.
Association Between Prescribed Antidepressants and Illicit Opioid Use
Table 2 summarizes the point-biserial correlation scores and the corresponding significance to examine the correlation between prescribed antidepressants and the primary outcome. Escitalopram 10 mg was the only antidepressant that showed significant correlation with the proportion of urine tests positive for illicit opioid use. The nature of the correlation was negative (rpb = −.28, P = .02), suggesting that participants who received escitalopram 10 mg were less likely to use illicit opioids during the study period compared with those who did not.
Correlation Between Antidepressant Exposure and Proportion of Urine Tests Positive for Illicit Opioids (N = 92).
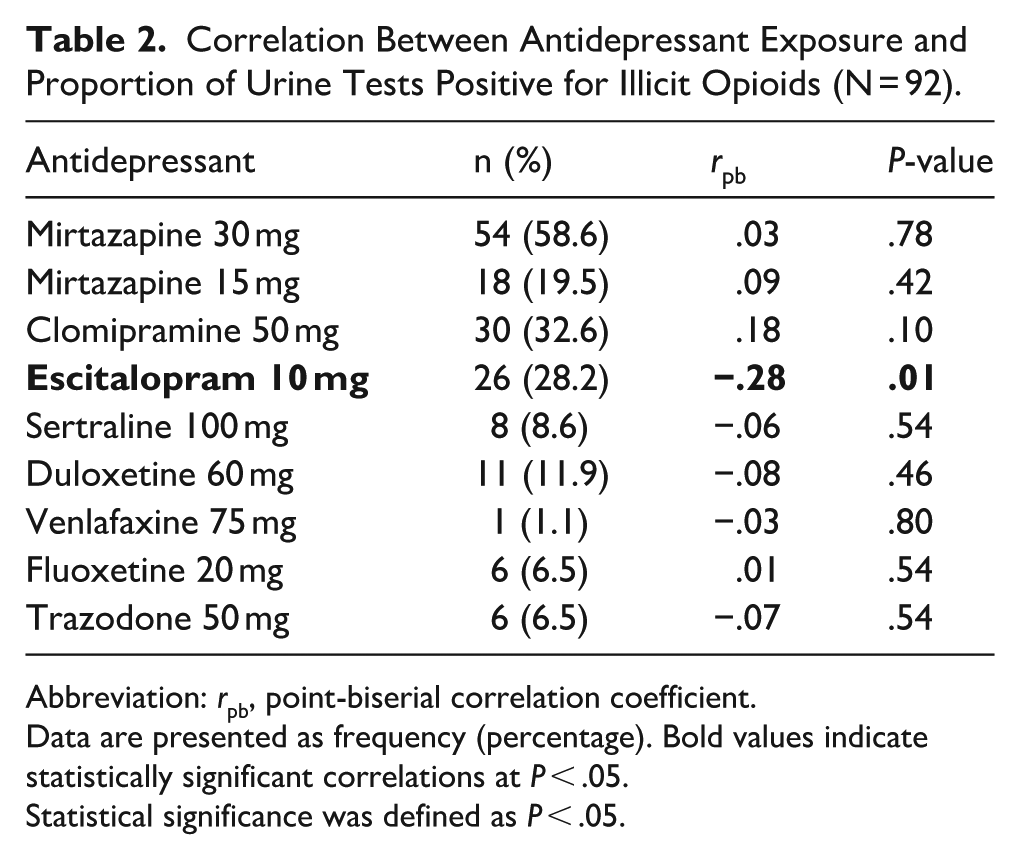
Abbreviation: rpb, point-biserial correlation coefficient.
Data are presented as frequency (percentage). Bold values indicate statistically significant correlations at P < .05.
Statistical significance was defined as P < .05.
A multivariate linear regression model was developed to model illicit opioid positive tests and exposure to escitalopram 10 mg accounting for age, buprenorphine elimination rate constant, and study allocation group. The model demonstrated a good fit, with lower variability than expected (Deviance/df = 0.12; Pearson χ2/df = 0.12) and provided better data fit compared with the intercept-only model (χ2(4) = 13.64, P = 0.009). Table 3 summarizes the regression model output. Accounting for buprenorphine elimination rate and study allocation group, escitalopram 10 mg (B = −0.22 [95% CI −0.39 to −0.04]) demonstrated significant negative association with illicit opioid use. Results suggest that participants who received escitalopram 10 mg were less likely to use illicit opioids compared with those who did not. In other words, for every prescription of escitalopram 10 mg, the proportion of urine tests positive for illicit opioids decreased by 0.22%. Similarly, age demonstrated significant negative correlation with illicit opioid use (B = −0.01 [95% CI −0.02 to 0.00]), suggesting that older participants are less likely to use illicit opioids compared with younger participants: that is, for every one-year increase in age, the proportion of urine tests positive for illicit opioid use decreases by 0.01%.
Multivariable Linear Regression Model of Escitalopram Exposure and Proportion of Urine Tests Positive for Illicit Opioids.
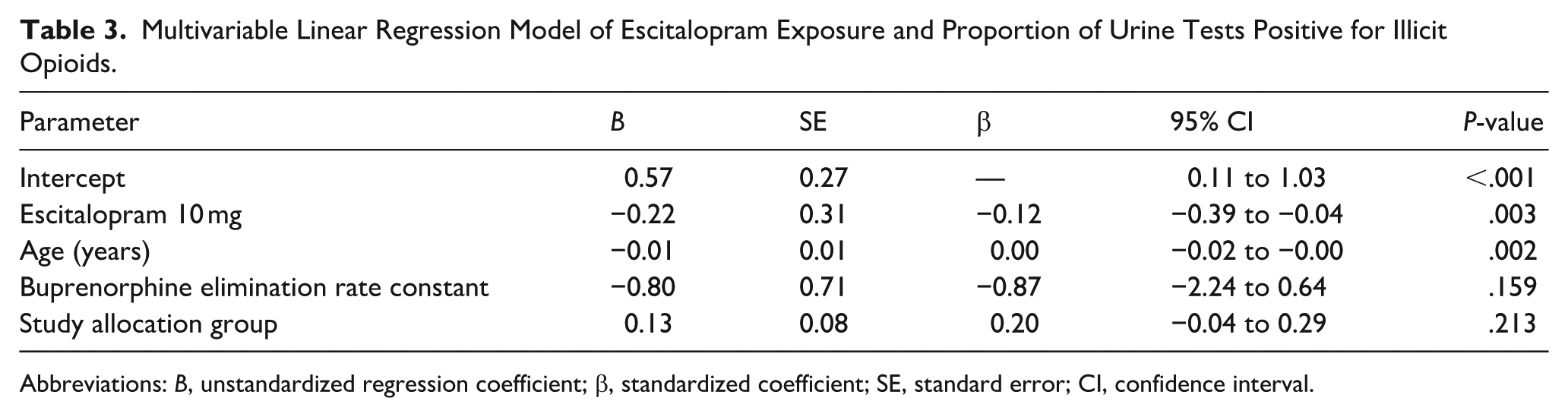
Abbreviations: B, unstandardized regression coefficient; β, standardized coefficient; SE, standard error; CI, confidence interval.
Table 3. Primary regression model of exposure to escitalopram 10 mg and illicit opioid use accounting for age, buprenorphine elimination rate constant and study group allocation.
The regression model was updated to add a two-way interaction between exposure to escitalopram 10 mg and age. The updated model was found to fit the data well with lower variability than expected (Deviance/df = 0.11; Pearson χ2/df = 0.11) and provided better data fit compared with the intercept-only model (χ2(5) = 18.92, P = .002). Table 4 presents the results of the updated regression model. Escitalopram 10 mg and age demonstrated a negative association with the proportion of urine tests positive for illicit opioid use (B = −0.93 [95% CI −1.54 to −0.32]) and (B = −0.02 [95% CI −0.04 to −0.01]), respectively. In contrast, the interaction between escitalopram 10 mg and age demonstrated a positive association (B = 0.025 [95% CI 0.004 to 0.04]). Results of this interaction suggest that the association between escitalopram exposure and illicit opioid use may vary by age.
Multivariable Linear Regression Model Including Interaction Between Escitalopram Exposure and Age.
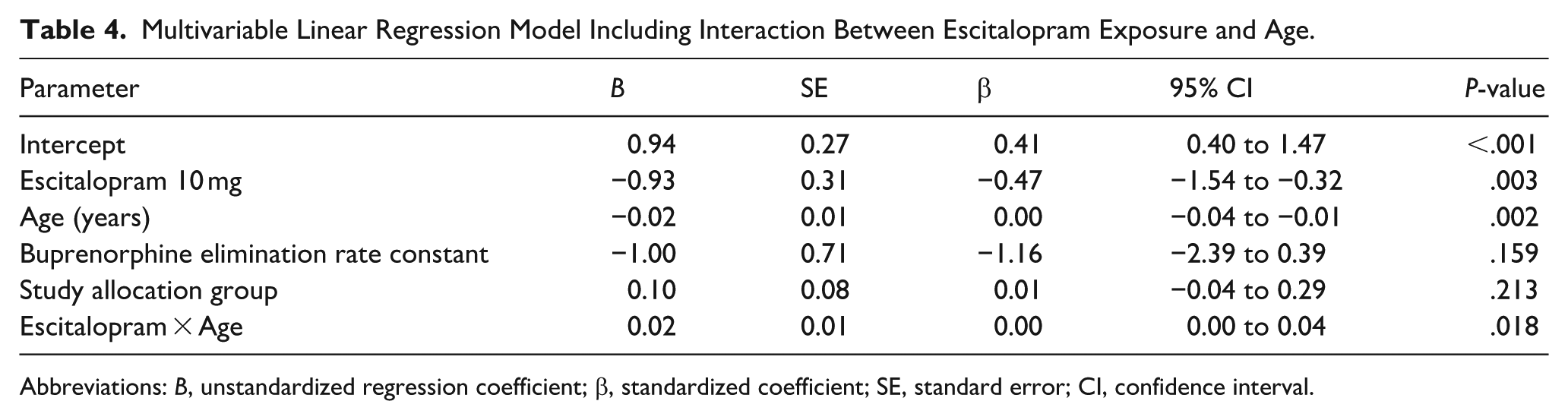
Abbreviations: B, unstandardized regression coefficient; β, standardized coefficient; SE, standard error; CI, confidence interval.
Discussion
This study explores whether antidepressants prescribed for adults with OUD and co-occurring mood disorders receiving buprenorphine/naloxone correlated with illicit opioid use. The null hypothesis set was that there is no correlation. Results indicate that exposure to escitalopram 10 mg was significantly correlated with lower rates of illicit opioid use. No correlation was observed with other antidepressants. Hence, the null hypothesis was rejected only for escitalopram 10 mg but retained for all other antidepressants.
The regression model developed to examine the association of escitalopram 10 mg with illicit opioid use accounted for variables reported to demonstrate significant correlation with illicit opioid use in this cohort, that is, age, buprenorphine elimination rate constant, and study allocation group.16,18 No other variable was included in the model to optimize the statistical power and precision. Results show a negative association between age and illicit opioid use, suggesting that the likelihood of illicit opioid use decreases with age. Furthermore, the interaction between exposure to escitalopram 10 mg and age revealed a significant positive correlation with illicit opioid use. Larger studies are required to understand the impact of this interaction on illicit opioid use and explore moderating factors associated with this interaction.
Despite the relatively weak associations observed with illicit opioid use, the findings of this study are of importance in the absence of, and the need for, specific guidelines on the treatment of adults with co-occurring OUD and mood disorders receiving MOUD. 23 Prior studies examining the association between antidepressant use and treatment retention have shown mixed findings and recommend further investigation of the impact of antidepressants on opioid use outcomes.13-15 To the authors’ best knowledge, no study has examined such impact or correlation despite the substantial prevalence of depression and prescribed antidepressants in adults with OUD. In fact, the present study reported a higher rate of prescribed antidepressants than previously reported rates (65.2% vs 35.4%). 12
The mechanism by which escitalopram affects illicit opioid use is unclear, nor is it clear whether this effect is dose dependent. Escitalopram, a selective serotonin reuptake inhibitor (SSRI), is indicated for the treatment of MDD and generalized anxiety disorder. 24 Emerging data suggest that serotonergic agents may influence opioid dysregulation, 25 play a role in inflammatory pain management, and attenuate opioid tolerance and dependence, providing a biologically plausible pathway for indirect effects on opioid use behaviors. 26 Additionally, SSRIs, mirtazapine, and tricyclic antidepressants were shown to indirectly affect opioid signaling through modulation of serotonin and opioid pathways.27,28
Limitations
Several limitations are to be considered when interpreting the findings of this study. First, this exploratory sub-analysis was not powered to detect correlations. Second, limited participation of females may contribute to limited generalizability of results due to the reported gender differences in the clinical profile of OUD29,30 and the level of response to buprenorphine-based treatment measured by illicit opioid use.31,32 Third, participants received antidepressants according to patient-specific clinical judgment rather than random allocation, hence introducing the possibility of confounding by indication and residual bias. Finally, the analyses were limited to the antidepressants and their respective doses prescribed in the primary study.
Conclusion
In this exploratory sub-analysis, the null hypothesis regarding the correlation between antidepressant exposure and illicit opioid use was rejected only for escitalopram 10 mg. Exposure to escitalopram 10 mg was associated with lower illicit opioid use among adults with OUD receiving buprenorphine/naloxone. The results should be interpreted considering the observational nature of the analysis and the relatively small sample size.
Larger, adequately powered prospective studies are needed to establish these findings, examine the effect of different doses of escitalopram on illicit opioid use, understand potential mechanisms underlying the association, and identify the impact of the escitalopram exposure and age interaction on illicit opioid use. Despite its limitations, this study highlights the potential clinical relevance of antidepressant selection to optimise treatment outcomes in individuals with OUD and co-occurring mood disorders receiving MOUD.
Footnotes
Acknowledgements
The authors would like to thank the Scholarship Office (SCO) at the Ministry of Presidential Affairs in the United Arab Emirates for providing the educational assistance required to accomplish this work. The authors would like to express their gratitude to the National Rehabilitation Center-Abu Dhabi in the United Arab Emirates.
Ethical Considerations
This sub-analysis of data from the Suboxone Treatment and Recovery Trial (STAR-T) 18 was conducted in accordance with the International Conference on Harmonisation Good Clinical Practice guidelines and the Declaration of Helsinki. Ethics approval was obtained from the Institutional Review Board of the National Rehabilitation Centre (NRC), Abu Dhabi, United Arab Emirates (Approval No. NRC/2/2014). The trial was registered with ISRCTN (ISRCTN41645723). All participants provided written informed consent, and data were managed in accordance with applicable governance and confidentiality standards.
Author Contributions
The study was a collaborative effort among multiple contributors:
• Hesham Farouk Elarabi contributed significantly to the conceptualization, design, methodology, data analysis, and manuscript writing.
• John Marsden provided valuable insights during data interpretation and contributed substantially to manuscript revision.
• Abdu Adem was instrumental in developing the study’s theoretical framework and refining the methodology.
• Hamad Al Ghafri contributed to the conceptualization, design, methodology, data analysis, and manuscript review.
• Ahmad Muneer (Corresponding Author) played a key role in the conceptualization, methodology development, and preparation of the manuscript.
• Amanda J. Lee contributed to data interpretation and provided critical feedback during the manuscript revision process.
• Mansour Assaf provided vital input to the study’s conceptualization and participated in the critical revision of the manuscript.
All authors have reviewed and approved the final manuscript for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All expenses associated with the study were covered by the authors themselves.