
Abstract
Background:
Cardiovascular side effects are commonly reported by men who use anabolic-androgenic steroids (AAS), yet little is known about the factors that increase risk. This study examines data from the 2024 Global Drug Survey (GDS2024) to identify whether route of administration (ROA), image-and performance enhancing drug (IPED) polypharmacy and licit substance use are associated with self-reported cardiovascular-related concerns.
Methods:
The dataset comprised 1167 males (≥16 years) who had used AAS within the previous 12 months. Descriptive statistics summarized demographic and substance use characteristics. Chi-square tests explored associations between self-reported cardiovascular side effects and ROA (oral vs injectable), IPED polypharmacy, and licit substance use respectively. Independent predictors were identified through multivariable binary logistic regression. Associations between substances were investigated using pairwise models. Visualizations included heatmaps, bar charts, forest plots, trend stability, and performance comparisons across models.
Results:
Showed that, among AAS consumers, 35.7% reported a self-reported cardiovascular-related concern. Alcohol (79.4%), tobacco (42.0%), and E-cigarette use (40.5%) were prevalent among AAS consumers. Clenbuterol use differed significantly by ROA, reported by 28.4% of oral and 24.3% of injectable AAS consumers. Injectable AAS use was strongly associated with concurrent human hormone growth (HGH) and insulin use. In adjusted models, injectable AAS use showed the strongest association with self-reported cardiovascular-related concerns (OR = 10.57, P < .001), followed by oral AAS use (OR = 1.92, P < .001) and clenbuterol use (OR = 1.44, P = .044). Age, HGH, insulin, alcohol, tobacco, and e-cigarette use were not significantly associated with cardiovascular-related concerns. Pairwise analyses indicated that clenbuterol-containing substance combinations were associated with higher odds of reporting cardiovascular-related concerns, highlighting the relevance of ROA and patterns of concurrent substance use.
Conclusions:
Negative cardiovascular health concerns among AAS consumers are most strongly associated with oral routes and use of substances like clenbuterol.
Keywords
Highlights
Cardiovascular-related concerns were common among AAS consumers.
Route of administration influenced cardiovascular risk profiles.
Clenbuterol-containing drug combinations showed elevated risk.
Introduction
Use of anabolic-androgenic steroids (AAS) has expanded over recent years from competitive sports to recreational fitness environments across the world. 1 Although AAS were originally developed for clinical applications (eg, treatment of hypogonadism),2,3 they are now used to improve their physique and performance. 4 This “off-label” use typically involves supraphysiological dosages of AAS and conjoint use of other image-and performance-enhancing drugs (IPEDs; eg, human growth hormone).5,6 Prevalence rates worldwide are around 3%, with markedly higher use in males,7,8 and initiation of use typically occurs before the age of 30. 9 AAS use has been associated with a wide range of adverse psychosocial concerns, including aggression, mood destabilization, and schizophrenia-related disorders,10,11 alongside significant physical harms such as endocrine disruption, gynecomastia, and cardiovascular dysfunction.12,13 These adverse outcomes warrant further investigation.
Cardiovascular complications are among the most frequently reported and clinically important concerns associated with AAS exposure.14,15 Cardiology-focused studies have demonstrated associations between AAS exposure and left ventricular dysfunction, reduced ejection fraction, impaired systolic function, and myocardial structural changes.16,17 Other alterations that have been reported include things such as elevated blood pressure, increased heart rate, maladaptive lipid profiles, left ventricular wall thickening, inflammatory activation response, and continuing atrial remodeling.18,19 These abnormalities contribute to heightened risks of arrhythmias, cardiomyopathy, and sudden cardiac death.15,20 Long-term AAS exposure is associated with elevated risks of cardiovascular-related risks, 21 with most documented cases presenting with left ventricular dilation and reduced ejection fraction. 15 Despite growing awareness of physiological risks, little is known about which patterns of AAS use and co-substance involvement place the greatest burden on the cardiovascular-related concerns.
A notable yet currently underexplored aspect of AAS use is route of administration (ROA), most commonly oral or injectable. 22 Oral AAS are commonly used during initial exposure because they are convenient and have a rapid onset of action, but they also offer more hepatotoxic effects, profound hormonal changes and an impact on lipid metabolism.23,24 Severe hepatic complications, such as cholestasis, peliosis hepatis, and hepatocellular carcinoma, along with neuropsychiatric effects like mood instability and libido dysregulation have been reported with oral use.25-28 In contrast, long entered injectable AAS have greater half-lives and bioavailability and more uniform pharmacokinetics with less hepatic compromise,23,29 but also result in gonadotropin suppression, hypogonadism, erectile dysfunction, atherogenic lipid profiles, abnormal diastolic blood pressure and an increased risk of cardiovascular disease.29-33 Though injectable formulations may have a more favorable hepatic profile,30,31 their long-term use is linked to adverse cardiometabolic and neuroendocrine outcomes.33-35
People who consume AAS frequently engage in polypharmacy, combining AAS with substances such as HGH, insulin, amphetamines, and clenbuterol to potentiate anabolic effects, accelerate fat loss, or counteract perceived adverse consequences of AAS use. 6 These combinations substantially elevate cardiovascular risk markers.36,37 Insulin doping, for example, has been associated with reduced HDL-cholesterol, elevated liver transaminases, and disruptions in fatty acid metabolism, 38 while clenbuterol, despite limited evidence suggesting improved glucose disposal, 39 is strongly linked to severe cardiovascular complications, 40 including supraventricular tachycardia, atrial fibrillation, and potential myocardial injury among athletes and IPEDs consumers.39,40 HGH use further contributes to cardiovascular vulnerability; although short-term recombinant growth hormone (GH) may transiently improve endothelial markers, its broader cardiovascular effects remain uncertain and potentially harmful.41,42 Such polypharmacy complicates causal attribution, as co-used substances may mask, mimic, or exacerbate AAS-related cardiovascular risk markers.14,18,37,43
In addition to IPED polypharmacy, many AAS consumers also use licit substances including alcohol, cigarettes, and tobacco, which independently increase cardiovascular risk. 44 Even minimal tobacco and cigarette exposure are associated with markedly elevated cardiovascular risk.45-47 E-cigarette use impairs endothelial function and elevates long-term coronary risk, 47 while tobacco consumption broadly contributes to hypertension and adverse lipid profiles. 48 Alcohol further influences cardiovascular risk in a dose- and pattern-dependent approaches, with heavy use contributing to cardiovascular failure risk despite some favorable changes seen with moderate intake.49,50 The evidence indicates that the use of AAS, polypharmacy, and licit substance usage may exert a significant cardiovascular risk,14,15,36,51-53 but there is a significant lack of concrete evidence on how polypharmacy among AAS consumers affects cardiovascular health, highlighting a crucial gap in current scientific research. 54
Despite substantial evidence for individual substance risk, limited research has comprehensively evaluated how AAS-based co-substance (polypharmacy, licit) use affects IPED consumers’ cardiovascular trajectories. 55 Most existing studies rely on small clinical samples, focus on single compounds, or do not account for the complexity of polypharmacy and co-substance use, 19 and no large, international dataset has systematically examined how demographic characteristics and patterns of IPED polypharmacy, ROA, and licit substance use patterns are associated with self-reported cardiovascular-related concerns. Given these gaps, this research aimed to (i) describe consumer characteristics and patterns of ROA and co-substance use; (ii) examine how substance use patterns, ROA, and age are associated with self-reported negative cardiovascular-related concerns, including the relative contribution of individual substances and their combinations.
Methods
Sample and Procedure
The study employed a cross-sectional design, using data from the 2024 Global Drug Survey (GDS2024), an international, large, online survey aimed at describing global patterns of drug use. The self-report survey is anonymous and provided on-line and distributed throughout the world across a variety of recruitment efforts including mainstream media (eg, The Sydney Morning Herald), social media (eg, X [formerly Twitter], YouTube), as well as partnerships with online content creators and influencers (eg, Vigorous Steve) who promoted participation in the survey.
Comprehensive sociodemographic data, substance use behaviors and related health information were obtained through the questionnaire. Anatomical specifics differentiated between AAS and corticosteroids to reduce the risk of misclassification. The full questionnaire collects detailed information on substance use behaviors, patterns and consequences.
The GDS2024 was available from January 10 to April 30, 2024, and completion time varied from about 15 to 60 minutes depending on participants’ substance use profiles. Documentation of survey development, recruitment process and validation procedures had been described in many previous publications.56,57 Ethical approval was obtained from The University of Queensland’s Human Research Ethics Committee (2023/HE001927). Individuals were eligible to participate if they were male, aged 16 years or older and had used AAS within the past 12 months. The survey was completely anonymous; no names, IP addresses, dates of birth, or other identifying details were collected. Reporting follows the STROBE guidelines for observational research.
Measures
The present study utilized demographic information related to age, gender, country of residence, ethnicity, and highest education. Further, questions were asked about participants’ AAS usage, including whether they have used AAS within the past 12 months, and ROA (eg, injectable, oral). In addition, the questionnaire assessed IPED polypharmacy, and licit polysubstance use, capturing participants’ use of alcohol, tobacco, E-cigarette, HGH, insulin, and clenbuterol.
The GDS employs a structured, self-completed questionnaire, and its validity and reliability for assessing substance use behaviors and related concerns have been demonstrated in multiple peer-reviewed publications.56-58 The survey also collected data on self-reported physical concerns including perceived cardiovascular-related effects. Participants were asked about perceived cardiovascular-related concerns of AAS use, including items such as “physical concern: negative impact on the heart.” These were presented as binary (Yes/No) response items and have been presented comprehensively previously.59,60
Analysis
All analyses were conducted using RStudio (v2024.12.0), and Python (v3.12) was used for data visualization. Demographic factors and co-substance use patterns were summarized as means, standard deviations, or percentage using descriptive statistics. Chi-square (χ2) analyses were used to compare the differences across substances for substance-use patterns, and between involving co-substance comorbidities prevalence, enabling evaluation of statistically significant relationship between categorical data. Factors associated with self-reported negative cardiovascular-related concerns were explored using binary multivariable logistic regression. The first model was the null model (M0), which included only the intercept. In the complete adjusted model (M1), substance-use variables were presented simultaneously: oral AAS, injectable AAS, alcohol, tobacco, E-cigarette, HGH insulin, and clenbuterol, together with age. The fit of the model was assessed by AIC, BIC, and pseudo-R2. Odds ratios (OR) with 95% confidence intervals were calculated to determine the association of each factor with self-reported cardiovascular-related concerns.
To further explore associations between combinations of substances, pairwise logistic regression models were conducted. Each model evaluated the association between a specific substance and self-reported cardiovascular-related concerns while adjusting for concurrent use of other substances. This approach enabled the determination of a dominant effect-producing substance and revealed compound amplification of cardiovascular-related concerns with implications for common trends in IPED polypharmacy and licit polysubstance use. The model’s performance will be assessed and verified with the assessment metrics provided in the comparative performance plot, which includes area under the curve (AUC), accuracy, sensitivity, specificity, precision, F1-score, balanced accuracy, Kappa, positive predictive value (PPV), negative predictive value (NPV), and Brier score.
To visualize model results, we generated forest plots for odds ratios and confidence intervals, and heatmaps and bar charts to show the prevalence of cardiovascular-related concerns by age and substance. A trend stability plot assessed the robustness of predictor effects across model specifications. Model performance was compared using bar charts for 5 model variants.
Results
Descriptive Statistics
Demographic Characteristics
The study included 10 120 participants (Mage = 32.90 years, SD = 11.30) from 119 countries. From this cohort, our final analytic sample comprised 1167 male AAS/IPED consumers who had used AAS within the past 12 months, representing respondents from 69 countries (Mage = 31.44 years, SD = 9.89). The majority of participants self-identified as White (n = 918, 78.4%), followed by Hispanic/Latinx (n = 82, 7%). Education levels were generally high, and over 22.1% reported college certificate/diploma qualifications (Table 1).
Demographic Characteristics of Male AAS Consumers (N = 1167).
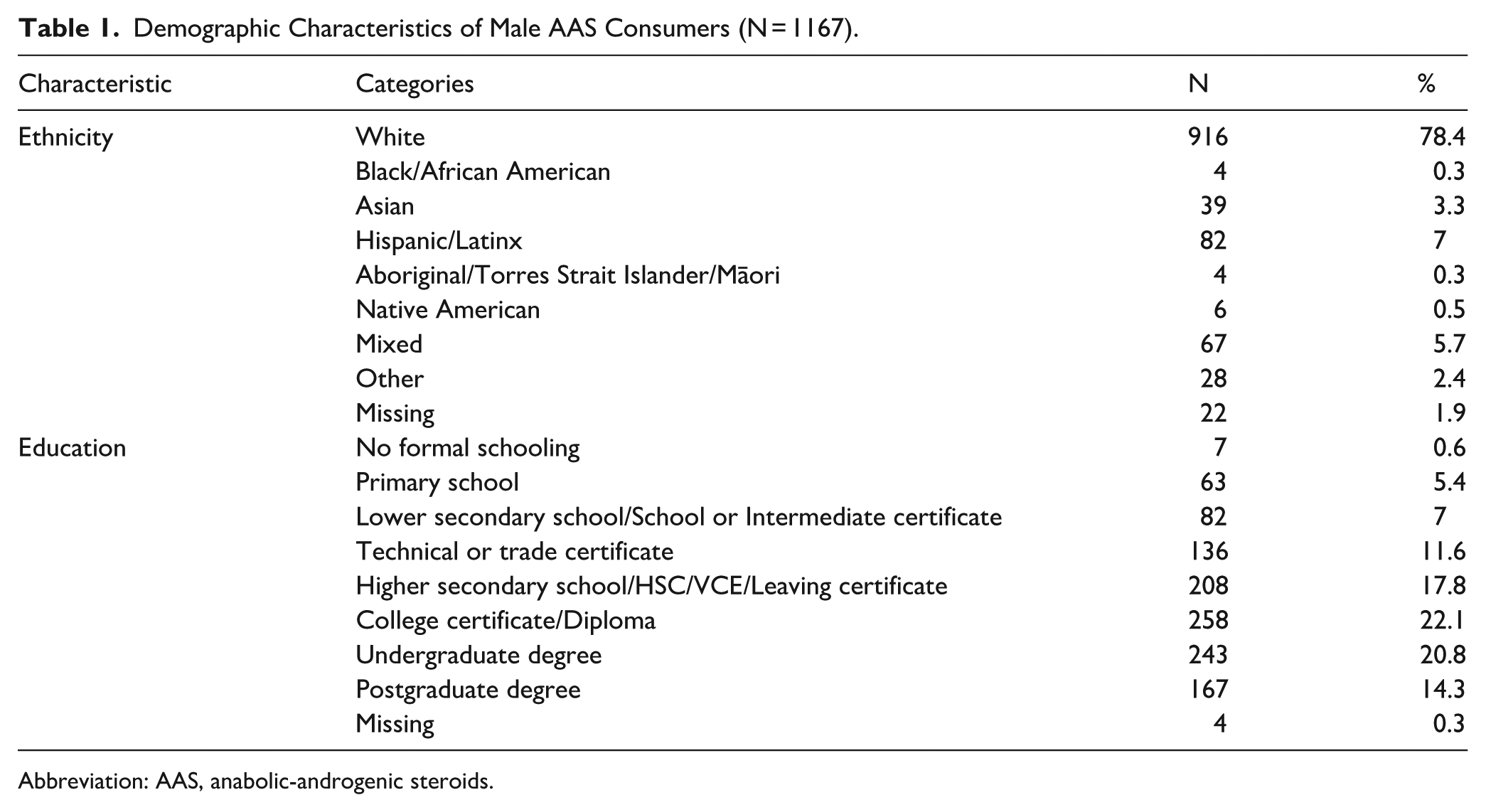
Abbreviation: AAS, anabolic-androgenic steroids.
IPED Polypharmacy and Licit Polysubstance Use Patterns
To explore the co-occurrence of AAS use with co-substance use and self-reported cardiovascular-related concerns, associations between ROA and different forms of co-substance use were evaluated (see Table 2). Substance use was common in the sample, and alcohol, tobacco, and E-cigarette consumption were commonly reported. Significant associations were found between both oral (Alcohol: χ2(1) = 5.88, P = .015; Tobacco: χ2(1) = 4.70, P = .032) and injectable AAS consumers (Alcohol: χ2(1) = 5.48, P = .019; Tobacco: χ2(1) = 14.85, P < .001) in relation to these substances. Although E-cigarette use was significantly associated only with injectable use (χ2(1) = 9.31, P = .002), it was still commonly reported by oral consumers as well.
Prevalence of Co-Substance Use and Its Association with ROA among Past 12-Month AAS Consumers (N = 1167).
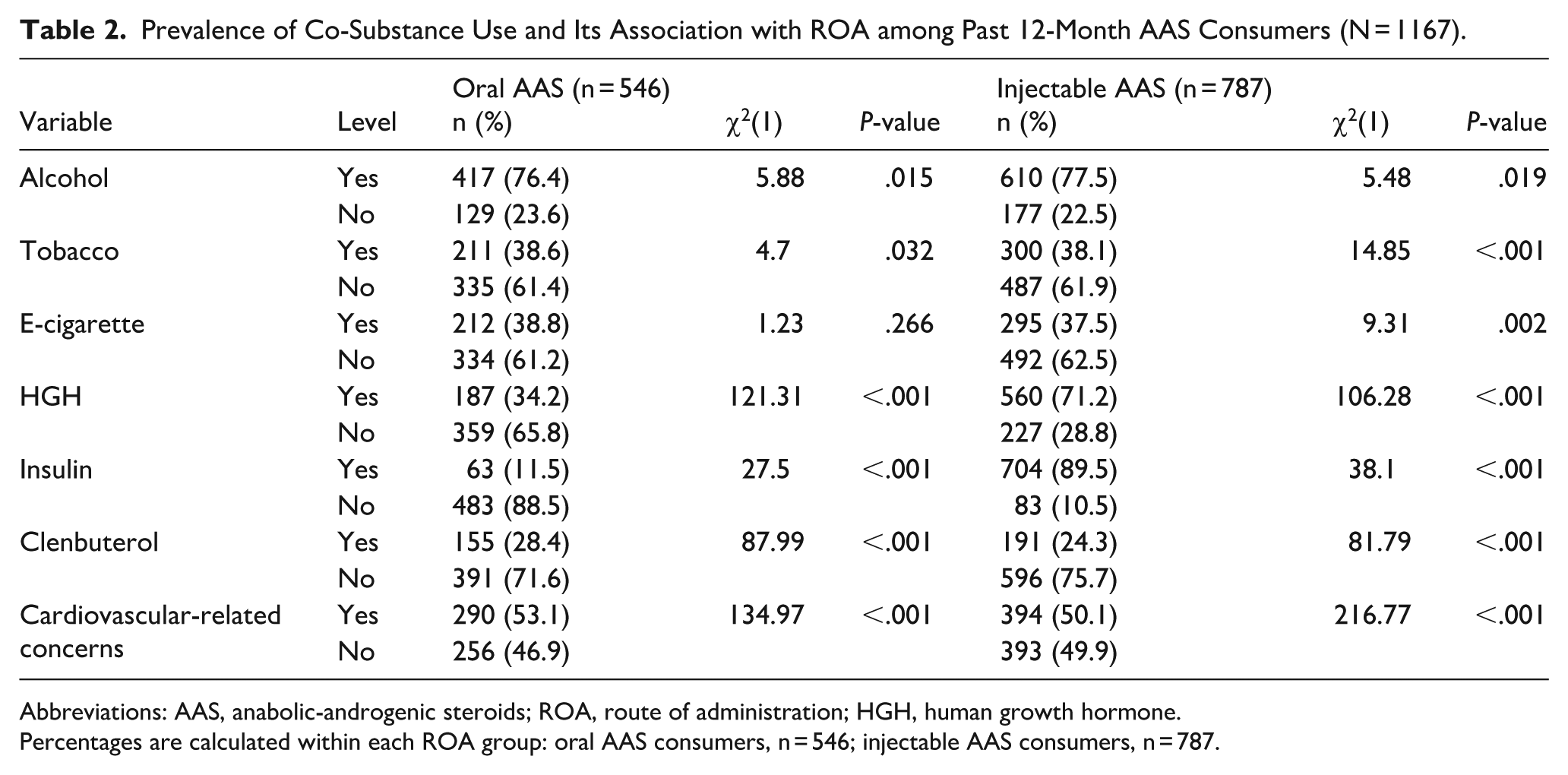
Abbreviations: AAS, anabolic-androgenic steroids; ROA, route of administration; HGH, human growth hormone.
Percentages are calculated within each ROA group: oral AAS consumers, n = 546; injectable AAS consumers, n = 787.
Use of HGH and insulin was substantially higher among injectable AAS consumers, with large and highly significant associations observed (HGH: χ2(1) = 106.28, P < .001; insulin: χ2(1) = 38.10, P < .001). Clenbuterol use was also significantly associated with both oral AAS use (χ2(1) = 87.99, P < .001) and injectable AAS use (χ2(1) = 81.79, P < .001) and was reported by 28.4% of oral AAS consumers and 24.3% of injectable AAS consumers.
Finally, there was a strong and statistically significant association between self-reported cardiovascular-related concerns with both oral (χ2(1) = 134.97, P < .001) and injectable (χ2(1) = 216.77, P < .001) AAS use.
IPED Polypharmacy, Licit Polysubstance Use, Age Patterns in Cardiovascular-Related Concerns
To characterize differences in cardiovascular-related concerns by substance type and age group, a multidimensional visualization integrating prevalence data, age-stratified heatmaps, and group-level patterns were developed (see Figure 1). There was considerable variation in cardiovascular-related concerns depending on the type of exposure. Pharmacological substances, such as injectable AAS, oral AAS, HGH, insulin, and clenbuterol, showed significantly higher reported rates of negative cardiovascular-related concerns, all consistently exceeding 50%. By contrast, licit substances (ie, E-cigarette, tobacco, and alcohol) were associated with much lower negative cardiovascular-related concerns, generally between 30% and 38%. This reflects a clear absolute risk gap, with polypharmacy showing negative cardiovascular-related concerns that are roughly 15% to 25% higher than licit substances.
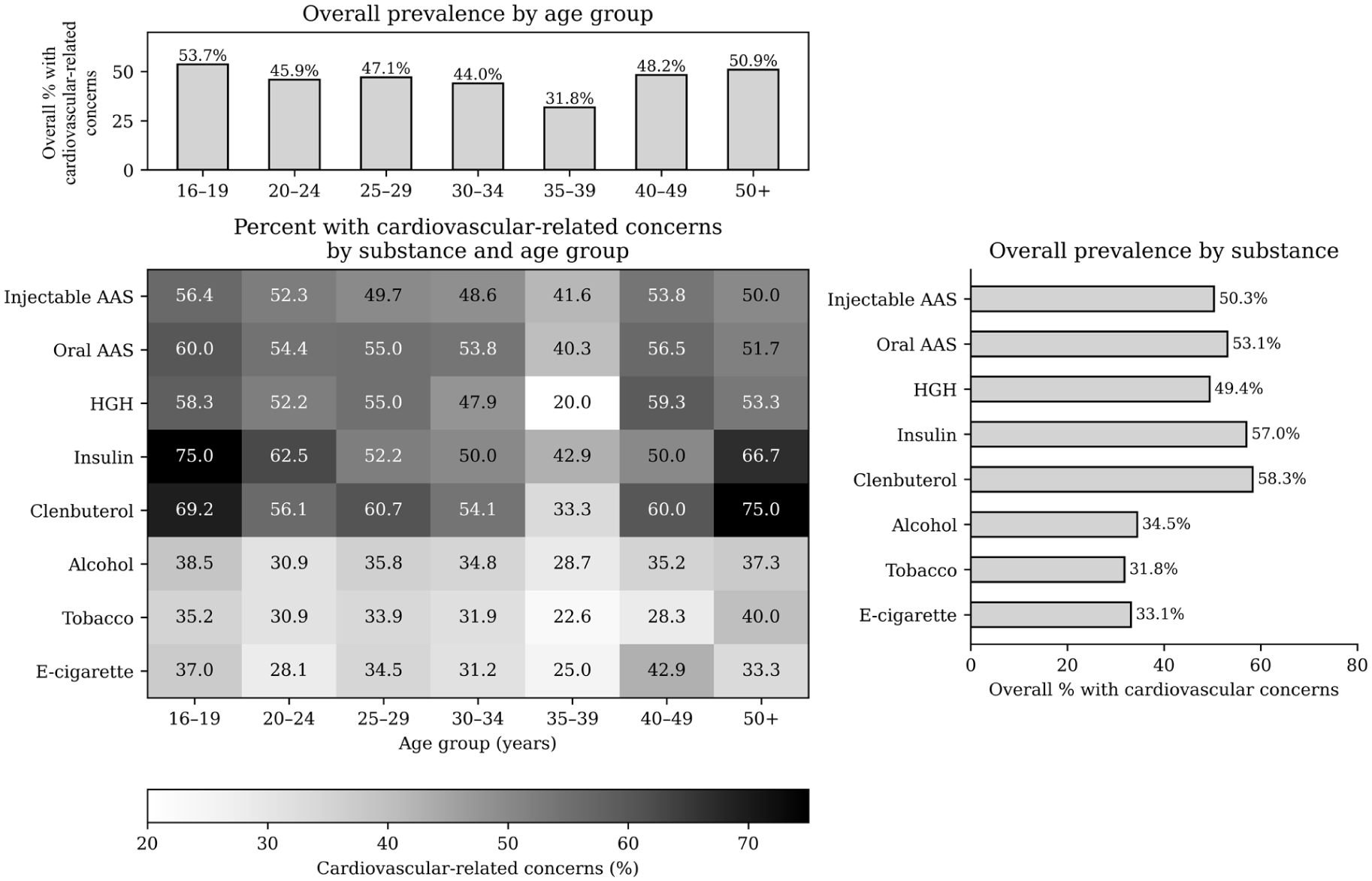
Prevalence of negative cardiovascular-related concerns across substance use, and age groups.
The age-stratified heatmap further uncovers key statistical patterns. Young adults (ages 16-24 years) exhibited some of the highest levels of self-reported cardiovascular-related concerns, particularly for injectable AAS, insulin, and clenbuterol, with prevalence exceeding 60% and approaching 70% to 75% for insulin and clenbuterol. The most striking example was insulin use in the 16 to 19 age group, where cardiovascular-related concerns peaked at 75%, a significant outlier compared to other age groups. In contrast, people aged 35 to 39 consistently had the lowest negative cardiovascular-related concerns, forming a distinct low point on the age-distribution curve. However, E-cigarette use, and to a lesser extent clenbuterol, showed limited age-related variability in the prevalence of self-reported negative cardiac impact (approximately 28%-43%), whereas tobacco and alcohol use exhibited greater age-dependent variation, with prevalence decreasing to around 23% to 29% in mid-adulthood and increasing again to approximately 37% to 40% in older age groups.
These patterns are further confirmed by the age-group summary plot, which shows that the youngest (16-19 years) and oldest (50+ years) consumers have the highest overall rates of negative cardiovascular-related concerns, at 46.1% and 47.1%, respectively. This supports the presence of a meaningful bimodal trend, with middle-aged adults (especially those aged 35-39, at 32%) forming a contrasting low point.
IPED Polypharmacy, Licit Polysubstance Use, Qualification Patterns in Cardiovascular-Related Concerns
A multidimensional visualization characterizing cross-classification of cardiovascular-related concerns by substance type and qualification was developed (see Figure 2), integrating prevalence data, qualification-stratified heatmaps, and group-level patterns. Substance exposure type was associated with very different cardiovascular concerns. Reported rates of cardiovascular-related concerns associated with the use of pharmacological substances (ie, injectable AAS, oral AAS, HGH, insulin and clenbuterol) were consistently high overall and generally over 50% per qualification level. On the contrary, the usage of licit substances (ie, alcohol, tobacco and E-cigarettes) was associated with lower prevalence compared to illicit substances through various studies ranging from an estimate of just over 30% to around 48%. The implication is a large absolute difference in cardiovascular concerns visibility or experience between IPED use and licit substance use (older pharmacological substances showed around 10%-25% elevated rates overall).
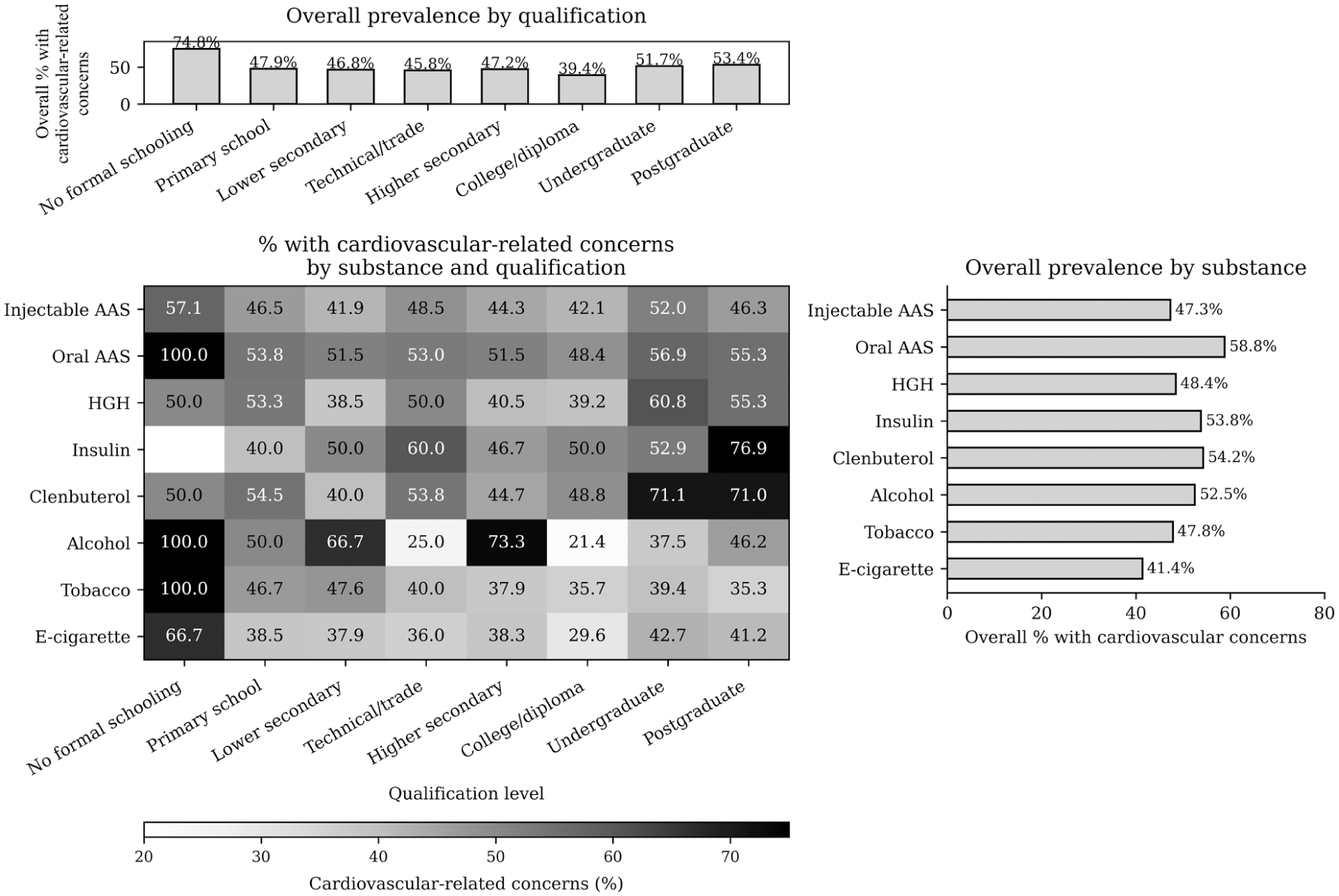
Prevalence of negative cardiovascular-related concerns across substance use and qualification.
The qualification-stratified heatmap further illustrates clear qualification levels in cardiovascular-related concerns. No formal schooling level also had among the highest self-reported prevalence (oral AAS, alcohol and tobacco reached values of 100%), however, these represent subgroups with few individuals. Usage of insulin and clenbuterol was especially pronounced as a concern in subjects with higher degrees, with this prevalence reaching around 76.9% for postgraduate individuals and 71.0% to 71.1% in undergraduates. In contrast, AAS consumers with mid-level education (eg, technical/trade and college/diploma) generally exhibited more moderate and stable prevalence for most substances, indicating a potential attenuation of concerns in these groups. Licit substances were less variable across qualification levels, though alcohol and tobacco did show some variation with lower prevalence in higher secondary and college/diploma groups.
Overall, further patterns were supported by a summary plot of self-reported cardiovascular concerns by qualification level; those without formal schooling had the highest overall prevalence of self-reported cardiovascular morbidity (74.8%) and postgraduate students (53.4%) and undergraduates (51.7%). In contrast, the prevalence among college/diploma educated was very low (39.4%) and represented a clear minimum in the distribution. This indicates a non-linear association between qualification levels and cardiovascular-related concerns; with both the lowest as well as the highest levels associated with increased prevalence, while intermediate levels seem to convey relatively decreased concerns.
Associations of IPED Polypharmacy and Licit Substances on Cardiovascular-Related Concerns
A multivariable binary logistic regression analysis was conducted to examine the independent associations between IPED use, licit substances, and self-reported cardiovascular-related concerns among AAS consumers. The full model (M1), which included age, ROA, IPED polypharmacy, and licit substance use, significantly improved model fit compared to the null model (Δχ2 = 289.34, P < .001), explaining a moderate proportion of variance (McFadden R2 = 0.190; Nagelkerke R2 = 0.301).
After adjustment for all covariates, injectable AAS use emerged as the strongest predictor of cardiovascular-related concerns (OR = 10.57, 95% CI: 6.56-17.02, P < .001), indicating more than a tenfold increase in odds. Oral AAS use was also significantly associated with increased odds (OR = 1.92, 95% CI: 1.47-2.59, P < .001), while clenbuterol use showed a smaller but statistically significant association (OR = 1.44, 95% CI: 1.01-2.05, P = .044).
In contrast, age and other substances (HGH, insulin, alcohol, tobacco, and e-cigarette use) were not significantly associated with cardiovascular-related concerns after adjustment (all P > .05) (Figure 3a; Table 3).
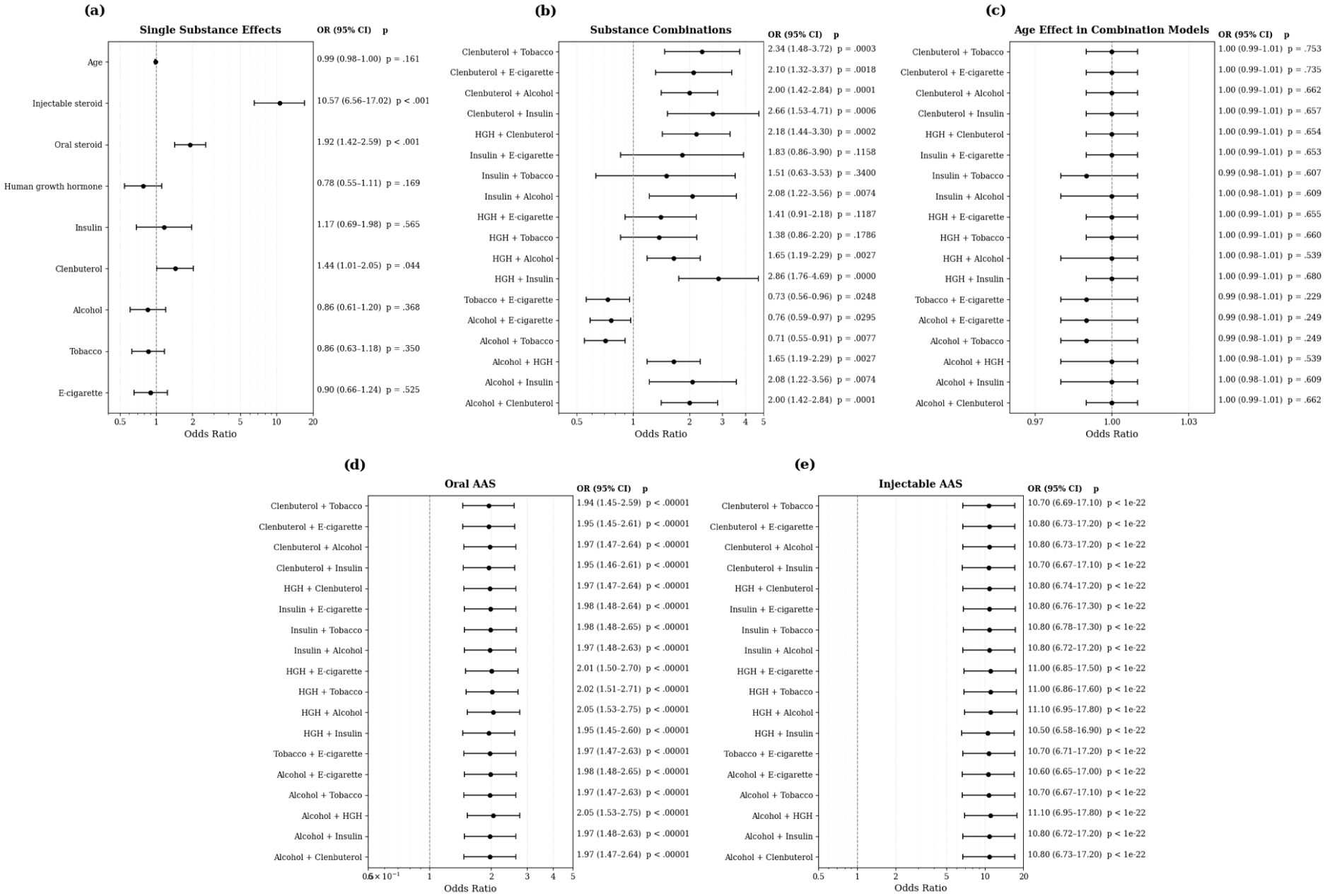
Odds ratios for negative cardiovascular-related concerns by substance and substance pairings: (a) single substance effects; (b) substance combinations; (c) age effect in combination models; (d) oral AAS; and (e) injectable AAS.
Multivariable Binary Logistic Regression Predicting Cardiovascular-Related Concerns Among AAS Consumers.
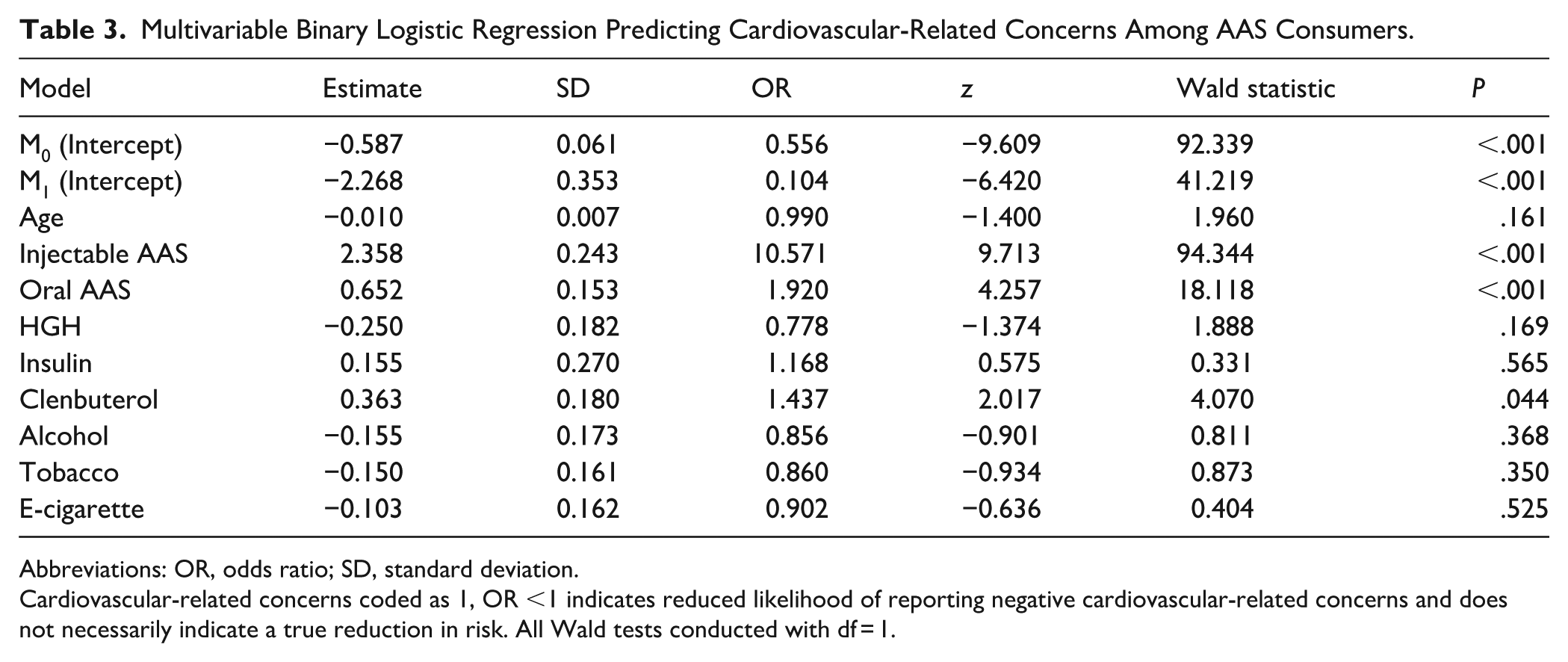
Abbreviations: OR, odds ratio; SD, standard deviation.
Cardiovascular-related concerns coded as 1, OR <1 indicates reduced likelihood of reporting negative cardiovascular-related concerns and does not necessarily indicate a true reduction in risk. All Wald tests conducted with df = 1.
To evaluate how different substance combinations relate to self-reported cardiovascular-related concerns, pairwise logistic regression models were used, assessing the effect of each substance while controlling for the concurrent use of another substance, age, and ROA.
In the pairwise combination models (see Figure 3b and Table S2), several two-substance combinations were associated with higher odds of reporting cardiovascular-related concerns. The highest odds ratios were observed for combinations involving clenbuterol and/or insulin, particularly clenbuterol + insulin (OR = 2.66, 95% CI = 1.53-4.71, P = .0006) and HGH + insulin (OR = 2.66, 95% CI = 1.76-4.69, P < .0001). Other clenbuterol-based pairs, such as clenbuterol + tobacco (OR = 2.34, 95% CI = 1.48-3.72, P = .0003), clenbuterol + E-cigarette (OR = 2.10, 95% CI = 1.32-3.37, P = .0018), and clenbuterol + alcohol (OR = 2.00, 95% CI = 1.42-2.84, P = .0001), also showed significantly elevated concerns, as did combinations such as insulin + alcohol (OR = 2.08, 95% CI = 1.22-3.56, P = .0074) and HGH + alcohol (OR = 1.65, 95% CI = 1.19-2.29, P = .0027). While some pairs of alcohol and tobacco substances (eg, tobacco + E-cigarette, alcohol + E-cigarette, or alcohol + tobacco) had odds ratios below 1.0 with P < .05, indicating a lower relative odds of reporting cardiovascular-related concerns within specific pairings. Age effects within the combination models were essentially null across all pairs (ORs = 1.00, 95% CIs = 0.99-1.01, all P > .20; see Figure 3c, Table S3), indicating that the excess concern associated with IPED polypharmacy patterns is largely age independent. When oral and injectable AAS effects were decomposed within the combination models (see Figure 3d and e, and Tables S4 and S5), oral AAS showed a stable, moderate elevation in concern across all combinations (ORs = 1.9-2.1, 95% CIs = 1.45-2.7, P < .00001), whereas injectable AAS consistently produced very large odds ratios of approximately 10 to 11 (95% CIs = 6.7-17.3, P < 10−22) irrespective of co-substance.
Model Performance and Predictive Validity
To evaluate the validity and predictive balance of the combination models illustrated in the forest plots, model performance was assessed across 11 evaluation metrics (see Figure 4 and Table S6). The base combination model demonstrated very high sensitivity (0.93), indicating strong ability to identify individuals reporting negative cardiovascular-related concerns; however, this was accompanied by low specificity (0.19), reduced discrimination (AUC = 0.61), and weaker calibration (Brier score = 0.21), reflecting a trade-off toward false-positive classification. Adding age to the combination model did not alter any performance metric, confirming that age contributes minimal predictive value and does not meaningfully modify substance-related cardiac concern.
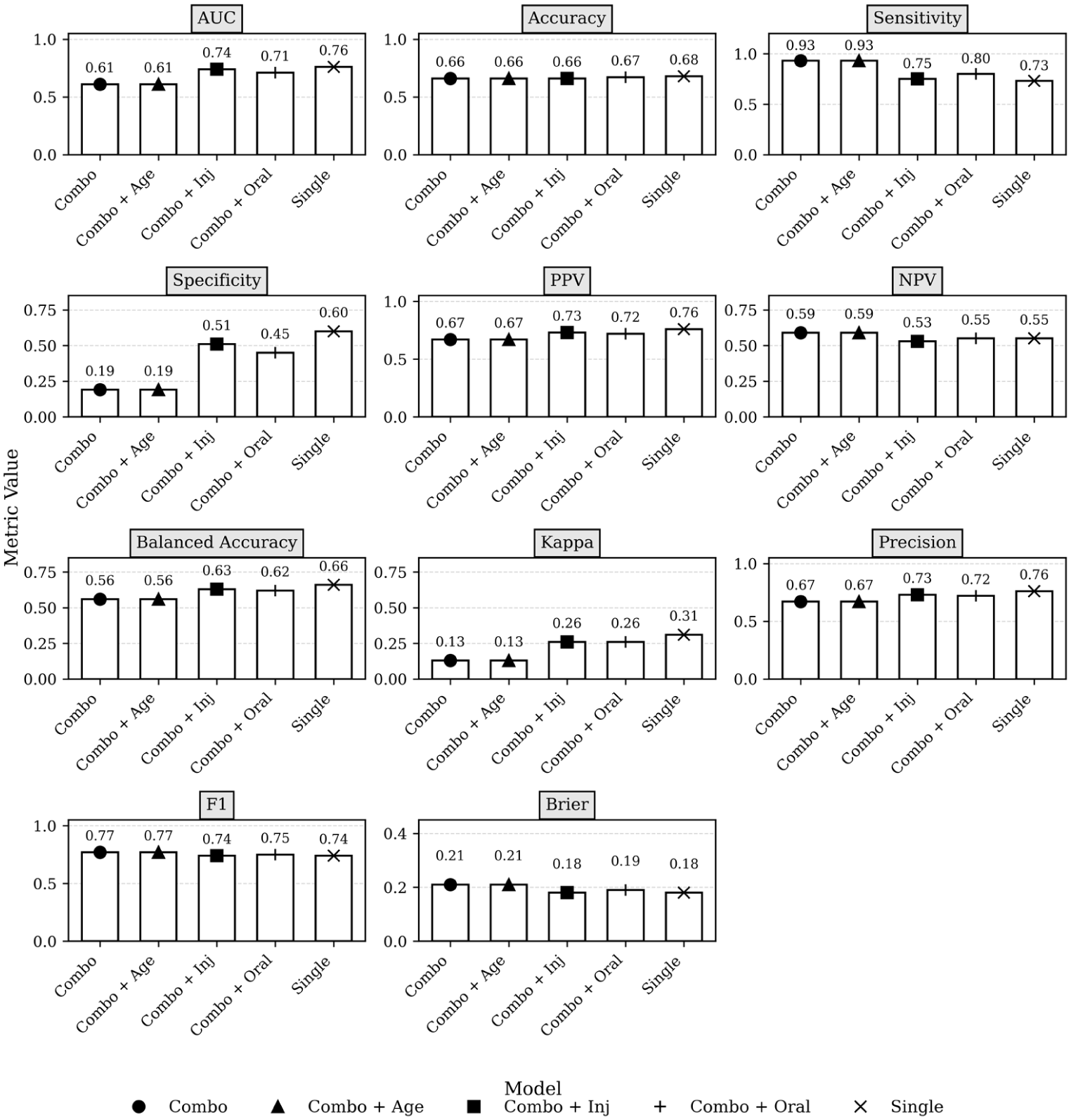
Comparison of 5 predictive models across 11 performance metrics.
In contrast, explicit inclusion of ROA substantially improved model performance. The Combo + Oral AAS model showed higher discrimination (AUC = 0.71), improved specificity (0.45), greater balanced accuracy (0.62), and stronger agreement (κ = 0.26), while maintaining acceptable sensitivity (0.80). Similarly, the Combo + Injectable AAS model further improved discrimination (AUC = 0.74), specificity (0.51), balanced accuracy (0.63), and calibration (Brier score = 0.18), approaching the performance of the single-substance model. Collectively, these findings indicate that while unadjusted combination models prioritize sensitivity, ROA, particularly injectable AAS, restores predictive balance and supports the robustness of the observed concern estimates, whereas age provides no meaningful enhancement to model validity.
Trend Stability and Spearman’s Rank Correlation (ρ) Analysis
The stability of trends was analyzed through leave-one-out models with Firth penalized logistic regression to confirm the robustness of multivariable logistic regression results. Spearman’s rank correlation coefficient (ρ) is a non-parametric measure which indicates the consistency between predictor OR patterns in different model settings. Spearman’s ρ assesses the concordance of the rank order and sign of OR estimates when model structure changes, as opposed to focusing on numeric equality. Low ρ values show high sensitivity of the model and higher values correspond to consistent correlations (without any covariates) (see Figure 5 and Table S7).
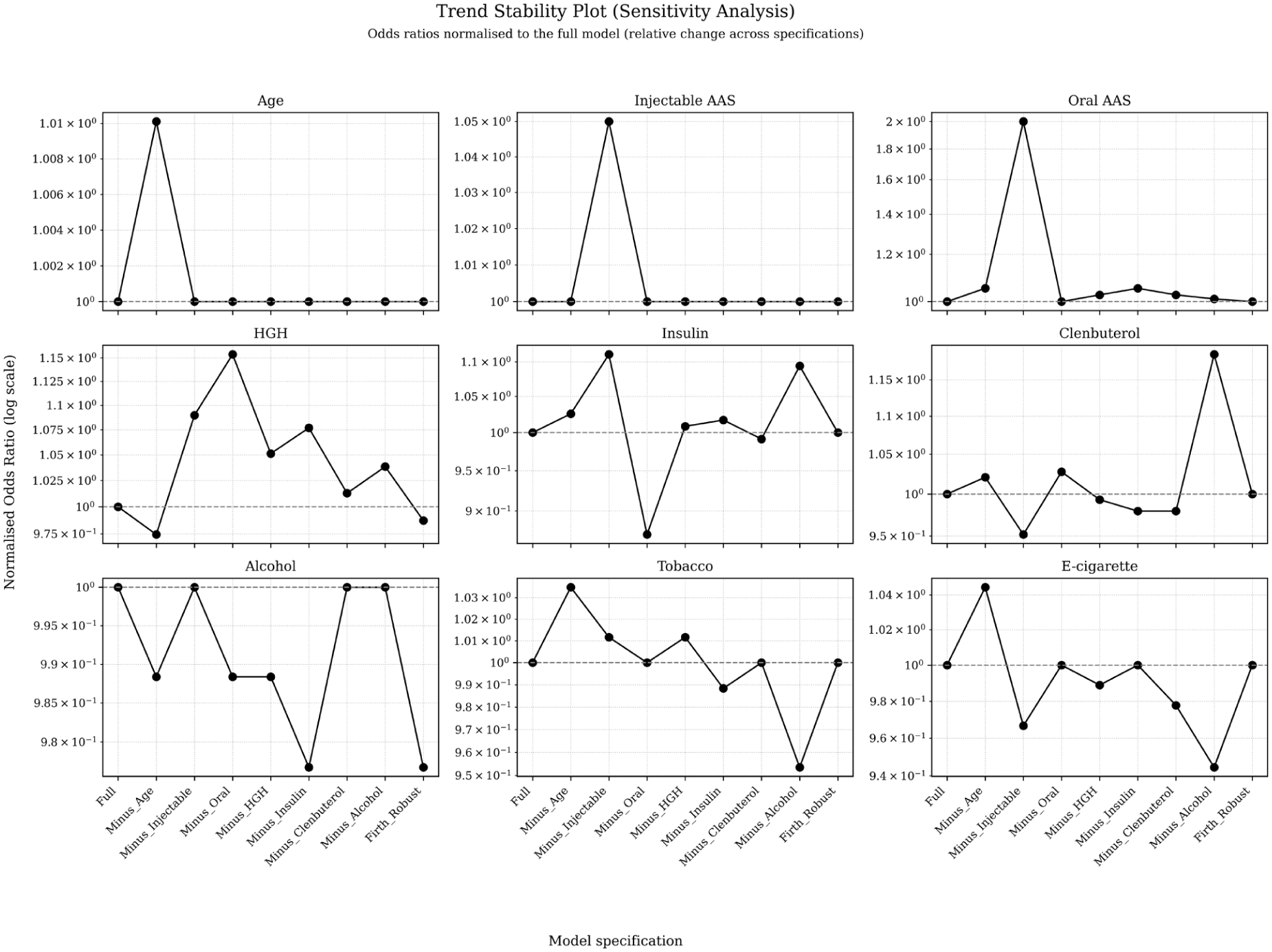
Trend stability of predictors across sensitivity models.
Trend stability for the use of injectable AAS was quasi-perfect in sensitivity analysis, exhibiting higher ORs under all 3 model options. The pattern has a high ρ, indicative of its strong cardiac association independent of the model. Maintained consistency of this effect suggests that it can be considered a strong and independent risk factor. The crest of the OR magnitude curve for oral AAS use also varied greatly when injectable AAS usage was omitted from the model; however, direction parameters were unchanged. If the ρ is high but not 1 (ie, ρ < 0.95), there could be some confounding or overlapping exposure patterns reflected by a lower but non-perfect ρ, not by relationship instability.
Clenbuterol positively correlated to all models with a high ρ value and a narrow range of OR values. Insulin was more variable, with ORs close to one in some of the models. The pattern shows moderate ρ and a context-dependent relationship. The OR estimates for HGH alcohol, tobacco, and E-cigarette use were around or <1 in all moderately heterogeneous models. Such significant but weak connections are indicated by the large ρ values. Age was not associated with OR in any of the models, suggesting very good temporal trend stability (although not a clinically relevant one). The Spearman’s ρ-based sensitivity analysis of trend stability shows that the main study findings, particularly the significant cross-link between injectable AAS consumers and cardiac concerns, are insensitive to model choice and sparse data bias.
Discussion
This study found that negative cardiovascular-related concerns among a large international sample of men who use AAS is driven primarily by injectable AAS, oral AAS, and clenbuterol, which were the only substances independently associated with negative cardiovascular-related concerns. Pairwise analysis showed that cardiovascular-related concerns in AAS consumers is driven predominantly by injectable AAS, with oral AAS and clenbuterol acting as additional independent contributors. Furthermore, certain IPED polypharmacy patterns, particularly combinations that include clenbuterol and/or insulin together with AAS, substantially amplify the likelihood of negative cardiovascular-related concerns. These findings indicate that negative cardiovascular-related concerns are shaped not only by individual substances but also by synergistic interactions between them.
Considering the prevalence of co-substance use, evidence showed consumers often combine multiple substances such as alcohol, tobacco, HGH, insulin, and clenbuterol,6,61 to enhance effects, combat side effects, or for recreational purposes. 6 This aligns with extensive evidence showing that AAS use rarely occurs in isolation; rather, individuals commonly engage in complex IPED polypharmacy with licit substances use.62-64 This reflects a distinct enhancement typology rather than recreational substance use alone. Within this context, cardiovascular concerns appear to be driven primarily by pharmacological burden and biological interaction, rather than by lifestyle behaviors.
Moreover, IPED polypharmacy frequently occurs alongside AAS use and is associated with greater self-reported cardiovascular-related concerns. Insulin use alone is associated with a 52% increase in cardiovascular risk,65,66 while HGH shows mixed profiles, improvements in lipid and blood pressure markers have been reported, 67 yet without consistent reductions in cardiovascular mortality. 68 Clenbuterol stands out as a particularly hazardous component of enhancement-oriented polypharmacy. Commonly combined with AAS during cutting phases to accelerate fat loss and improve muscular definition, 6 it carries well-documented cardiotoxic risks, including tachyarrhythmias and acute cardiovascular instability.40,59,69 Additional reports describe structural myocardial injury, supraventricular tachycardia, hypokalemia, and acute cardiac-electrolyte disturbances.70-72 These findings imply that AAS and frequently co-administered substances like insulin and clenbuterol exacerbate cardiovascular-related concerns among AAS consumers. The combined, or synergistic toxicities of these substances may underlie consumers’ polypharmacy-related additional cardiovascular-related concerns, underscoring the importance of examining combination versus single compound approaches to exposure analysis.
In contrast to enhancement-oriented polypharmacy, the role of licit substances such as alcohol, E-cigarettes, and tobacco warrants separate consideration. Although licit substance use was prevalent among AAS consumers in this sample, these substances were associated with increased cardiovascular-related concerns 73 ; however, their independent effects were attenuated after accounting for AAS/IPED use. This suggests that licit substances may contribute to cardiovascular-related concerns,47,74 their influence is likely secondary to the more salient effects of AAS use and enhancement-oriented polypharmacy. This finding should not be interpreted as indicating cardiovascular safety; but rather as reflecting differences in how risk is perceived and contextualized within this population. AAS consumers who engage in licit substance use may represent more recreational or socially oriented typologies, where substance use is associated with social interaction, stress relief, or lifestyle behaviors rather than targeted physiological enhancement. 75 As such, cardiovascular concerns in this group may be less directly attributed to substance use and more diffuse in nature.76,77
Perception-related factors may further explain these findings. Widespread public health messaging and media coverage regarding the harms of alcohol and tobacco may increase general awareness of cardiovascular risk,78,79 potentially elevating concern among AAS consumers. Conversely, familiarity with these substances and their normalization in social settings may reduce the perceived immediacy or severity of cardiovascular consequences compared to AAS or polypharmacy use. 6 In this context, cardiovascular-related concerns likely reflect a balance between awareness, personal experience, and perceived controllability of risk.
Regarding AAS use, the observed association with increased cardiovascular-related concerns may be interpreted considering existing knowledge regarding their potential adverse effects.15,53 While the present study does not assess clinical cardiovascular outcomes, prior evidence linking AAS exposure to adverse cardiac effects may contribute to heightened risk perception among consumers.21,51,52,80 Exposure to such information may shape consumers’ awareness and contribute to increased reporting of cardiovascular concerns. Additionally, personal experiences such as palpitations, fluctuations in blood pressure, or reduced exercise tolerance may further reinforce these perceptions.14,15,81
With regard to IPED polypharmacy and cardiac-related concerns, there remains a substantial gap in the literature on how combinations of AAS and co-administered substances shape cardiac concerns among AAS consumers. The concurrent use of multiple substances 82 may increase consumers’ awareness of potential additive or synergistic effects, particularly within communities where information sharing and experiential knowledge are common.13,14,83 In the absence of clear clinical evidence, this awareness may amplify concern, especially among individuals who have previously experienced adverse symptoms or are exposed to discussions emphasizing the risks of combining substances.
Implications
This study carries important clinical, public health, and policy implications. The findings indicate that AAS use is associated with greater self-reported cardiovascular-related concerns, highlighting the importance of routine screening for AAS use in clinical settings and careful consideration of cardiovascular health. Prevention and harm reduction must work in tandem. While cessation should remain a prevention goal, abrupt discontinuation is rarely feasible for consumers; structured cessation and recovery approaches, including appropriate post-cycle therapy, are necessary to reduce withdrawal-related and endocrine risks. 84
From a harm reduction perspective, accessible and routine cardiovascular monitoring is essential. Simple measures such as regular blood pressure and heart rate checks provide quick, low-cost indicators of strain, while echocardiography offers a more precise tool to detect left ventricular hypertrophy and other early signs of cardiac remodeling. Importantly, presenting consumers with objective clinical data can prompt meaningful behavior change, consistent with evidence from other biometric-informed interventions.85, 86
Intervention approaches may differ by level of perceived concern: individuals with low concern may require targeted education to improve concern awareness, whereas those with higher concern may benefit from structured clinical engagement, including monitoring and reassurance.
At a population level, these results highlight the need for targeted education and health promotion that clearly communicates the potential cardiac concerns of AAS and polypharmacy. Improving access to knowledgeable healthcare providers, reducing stigma, and supporting early diagnostic pathways can help prevent serious cardiovascular events. Further research using standardized, reliable measures of AAS and IPED polypharmacy and polysubstance use, alongside prospective monitoring of cardiac concerns, is needed to strengthen the evidence base and inform effective interventions.
Limitations
The present study is not without its limitations, which should be considered when interpreting these findings. Recall bias, underreporting and response error may have arisen because of relying on self-reports. Additionally, self-reported cardiovascular-related concerns may be influenced by cognitive bias (eg, the Dunning-Kruger effect), leading to underestimation due to poor insight or overestimation with greater awareness. Thus, reported concerns may reflect differences in perception and health literacy rather than true cardiovascular status. 87 Similarly, while there were observed correlations between substance use and cardiac measures, the cross-sectional nature of this study precludes inferences about temporal ordering or cause-effect relationships. In addition, the outcome measure does not constitute a validated clinical assessment of cardiac health, is based on subjective perceptions, and does not identify specific cardiac conditions; therefore, validation by healthcare professionals is recommended. Information on dosage, duration and patterns of use, stacking practices, and prescription status was not available; these factors are likely to moderate risk and warrant dedicated modeling in future research. Despite the international scope of this study, country-level regulatory, healthcare, and cultural factors that may influence substance-use patterns and risk perception were not fully addressed. Finally, the recruitment process may have over-represented digitally connected individuals while under-sampling those who are more marginalized or disengaged from health services.
Conclusion
This international study highlights that negative cardiovascular-related concerns among AAS consumers is mainly influenced by ROA as well as IPED polypharmacy (eg, clenbuterol), rather than by licit substances (eg, alcohol). Injectable AAS, oral AAS, and clenbuterol each independently contribute to negative cardiovascular-related concerns, with injectable AAS showing by far the most pronounced effect. Clenbuterol has a substantial independent effect and it increases concern when combined with other substances. These results offer that cardiovascular-related concerns are associated with not only isolated substances (particularly injectable AAS), but also their interactions in IPED polypharmacy, ROA, and licit substance. These findings highlight the necessity of rising awareness regarding cardiac concerns linked to injectable AAS polypharmacy, especially concerning high-risk substances like clenbuterol, to help mitigate preventable cardiovascular-related concerns among AAS consumers.
Supplemental Material
sj-docx-1-saj-10.1177_29767342261460762 – Supplemental material for How Substance Use Patterns Shape Perceived Cardiac Concern Among An International Sample of Men Who Use Anabolic-Androgenic Steroids
Supplemental material, sj-docx-1-saj-10.1177_29767342261460762 for How Substance Use Patterns Shape Perceived Cardiac Concern Among An International Sample of Men Who Use Anabolic-Androgenic Steroids by Bahareh Ahmadinejad, Benjamin Bonenti, Kimberley Akrigg, Jason Ferris, Adam Winstock, Lauren Ball, Jason M. Nagata, Kyle T. Ganson and Timothy Piatkowski in Substance Use & Addiction Journal
Footnotes
Acknowledgements
We would like to thank all the participants of the Global Drug Survey who donated their time to completing the survey. We would also like to thank A/Prof Monica Barratt and Dr Cheneal Puljevic, for their intellectual contribution to the conceptualization and methodology of the GDS.
Ethical Considerations
Ethical approval was obtained from The University of Queensland’s Human Research Ethics Committee (2023/HE001927).
Consent to Participate
All participants provided informed consent via the survey checkbox.
Author Contributions
BA: Conceptualization, Formal analysis, Data curation, Visualization, Writing – original draft. BB: Writing – review & editing. KA: Writing – review & editing. JF: Methodology, Writing – review & editing. AW: Methodology, Writing – review & editing. LB: Writing – review & editing. JMN: Writing – review & editing. KTG: Writing – review & editing. TP: Conceptualization, Methodology, Supervision, Writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TP is supported by a National Health and Medical Research Council Investigator Grant (2041822).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Adam Winstock is the founder and owner of Global Drug Survey (GDS) Ltd, an independent data exchange hub. Jason Ferris is a member of the GDS Core Research Team.
Data Availability Statement
Data available from the corresponding author on reasonable request.*
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.