
Abstract
Background:
Ongoing cocaine use is common during methadone treatment and is associated with poorer outcomes. Digital health tools offer promising new ways to enhance methadone treatment through remote delivery of adjunctive behavioral health interventions. The experiences of patients on methadone who also use cocaine are under-represented in the recent literature. This qualitative study of recently admitted patients on methadone who also used cocaine examines their experiences and views on drug use and treatment.
Methods:
Twenty-one participants were purposively sampled from the intervention arm of an ongoing multi-site clinical trial of a digital behavioral intervention. Qualitative interviews were carried out approximately 3 months after randomization into the parent study.
Results:
Three themes emerged from the analysis: (1) Cocaine Use as a Response to Physical and Emotional Factors; (2) Cycles of Use and Recommitment to Treatment; and (3) Active Efforts to Sustain Engagement in Treatment. Participants were able to identify and share reasons for entering treatment and their persistent cocaine use. Many participants emphasized a hope that methadone treatment would be temporary. Several participants highlighted the role of internal factors (eg, stress, shame, and desire for stability) related to treatment engagement, and the role of adjunctive behavioral supports in targeting internal factors.
Conclusions:
Individuals with opioid and cocaine use enter methadone treatment for different reasons, often with co-occurring substance use disorders. Aligning care with their individual goals can potentially improve outcomes. Grounding treatment strategies in individuals’ lived experiences can deepen understanding of how adjunctive digital behavioral interventions can best support engagement, retention, and recovery during the critical early phases of treatment, especially as the illicit drug supply becomes more complex.
Keywords
Highlights
Cocaine use is common among patients on methadone and affects treatment retention.
Few studies explore the views of patients on methadone with concurrent cocaine use.
Understanding patient perspectives can improve methadone treatment strategies.
Innovative adjunctive therapies hold potential to improve engagement and outcomes.
Introduction
There were over 80 000 drug overdose deaths in the United States in 2024, 1 demonstrating a critical and ongoing public health crisis. Shifts in the drug supply from heroin to fentanyl, alongside concurrent use of stimulants, are key factors driving the ongoing evolution of the overdose crisis. 2 Methadone treatment is effective in reducing non-prescribed opioid use, 3 and treatment engagement is associated with a reduced risk of overdose death. 4 However, the current prevalence of co-occurring cocaine use among patients on methadone is increasing and interferes with methadone treatment success. 5 Successfully treating co-occurring opioid and cocaine use is a necessary step in overcoming the current opioid epidemic.6,7
Concurrent cocaine use is associated with poorer methadone treatment outcomes.8-10 For decades, clinical trials have shown that contingency management (CM) and cognitive behavior therapy (CBT) can decrease cocaine use among patients in methadone treatment.11-15 Yet CM and CBT remain under-utilized for people using cocaine in methadone treatment due to the need for staff training and supervision, added requirements for staff time, and the funding structure of methadone treatment and lack of widespread insurance coverage for CM in the United States.16,17
Digital health tools provide a promising approach for overcoming barriers to delivering CM and CBT for people with substance use disorders (SUDs). 18 Digital therapeutics for the treatment of SUDs are rooted in behavior change theory19,20 and include applications such as ReSet-O 21 and DynamiCare Health. 22 Digitally delivered CM offers a more scalable, accessible, and user-centered approach than traditional CM by providing participants with monetary incentives for meeting treatment goals (eg, remotely observed negative drug tests). 18 Similarly, digitally delivered CBT modules, including educational content and reflective exercises with immediate feedback, can provide a more individualized, accessible approach to internal factors related to substance use, such as stress, anxiety, shame, and cravings. Digital health tools have the potential to improve engagement in opioid use disorder (OUD) treatment and prevent early drop-out. 19 Despite these advances, little is known about the recent experiences of individuals who continue to use cocaine while in methadone treatment, particularly in the context of emerging digital interventions such as CM.
Current patient perspectives on drug use and methadone treatment in the era of fentanyl, including individuals’ motivations for entering and remaining in treatment in the context of co-occurring cocaine use, could help inform treatment innovations.23,24 This study examines how concurrent cocaine use shapes participants’ experiences with methadone treatment, including treatment entry, engagement, and maintenance, as well as the perceived benefits of a digital behavioral intervention as an adjunctive behavioral therapy to methadone treatment.
Methods
This study was conducted as a part of a randomized controlled trial (R01CA255414) evaluating the efficacy of a digital behavioral intervention designed to improve outcomes among individuals with co-occurring opioid and cocaine use entering methadone treatment, the methods of which are described elsewhere. 25
Participants
Participants were eligible for inclusion if they had a recent history (ie, past 30 days) of co-occurring opioid and cocaine use and were enrolled in methadone treatment at 1 of 4 OTPs in Baltimore, Maryland. All qualitative interview participants were randomly assigned to the intervention arm and received a digital behavioral intervention through the DynamiCare Health app. The app includes CBT-based educational modules and is engineered to deliver CM with financial incentives for 2 separate behaviors: (1) cocaine- and opioid-negative oral fluid tests, for which participants were prompted by the app at random (1-2 times weekly) to upload a video of the self-administered oral fluid test and (2) picking up scheduled methadone doses at the OTP, either directly observed or as take-home medication. 25 An ascending incentive scale for participants who submitted oral fluid tests can be viewed in the published protocol. 25 Participants received $50 for each qualitative interview completed (up to 3). All participants provided informed consent, and the WCG Institutional Review Board approved this study (IRB#20224448).
Procedures
Between March 2024 and July 2025, 2 researchers conducted and recorded qualitative interviews approximately 3 months after each participant’s admission into the OTP. Each interview lasted approximately 45 minutes and used a semi-structured interview guide (Figure 1) that explored participants’ experiences with cocaine use during methadone treatment, treatment entry and engagement, and perspectives on the digital behavioral intervention through the DynamiCare Health app. Participant demographic information was collected at the time of the interview.
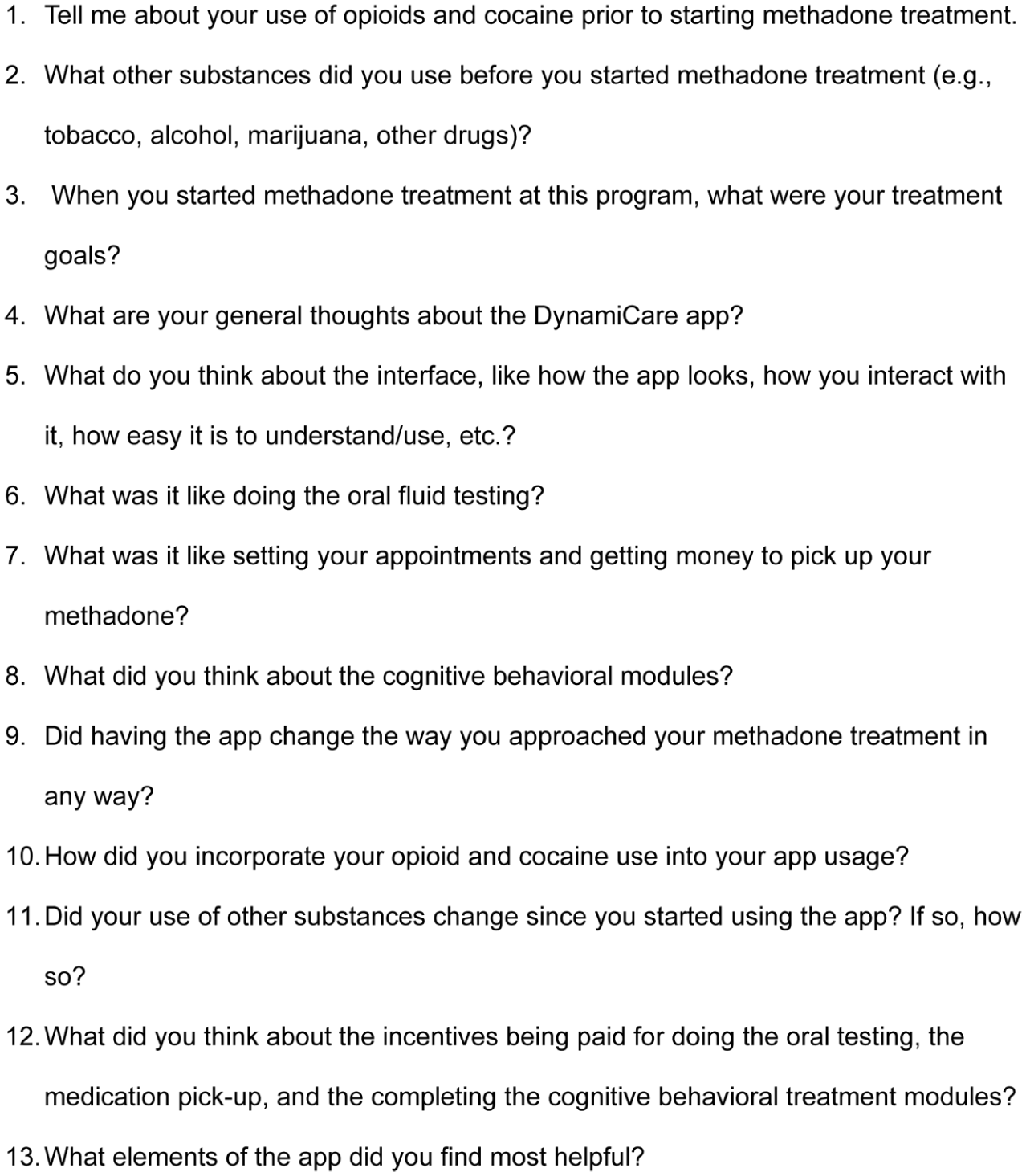
Semi-structured interview guide. These questions were used during the interview with participants who used the DynamiCare Health app.
Data Analysis
All interviews were digitally recorded and transcribed verbatim, with participant names and other potentially identifying information omitted. Transcripts were reviewed for accuracy and imported into NVivo software (NVivo 15) for organization and coding. The research team used a thematic analysis approach, as outlined by Braun and Clarke.26,27 We followed a systematic process where we (1) familiarized ourselves with the transcripts, (2) generated initial codes to identify key features of the data, and (3) grouped these codes into potential themes. The coding team (R.F., K.A., A.Schachter) independently double-coded 27% of transcripts, with discrepancies discussed until consensus was reached and the codebook refined iteratively. The remaining transcripts were subsequently coded independently by members of the coding team using the established codebook. Codes were iteratively reviewed and refined, ensuring they accurately represented the data and were distinct from one another. The final analysis stage involved defining and naming each theme, with a constant awareness of how our perspectives and assumptions influenced the process of constructing meaning from the dataset.
Results
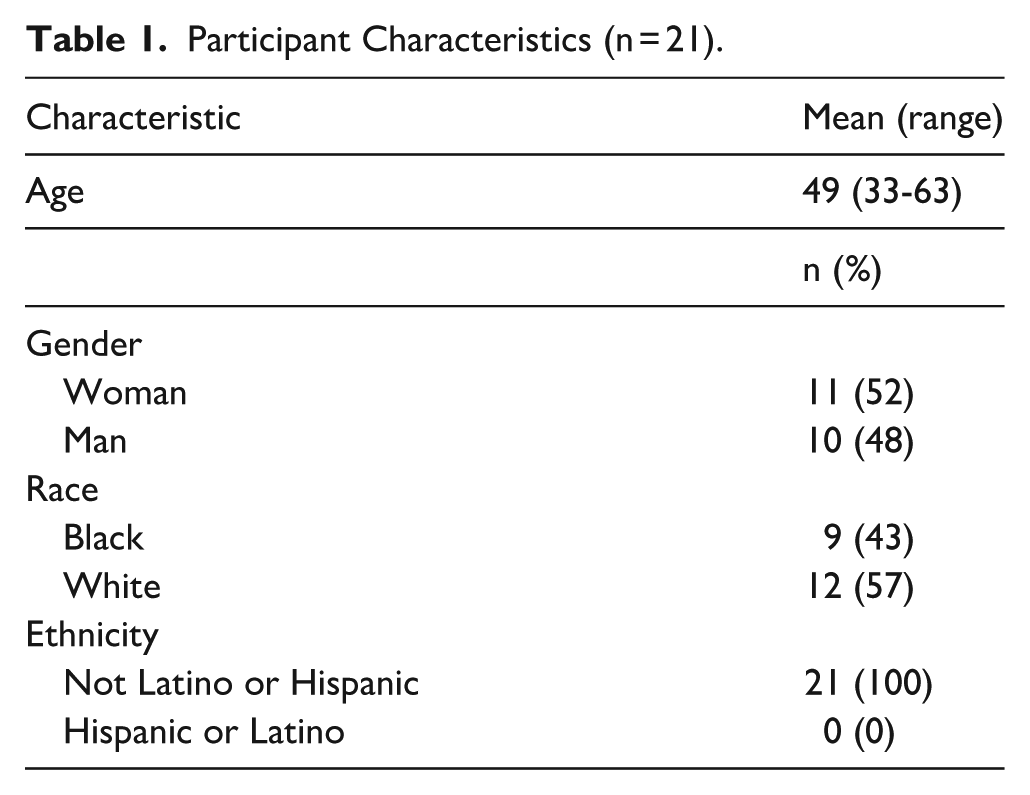
We conducted interviews with 21 participants who had a recent history of co-occurring opioid and cocaine use, had recently begun methadone treatment, and were randomized to the digital behavioral intervention. Participant characteristics are found in Table 1. Participants were on average 49 years old, ranging between 33 and 63 years of age. The sample was almost evenly divided by gender, with 11 female participants (52%) and 10 male participants (48%).
Participant Characteristics (n = 21).
Three themes emerged from the analysis: (1) Cocaine Use as a Response to Physical and Emotional Factors; (2) Cycles of Use and Recommitment to Treatment; and (3) Active Efforts to Sustain Engagement in Treatment. Illustrative quotations for Themes 1 to 3 are found below and in Tables 2 to 4, respectively.
Illustrative Quotations for Theme 1: Cocaine Use as a Response to Physical and Emotional Factors.

Illustrative Quotations for Theme 2: Cycles of Use and Recommitment to Treatment.

Illustrative Quotations for Theme 3: Active Efforts to Sustain Engagement in Treatment.

Theme 1: Cocaine Use as a Response to Physical and Emotional Factors
Nine participants (4, 5, 6, 8, 9, 12, 17, 19, 20) described continued cocaine use during methadone treatment as a response to both physiological and emotional instability. While methadone addressed opioid withdrawal, many participants (8,9,12,19, 20) reported persistent cravings, emotional distress, and environmental triggers that contributed to ongoing cocaine use. These participants reported using drugs to cope with emotional distress, such as trauma, grief, and depression, as well as to manage physical symptoms of withdrawal and dependence, with these motivations varying by substance. As one participant shared: “[Drugs] just alleviate, just lessen my pain away from the problem for a minute. That’s all.” (Participant 5). Another participant noted that loneliness and routine contributed to use while in treatment: “I know that boredom plays a big part in it. . .because I stay to myself in my house most of the time. I think it’s mostly boredom and just being used to doing a substance.” (Participant 4).
The remaining illustrative quotations for Theme 1 are found in Table 2. Many participants (8, 19, 20) reflected on prior drug use before entering treatment and reported using drugs to ease mental health symptoms, such as unresolved grief or depression. Participants (9, 19) also commented on the ubiquity of drugs in their social circles, which facilitated continued use. Some participants (9, 12) felt that the changing drug supply in Baltimore contributed to their drug use.
Differences in use patterns were noted between cocaine and opioids, with particular attention given to how cocaine interacts with methadone. Participants (5, 9, 17, 20) often referred to opioids as “heroin” or “dope,” even when acknowledging that fentanyl was the opioid dominating their supply. Many participants (5, 8, 12, 17, 18) described their opioid use as decreasing as their methadone dose increased, but this was contrasted with their cocaine use. Experiences of continued cocaine use were more common and varied, with some participants (12, 18) reporting that their cocaine use stayed stable or increased, while others (5, 17) reported gradual decreases in cocaine use. Participant 8 spoke of cocaine cravings increasing after beginning methadone treatment. Even with physical dependence to opioids addressed through methadone dosing, participants said the craving and desire “to get high” remained.
Theme 2: Cycles of Use and Recommitment to Treatment
Participants’ decisions to enter or return to methadone treatment often reflected cycles of drug use and recommitment to recovery, shaped by strong internal factors such as self-awareness of negative consequences and a desire for stability. Eleven participants (2, 3, 6, 7, 8, 9, 13, 15, 16, 18, 19) entered treatment as a response to an unwanted return to drug use, deciding to stop all drug use, or confronting the emotional and social impacts of use, including self-stigma and shame.
Unwanted Return to Drug Use
Many participants (6, 15, 16, 20) mentioned that they sought treatment as a response to their unwanted return to drug use. As one participant described: “I had relapsed and I was done using, and . . . Well, I started using the fentanyl and then I had enough of the fentanyl, so I got back on the methadone.” (Participant 15). The decision to re-enter treatment reflects a clear recognition of the need for support and a desire to regain stability. For some, this moment of clarity becomes the catalyst for re-engaging with treatment services, even after prolonged periods of drug use. Another participant shared: Prior to [entering treatment], I’ve been clean for a couple years and in doing so, I relapsed, went back to using a couple times a week and turned into four or five times a week, then it turned into every day. . . And after ripping and running for about a year and a half or so, I relapsed and pretty much that’s what brought me to the program. (Participant 20).
The remaining illustrative quotations for Theme 2 are found in Table 3.
Making Up One’s Mind to Stop Drug Use
Many participants (2, 9, 18, 19) identified their own desire to stop drug use as a turning point for entering treatment, often accompanied by feelings of being “sick” and “tired” of their drug use and consequently their life circumstances. Participant 9 shared that their experience with recovery played a significant role in their decision to enter treatment. For this participant, recalling the sense of stability and improved quality of life during prior recovery created a compelling reason to re-engage with treatment, highlighting how internal reflection with “what is possible” can create intrinsic motivation and sustain hope despite repeated relapses.
Awareness of Negative Sequelae of Drug Use
Five participants (3, 9, 13, 15, 19) were aware of the negative sequelae associated with drug use, noting the physical, psychological, social, and financial effects of drug use on their lives. As one participant noted, “It caused money problems, financial problems, fighting problems in my relationship. . . I lost my kids. It ruins my life.” (Participant 15). Another participant shared that they would pursue drugs “By any means necessary, when I saw something I wanted, that I would go out and get it, whether it was stealing it, robbing or whatever, selling drugs, whatever.” (Participant 19). These effects served as a catalyst to pursue treatment. One participant (9) acknowledged being aware of unwanted substances in the current drug supply but still choosing to use them. Some participants recognized the significant impact their addiction had on their decision-making. Participants (9, 19) mentioned that they were often at a point where they would do anything for drugs. The recognition of these consequences led some participants to seek treatment.
Self-Stigma and Shame
Participants (2, 7, 8, 9) highlighted internal factors, such as self-stigma and shame associated with their drug use, often expressing the need to hide their drug use from others. For some participants, feelings of stigma and shame contributed to isolation. For others, isolation fueled a desire to seek treatment.
Theme 3: Active Efforts to Sustain Engagement in Treatment
Ten participants (4, 8, 9, 14, 15, 16, 18, 19, 20) described engagement in treatment as targeting their physical and emotional needs, supported by interpersonal relationships, internal motivation, and structural supports. Key treatment facilitators included: support from family and/or partners, internal motivation and future-oriented goals, personal healing and growth, support from treatment programs and professionals, short-term or immediate effects of treatment, and the therapeutic benefits of methadone. Adjunctive, behavioral support, such as the digital behavioral intervention, was considered by some to be a facilitator of treatment engagement and success. These supports were often described in relation to maintaining engagement in treatment while managing ongoing cocaine use.
Support From Family and/or Partners
Many participants (3, 9, 14, 15) felt that support from their family and/or partners was an important factor in their treatment progress. As one participant explained: “She know[s] what I’ve been doing with y’all. . . My mom’s always in my corner.” (Participant 14). Additional illustrative quotations for Theme 3 are found in Table 4. Some participants were undergoing treatment alongside their partners and felt that this supported their progress.
Internal Motivation, Goals, and Personal Growth
Seven participants (3, 6, 8, 12, 14, 19, 20) acknowledged that addressing their internal challenges and focusing on personal growth were essential for progress in their treatment. Participants (14, 20) described internal motivation as coming from self-reflection and healing, and also as a future-oriented process that included setting long-term goals and reevaluating the role of substances and treatment in their lives. Beyond self-reflection, participants turned to sources of strength outside themselves. For some, spirituality offered a framework for resilience and guidance in recovery.
Participants’ motivation to remain engaged in treatment was often linked to aspirations beyond immediate stabilization, including employment, education, family reconciliation, and regaining a sense of autonomy. Many participants (9, 19) articulated a desire to eventually discontinue methadone treatment, viewing it as a temporary support rather than a lifelong intervention. As one participant shared: “I needed methadone to help me get clean and maybe help me abstain for a little while. . . If you’re clean and you’re doing what you’re supposed to do, there’s no reason to be on it so long.” (Participant 9). Other participants (12, 19) described the effects they believed methadone could have with long-term use. One participant said: I know I’m going get off the methadone too, because just due to the effects of it. . . I just want to be, one of the things I often think about is how it feels not to have to put anything [in my body] in order to change, deal with pain or to change my mood or anything. You know what I mean? (Participant 19).
While participants recognized that tapering methadone is complex and challenging, these reflections were not expressions of disengagement. Rather, they reflected an active process of meaning-making and goal-setting that helped sustain engagement in the present while imagining a different future. Continued treatment engagement was therefore shaped by a tension between the benefits of stabilization and the desire for long-term autonomy, a tension often compounded by stigma surrounding methadone treatment.
Support From Treatment Programs and Professionals
Five participants (8, 9, 15, 17, 19) highlighted the valuable role that treatment programs and professionals played in their treatment. Supports included participation in group sessions, 12-step meetings/Narcotics Anonymous (NA), and relationships with counselors and sponsors. Participants felt that these sources of support provided encouragement and a sense of accountability. Some participants (15, 17) found value in attending NA meetings and engaging with their sponsors. One participant (15) emphasized the importance of working the program with their sponsor.
Short-Term or Immediate Effects of Treatment
Four participants (8, 12, 14, 18, 19) described notable positive physical and mental effects of starting treatment and reported an increase in mental clarity and overall well-being. In addition, some participants (12, 14, 18) mentioned that their energy and appetite have improved drastically since beginning methadone treatment. One participant noted that treatment helped “in a lot of ways. I go to sleep on time, brush my teeth, wash my feet or take a shower every day. I eat every day something. I wasn’t doing none of that.” (Participant 18).
Participants were knowledgeable about the therapeutic effects and benefits of methadone treatment, and they understood methadone as both physiologically effective and practically beneficial in supporting recovery. For some, methadone was able to reduce physical dependence symptoms but did not address psychological symptoms, underscoring the distinction participants made between physical stabilization and the ongoing psychological struggle with use.
There was a broader concern among some participants that concurrent cocaine use may interfere with the effectiveness of methadone. Participants (8, 9) noted that methadone is widely thought to be less effective in the context of continued cocaine use. These concerns illustrate how co-use of stimulants shaped participants’ beliefs about the limitations of methadone treatment, beliefs grounded in physiological experiences. The bidirectional feedback between body and mind highlights the potential of digital therapeutics to enable participants to obtain personal insight and self-manage this cycle outside of traditional clinical settings.
The Digital Behavioral Intervention
Five participants (4, 9, 15, 16, 20) described the digital app as a facilitator of treatment engagement and highlighted how the app’s CBT content and CM incentive structure supported their motivation and adherence to treatment goals. As one participant reflected, “Your app, I guess, really had a big part [in my recovery] too. That helped me as well. Just being in this program has helped a lot tremendously.” (Participant 15). Another participant similarly shared that “[The incentives] does motivate me to get my methadone. It really does.” (Participant 16). Some participants (4, 15) noted that they were able to apply the educational modules to their recovery, with one participant sharing: “I like . . . learning different things because the more I learn, it helps me . . . apply it into my life.” (Participant 4). Other participants (16, 20) emphasized how the app bolstered their confidence and motivation, contributing to their desire to stay in treatment, sharing that “It kind of gives me my confidence back. Gave me stride and the desire to want to get clean.” (Participant 20).
Participants (9, 16, 20) also reflected on the benefits of CM, specifically how the incentives helped maintain treatment participation. One participant reflected that “It’s definitely a motivator to go and get that $2 for that day.” (Participant 20). The financial rewards were particularly valuable to those facing economic challenges. CM not only bolstered treatment commitment but also addressed immediate material needs, making participation more feasible and sustainable. These supports were critical for maintaining engagement while managing ongoing cocaine use.
Discussion
This qualitative study was conducted as part of an ongoing, multi-site randomized clinical trial examining the efficacy of a digital behavioral intervention during methadone treatment for people with co-occurring cocaine and opioid use. Participants described a range of reasons for drug use, including fear of withdrawal, coping with mental health challenges, including depression, and the normalization of drug use in their social environment. Decisions to enter treatment were often driven by the negative impact of drug use on their lives, their resolve not to return to use, and the stigma of drug use. Following treatment entry, key supports facilitated engagement, including interpersonal relationships, internal motivation and personal growth, supportive treatment environments, the therapeutic effects of methadone, and behavioral supports provided by the digital intervention. Participants more often viewed methadone treatment as temporary, rather than long-term, and frequently cited future goals to seek further education or employment.
Concurrent cocaine use alongside methadone treatment plays a distinct role in shaping treatment experiences during methadone care.28,29 Cocaine use in the context of OUD complicates treatment and is associated with negative outcomes.30-32 In our study, participants described cocaine use not simply as continued substance use, but as intertwined with efforts to manage mood, energy, and withdrawal-related discomfort. This finding underscores the need for treatment approaches that explicitly address internal factors related to use within opioid treatment settings, particularly during early treatment engagement. While participants described broader motivations for treatment, our analysis focuses on how these experiences intersect with ongoing cocaine use and engagement in methadone care. Extant research has infrequently explored patient perspectives on initiating methadone treatment within the context of co-occurring cocaine use. 33 Given the large-scale replacement of heroin with fentanyl in the drug supply in the United States and the increasing co-use of fentanyl and cocaine, it is essential to update our understanding of the perspectives and experiences of people on methadone using cocaine.5,7,34,35
Cocaine use is often driven by intense craving, emotional factors, and physiological dysregulation during OUD treatment.36,37 Participants in our study noted that cocaine use during methadone treatment can increase opioid craving, an observation consistent with prior research.38,39 In such cases, an increase in methadone dose can decrease non-prescribed opioid use and craving but not necessarily cocaine use. 40 As noted by one study participant, tolerance to cocaine itself can occur,23,41 intensifying cravings and physiological discomfort that may be misattributed to methadone. This interaction complicates treatment by creating a cycle in which stimulant-related restlessness and dysphoria undermine the stabilizing effects of methadone. Recognizing these physiologic dynamics is essential to understanding how co-use shapes perceptions of methadone’s effectiveness. Given the challenges presented by cocaine use in methadone treatment, it is essential to develop and scale up the use of adjunctive cocaine use interventions shown to be effective during standard methadone treatment.
Depressive symptoms played a role for some participants, but craving and physiologic distress appeared to be more central motivators of ongoing cocaine use during methadone treatment. Fortunately, depressive symptoms associated with SUD often improve with treatment. 42 Future treatment approaches must integrate a more comprehensive understanding of the physiological and affective dimensions of polysubstance use, recognizing the multifaceted needs of individuals navigating a shifting substance use landscape. 6
Both CM and CBT have demonstrated effectiveness in trials for cocaine use in methadone treatment.12,14,15 Unfortunately, these treatments remain underutilized in SUD treatment programs.43,44 Barriers to implementing CM include financial constraints and ideological resistance to providing rewards for recovery, while challenges related to CBT often involve the need for extensive staff training and ongoing supervision. 43 To address these barriers, novel approaches are still needed. 45
One novel approach to providing effective treatments for cocaine in the context of methadone treatment is to use digital therapies, as was implemented in the current study. A number of digital therapies show efficacy in treating SUD, including ReSet for cocaine and marijuana use, ReSet-O as an adjunct to buprenorphine treatment for OUD, and Dynamicare for nicotine use disorder. 20 The DynamiCare Health app was viewed by participants in the present study as beneficial for enhancing motivation through learning and small financial incentives. Participants’ perspectives on the digital behavioral intervention demonstrate its potential as a supportive tool for sustaining engagement, particularly through reinforcement, structure, and accessible, autonomous behavioral support. While the effectiveness of the digital behavioral intervention may be tied to participants’ existing motivation and readiness for change, participants also noted how the app was a motivating factor for them to engage with and stay in OUD treatment. It is possible that digital tools may function best as complements to, rather than substitutes for, relational and program-based supports. Building on participants’ insights regarding their motivations for treatment and the facilitators of engagement, it is equally important to explore how the social context shapes treatment engagement and overall recovery experience. Participants emphasized forming new, non-drug-using social networks as a desired pillar of recovery and life improvement. 46
Many participants in this study planned on remaining in methadone treatment for a limited time only. Reasons for this view are complex, although stigma and misinformation may play key roles.47,48 It is critical for patients in methadone treatment to receive evidence-based information about the benefits of treatment retention and the risks associated with leaving treatment so that they may make an informed decision about leaving care. Many participants hoped to engage in workforce and educational opportunities in the future, though this study did not explore why participants felt unable to pursue such opportunities while in OUD treatment. Retention in treatment does not preclude education or employment, and future work should explore why people may view methadone treatment as incompatible with employment or education. Individuals with OUD face a significantly heightened risk of return to use and overdose when not in treatment; maintaining engagement in care is often the most effective way to support long-term recovery and survival. 49
Our findings emphasize the need for treatment models that are flexible, responsive to patient-defined goals, and inclusive of the realities of polysubstance use. 50 Importantly, participants described recovery as a holistic process, including an emphasis on core values of stability, purpose, relationships, and self-worth. Recommendations based on our findings include assessing patients carefully for depression and unresolved grief, addressing stigma, providing accurate information about risks and benefits of methadone treatment, and utilizing CM.
This study has several limitations. First, the findings may not generalize to other parts of the United States or internationally, where methadone treatment is often delivered differently (e.g., through physician offices and pharmacies). Second, we recruited people who had been in treatment for approximately 3 months and were reflecting on their reasons for entering and remaining in treatment, which may be subject to recall bias and limit generalizability to retained participants. Finally, we did not interview individuals who had dropped out of treatment within the first 3 months, introducing a possible selection bias toward people more successful in remaining in treatment.
This report is part of an ongoing, larger clinical trial evaluating the integration of a digital behavioral intervention involving digital CM and CBT into methadone treatment with a focus on improving methadone retention and reducing opioid and cocaine use. 25 Together, these efforts aim to enhance the effectiveness of methadone treatment for individuals with co-occurring OUD and cocaine use. Further qualitative research is needed to explore recovery narratives across diverse populations to inform more responsive and equitable treatment approaches.
Conclusions
These qualitative findings offer rich insights into the multifaceted experiences related to entering methadone treatment in the fentanyl era with co-occurring cocaine use while using an adjunctive CM app. The themes that emerged highlight the importance of using a person-centered behavior change approach. An approach grounded in individuals’ perspectives will aid in the understanding of the role that adjunctive behavior change interventions can play in the treatment and early recovery process.
Footnotes
Acknowledgements
The authors would like to thank the participants who shared their valuable perspectives for this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors (KA, AS, JG) received funding from NIDA grant R01DA057608 during the preparation of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.