
Abstract
Climate change broadly threatens the health of individuals and communities. As adverse health impacts of climate change become more prevalent, researchers are beginning to investigate how climate-related events (CRE), such as extreme temperatures, intensified hurricanes, etc., impact the health of people who use alcohol and other drugs (PWUD). A growing body of evidence suggests that CREs exacerbate harms related to substance use and disrupt treatment and harm reduction services, exposing PWUD and those with substance use disorders (SUDs) to increased morbidity and mortality. The adverse health impacts of CREs and substance use interact in a synergistic manner, influenced by individual, community, and structural factors. Understanding this evolving intersection is crucial for developing policies and interventions to reduce the increased risk to PWUD. CREs exact a costly toll on health and healthcare infrastructure and are increasing in frequency and severity. Concurrently, substance use and addiction result in thousands of deaths each year and cost the United States hundreds of billions of dollars annually. Without efforts to improve our understanding of the social, medical, and economic implications of CREs on PWUD, and develop more prepared, resilient systems of care, we can expect this compounding burden to intensify over time with deadly consequences. Effective action will require sustained, multi-level commitments from researchers, policymakers, as well as frontline clinical and non-clinical service providers. AMERSA recommends 3 areas of action: advancing research at the intersection of CREs and substance use, enhancing policies and practice guidelines to ensure uninterrupted treatment and harm reduction services during and following CREs, and facilitating education and training for awareness and preparedness. AMERSA endeavors to provide leadership and guidance in fostering more resilient and adaptive systems of care for PWUD and those with SUD as characterized by driving awareness, understanding, preparedness, and the production of a climate change-prepared addiction workforce.
Keywords
Highlights
Climate-related events (CREs) disrupt substance use prevention, treatment, and harm reduction services, increasing mortality risk and worsening outcomes among people who use drugs (PWUD) and those with substance use disorders.
The health impacts of CREs and substance use interact synergistically across individual, community, and structural levels, compounding pre-existing vulnerabilities in marginalized populations.
Research at the intersection of climate change and substance use remains critically limited despite escalating frequency and severity of CREs and an ongoing overdose crisis.
Momentum toward establishing evidence-based protocols for preparedness, coupled with development of education, research, and policy in these areas is needed.
AMERSA recommends advancing research, ensuring continuity of treatment and harm reduction services, and delivering multidisciplinary education and training to develop a climate change-prepared workforce and more resilient systems of care for PWUD.
Background
Climate change broadly threatens the health of individuals and communities by introducing new environmental hazards and exacerbating fundamental social, economic, and geographic disparities influencing the health of populations and particularly those populations that are most vulnerable and marginalized. As the adverse health effects of climate change become more prevalent, researchers are just beginning to examine the impact of climate-related events (CREs) such as extreme temperatures and intensified hurricanes on the health and well-being of people who use alcohol and other drugs (PWUD).
CREs can disproportionately impact PWUD and those with substance use disorder (SUD) by disrupting access to substance use treatment, prevention, and harm reduction services,1-4 producing drug market volatility, 5 and increasing risk for overdose, toxicity, withdrawal,2,6,7 other injuries,8,9 and exacerbation of preexisting chronic disease. Insofar as PWUD and those with SUD are often predisposed to greater socioeconomic vulnerability, 10 the adverse impact of CREs on capacity to meet basic needs (eg, housing, food, electricity, childcare)11,12 may be especially significant. During and in the aftermath of a CRE, these myriad challenges contribute to the broader intersectional risk environment, 13 that shapes an individual’s morbidity and mortality.14-16 Longitudinally, CREs are shown to influence initiation and worsening severity of alcohol and other drug use, retention in substance use treatment, and incidence of concomitant mental health diagnoses such as depression, anxiety, and post-traumatic stress disorders.17-21
The interacting health impacts of CREs, acute symptoms of substance use, and intoxication, and conditions resulting from or exacerbated by SUD are influenced by factors operating at individual, interpersonal, institutional, community, and structural levels.22-24 Figure 1 applies a social-ecological model to illustrate some of these relevant factors and is followed by an illustrative vignette.
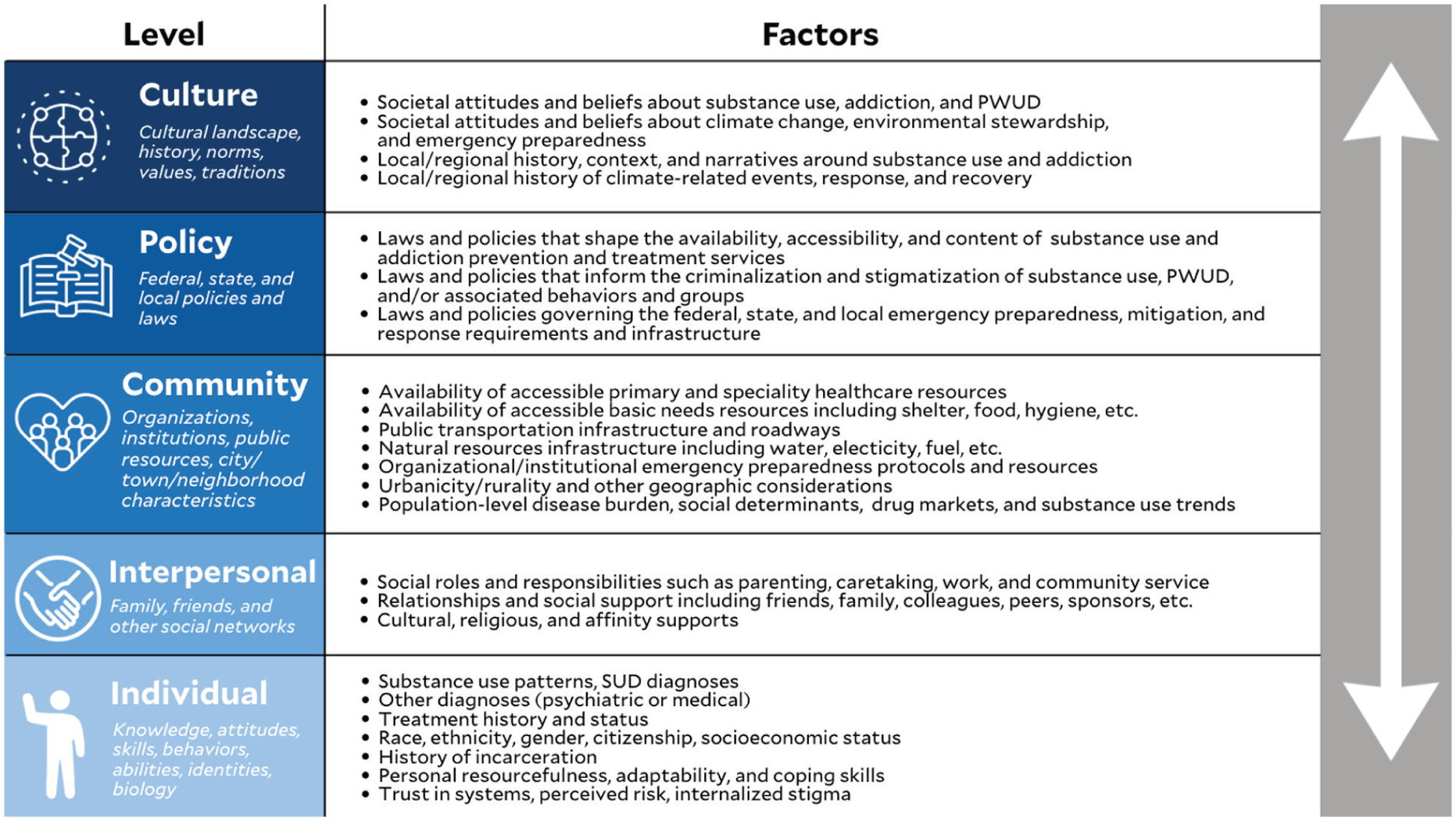
A social-ecological presentation of multilevel factors influencing the intersecting health impacts of CREs, substance use, and SUD. CRE, climate-related events; SUD, substance use disorder.
Vignette
Consider the example of Sam, a 45-year-old Hispanic male with a history of opioid use disorder who has recently enrolled in an opioid treatment program (OTP) to begin methadone treatment for the first time. Sam lives in a mid-sized Midwestern city that experienced severe flooding. The flood has rendered his home uninhabitable, and he is forced to evacuate on foot to an emergency shelter, leaving his car behind due to impassable roadways. At the individual level, Sam’s SUD diagnosis, recent treatment initiation, and loss of housing and transportation may place him at higher risk for adverse health outcomes. Before the flood, Sam drove daily to his OTP, located in a neighboring city. With that facility no longer reachable, his ability to continue taking methadone will depend on community-level alternatives, such as access to other, more proximal OTPs that are open, operational, and willing to guest-dose or provide take-home doses, the ability to receive his medication at a shelter, or the rapid restoration of transportation infrastructure.
There is no guarantee that emergency shelters will have bed availability or accept an individual currently on medications for opioid use disorder. Some but not all shelters may be equipped with medical personnel, supplies, and medications. Additionally, loss of electricity and cellular service, as well as limitations on interagency data access, may make it difficult to coordinate Sam’s care or confirm details of his medical history. Providers Sam encounters may have variable levels of comfort and clearance to prescribe or fill medications for Sam in the absence of this information.
With Sam’s treatment interrupted, he faces increased risk of opioid withdrawal. This, coupled with housing instability, stress, or other exposures, may precipitate a return to unregulated opioid use. Sam may lack access to harm reduction supplies to facilitate safer use and may be unable to store any supplies he does have securely. If he is unable to maintain shelter and is engaging in substance use, sedation and other effects of opioid use may increase his risk of harmful environmental exposures, such as overheating, burns, hypothermia, or dehydration, depending on the time of year. Sam may find himself reliant on interpersonal and community-level resources, such as friends and family, emergency departments, and mutual aid organizations, to meet basic needs, escape the elements, and ultimately restore social, economic, and medical stability. He may struggle to connect with these resources unassisted, absent cellular service or transportation. The availability and accessibility of these resources and services depend upon institutional, local, state, and federal policies that underpin the preparedness of the systems of care designed to support the wellbeing of individuals like Sam. In turn, these policies and their enforcement reflect broader cultural sentiment and historical investment by public and private sector stakeholders in climate change readiness and consideration of the needs of PWUD and those with SUD.
Issue
Sam and others are caught at the crossroads of 2 simultaneous crises. Amidst an ongoing climate crisis, the frequency and severity of CREs affecting the United States are increasing. 25 The National Oceanic and Atmospheric Administration (NOAA)’s National Centers for Environmental Information (NCEI) reported 27 large-scale CREs in 2024 alone that individually resulted in more than $1 billion in damages, costing the United States an estimated $182.7 billion in total. 26 Healthcare expenses comprise a substantial portion of the costs associated with CREs. A 2019 analysis of 10 CREs that occurred in 2012 estimated the associated healthcare expenses at $10 billion, accounting for deaths, hospitalizations, emergency department utilization, and related medical services. 27 This does not account for downstream healthcare costs in the months and years following a CRE.
The current overdose crisis is characterized by broad suffusion of fentanyl in the unregulated opioid supply and, increasingly, stimulant and benzodiazepine supplies as well. 28 Emerging adulterants (eg, xylazine, medetomidine) have introduced a new constellation of health risks and complications for PWUD. While available data indicate that overdose deaths have declined in recent years, 29 the annual death toll remains significant. The Centers for Disease Control and Prevention provisionally estimate that over 70 000 overdose deaths occurred in the 12-month period ending September 2025. 30 Cumulative healthcare costs associated with addiction and overdose in the United States are estimated in the trillions of dollars. 31
CREs exacerbate the health harms of substance use and addiction, and vice versa, disproportionately affecting populations that are, in many cases, already at heightened vulnerability and disadvantage. It is imperative that researchers, policymakers, and health care service providers improve their understanding of and capacity to respond to these intersecting crises. To date, however, research, evaluation, and practice innovation in this area are quite limited. 32 As a result, when CREs occur, systems of care serving PWUD and those with SUD are often unprepared, producing service disruptions and associated adverse outcomes. 33
Policy and Practice Recommendations
Policy and practice recommendations to improve understanding of CREs as they impact PWUD and those with SUD and capacity to mitigate and respond to such events, should broadly focus on expanding resources available to study the nexus of climate change and substance use, integrate substance use and SUD considerations into general emergency planning and adapt existing treatment, harm reduction, and prevention services to ensure continuity of care during and after CREs.
AMERSA’s recommendations fall within 3 core interventional domains:
Advancing Research at the Intersection of Climate Change and Substance Use.
Facilitating Continuity of Treatment and Harm Reduction Services During and After CREs.
Delivering Multidisciplinary Education and Training for Awareness and Preparedness.
Advancing Research at the Intersection of Climate Change and Substance Use
AMERSA supports the conduct of quantitative, qualitative, and mixed-methods research to define, describe, and characterize the unique risks and impact of CREs on PWUD and those with SUDs. Research should center people with lived experience of CREs, substance use, and SUD, and prioritize community-engaged methodologies.
AMERSA supports the conduct of needs and assets assessments examining integration of PWUD and SUD considerations into existing state-, county-, and municipal-level preparedness planning activities (eg, protocols, guidance, drills).
AMERSA supports the conduct of medical education research to establish best practices in the education of health professions about the intersection between climate change, substance use, and addiction, and the ethical pursuit of research at this intersection.
AMERSA supports the conduct of qualitative, quantitative, and mixed-methods research to establish best practices in protecting and fostering addiction workforce resilience during and after CREs.
AMERSA supports efforts to advocate for, preserve, and expand public and private funding mechanisms for research and evaluation concerning the impact of CREs on PWUD and those with SUD.
Facilitating Continuity of Treatment and Harm Reduction Services During and After CREs
AMERSA endorses the Addressing Addiction After Disasters Act (H.R. 5623, or the AAAD Act), which would amend Section 416 (P.L. 100-707) of the Robert T. Stafford Disaster Relief and Emergency Assistance Training Act to include SUD services among those eligible for emergency funding and provision by the Federal Emergency Management Agency (FEMA) under the Crisis Counseling Assistance and Training Program. 12
AMERSA reaffirms its prior endorsement of the Modernizing Opioid Treatment Access Act (S.644, MOTAA) with particular emphasis on prospective benefits of policy and practice proposed therein to methadone treatment access and continuity in emergency circumstances (The Stafford Act authorizes the provision of grant funding by FEMA to provide counseling services and other broadly defined “mental health services” to victims of major disasters via a Crisis Counseling Assistance and Training Program (CCATP). The AAAD Act, introduced in the House of Representatives in November 2025, would amend the Stafford Act to extend FEMA’s authorization to include funding and provision of SUDs services under the CCATP.34-36).
AMERSA supports efforts to advocate, pilot, and scale innovative MOUD delivery and financing models to expand treatment access, improve adaptability of treatment systems, and support treatment continuity in the setting of CREs.
AMERSA supports efforts to advocate, pilot, and scale innovative harm reduction service delivery and financing models to ensure uninterrupted access to naloxone and safer use supplies in the setting of CREs as well as appropriate administrative and operational support for frontline workers.
AMERSA supports policy and practice interventions that facilitate interagency and interstate collaborations in crisis mitigation and response, such as resource stockpiling, data-sharing, crisis communication and supply chain plans, standardization of regional preparedness protocols, and joint training exercises.
Delivering Multidisciplinary Education and Training for Awareness and Preparedness
AMERSA supports the development, evaluation, and dissemination of educational resources (eg, curricula, trainings, factsheets, and other guidance, etc.) on the interactions between climate change and substance use for key audiences including health professions learners, multidisciplinary healthcare providers, PWUD and individuals with SUD, policymakers, social services professionals, law enforcement, harm reduction and mutual aid workers, and funders.
AMERSA supports the development, evaluation, and dissemination of CRE preparedness education and planning tools specific to substance use and addiction (eg, curricula, case studies, trainings, toolkits, protocols, care pathways, checklists, drill templates, etc.) for key audiences including government, professional associations, community- and hospital-based treatment facilities, pharmacies, shelters, harm reduction organizations, law enforcement, and carceral facilities.
AMERSA supports the production of informational resources on notable federal, state, and local policy options, and best practice case studies for use by policymakers, advocates, and health policy researchers.
Footnotes
Acknowledgements
Position statements clarify key issues that are in alignment with the vision, mission, and values of AMERSA, Inc. This Position Statement, endorsed by their Board of Directors on April 10, 2026, amplifies the position of the organization, guides their activities, and informs the public and policy makers on the organization’s stance on this issue. We thank the AMERSA Board of Directors for their review of various drafts of this position statement and endorsement of the final version. The Board of Directors has been deemed not to have any conflicts of interest with the approved Position Statement. Potential conflicts of interest of the AMERSA Board of Directors are on file with AMERSA office and accessible upon Request. The following Board of Directors member(s) declares, and is deemed to have, a conflict of interest for this Position Statement: Jenna Butner and Shannon Smith-Bernardin are on the AMERSA Board of Directors and have abstained from voting for its approval.
Author Note
The opinions expressed in this article represent those of AMERSA and the authors, not necessarily the affiliated institutions.
Ethical Considerations
Institutional Review Board Approval was not required.
Author Contributions
Jenna L. Butner: Conceptualization, Writing—Original Draft, Review, and Editing; Shannon Smith-Bernardin: Writing, Review, and Editing; Joyce Roberson-Steele: Writing/Review; Brandee Madden: Conceptualization; Valerie A. Gruber: Conceptualization, Review; Judith I. Tsui: Conceptualization, Review, Editing, Supervision; Emma T. Biegacki: Conceptualization, Writing—Original Draft, Review, and Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.