
Abstract
Background
Despite the recognition of substance use and sex work as public health issues, the intersection of these areas, especially within the rural US, is an area of special importance.
Methods
The Rural Opioid Initiative comprises of eight research cohorts spanning 10 states and 65 rural US counties. Between 1/2018-3/2020, individuals who reported past 30-day substance injection or opioid misuse were recruited. Analyses were restricted to people who use drugs (PWUD) who reported trading “vaginal or anal sex for drugs, money, housing, or other things you need” in the past 30 days. We analyzed cross-sectional associations between injection drug use and sexual behaviors associated with hepatitis C virus (HCV)/HIV infection transmission, access to harm reduction, and HCV status among PWUD and engaged in sex work in rural US areas.
Results
Of the 2045 participants, 9% (n=180) reported engagement with sex work, with just over half being women (58% [n=104]). In adjusted models, people who engaged in sex work, compared to PWUD who did not, had higher prevalence ratios of past 30-day receptive syringe sharing (adjusted prevalence ratio [aPR]=1.69, 95% Confidence Interval [95%CI]=1.44–1.98), practice of multiple injections per injection episode (aPR = 1.28, 95% CI = 1.15–1.43), practice of syringe mediated drug sharing (aPR=1.50, 95% CI=1.32–1.71), condomless sex (aPR=1.62, 95% CI=1.48–1.77) and condomless sex with someone who injects drugs (aPR=2.05, 95% CI=1.76–2.39). PWUD engaged in sex work were less likely to report easy condom access (aPR=0.88, 95% CI=0.80–0.96), while no significant differences were observed for most other harm reduction access measures.
Conclusion
PWUD engaged in sex work in the rural US had higher likelihood of injection drug use and sexual behaviors associated with HCV/HIV infection transmission, while having lower use of and access to condoms. This study emphasizes the importance of ensuring affordable access to condoms within the context of harm reduction services, especially given the limited access to health care and supportive services, particularly in rural communities.
Keywords
Introduction
Over the past 20 years there has been a sharp increase in opioid use across the United States (US), coinciding with the six-fold increase in the number of opioid overdose deaths from 1999 to 2021. 1 The US opioid crisis is marked by the inclusion of multiple substances, including shifts of use across the lifespan of an individual. 2 This increase in substance use has exacerbated socio-economic vulnerabilities, such as being unhoused, poverty, and unemployment. 3 Many people begin selling or trading sex to gain economic support or obtain necessities when they experience these socio-economic vulnerabilities.3,4
The relationship between substance use and sex work has long been documented,5-7 with one study finding that lifetime substance use among females engaged in sex work as high as 84% in North America. 8 Some individuals begin sex work as a means to pay for their substance use practice, 6 while others initiate or continue substance use as a coping mechanism in response to trauma, stigma, violence, or psychological distress associated with sex work. 9 Substance use may also assist in sex work as a social function or an enhancement motivation, 10 such as increased confidence, reduced anxiety, enhancing pleasure, or facilitating interpersonal interactions.10,11 These motivations may shape injection and sexual behaviors among PWUD who sell sex and are important to consider when examining infectious disease transmission vulnerability among people who sell sex.
Substance use and sexual risk behaviors intersect through several behavioral pathways that increase vulnerability to HIV and HCV transmission. Substance use before or during sexual activity reduces the likelihood of condom use, 12 while also increasing the likelihood of engaging with multiple or higher risk sex partners.13,14 People engaged in selling sex have high rates of present or past injection drug use, 5 which is associated with behaviors that increase the risk of blood-borne infections. 15 This risk is further compounded by the criminalization of both sex work and substance use, which can deter individuals from seeking harm reduction services they need. 5
Illicit substance use and in-person, physical sex work are criminalized across the US. The multifaceted criminalization promotes stigmatization and discrimination in legal and regulatory settings for people who use drugs (PWUD) and people who sell sex– independently and especially at their intersection. 16 The stigma towards substance use and sex work further exacerbates the barriers to accessing key services for this population. 17 Due to the criminalized nature of sex work, many people who sell sex experience frequent interactions with law enforcement, including routine stops and enforcement activities, with some reporting encounters on a weekly or even daily basis. 18 People engaged in sex work also have lower access to harm reduction programs as a result of policing practices. 5
Despite the recognition of substance use and sex work as public health issues, the intersection of these areas, especially within the rural US, is an area of special importance for understanding marginalized populations. Compared to urban areas, rural communities often have more limited access to harm reduction services, fewer healthcare providers, greater transportation barriers, and heightened stigma due to reduced anonymity. 19 These structural and geographic barriers may exacerbate risk environments for PWUD who engage in sex work and limit access to prevention and care services. Additionally, rural community members engaged in sex work experience multi-faceted levels of stigma ranging from rural PWUD who hold negative attitudes and perception towards people who sell sex in their community and from health care providers which deters people who sell sex from accessing key health services.8,20-23 Past research has been predominantly focused on females engaged in street-based sex work in urban areas and far fewer studies have focused on rural areas.17,18,23-34 As a result, findings from urban-based studies may not be generalizable to rural populations.
This study aims to examine whether engagement in sex work among PWUD in rural US settings is associated with differences in injection-related risk behaviors, sexual risk behaviors, access to harm reduction resources, and HCV status.
Methods
This cross-sectional, multi-study analysis utilizes data from the Rural Opioid Initiative (ROI). The ROI, which has been previously described here, 35 is a biphasic, multi-agency cooperative agreement with the goal to better understand the opioid overdose epidemic in the rural US. The ROI comprises of 8 research cohorts which span 10 states (Illinois, Kentucky, Massachusetts, New Hampshire, North Carolina, Ohio, Oregon, Vermont, West Virginia, and Wisconsin) and 65 rural US counties. ROI participants were recruited from January 2018 to March 2020. All cohorts obtained approval from their local institutional review board for research activities and data sharing within ROI. Past 30-day sex work was not asked of all participants from WI, therefore, we excluded WI from the analysis.
Study Participants
Eligibility criteria for ROI participation included: self-reported injection of any substance or use of opioids (e.g., heroin, fentanyl, opioid pain medication, etc.) via any route “to get high” in the past 30-days; residence in one of the participating rural counties; and a minimum age (≥18 for 6 studies and ≥15 for 2 studies). Although two cohorts allowed enrollment of participants 15-17 years, no participants under the age of 18 were present in the analytic sample. All participants provided written consent prior to partaking in the study.
We restricted this analysis to ROI participants who self-reported their past 30-day engagement with sex work from the seven cohorts that asked. We additionally restricted this analysis to participants who self-reported their gender as female or male, excluding participants who self-reported transgender (n = 4) as their gender identity due to small numbers and concerns of confidentiality.
Study Procedures
ROI utilized respondent driven sampling 36 (RDS) to recruit participants from various venues, including local health departments, community health centers, syringe service programs, and community outreach centers. As described in detail elsewhere, 37 each cohort recruited seeds from their target population to initiate peer recruitment. The participants that were recruited as seeds then provided coupons to recruit peers. Financial incentives were provided to seeds for recruitment ($10-$20 per eligible peer recruited) and to study participants ($40-$60). Participants were administered a standardized survey either through computer-assisted self-interviews 38 (CASI), computer-assisted personal interviews 39 (CAPI), or audio computer-assisted self-interviews 40 (A-CASI).
Measures
ROI participants were asked, “in the last 30 days, how many times did you trade vaginal or anal sex for drugs, money, housing, or other things you need,” and were allowed to provide a discrete number ranging from 0 to 900. ROI participants are considered having engaged in sex work if they responded ≥1 to the question.
Measurements of past 30-day substance use and frequency of use “to get high” are used to describe substance use patterns. Participants were asked about past 30-day drug use of the following substances: heroin, fentanyl, prescription opioid misuse, buprenorphine, methadone, benzodiazepines, cocaine/crack, methamphetamine, gabapentin, or clonidine; and simultaneous injection of an opioid and a stimulant. In addition, participants were asked about their heavy episodic drinking, defined as having 4 drinks (females)/5 drinks (males) or more in a day.
We evaluated outcomes in four domains: 1) injection drug use behaviors associated with HCV/HIV infection transmission in the past 30 days (current injection drug use, receptive syringe sharing [i.e., use of a syringe or needle previously used by someone else], syringe mediated drug sharing [i.e., injecting substances that somebody else prepared, mixed, or divided with a used syringe], and use of multiple injections per injection episode); 2) sexual behaviors associated with infectious disease transmission in the past 30 days (sex without a condom and sex with someone who injects substances without a condom); 3) access to harm reduction methods (current possession of naloxone, a majority of syringes/needles coming from a pharmacy or syringe/needle exchange program, ease of obtaining new, clean syringes/needles and condoms), and 4) hepatitis C virus (HCV) status (self-reported ever being told they tested positive for HCV).
Statistical Analyses
We conducted analyses in our overall study population to describe various demographic characteristics, substance use patterns, and the four outcome domains of ROI participants as they relate to sex work engagement. We estimated associations using multivariable relative risk regression employed through applying Poisson regression to binomial data to estimate adjusted prevalence ratios (aPR). 41 Of interest was the association between engagement in sex work and our stated outcomes of interest, including injection drug use and sexual behaviors associated with infection transmission, access to harm reduction methods, and HCV status. To address confounding among our study population, participants who reported engaging in sex work were matched without replacement 1:3 to participants who reported not engaging in sex work. Matching criteria included age (within 5 years), gender (female, male), and geographic area. Exact matching for all three matching criteria was possible for all participants who reported engagement with sex work. We additionally adjusted for age as a continuous linear variable.
A sensitivity analysis was conducted by replicating the methods used in the main multivariable analysis to estimate prevalence ratios using multivariable relative-risk regression restricted to participants who reported past 30-day injection drug use.
In our supplemental tables, we replicated the methods utilized for the multivariable models in the main analysis and additionally adjusted for experiencing houselessness (Supplemental Table 1). We also provided demographic characteristics by sex work engagement for study participants who reported past 30-day injection drug use (Supplemental Table 2). All analyses were completed in STATA v. 17.0 (College Station, Texas).
Results
Demographic Characteristics by Sex Work Engagement Among Rural Opioid Initiative Participants Who Self-Reported Their Past 30-Day Sex Work Engagement, by Geographic Area (N=2041)
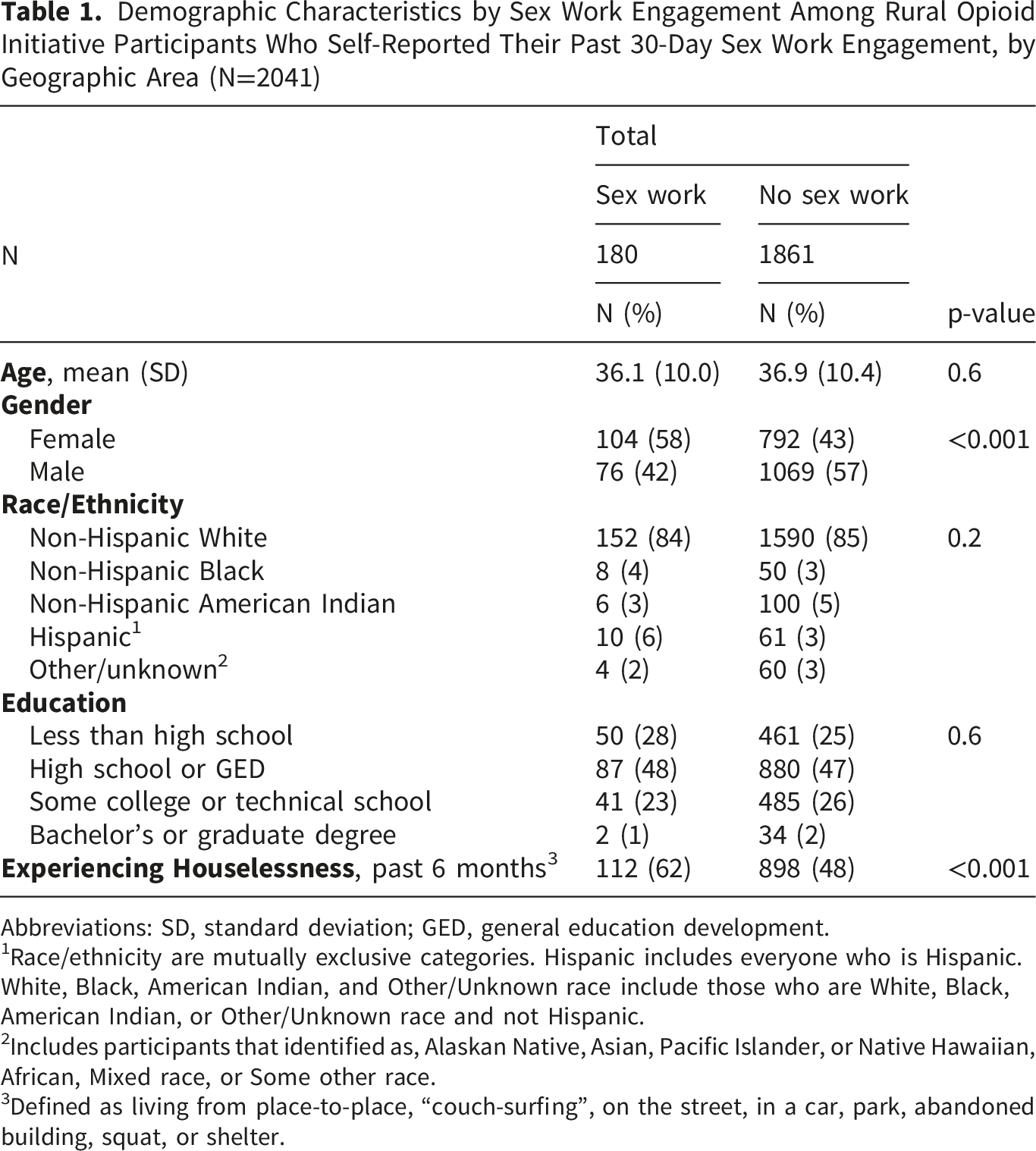
Abbreviations: SD, standard deviation; GED, general education development.
1Race/ethnicity are mutually exclusive categories. Hispanic includes everyone who is Hispanic. White, Black, American Indian, and Other/Unknown race include those who are White, Black, American Indian, or Other/Unknown race and not Hispanic.
2Includes participants that identified as, Alaskan Native, Asian, Pacific Islander, or Native Hawaiian, African, Mixed race, or Some other race.
3Defined as living from place-to-place, “couch-surfing”, on the street, in a car, park, abandoned building, squat, or shelter.
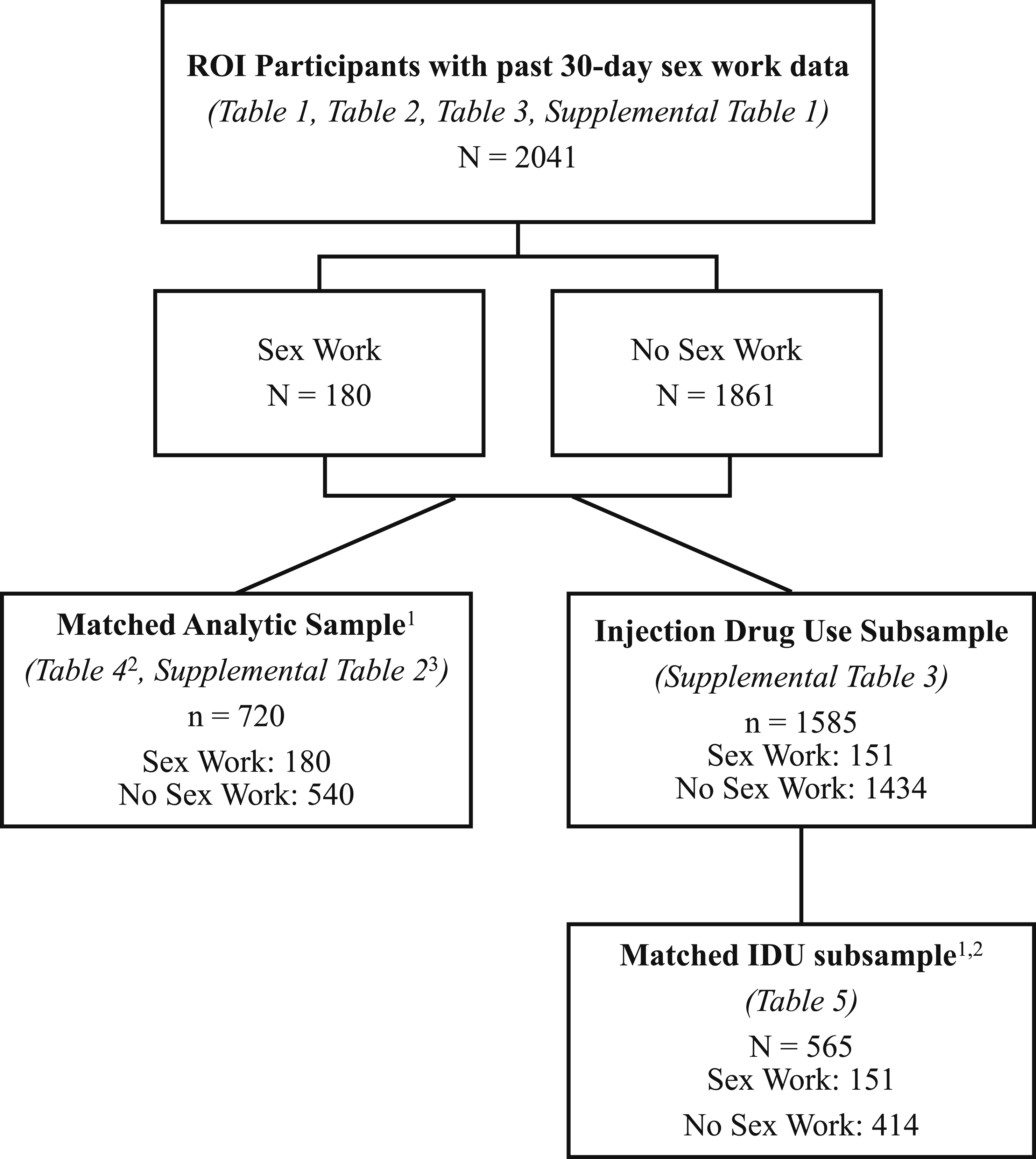
Flow diagram of analytic sample selection for main and supplemental analyses1 Matched sample 1:3 without replacement, matched on age ± 5 years, gender, geographic area2 Modified Poisson regression analysis estimating prevalence ratios adjusted for age3 Modified Poisson regression analysis estimating prevalence ratios adjusted for age and housing status
Patterns of Substance Use Among People Who Use Drugs From Rural Regions Across the United States by Engagement in Sex Work in Prior 30 days (N=2041)
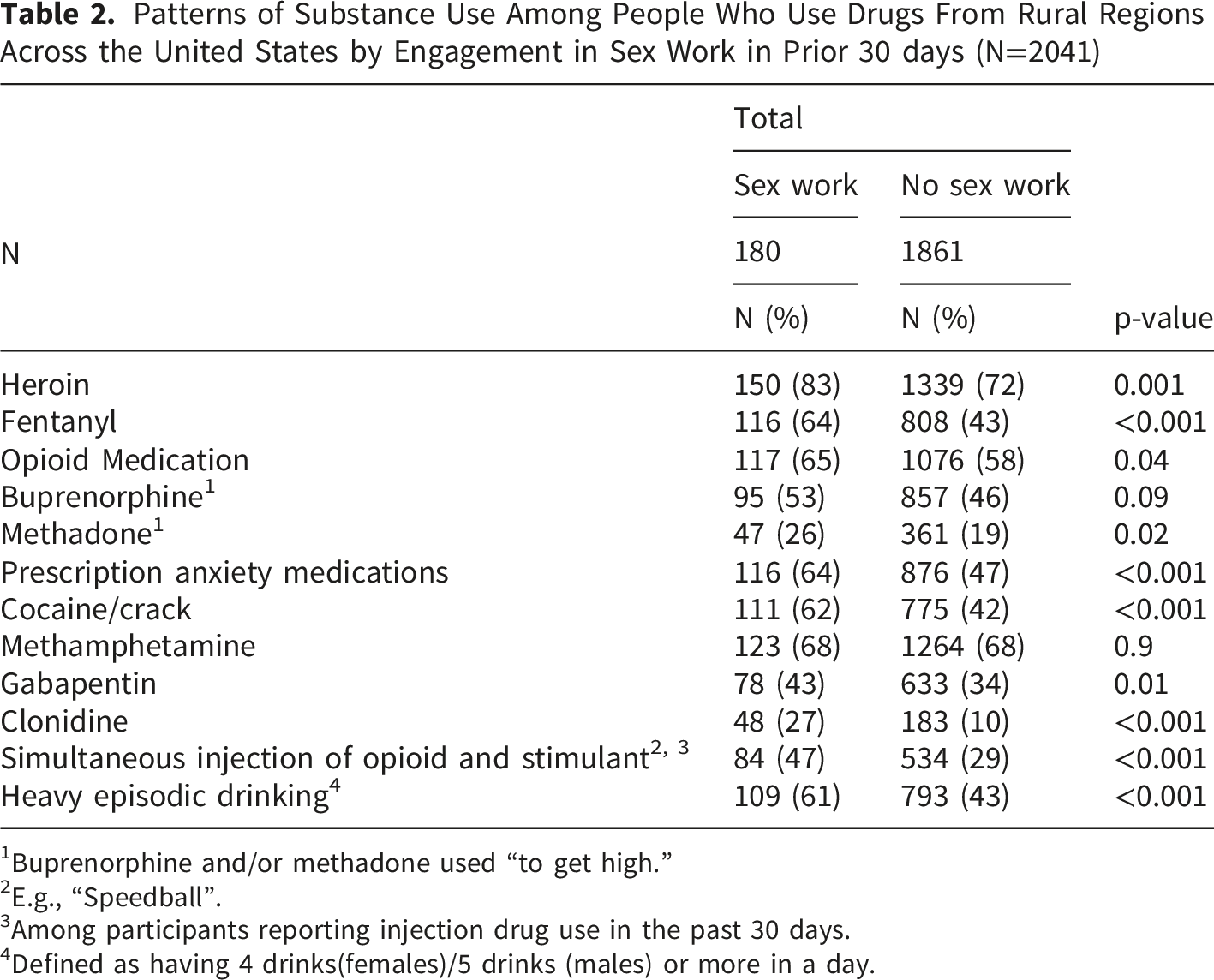
1Buprenorphine and/or methadone used “to get high.”
2E.g., “Speedball”.
3Among participants reporting injection drug use in the past 30 days.
4Defined as having 4 drinks(females)/5 drinks (males) or more in a day.
Injection Drug Use and Sexual Behaviors Associated With Hepatitis C Virus/HIV, Access to Harm Reduction Services, and Hepatitis C Virus Status Among People Who Use Drugs From Rural Regions Across the US by Engagement in Sex Work in Prior 30 days (N=2041)
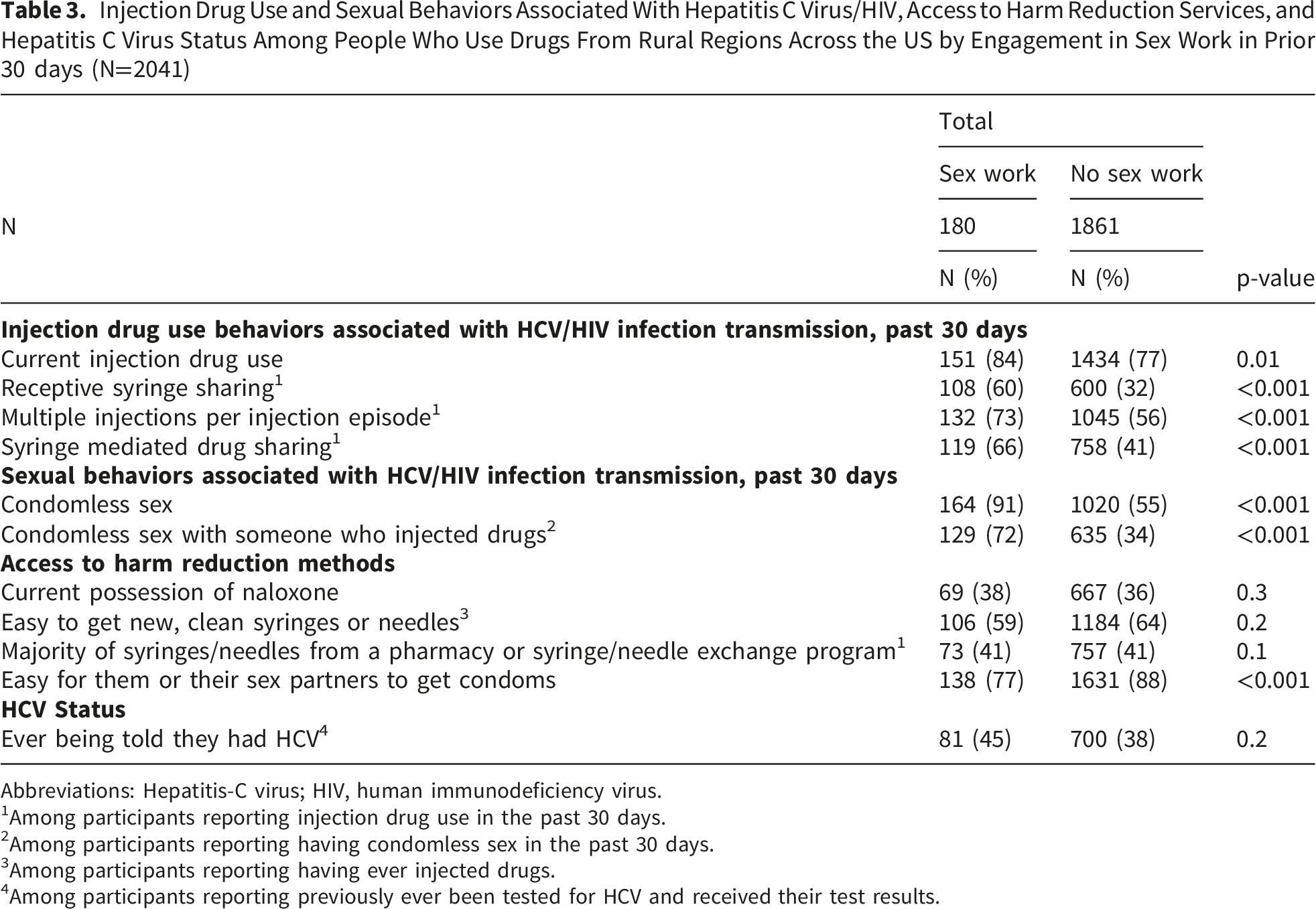
Abbreviations: Hepatitis-C virus; HIV, human immunodeficiency virus.
1Among participants reporting injection drug use in the past 30 days.
2Among participants reporting having condomless sex in the past 30 days.
3Among participants reporting having ever injected drugs.
4Among participants reporting previously ever been tested for HCV and received their test results.
Sex without a condom and sex with someone who injects substances without a condom, were more prevalent among participants engaged in sex work compared to those who were not (91% vs. 55% and 72% vs. 34%, respectively) (Table 3). Participants engaged and not engaged in sex work reported similar prevalences for a majority of their syringes/needles coming from a pharmacy or syringe/needle exchange program, (41% and 41%). More than half of participants engaged in sex work and participants not engaged in sex work reported it was easy to get new, clean syringes or needles (59% and 64%). Participants engaged in sex work also less frequently reported easy condom access for their partner(s) or themselves (77% and 88%). PWUD who sell sex had a higher prevalence of ever being told they tested positive for HCV (45% vs. 38%) (Table 3).
Multivariable Prevalence Ratio Regression Associations by Engagement With Sex Work and Outcomes of Interest, Adjusting for Age Among Participants in the Rural Opioid Initiative Who Self-Reported Their Engagement With Sex Work in the Past 30 days (Reference: Participants Who did Not Engage in Sex Work) 1
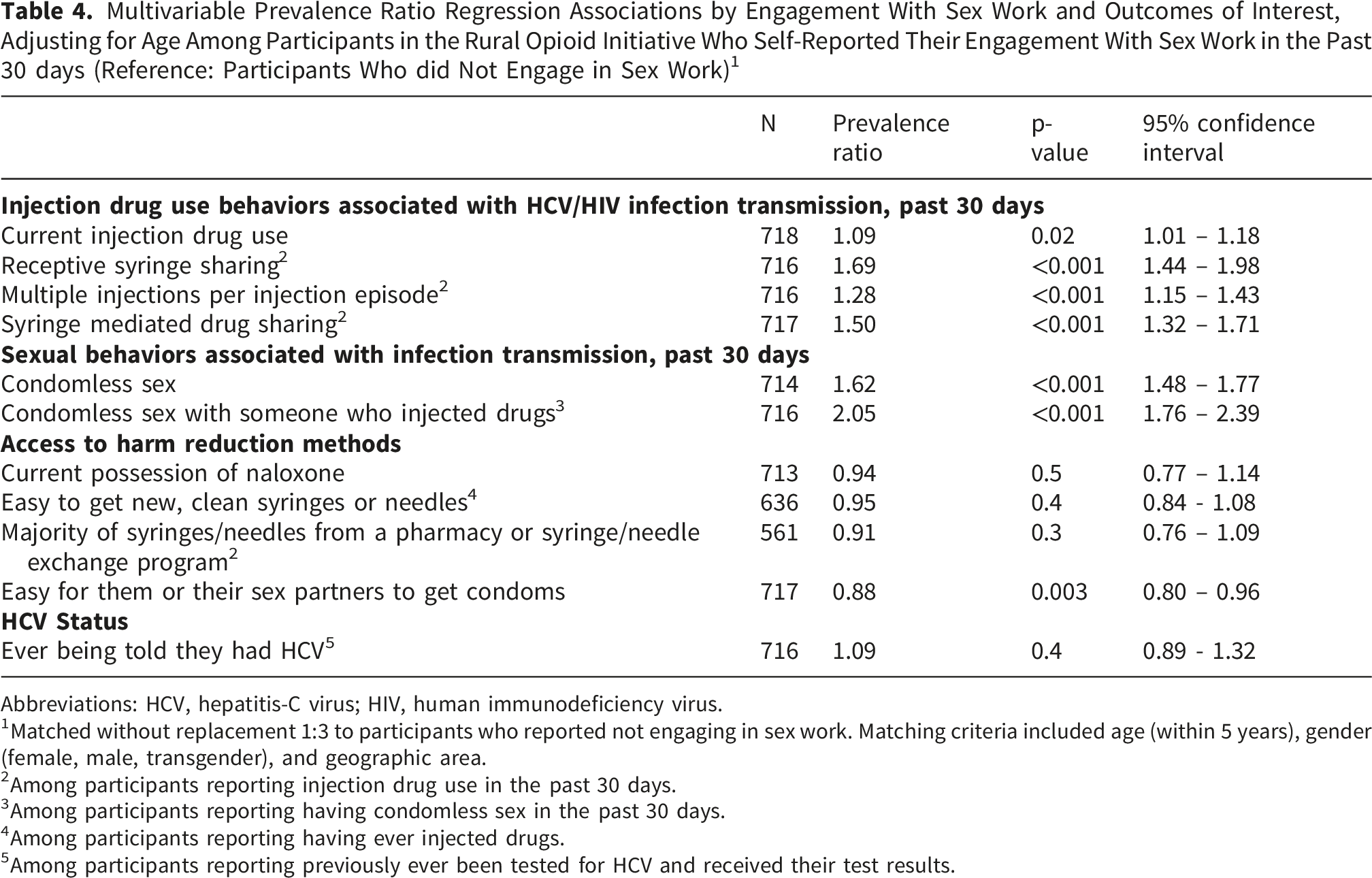
Abbreviations: HCV, hepatitis-C virus; HIV, human immunodeficiency virus.
1Matched without replacement 1:3 to participants who reported not engaging in sex work. Matching criteria included age (within 5 years), gender (female, male, transgender), and geographic area.
2Among participants reporting injection drug use in the past 30 days.
3Among participants reporting having condomless sex in the past 30 days.
4Among participants reporting having ever injected drugs.
5Among participants reporting previously ever been tested for HCV and received their test results.
Multivariable Prevalence Ratio Regression Associations by Engagement With Sex Work and Outcomes of Interest, Adjusting for Age Among Participants in the Rural Opioid Initiative Who Self-Reported Their Engagement With Sex Work in the Past 30 days and Reported Injection Drug Use in the Past 30 days (, Reference: Participants Who did Not Engage in Sex Work) 1
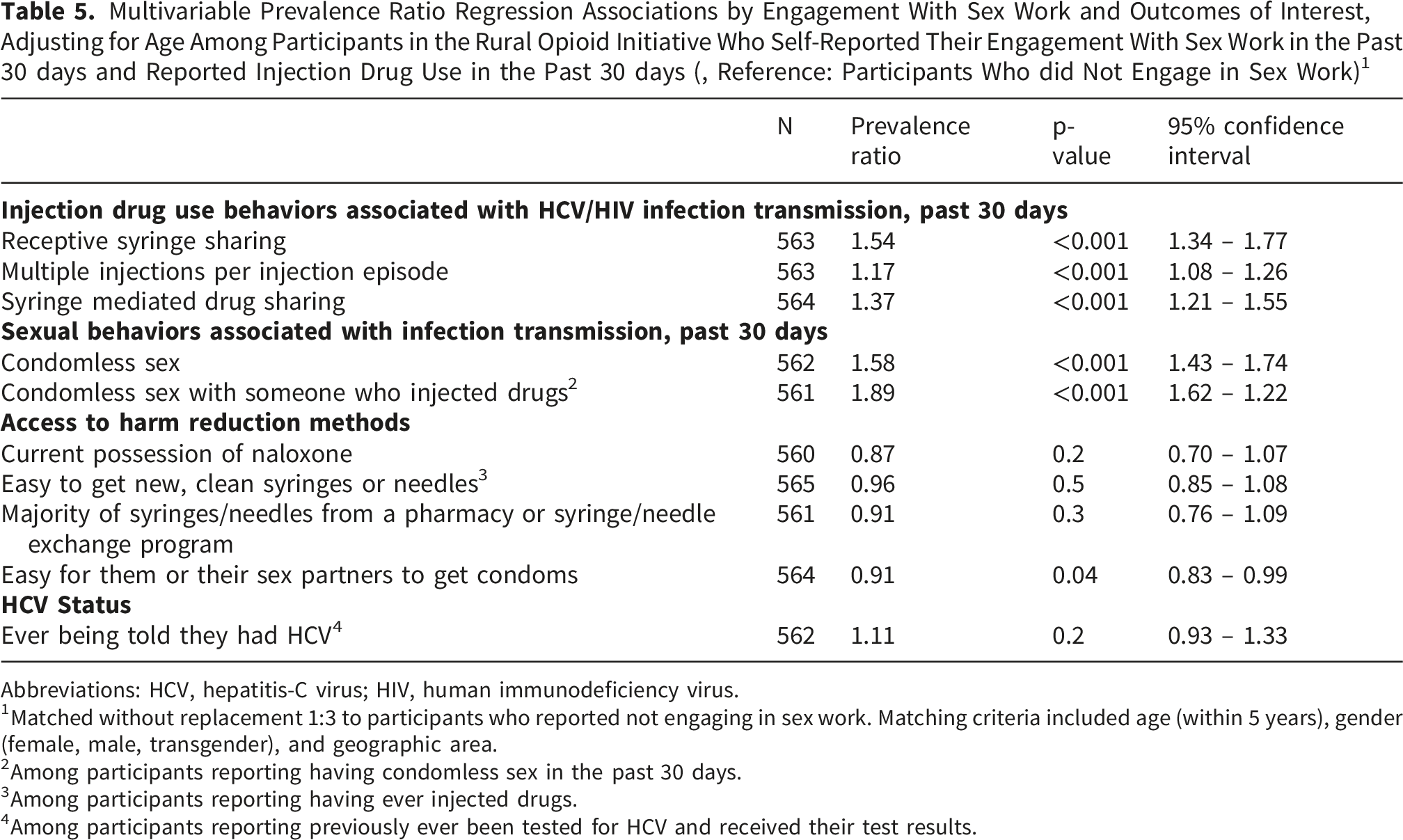
Abbreviations: HCV, hepatitis-C virus; HIV, human immunodeficiency virus.
1Matched without replacement 1:3 to participants who reported not engaging in sex work. Matching criteria included age (within 5 years), gender (female, male, transgender), and geographic area.
2Among participants reporting having condomless sex in the past 30 days.
3Among participants reporting having ever injected drugs.
4Among participants reporting previously ever been tested for HCV and received their test results.
Discussion
We investigated the complex interaction between engagement in sex work and various injection drug use and sexual behaviors among PWUD in rural settings, emphasizing how these overlapping risks manifest in rural communities. Our findings highlight the unique and nuanced challenges that this population faces. In this study, we found a notably high prevalence of male PWUD who sell sex. We also observed that engagement in sex work is associated with a higher likelihood of injection drug use practices, such as, receptive syringe sharing, practicing multiple injections per injection episode, and syringe mediated drug sharing, which elevate risk of HCV and HIV infection transmission. Additionally, we found that participants engaged in sex work in rural communities had more difficult access to condoms and were more likely to engage in condomless sex. These results highlight the need for targeted interventions in rural settings that address both structural and individual factors that contribute to these elevated risks in the rural setting.
ROI participants engaged in sex work had 12% lower prevalence ratio of perceiving it easy for themselves or their partners to access condoms, compared to PWUD who did not engage in sex work. This is echoed by our findings that participants engaged in sex work in rural communities had 62% higher prevalence ratio of having condomless sex and an over two-fold higher prevalence ratio of condomless sex with someone who injects drugs. Condomless sex increases the risk of various sexually transmitted infections (STIs) and blood-borne diseases, such as HIV; it is the most proximal risk for HIV acquisition among females who sell sex. 7 People who inject drugs (PWID) are at increased risk for HCV infection through contaminated needles and injection equipment. 42 PWID also are more likely to engage in condomless sex, placing them and their partners at higher risk of contracting and transmitting HIV and STIs. 43
There are many factors that may lead to having condomless sex, including consumption of alcohol and substance use. In our study population of PWUD who sell sex, the use of drugs at the time of sexual intercourse may affect their condom use. While some people who engage in sex work are also willing to take an increased risk and have condomless sex if their clients are willing to pay more money or provide drugs for the exchange, 29 others are forced into condomless sex through client physical threats and coercion. 44 Another potential reason for condomless sex is to prevent the submission of condom use as evidence of sex work by law enforcement. 45 The common and widespread practice of confiscating condoms from individuals as evidence of sex work puts these sex work engaged individuals at increased risk of condomless sex. 45 Other factors leading to condomless sex among people who sell sex include: the lack of legal protection for sex work, the extreme social isolation, and the lack of community support. 44 While we have listed many reasons a sex work engaged individual may not use a condom during sex, our findings that people who sell sex or their partners also had a lower prevalence ratio of easily attaining condoms may be an additional barrier to condom use.
Previous studies have found the cost of condoms to be a barrier to access and people who sell sex used condoms consistently when condoms were available and affordable.26,46 We found no association in our study population between sex work engaged participants and reporting it was easy for them to access syringes or a majority of their syringes/needles coming from a pharmacy or syringe/needle exchange program in our adjusted models. Additionally, 59% of our study population who sell sex affirmed it was easy for them to get clean syringes and 41% self-reported a majority of their syringes/needles came from a pharmacy or syringe/needle exchange program. For these reasons, a clear point of access for condoms would be at locations where clean syringes/needles are dispensed (i.e. pharmacies and syringe/needle exchange programs). As the majority of our study population of PWUD who sell sex also currently injects drugs (84%), this would give PWID the opportunity to easily obtain condoms when they obtain their clean syringes/needles. Efforts to improve access to condoms within the context of sex work in rural communities, especially amongst PWUD are essential for reducing the risk of HIV and STIs within this population. However, the power and consent imbalances often found in the sex work industry may contribute to the lack of access to condoms that the person engaging in sex work experiences, as well as the customer purchasing the act of sex may coerce individuals engaged in sex work.47,48
In our study of PWUD, we also found higher prevalence ratio for people who sell sex to engage in injection behaviors associated with high risk for HCV/HIV infection transmission, including receptive syringe sharing, using multiple injections per injection episode, and practicing syringe mediated drug sharing, compared to people who are not engaged in sex work. Sex work is associated with substance use severity, meanwhile, substance use severity is positively associated with injection drug use.34,49,50 We found that within our population, ROI participants who engaged in sex work had nearly 70% higher prevalence ratio of receptive syringe sharing. There are many factors that may lead someone to practice receptive syringe sharing, including byproducts of the power imbalance found between the person engaged in sex work and their client/partner, such as client-based violence 27 and being injected by others. 27 This power dynamic may also include differing access to drug-related activity knowledge, i.e., injection practices.27,51 If the participant engaged in sex work lacks the confidence or knowledge to self-inject, they may resort to being injected by others as a form of harm reduction. 27 However, the practice of allowing someone else to inject you increases your likelihood to practice receptive syringe sharing, 27 thus increasing the risk of infection transmission. 52 Some sex work engaged participants may also feel pressure to engage in receptive syringe sharing to build relationship intimacy.53,54 Intimate partner injection drug use and using substances with a sexual partner is also associated with increased odds of receptive syringe sharing. 55
Additional studies have found that syringe sharing is associated with experiencing houselessness56,57 and availability of syringes/needles.56,58 Both men and women report syringe sharing, though women may be at greater odds to engage in receptive syringe sharing. 59 These previous findings may explain why PWUD who sell sex in our study population have higher likelihood of receptive syringe sharing, since most participants in our study population are women and experienced houselessness in the past 6 months.
We also found a higher prevalence ratio of syringe mediated drug sharing in our study population. Syringe mediated drug sharing, the act of sharing a syringe to prepare and divide substances, is common among PWID(60). PWID commonly pool resources to purchase substances which promotes syringe mediated drug sharing. 60 Syringe mediated drug sharing has become an increasingly important route of blood-borne disease transmission, including HCV and HIV through contaminated syringes. 61 In our study, people who sell sex had over 50% higher likelihood of practicing syringe mediated drug sharing, compared to people who did not sell sex.
In addition, we found people who sell sex had a 28% higher prevalence ratio of practicing multiple injections per injection episode. Multiple injections per injection episode is often found in the context of sharing drugs and injection equipment, which increases the risk of HCV and HIV transmission.62,63 Multiple injections per injection episode also increases the risk of injection-related complications, such as soft tissue bacterial infections and acute sepsis.62-66 Overall, we found that our study participants of people who sell sex have higher likelihood of engaging in injection behaviors associated with high risk for infection transmission, suggesting a heightened risk of blood-borne infections.
Although we did not observe differences in access to naloxone or clean syringes/needles, we identified substantial differences in injection and sexual risk behaviors. This highlights an important gap between access to harm reduction supplies and implementation of use. While individuals may report that resources were available, the ability for individuals to utilize these resources may be influenced by interpersonal, structural, and situational factors. Many people engaged in sex work experience violence from clients, law enforcement, romantic partners, and others, which are further exacerbated by stigma and criminalization of both sex work and substance use.8,67 The violence and power imbalances make it difficult for people engaged in sex work to assert control over their working conditions, negotiate safer sex or substance use practices, or to seek help when necessary.48,68-72 These findings may suggest that interventions that focus solely on improving access may be insufficient in addressing high risk injection and sexual risk behaviors without also addressing the contextual and relational factors that influence the use of accessed harm reduction supplies.
As noted previously, our study had markedly high prevalence of males engaged in sex work, 42%. This is notable as research related to people engaged in sex work is predominantly on females engaged in street-based sex work in urban areas. Men who engage in sex work may experience different risk environments from women, including differences in partner types, substance use, and barriers to accessing harm reduction services and health care. 73 In rural areas, sex work may be characterized by more informal and transactional exchanges, 74 which further underrecognizes men in rural areas engaged in sex work within research. These findings highlight the need for future research that is focused on gendered differences amongst PWUD and engage in sex work in rural areas in order to identify tailored interventions to address unique challenges experienced by men who sell sex in the rural US.
Our findings in a rural population are consistent with prior studies on sex work in urban settings demonstrating elevated injection and sexual risk behaviors among PWUD and engage in sex work. 33 However, these risks are exacerbated by the unique structural and interpersonal factors present within rural communities. For example, compared to urban areas, rural communities have fewer harm reduction services, with 30% of urban counties having a syringe service program compared to only 12% of rural counties. 75 This highlights a substantial disparity to access for harm reduction services, which may contribute to a higher reliance on syringe sharing and other higher risk substance use practices, such as sharing used supplies and syringe mediated drug sharing. Even within counties with syringe service programs, rural communities face transportation barriers and longer distances traveled to these services, 76 which may impede consistent access to harm reduction supplies, such as condoms and sterile syringes. Finally, rural PWUD who sell sex experience heightened levels of stigma, which are further compounded by reduced anonymity and limited provider options, 19 which affects the access to timely and consistent health care. These factors, alongside other structural factors such as poverty and limited economic opportunities, uniquely affect rural areas and promote sustained elevated risk for adverse health outcomes among PWUD and sell sex within these communities.
There is no specific guidance as to how to provide services for PWUD who sell sex. 77 The most commonly suggested interventions for people who sell sex are HIV prevention-based and very few interventions incorporate the individual’s substance use. 78 Providing interventions that targeted structural changes (i.e. harm reduction, empowerment to practice safer sex, access to sex work specific health services), in addition to individual changes (i.e. substance use counseling), were more successful than programs that targeted individual changes alone. 78 Integrated services that provide resources and treatment for PWUD who sell sex will be crucial to combat morbidity and mortality within the opioid overdose epidemic in the US(17). These services should also work to address the violence perpetrated on to people engaged in sex work and the power imbalances they often face. In addition, fostering collaboration between healthcare providers, social workers, and community organizations is vital for establishing holistic support systems that prioritize the well-being and autonomy of PWUD who engage in sex work. Furthermore, it will be necessary to address the barriers attributed to accessing existing services, such as stigma and criminalization practices surrounding both substance use and sex work, which further marginalize this population. By addressing both the structural and individual needs of PWUD who sell sex, communities can provide comprehensive assistance to address the full spectrum of challenges faced by this unique population.
Limitations & Strengths
The findings of this study should be considered within the context of several potential limitations. The study was a cross-sectional secondary analysis, which precludes the use of a priori power calculations for sample size. 79 Participants may have underreported their engagement in sex work due to widespread stigma. The question assessing a participant’s engagement in sex work does not let us parse whether the exchange should be considered sex work or transactional sex. We elected to use the term ‘sex work’ to maintain clarity and alignment with existing literature.80,81 Additionally, this question is limited to in-person, physical sex work and excludes online/platform-based sex work (e.g., camming, content creation). There was not a high enough prevalence of HIV among ROI participants to include HIV as an outcome in our analysis. The exclusion of participants from WI could affect the representativeness of these findings in Midwest areas. Furthermore, the cross-sectional study design prohibits causal inference. Additionally, we did not assess patterns of polysubstance use or co-use of substances which may influence associations between sex work engagement and risk behaviors. While frequency questions are commonly used in substance use research82-87 and several ROI questionnaire items were adapted from established instruments, the ROI specific questions were adapted as part of a rapid epidemiological assessment, thus not specifically pilot tested.
Finally, the question assessing access to condoms stated, “it’s easy for me and my sex partners to get condoms,” which introduces the possibility that responses are not limited to people engaging in sex work and may also include their partner(s). Additionally, people who sell sex may not have knowledge about their clients’ access to condoms and given that sex work may involve multiple partners with differing levels of access, responses may reflect a generalized perception, rather than partner-specific observations.
Despite these limitations, our study possesses several key strengths. First, the large sample size of PWUD who engage in sex work in rural areas provides robust data on a population that is understudied. Additionally, the ROI cohort represents a broad geographic scope through data collection from multiple geographic areas. This study provides rich data on injection drug use and sexual behaviors associated with HCV/HIV infection transmission, access to harm reduction methods, and HCV status in the context of the opioid overdose epidemic, which is an area of critical importance for public health concerns in the rural US. These findings also support several opportunities for future work. Longitudinal data could provide valuable insight into changes in injection drug use behaviors, sexual practices, and access to harm reduction services over time, which could be utilized for intervention development and evaluation. Ecological momentary assessment approaches could be used to better characterize the dynamic risk environment experienced by PWUD who engage in sex work, while reducing recall bias. Assessment of frequency and intensity of engagement in sex work may differentially influence risk and should be studied further. Additionally, a better understanding of other factors that are related to sex work, such as social determinants of health, including gender disparities, stigma, policing practices, and resource availability, may have significant downstream impacts on overall health outcomes and harm reduction utilization in future investigation.
Conclusion
In conclusion, our study found that PWUD who sell sex in the rural US have a higher likelihood of injection drug use and sexual behaviors associated with HCV/HIV infection transmission, while having lower access to condoms. Most notably this study emphasizes the importance of ensuring affordable access to condoms within the context of harm reduction services, such as syringe service programs, especially given the limited access to health care, harm reduction infrastructure, and supportive services in rural communities. In addition, the results of this study emphasize the importance of a holistic harm reduction intervention to help address both substance use and sex work among PWUD who sell sex. We also acknowledge the power imbalance that is present within the context of sex work that likely affects the ability of PWUD engaged in sex work to be fully autonomous of their decisions. These findings uniquely describe the complex intersection between PWUD and people who engage in sex work in the rural US, an area that is vastly understudied amongst a community that faces unique challenges due to complex systemic barriers.
Supplemental Material
Supplemental Material - Injection Drug Use and Sexual Behaviors Associated With Infection Transmission and Access to Harm Reduction for People Who Use Drugs and Sell Sex in the Rural US
Supplemental Material for Injection Drug Use and Sexual Behaviors Associated With Infection Transmission and Access to Harm Reduction for People Who Use Drugs and Sell Sex in the Rural US by L. Sarah Mixson, April M. Young, Judith I. Tsui, Wiley D. Jenkins, Mai T. Pho, David W. Seal, Lydia N. Drumright, Stephanie A. Ruderman, Thomas J. Stopka, P. Todd Korthuis, Bridget M. Whitney, Peter D. Friedmann, Ryan P. Westergaard, Vivian F. Go, William C. Miller, Dalia Khoury, Judith Feinberg, Gordon Smith, Hannah L.F. Cooper, Joseph A. Delaney, Heidi M. Crane in Substance Use: Research and Treatment
Footnotes
Acknowledgement
The authors thank the other ROI investigators and their teams, the ROI Executive Steering Committee chair, Dr. Holly Hagan, the NIDA Science Officer, Dr. Richard Jenkins, and particularly, the participants of the individual ROI studies for their valuable contributions. A full list of participating ROI investigators and institutions can be found on the ROI website at ![]() .
.
Ethical Considerations
All studies obtained local institutional review board approval for research activities and data sharing within the ROI. Illinois: Biological Sciences Division/University of Chicago Medical Center Institutional Review Boards (UC:IRB17-1630), Kentucky: University of Kentucky Research – Office of Research Integrity Institutional Review Board (43520), Ohio: Ohio State Office of Research Institutional Review Board (2017B0328), Oregon: Oregon Health Sciences University Institutional Review Board (STUDY00017233), North Carolina: RTI International Institutional Review Board ((Internal RTI IRB): CR00000959) and Advarra Institutional Review Board ((external Advarra IRB): Pro00050894), New England: Bayside Medical Human Research Protection Program Institutional Review Board (UH3DA044830), Wisconsin: University of Wisconsin-Madison Human Research Protection Program Institutional Review Board (2017-0866), West Virginia: West Virginia University - Office of Research Integrity and Compliance (1707651279).
Consent to Participate
All ROI study participants provided written consent before administration of the questionnaire.
Authors Contributions
LSM, LND, JIT, HMC, JAD were involved in the conceptualization of the research goals and aims. LSM, JAD were involved in the formal analysis. BMW was involved in the data curation. MTP, WDJ, RPW, DWS, VFG, WCM, WCZ, PTK, PDF, TJS, JF, GS, HLFC, AMY, JIT, HMC were involved in funding acquisition. MTP, WDJ, RPW, DWS, VFG, WCM, WCZ, PTK, PDF, TJS, JF, GS, HLFC, AMY were involved in conducting research investigation. BMW, JIT, HMC, JAD were involved in supervision of research planning activities. LSM, JAD were involved in the development of methodology design. LSM was responsible for the original draft of the manuscript. All authors were involved in reviewing and editing the manuscript. All authors gave meaningful input on the manuscript. All authors have approved of the final article.
Funding
This publication is based upon data collected and/or methods developed as part of the Rural Opioid Initiative (ROI), a multi-study cohort with a common protocol which was developed collaboratively by investigators at eight research institutions and at the National Institute of Drug Abuse (NIDA), the Appalachian Regional Commission (ARC), the Centers for Disease Control and Prevention (CDC), and the Substance Abuse and Mental Health Services Administration (SAMHSA). Research presented in this publication is the result of secondary data harmonization and analysis and supported by grant U24DA048538 from NIDA. Primary data collection was supported by grants UG3DA044829, UG3DA044798, UG3DA044830, UG3DA044823, UG3DA044822, UG3DA044831, UG3DA044825, UG3DA044826, U24DA044801, UH3DA044829, UH3DA044798, UH3DA044830, UH3DA044823, UH3DA044822, UH3DA044831, and UH3DA044826 co-funded by NIDA, ARC, CDC, and SAMHSA. This project was supported by grant number T32DA057920 from the National Institute on Drug Abuse. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.