
Abstract
Background and Objectives:
The current study investigates the roles of assertive outreach, individual participant involvement, and treatment significant other (TSO) involvement through the Medication Adherence Therapy: Psychosocial Leverage Using a Significant other (MAT-PLUS) intervention on extended-release naltrexone (XR-NTX) adherence for the treatment of opioid and/or alcohol use disorder (OUD/AUD).
Methods:
Participants receiving XR-NTX for OUD and/or AUD received 16 weeks of the MAT-PLUS intervention through a prior randomized controlled trial (RCT). Logs tracked XR-NTX adherence, treatment team outreach, and participant/family communications and sessions.
Results:
Of the contact types examined, only the number of family sessions attended significantly predicted next XR-NTX dose receipt (OR = 8.74, 95% CI [1.84, 54.41]) in n = 12 participants.
Conclusions:
Family involvement is an important component of OUD/AUD treatment that may improve XR-NTX adherence.
Clinical Trial Registration:
Treatment of opioid use: Medication Adherence Therapy (MAT-PLUS), https://clinicaltrials.gov/study/NCT03567356?term=MAT-PLUS&rank=1, NCT03567356
Highlights
Secondary analysis of the Medication Adherence Therapy: Psychosocial Leverage Using a Significant other (MAT-PLUS) intervention pilot randomized controlled trial data examining predictors of extended-release naltrexone adherence.
Treatment significant other attendance in family sessions strongly associated with receiving the next extended-release naltrexone dose (OR = 8.74, 95% CI [1.84, 54.41]).
Introduction
Extended-release naltrexone (XR-NTX) is effective for treating opioid use disorder (OUD) and alcohol use disorder (AUD). 1 However, issues with medication adherence remain an understudied obstacle in the effectiveness of XR-NTX. 2 Although there are several promising strategies to improve medication adherence, few have been investigated in the context of substance use disorders (SUDs).
Assertive outreach has improved treatment engagement and retention among individuals with severe mental illness,3,4 and there is a growing interest in its application to SUDs. The overarching principle is to proactively stay engaged with high-risk populations in order to reduce crisis-driven healthcare utilization and improve quality of life. 4 Assertive outreach models anticipate significant barriers to consistent engagement and push staff to initiate contact to keep patients connected. These principles could be leveraged to improve adherence to pharmacotherapy for SUD, but this area of research is underdeveloped.
Another promising strategy to improve medication adherence is involving family members or treatment significant others (TSOs) in treatment. Involving TSOs typically entails 2 guiding principles: partnering with the patient’s family or other supporters to help the patient initiate and stay in treatment; and providing support for the supporters themselves. 5 This approach leads to better outcomes for the patient and their TSOs, including increased pharmacotherapy adherence and treatment engagement, reduced substance use, continued abstinence, decreased stress and strain in support persons, and improved family functioning.5,6 Despite the evidence and expert consensus, family-based interventions are underutilized in usual practice due to barriers related to cost, logistics, and inadequate training. 7
Another important factor in improving treatment outcomes for behavioral interventions is the degree to which a patient engages in the intervention components. Patient engagement during treatment, often modeled as therapeutic involvement and attendance, positively predicts treatment outcomes, including retention. 8 However, many previous studies evaluate therapy attendance while individuals are inpatient, during which attendance is often mandatory or enforced, and little research has been conducted on the impact of engagement on outpatient medication adherence.
The Medication Adherence Therapy: Psychosocial Leverage Using a Significant other (MAT-PLUS) intervention is a novel, multicomponent, behavioral approach and service delivery model incorporating assertive outreach and TSO involvement to promote adherence to XR-NTX. The model has shown preliminary positive effects on XR-NTX retention in a pilot randomized controlled trial (RCT), with participants in the MAT-PLUS intervention receiving more doses than those in the treatment-as-usual (TAU) group: 3.4 versus 2.5 doses and 61.1% receiving all prescribed doses versus 30.4%, giving a Number Needed to Treat of 3.3. 9 Although these findings point to the preliminary efficacy of the MAT-PLUS intervention, the degree to which its components and engagement in its components impact XR-NTX adherence is unknown. Therefore, the purpose of this secondary analysis was to investigate the impact of the MAT-PLUS intervention components (ie, assertive outreach, individual sessions, and family sessions) on medication adherence by evaluating the likelihood of receiving the next XR-NTX dose. We hypothesized that participants with greater engagement indicators and uptake of the intervention components would be more likely to receive their next XR-NTX dose.
Methods
This study is a secondary analysis of a pilot RCT of MAT-PLUS, which tested MAT-PLUS layered on top of TAU versus TAU alone on the primary outcome of the number of XR-NTX doses received over the 16-week intervention. In the parent study, a convenience sample of 45 participants with OUD and/or AUD who were planning to initiate treatment with XR-NTX were recruited from a residential SUD treatment program (ie, American Society of Addiction Medicine level 3.5 or above) and randomized equally to 16-weeks of MAT-PLUS or TAU. Other inclusion criteria were: endorsed opioid and/or alcohol use within the past month, planned to engage in outpatient care with the same community treatment provider, identified a potential TSO to be involved in their SUD treatment, and did not have medical, legal, or living situations that would make participation in the study unsafe. 9 Prior to discharge from the residential treatment setting, usual care consisted of SUD counseling and care coordination to facilitate the transition to outpatient care. Outpatient usual care included individual and group SUD counseling sessions, medication management, and XR-NTX. The MAT-PLUS intervention incorporated TSO involvement (e.g., family sessions with MAT-PLUS therapist focused on XR-NTX adherence) and assertive outreach (e.g., text messaging, phone calls, appointment reminders related to XR-NTX adherence and relapse prevention). Investigators held weekly supervision with the MAT-PLUS therapists and study team to increase fidelity to the model, as the MAT-PLUS intervention has a flexible rather than manualized approach in order to accommodate the needs of the participants. A more thorough description of the intervention is available in the parent study. 9 All procedures for the parent RCT and the current study were approved by an Instiutional Review Board (IRB), and all participants gave written consent to participate.
The current study analyzed a subset of participants from the MAT-PLUS pilot RCT who were randomized to the MAT-PLUS intervention, had a TSO, and received their first dose of XR-NTX (n = 12). This study analyzed only this subsample because participants in the TAU condition did not receive the MAT-PLUS intervention components relevant to the current research question. The primary outcome was the receipt of the next XR-NTX dose during the 16-week intervention period and was measured using data from participant health records. Predictor variables were: (1) days of “Team contact Participant” (any phone/text/email/brief contact with the participant that was not considered a therapy session); (2) days of “Participant contact Team”; (3) days of “Team contact TSO”; (4) days of “TSO contact Team”; (5) days of “Individual sessions” (in-person or telehealth between participant and study therapist); (6) days of “Family sessions” (in-person or telehealth between the participant, TSO, and study therapist). TSO consent to participating in at least 3 family sessions (target 60 minutes with flexibility, in-person/telehealth) during the course of the study that focus on addiction education, goal setting, and progress debriefing to promote adherence to treatment. All contacts and therapy sessions were tracked by the study team using a daily log, coding each type of contact dichotomously for each day. Logs were completed by research assistants and study therapists.
To calculate the impact of these 6 predictor variables on the likelihood of receiving the next XR-NTX dose, we used a time-varying approach in which the days of contact occurring between XR-NTX doses were totaled and entered as a predictor into 6 logistic regression models using R and RStudio.10,11 This way, each dose of XR-NTX received during the study was tied to the number of contacts or sessions during a specific time period that occurred before the dose was received. If a subsequent XR-NTX dose was not received, the recommended time between doses, 28 days, was chosen as the time period for days of contact. This approach splits each participant into multiple time intervals, leading us to a sample of n = 37 participant time periods. Independence was assumed, meaning that SEs could have been underestimated and significance could have been overestimated.
Results
The mean age of the analyzable participant sample (n = 12) was 36 years. 83% of the population self-identified as male, 50% self-reported as Black, 33% as White, and 17% as Hispanic. Half of the sample had AUD but not OUD, 42% had OUD but not AUD, and 1 person had both AUD and OUD (Table 1). Participants received M = 3.58 (SD = 1.51) out of a total of 5 expected XR-NTX doses during the study. The number of days between doses was M = 28.35 (SD = 2.99). Between each dose, the number of days on which the team contacted the participant was M = 8.08 (SD = 4), participant contacted the team was M = 5.19 (SD = 3), team contacted the TSO was M = 3.32 (SD = 2.76), and the TSO contacted the team was M = 2.11 (SD = 1.74). Participants had M = 1.89 (SD = 1.43) individual sessions and M = 0.81 (SD = 0.52) family sessions between doses.
Participant Characteristics.
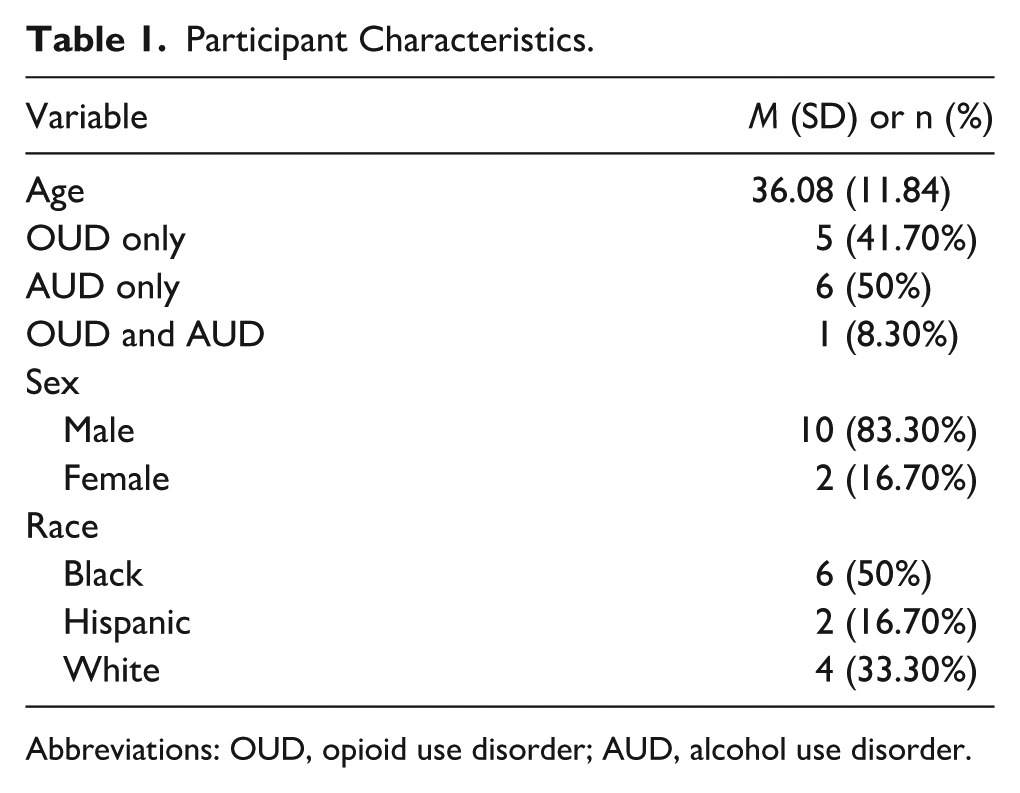
Abbreviations: OUD, opioid use disorder; AUD, alcohol use disorder.
Results of the logistic regressions revealed that, of the 6 contact types, only family sessions (OR = 8.74, 95% CI [1.84, 54.41]) were positively associated with receiving the next XR-NTX dose. There were no significant associations between the number of days of team, participant, or TSO contacts or individual sessions on XR-NTX dose receipt (team contact participant OR = 1.04, 95% CI [0.86, 1.27]; participant contact team OR = 1.21, 95% CI [0.93, 1.70]; team contact TSO OR = 0.93, 95% CI [0.69, 1.24], TSO contact team OR = 1.14, 95% CI [0.74, 1.85], individual session OR = 1.52, 95% CI [0.88, 2.89]) (Figure 1).
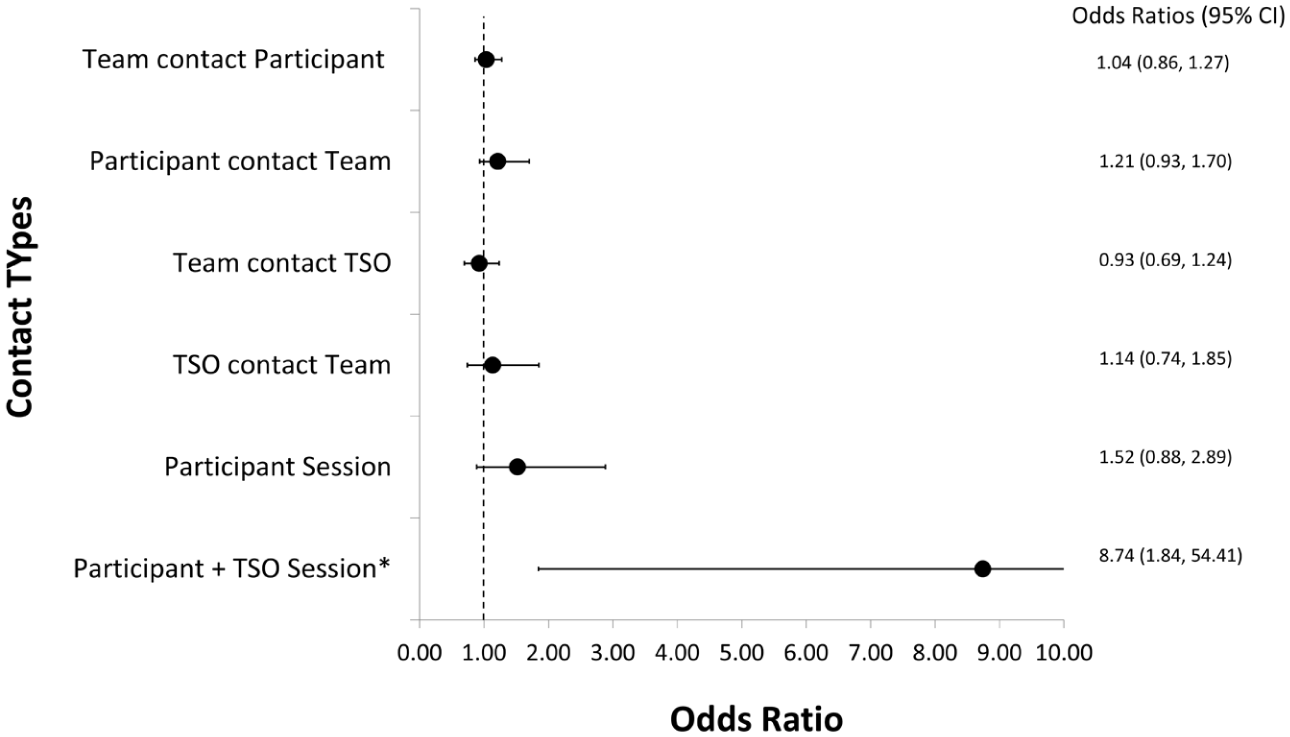
Odds of next XR-NTX dose receipt by contact type.
Discussion
This study adds to the existing evidence that involving family and other TSOs is associated with positive SUD treatment outcomes. Our hypothesis was supported: greater TSO engagement increased the likelihood that the next XR-NTX dose was received. For each additional family session between XR-NTX doses, the odds of receiving a subsequent XR-NTX dose increased nearly 9-fold. Prior literature is consistent with our findings, with many studies confirming that family involvement, family treatment, and couples therapy have positive effects on SUD treatment outcomes in general, despite their underutilization. 7 However, there has been less research on the impact of family involvement on medication adherence for SUD specifically, making the results of this study a novel contribution. These results emphasize the importance of implementing TSO involvement in AUD/OUD treatment plans.
In contrast, we failed to find significant relationships between quantitative measures of assertive outreach and other types of patient engagement indicators and subsequent XR-NTX injections, contrary to evidence in past literature.3,4,8 The null findings may be attributable to other components of the MAT-PLUS intervention masking the impact of assertive outreach, or other reasons such as small sample size. It could also be that our method of assessing engagement (i.e., days of contact) did not adequately capture the nuances of complex communication processes. For instance, “days of contact” does not take into consideration the context (e.g., which party initiated the contact) or the content of the contact (e.g., offering general support vs. addressing crises, scheduling an injection or session). Family session attendance may also have been more significant in predicting XR-NTX dose receipt than TSO contacts because the sessions are more involved than communication through a text or call, so family session attendance could demonstrate more motivation from the TSOs to engage than phone contacts.
Although these results are promising, this study was limited by a small sample size over a relatively limited duration. These findings regarding the impact of family sessions are preliminary in nature due to the small sample and wide CI, and have risks of Type II error, selection bias as only XR-NTX who also have TSOs are included in the study, and unmeasured confounding factors such as participant motivation influencing session attendance and adherence. Additional research is needed to confirm our findings that family sessions are associated with improved XR-NTX and other medication adherence. Our future research priorities include improving assertive outreach and family engagement metrics, such as investigating the role of contact context and content. Finally, a future study could use a randomized factorial trial design to better estimate the specific impact of the MAT-PLUS intervention components and their potential synergistic effect.
Conclusions
This study found that increased involvement from TSOs in the form of family session attendance increased the likelihood that the participant would receive their next dose of XR-NTX. The positive role that TSOs play in substance use treatment success emphasizes the need to incorporate them more frequently in treatment.
Footnotes
Acknowledgements
The authors would like to thank the other individuals who contributed to this project including study therapists Luciana Lavorato, LCPC, MA and Kamala Mallik-Kane, LCPC, MA, MPH as well as research assistants Jared Wildberger, MS and Jennifer Stidham, MS. The authors would also like to sincerely thank the individuals who participated in this study.
Ethical Considerations
This study was conducted according to the World Medical Association Declaration of Helsinki. This study was approved by the Johns Hopkins University Institutional Review Board (IRB00177313) on January 13, 2022.
Consent to Participate
All participants provided written informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Alkermes, Inc. (Dublin, Ireland) through the Investigator-Sponsored-Studies grant award program to author Fishman (FIS-IIT-208). Alkermes, Inc. was not involved in the study design, data collection, analysis, interpretation of the data, or decision to submit the article for publication.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marc Fishman received grant funding from Alkermes, the manufacturer of extended-release naltrexone, for this study. The authors alone are responsible for the content and writing of this paper.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request.