
Abstract
The expansion of peer recovery support services has not only rapidly integrated peers across service systems but also threatens to drift peer roles toward clinical duties and erode values that gave rise to the peer support movement. The earliest peer professional roles emerged from social advocacy efforts that rejected clinical, hierarchical, and coercive models of care, instead advancing nonclinical, mutual, and person-centered recovery support. As the U.S. Office of National Drug Control Policy calls to strengthen the peer workforce, it offers an opportunity to revisit the social movements that built peer support, clarify why these founding values were considered essential, and use these principles to guide contemporary policy and funding decisions. In this commentary, we provide historical context for the intention of professional peer support roles and articulate how federal and state policy can resist the force of role drift by grounding future workforce development in the movement’s original values.
Highlights
Social movements established peer support to be nonclinical, mutual, and person- and community-centered.
Integration and expansion now risk eroding these values.
Policy should reinforce value-consistent peer roles through clear reimbursement guidance and alignment with Substance Abuse and Mental Health Services Administration competencies.
Investment must prioritize peer-led organizations and infrastructure for training and professional development.
Introduction
The United States has experienced a remarkable rise in peer recovery support services (PRSS) for substance use disorder (SUD) over the past 25 years, 1 supported by the emergence of peer certification, new funding streams for reimbursement, and the integration of peer specialists into a growing number of care settings.2-5 Most recently, this growth has been reinforced by federal interest in expanding the workforce. In 2026, the U.S. Office of National Drug Control Policy (ONDCP) called to “expand and enhance the Nation’s (PRSS) workforce and organizational infrastructure,” 6 signaling continued national investment in scaling peer-delivered services. However, this call for expansion comes at a time when the PRSS workforce is under increasing pressure to conform to clinical models of care. Concerns about fraud and role clarity have led some states to emphasize clinical supervision structures and certification models patterned after professional licensure,7-9 contributing to role drift toward clinical duties and the erosion of peer-specific values. These developments raise an important question: as policymakers seek to expand the peer workforce, how can the field avoid repeating historical patterns in which recovery support roles become absorbed into clinical paradigms, weakening the distinct contributions of lived experience?
In this commentary, we argue that social movements which birthed PRSS historically emphasized nonclinical, nonhierarchical, and person- and community-centered care, and these values should serve as a guide for contemporary workforce expansion, helping ensure that growth strengthens rather than dilutes the unique and clinically complementary role of peers in SUD care. We offer specific policy recommendations drawn on a narrative synthesis of historical, review of contemporary policy, and the authors’ collective experience as researchers and participants in workforce development initiatives.
Peer Support as a Social Movement
Professional peer support was born of 2 modern advocacy movements: the psychiatric survivors movement in mental health and New Recovery Advocacy Movement (NRAM) in the SUD field.10-13 In the 1960s and 1970s, the efforts of former mental health service recipients (calling themselves “survivors”) and allied social workers brought to light the poor conditions of psychiatric institutions, which stripped patients of their rights and put them through abuse by clinical staff.14-16 Survivors and their allies fought and won battles for deinstitutionalization, secured protection of patients’ rights, and introduced services operated by people with lived experience. 15 In 1986, the first professional peer roles (“consumer case aides”) were introduced in care settings in Colorado, and by 1999, Georgia requested and received the first state-wide Medicaid reimbursement for peer support services.17,18
There was just as significant a social movement in the SUD field to champion peer support. Specialty addiction treatment emerged and grew rapidly from the 1950s to 1970s, and people with lived experience initially made up much of its workforce.19,20 Nearly 70% of addiction counselors in the early 1970s reportedly had personal recovery experience, 10 but increased medicalization of SUD treatment and funding expansion encouraged a shift toward standardization and higher qualifications. 20 As a result, recovery representation declined to about 30% of counselors by the 2000s. 10 Representation would be key for NRAM, a grassroots reaction at the turn of the 21st century to perceived failures of SUD treatment systems.4,21,22 Like mental health advocates, NRAM leaders supported shifting the goal of treatment toward “long-term recovery.” This shift was reflected in the emerging framework of Recovery-Oriented Systems of Care, which emphasized mobilizing recovery support resources beyond acute treatment. 23 Within this vision, peer roles were designed to bridge professional treatment systems with nonprofessional recovery communities, and NRAM produced some of the earliest designs for professional peer support roles, emphasizing values to distinguish PRSS from traditional services.10,24,25
What were these values, and why were they emphasized? PRSS were to be nonclinical, as outlined by NRAM-era trainings and publications.10,26,27 This boundary was not intended to position peers in opposition to clinical care, but to define a distinct contribution alongside it. As early leaders noted, peer-based recovery support services were intended to complement professional treatment, enhancing engagement and helping sustain recovery beyond formal care. Where clinically oriented SUD services often focus inward on treating trauma and intrapersonal concerns, PRSS were to focus outward, linking people in or exiting treatment to resources and relationships in the community that support long-term recovery. 10 PRSS were to be nonhierarchical or mutual, where peers saw themselves and delivered services in a way that reflected equal power between them and service recipients.24,27 PRSS were not to involve enforcing compliance or conducting surveillance. Finally, PRSS were to be person- and community-centered, with support and “respect for diverse pathways and styles of recovery,” and appreciation for the role of community within the recovery process.24,27 Abstinence was not to be the one and only goal, nor 12-step the only pathway. The earliest trainers of the professional peer workforce (eg, the Connecticut Community for Addiction Recovery) explicitly instilled these values into their curricula as lessons from the addiction counseling workforce.24,26 NRAM advocates believed that over-professionalization had trained out the very qualities that had made peer-based SUD counseling originally effective. 10 They sought to avoid re-creating a bureaucratic and standardized workforce and keep PRSS focused on promoting long-term recovery.
Recommendations to Strengthen the PRSS Workforce
While the ONDCP call to strengthen the PRSS workforce is a symbol of progress, there are signs that this push threatens to replicate issues that negatively impacted addiction counseling. Peers increasingly work within clinical and regulated service environments, 28 where their roles can complement and improve traditional treatment. Yet these same environments also create conditions where role boundaries can blur. Peers report they are increasingly expected to perform clinical, hierarchical, and nonperson- and community-centered duties: providing psychotherapy, collaborating in surveillance (eg, urine analysis), endorsing specific recovery pathways, and completing regulatory paperwork.3,29,30 More alarming are examples like Kentucky, where licensure requirements for peers were recently introduced, structured on the licensing of professional counseling. 7 Without clear role protections, workforce expansion and integration into clinical systems may unintentionally produce scope creep, and we would again lose the value of a workforce with an intentional focus on shared lived experience and mutuality. Ultimately, the pressure to become more clinical threatens the willingness of individuals receiving care to trust and work alongside peer support workers.
If the current administration is interested in strengthening and expanding the PRSS workforce, it must support funding and policy informed by historical values meant to maintain the unique value of peer support.3,31,32 We recognize that these values risk being lost within systems governed by reimbursement and regulatory requirements. Integration into such systems brings pressure for adaptation and trade-off. However, historical examples such as the labor movement suggest that foundational values can still function as guideposts for shaping policy and practice, even as roles evolve across different service environments. 33 Seeking to preserve the founding values of peer support, we offer 2 overarching recommendations for future peer workforce development (recommendations summarized in Table 1):
Support a Role Definition that is Guided by the Original Values of Peer Support: Organizations like the International Certification & Reciprocity Consortium, the National Association of Peer Supporters (NAPS; recently dissolved), and the Substance Abuse and Mental Health Services Administration (SAMHSA) have carried forward the original values of peer support through their core competency and ethical guidelines for peer roles.34-37 For example, SAMHSA lists 5 “foundational principles” or values for the competencies of peer workers: recovery-oriented, person-centered, voluntary, relationship focused, and trauma-informed. 37 These guidelines have formed the basis of state-level certifications and trainings that exist in almost every U.S. state. 38 Role drift, however, primarily arises from the expectations of employers.29,39 For example, a recent study in Kentucky found that while peers’ training and self-definitions were consistent with SAMHSA’s core competencies, employers expectations fell well outside the peer scope, from peers taking out trash to violating ethics by reporting clients to law enforcement. 30
Strategies are needed to engage employers and incentivize proper structuring of the peer role. We suggest the following funding and policy directives to support a role definition consistent with peer values:
Incentivize Organizational Planning for Peer Integration and Education on the Peer Role: Although states have created peer certifications to access federal funding streams, few mechanisms ensure that organizational leadership or supervisors understand the peer role or intentionally plan for integrating PRSS, especially when working alongside clinical colleagues. Training and technical assistance should target employers and supervisors of peers to ensure they are trained on the peer role. States could address this by requiring agencies that bill for peer services to certify as qualified peer provider organizations, demonstrating that leadership and staff have completed peer and technical and that the agency has a plan for structuring the peer role. An existing comparison is California, where Medicaid Managed Care Plans are required to submit community health worker (CHW) integration plans for state approval before becoming eligible for reimbursement. 40 There is also a need to define “best practices” or “organizational competencies” to parallel peers’ individual competencies. ONDCP should convene an interagency working group, much like the recovery services interagency working group it convened in 2024, 41 to define best organizational practices for employing and integrating PRSS.
Tie Reimbursement to Clear Peer Support Role Definitions: Federal agencies, with leadership from the ONDCP, should help strengthen Medicare and Medicaid’s alignment with SAMHSA’s Core Competencies and National Model Standards. Medicaid guidance on peer support, first issued in 2007 and most recently updated in a 2024 FAQ, 42 references these documents only as optional resources and defers training, supervision, and scope-of-practice decisions to states. Medicare has recently allowed physicians to bill for peer support specialists as auxiliary personnel, 43 but has not published its own peer-specific guidance. ONDCP has helped clarify Medicaid policy in the past, such as working with Health and Human Services (HHS) to publish concrete examples of harm reduction services that states could include in their Medicaid State Plan Amendments to qualify for reimbursement. 44 In future policy directives, ONDCP should similarly direct HHS and CMS to provide examples of what peer activities should (and should not) be reimbursable and make alignment with SAMHSA’s core competencies and model standards an expectation in payment policy. The ONDCP should also encourage the removal of blanket criminal history restrictions that prevent peers with justice involvement from being reimbursed or certified. 45
Use Federal Grants and Demonstrations to Encourage Value-Consistent Peer Roles: The ONDCP should direct that federally funded service grants and demonstration programs involving PRSS require applicants to submit peer-specific job descriptions, employee manuals, and documentation of leadership training that align with SAMHSA’s Core Competencies and the National Practice Guidelines for Peer Supporters. While ONDCP does not directly administer grant programs, it has historically influenced federal funding priorities, for example, by directing health resources and services administration (HRSA) to allocate resources for SUD treatment services in primary care settings. 46 A preliminary step toward strengthening peer funding is the Providing Empathetic and Support Act, 47 introduced in April 2025, which would establish a Standard Occupational Classification (SOC) category for peer support specialists consistent with SAMHSA core competencies and NAPS guidelines, which advocate for mutual, nonclinical, and person-centered peer roles. Although SOC codes do not regulate scope of practice or prevent role misuse, creating a dedicated SOC would significantly increase the visibility of the peer workforce in federal labor statistics, supporting a stronger justification for workforce development funding.
2. Strengthen Peer-Led Organizations and Links to Community Recovery: Peer support was never meant to function as a standalone service; social movements envisioned it as a bridge between the individual, formal systems of care, and broader recovery support resources within the community, such as recovery community organizations (RCOs). NRAM advocates were especially concerned with ensuring that peer roles linked clinical, criminal-legal, and social service systems to nonprofessional recovery organizations and mutual aid networks, reinforcing long-term recovery rather than dependence on repeating cycles of acute care.10,24,27 As peers have become increasingly embedded within traditional service systems; however, this bridging function has weakened. Standardization, medicalization, and role drift threaten to pull peers into the logics of the systems they were meant to counterbalance, while recent funding disruptions highlight the vulnerability of a workforce largely housed within nonpeer institutions.
Given the shared emphasis on community linkage, it is tempting to merge PRSS into broader health workforce roles such as CHWs, 48 particularly as payment models seek standardized roles. While CHWs and peers may share functions such as outreach and system navigation, PRSS bring distinct forms of lived recovery expertise that could be lost in a generalist health role: mutual identification grounded in personal recovery experience, credible hope about the possibility of long-term recovery, and intimate knowledge of recovery-specific resources such as mutual aid and recovery housing.49,50 These capacities allow peers to engage individuals with high addiction severity and low recovery capital who may not be well served by generalist health roles, and to link them to recovery communities that sustain long-term recovery beyond formal treatment. 51
To strengthen the peer workforce in ways that honors its origins, policy must support peer-led professionalization efforts while simultaneously protecting the community-rooted nature of peer support. These dual aims are necessary to prevent co-optation and to ensure that peer roles remain grounded in the values and social connections that made them effective in the first place. We offer the following recommendations to advance these goals:
Link Technical Assistance Funding to Peer-Led Professional Organizations: In recent years, peer support workers have demonstrated the capacity to lead their own professional development. Much of this work has been driven by peer-led professional organizations dedicated to advancing the field through training and certification programs, hosting networking groups, and sustaining advocacy efforts that originally defined the peer movement.52,53 Peer-led organizations are those in which individuals with experience as peers hold primary leadership, shaping priorities and advocacy agendas in ways that center the professional needs of the peer workforce, rather than outside interests or the behavioral workforce at large. Examples include RCOs and peer-led professional development organizations. By a recent estimate, peer-led professional development organizations were present in at least 16 states. 3 The recent reauthorization of the SUPPORT Act strengthens this momentum by expanding SAMHSA’s Center for Addiction Recovery Support and authorizing new Regional Technical Assistance Centers to support peer professional development and the delivery of recovery support services in nonclinical settings. 54 This is an important opportunity for the federal government to partner with state-level peer-led organizations, ensuring that technical assistance, workforce investment, and policy implementation are shaped by those with lived experience and grounded in the founding values of peer support.
Design Reimbursement to Bridge Professional Treatment With Community Recovery Support: Payment models should explicitly fund peers as connectors between clinical care and community-based recovery, emphasizing their “outward” nonclinical role. Recently, the Alliance for Addiction Payment reform has lobbied to for a better recovery payor system through its Addiction Recovery Medical Home Alternative Payment Model. 55 The model bundles care to integrate treatment and recovery into a package that must include acute, outpatient, home health, recovery supports, and virtual services, all linked by shared workflows, discharge planning, and technology. It also creates a dedicated “community-based recovery management” episode in which bundled payments and quality metrics are tied to long-term recovery in the person’s natural living environment, incentivizing providers to partner with community recovery supports and prevent avoidable return to higher levels of care. Building on these principles, Medicaid and other payors should be directed to design benefits and alternative payment models that bundle services from peer-led recovery organizations and explicitly reimburse peer activities focused on linkage to mutual aid, recovery housing, and other community resources. Policymakers can also look outside the United States for models of funding peer support, like the United Kingdom’s National Health Service, which directly hires and salaries peer workers in acute and community care settings. 56
Peer Workforce Recommendations.
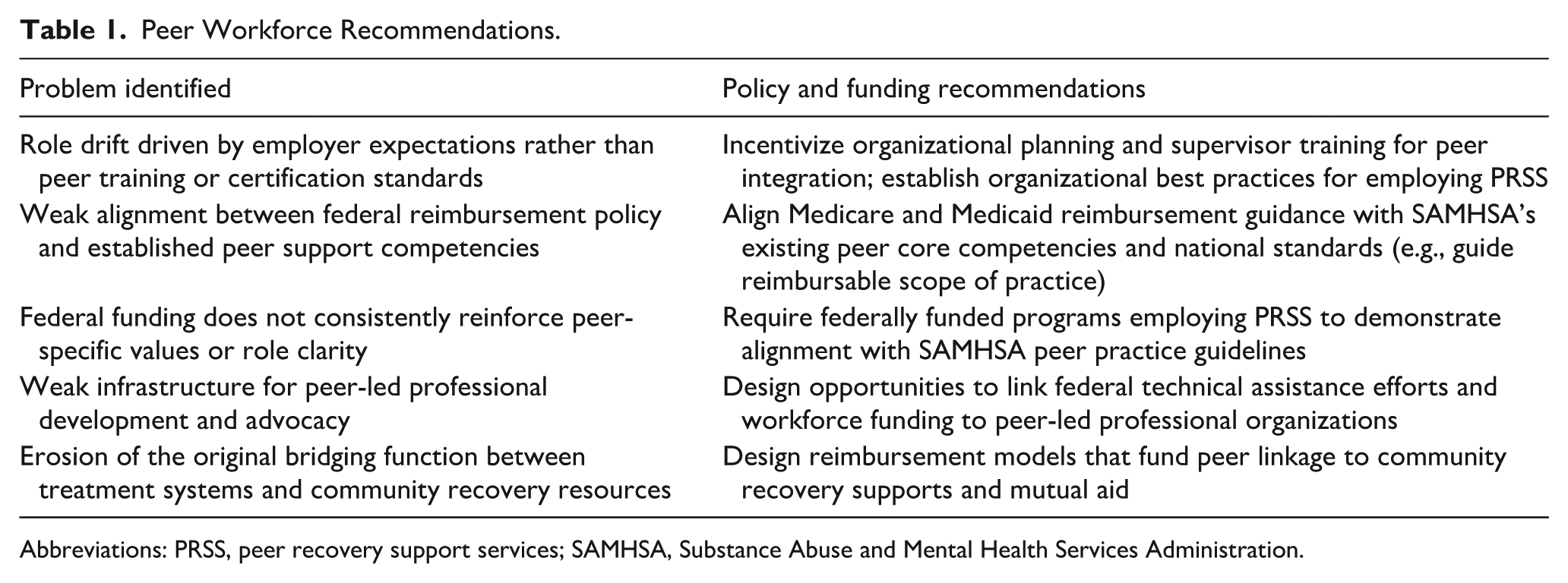
Abbreviations: PRSS, peer recovery support services; SAMHSA, Substance Abuse and Mental Health Services Administration.
Conclusion
Social movements in the 20th century imagined professional peer support would complement and improve SUD treatment by (1) offering a menu of nonclinical, nonhierarchical, and person- and community-centered services and (2) bridging formal treatment to recovery support in the community, to create pathways to long-term recovery. The ONDCP’s call to strengthen the peer recovery workforce offers an opportunity to resist the limitations and pitfalls of professionalization, and ensure these qualities are maintained as much as possible.
To do so, policymakers should prioritize 2 complementary strategies. First, workforce expansion should be grounded in clear role definitions aligned with the foundational values of peer support. This can be advanced through policies that incentivize organizational planning for peer integration, align reimbursement with established peer competencies, and ensure workforce initiatives reinforce these standards. Second, policy should bolster the role of peer-led organizations and emphasize the community-oriented nature of peer support, through investments in peer-led professional development, RCOs, and payment models that fund peers as connectors between treatment systems and community resources. By prioritizing these strategies, federal agencies can expand the peer workforce while preserving qualities that have historically made peer support a unique and effective component of the recovery ecosystem.
Footnotes
Ethical Considerations
There are no human participants in this article and informed consent is not required.
Author Contributions
JSB and DPW contributed substantially to the conceptualization, writing, and editing of the manuscript. AU, JS, and WLW contributed substantially to the writing and editing of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.