
Abstract
Intro
Kratom use is growing for both therapeutic and non-therapeutic effects. This survey assessed the temporal relationship between kratom initiation and prior, subsequent, or concurrent substance use or medical treatment.
Methods
This cross-sectional, anonymous electronic survey was disseminated to American Kratom Association and Global Kratom Coalition members from 3/2025-9/2025. Adults aged ≥18 years who reported past or current kratom use were eligible. A novel questionnaire was generated assessing: kratom and other substance use characteristics; pursuit of medical treatment for selected diagnoses; and temporal relationships between kratom use and substance use or medical treatment.
Results
Of 161 respondents included, most (95.7%) currently versus previously used kratom. Whole-leaf product use was reported most often (90.3%), with 38.3% reporting concentrated kratom extracts and 16.9% single alkaloid isolates. Reasons for kratom use were therapeutic (50.3%), non-therapeutic (16.1%), or both (33.5%). Therapeutic (self-treatment) use was most commonly cited for pain (86.2%), mental focus (52.3%), mental health (46.9%), sleep (43.1%), and substance use disorder (27.7%). Most respondents had used ≥1 other psychoactive substance in their lifetime, including cannabis (74.3%), alcohol (68.2%), stimulants (43.2%), sedatives (33.1%), non-prescribed opioids (26.4%), or tobacco (6.1%); 10.1% reported no prior substance use besides kratom. Whether used for non-therapeutic or therapeutic purposes, kratom was rarely initiated first. Among those with a substance use history, only 3-10% reported trying kratom prior to other substances reported. Among those with pertinent medical conditions, 0-20% initiated kratom before receiving medical care for their reported conditions.
Conclusion
This study builds on previous research assessing kratom use motivations, providing insight into the temporal relationship between kratom initiation and substance use or medical treatment. Kratom was rarely the first substance or therapeutic treatment tried, but rather most individuals initiated it concurrently with or after discontinuing other substances or medical care. Larger follow-up studies are warranted to confirm these results.
Introduction
Kratom (Mitragyna speciosa Korth., Rubiaceae) is a tree native to Southeast Asia whose leaves have been used for centuries as an herbal medicine due to its opioidergic, adrenergic, and serotonergic pharmacologic activity and reported stimulant and opioid-like effects. 1 Over the past decade, kratom availability and use have greatly increased in the United States (US), with estimated lifetime use prevalence as high as 9% among US adults.2-5 Prevalence is higher among those with substance use disorders (SUD), with past-year and lifetime use up to 10 and 21%, respectively. 6
In the US, kratom is not legally marketed as a drug product, dietary supplement, or food additive, but is instead designated as a new dietary ingredient with limited regulatory oversight. 7 It is now sold in many smoke shops, increasingly available at gas stations and bodegas, and readily available online.8,9 Reasons for kratom use vary, including: (1) to self-treat pain, SUD and drug withdrawal, and mental health conditions; (2) to enhance energy or focus; or (3) to achieve euphoric effects.10,11 Though anecdotal reports indicate it may provide some relief of these conditions, clinical evidence demonstrating these purported benefits is limited. 12 Kratom use carries risks of adverse effects (including nausea, constipation, somnolence, confusion, agitation, hypertension, and tachycardia), dependence, and overdose, particularly if used with other substances.10,13 This risk/benefit ratio is further complicated by a lack of product regulation, oversight, and good manufacturing practice requirements. Additionally, the development of increasingly diverse product formulations and semi-synthetic derivatives containing high concentrations of active alkaloids like mitragynine, 7-hydroxymitragynine, and mitragynine pseudoindoxyl, may increase risk potential. 1
While a growing body of evidence has begun to better characterize the reasons people use kratom,14-18 it is less clear what motivates people to initially try kratom versus seeking alternative options. Individuals may use kratom as a substitute or adjunct to pharmacotherapy and other treatment modalities when standard care is inaccessible or ineffective.19-21 They may view kratom as a “natural” alternative to Western medicine, 22 or as an accessible psychotropic substance sold legally in most US states. 23 Several questions remain regarding the motivations for kratom use and its relationship to conventional treatments and other substance use. For those individuals using it for therapeutic effects, do they first try kratom before seeking conventional medical treatment or as an adjunct/alternative when those options are not adequately providing relief? Similarly, for those using it for non-therapeutic effects, do individuals typically use kratom prior to, concurrently with, or after discontinuing use of other substances and why? This survey was conducted to investigate these temporal relationships and the factors driving kratom initiation.
Methods
Study Goals
The primary goal of this study was to gain insight into whether adults who use kratom typically initiate use before, during or after the use of other psychoactive substances (if using it for non-therapeutic reasons) or before, during, or after their receipt of medical treatment for selected diagnoses (for those using it for therapeutic reasons). Additional goals included assessing types of kratom used, reasons and motivations for kratom use, whether individuals informed their healthcare professionals (HCPs) of their kratom use, and opinions on the relative safety of kratom compared with Western medicine approaches.
Study Design and Data Collection
This cross-sectional study using convenience sampling consisted of an electronic survey of adults who use kratom. An electronic Qualtrics® (Provo, UT) survey link was disseminated to members of the American Kratom Association and the Global Kratom Coalition via member email lists of each organization. Multiple survey offers were provided, with approaches to prevent ‘ballot stuffing’ embedded in the survey design. Given the nature of the sampling frame, a specific response rate was not able to be calculated. Participation was voluntary and anonymous. No financial incentives were offered for participation. Inclusion criteria included adults 18 years and older who reported kratom use currently or at any point in the past. Screening was accomplished by providing electronic, written consent information and a 3-item screening questionnaire at the beginning of the survey. Survey participation was voluntary and the survey could be ended at any time. After viewing the consent information provided on the first page of the electronic survey, completion of the survey was considered implied consent. Persons who were under 18 years old, reported no kratom use history, or chose to opt out of the survey after reading the consent information were excluded. Surveys were collected from March through September 2025. Based on previous research estimating a lifetime prevalence of kratom use across the US adult population, 3 a 95% confidence level, and a 5% margin of error, a sample size of 385 was targeted.
Questionnaire Development and Description
Minimal research into this topic had been previously published (with a lack of existing validated questionnaires), so the investigators developed a novel survey tool for this investigation informed by previous research3,18,24,25 and subject matter expertise. The questionnaire (Supplemental Appendix) consisted of the following sections and items (dependent on survey logic): (1) reasons for kratom use (up to 3 items); (2) temporal trends of kratom with substance use (up to 12 items); (3) temporal trends of kratom with treatment for medical diagnoses (up to 13 items); and (4) demographics (7 items). Only selected substances and medical conditions were queried a priori in this survey, focusing on common substances and conditions that people may use kratom to self-treat. Question types included multiple choice, select all that apply, and free-response options to clarify “other” answer choices. The free responses were qualitatively categorized by the researchers and those described by more than one respondent were included in Supplemental Appendix. Response categories that were included based on free-response data are indicated in these appendixes. Several rounds of pilot testing with both healthcare professionals and people who use kratom were conducted, and the survey was edited based on this feedback.
Statistical Analysis
Anonymized data was exported from Qualtrics® into Microsoft Excel® (Redmond, WA) and IBM SPSS® (Chicago, IL) for data cleaning, standardization, and statistical analysis. All variables underwent basic descriptive analysis, with counts and percentages calculated for the nominal variables fully composing the questionnaire. Stratifications for the data included: (1) temporal relationships of kratom use to individual substances; and (2) temporary relationships of kratom use to individual medical conditions. Respondents were not required to answer all questions to complete the survey and skip logic was employed within the survey to exclude certain non-relevant questions based on previous responses, so the respondent denominators are not equal for all questions. Missing data were identified in tables categorically. Comparisons among stratifications were conducted using Chi-square tests/Fisher’s exact tests with an ɑ = 0.05.
This study was deemed Exempt Research by the University of Texas Health San Antonio institutional review board (protocol 00001351). Survey data was completely anonymous. The Checklist for Reporting of Survey Studies (CROSS) was used for reporting purposes. 26
Results
Sample Demographics and Characteristics
Sample Demographics and Characteristics (n=161)
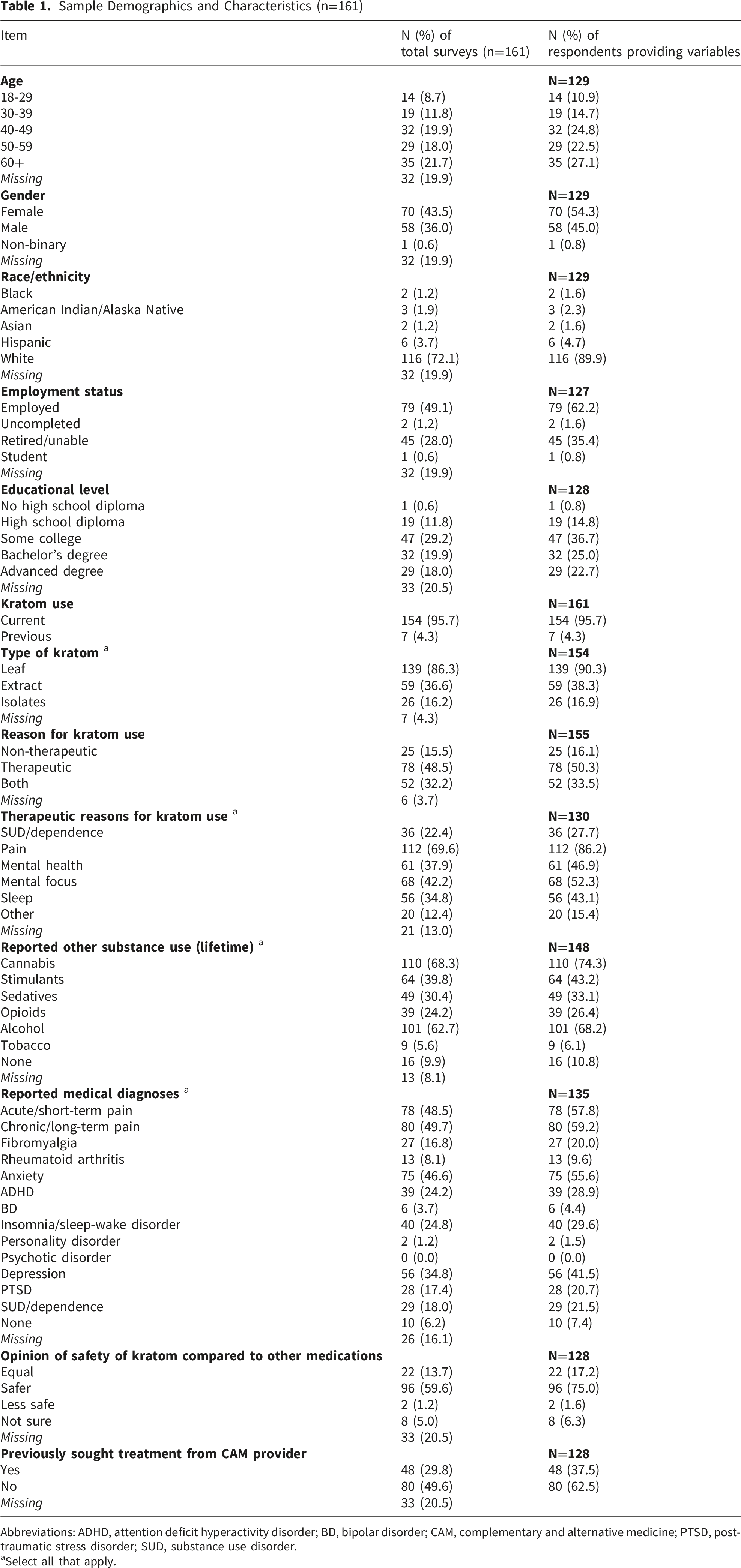
Abbreviations: ADHD, attention deficit hyperactivity disorder; BD, bipolar disorder; CAM, complementary and alternative medicine; PTSD, post-traumatic stress disorder; SUD, substance use disorder.
aSelect all that apply.
Most survey respondents reported multiple pertinent medical diagnoses, including acute or chronic pain, anxiety, depression, and attention deficit hyperactivity disorder (ADHD) in at least one-quarter of respondents. Only a small minority (<10%) did not report being diagnosed with at least one of the medical conditions included in the survey. In the past year, 136 respondents (84.5%) reported having seen an HCP at least once, including for a general wellness check (96; 59.6%), for pain management (41; 25.5%), for a physical health condition (51; 31.7%), or for a mental health condition (34; 21.1%).
Almost all respondents reported current kratom use. Most used kratom leaf products (e.g., dried kratom powder, capsules or tablets) followed by kratom extract products (e.g., kratom leaf material that contains higher levels of mitragynine or other alkaloids) and kratom isolates or single alkaloids (e.g., isolated mitragynine, 7-hydroxymitragynine, or mitragynine pseudoindoxyl). No consistent relationships between specific kratom type used and demographics or primary outcomes were observed.
Reasons for kratom use included therapeutic (50.3%), non-therapeutic (16.1%), or both (33.5%). Therapeutic use was most commonly reported for pain, mental focus, mental health, sleep, and SUD. Most respondents had used at least one other substance with misuse potential in their lifetime, most commonly cannabis, alcohol, stimulants, sedatives, opioids, or tobacco, with 10.1% reporting no prior substance use besides kratom. Nearly one in five respondents reported having a past or current SUD (either diagnosed by an HCP or self-diagnosed), related to alcohol (62.1%), opioids (51.7%), tobacco (31.1%), stimulants (20.7%), cannabis (20.7%), and sedatives (10.3%).
Relationship of Kratom to Other Substance Use
Temporal Relationship of Kratom to Other Substances
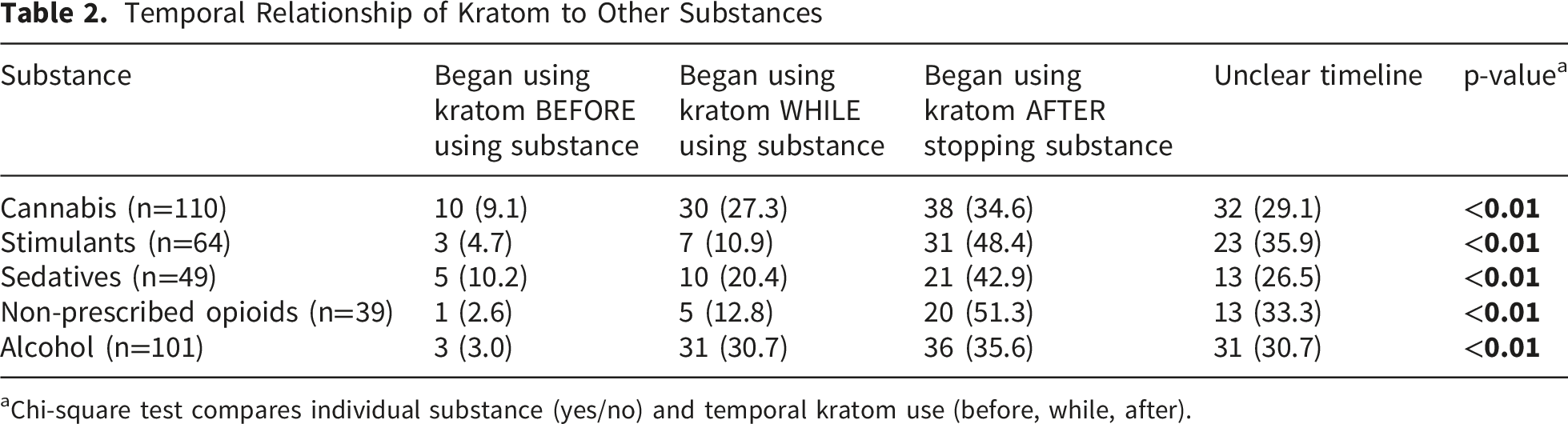
aChi-square test compares individual substance (yes/no) and temporal kratom use (before, while, after).
Respondents’ reasons for using kratom either concurrently with or after stopping other psychoactive substances are provided in the Supplemental Appendices. In both cases, initiating kratom use was often unrelated to their other substance use (e.g., they used the substances for different reasons). “Trying to quit”, “trying to cut down”, or “managing withdrawal” were among the most commonly reported reasons for using kratom concurrently with other substances and “reducing cravings” and “managing withdrawal” were among the most commonly reported reasons for initiating kratom after stopping other substances (specifically for stimulants, sedatives, non-prescribed opioids, and alcohol). However, a somewhat different relationship was observed between cannabis and kratom with regards to reasons for initiating kratom after stopping cannabis. With regards to cannabis, respondents were less likely to report initiating kratom to manage cravings or withdrawal than they were to report reasons related to preferring kratom (e.g., did not find cannabis effective or like its adverse effects). With the exception of alcohol, another reason noted for initiating kratom after stopping another substance was losing access to the other substance; this was reported by 8-14% of respondents, depending on the substance.
Relationship of Kratom to Medical Treatments
Temporal Relationship of Kratom to Treatment for Medical Conditions

Abbreviations: ADHD, attention deficit hyperactivity disorder; BD, bipolar disorder; PTSD, post-traumatic stress disorder; SUD, substance use disorder.
aPercentages are based on denominator of those diagnosed with condition.
bPercentages are based on denominator of those who received medical treatment for the condition.
cChi-square test compares individual medical condition (yes/no) and temporal kratom use (before, while, after).
Reasons for Initiating Kratom in Addition to or After Medical Treatment
The most common reasons respondents reported for initiating kratom concurrently with medical treatments from an HCP included feeling that: kratom was safer (55.6%); kratom was more effective (46.3%); their medical treatment was partially (42.6%) or not (29.6%) working; they experienced adverse effects related to their medical treatment (35.2%); they desired to use less of their prescribed medication (25.9%); their HCP did not offer treatment (5.56%); and other (18.5%). Among respondents reporting that they used kratom while receiving medical treatment from an HCP, 46% disclosed their kratom use to their HCP, with 33.3% continuing both kratom and medical treatment from their HCP, 51.9% discontinuing their treatment from their HCP and only using kratom, and 3.7% discontinuing kratom and continuing their medical treatment (7.4% did not endorse any of these options).
Among respondents who initiated kratom after discontinuing treatment from their HCP, the reasons for discontinuing that treatment included: preference for a natural or holistic treatment (56.5%); treatments did not help (30.4%); treatment costs (29.0%); lack of medical insurance (15.9%); opinions of others (8.7%); privacy concerns (7.3%); lack of time (5.8%); transportation barriers (4.4%); and other (26.1%).
Among 128 respondents who answered the question, 37.5% had previously sought treatment from a complimentary or alternative medicine (CAM) provider. Of these, 75% initiated CAM treatment prior to kratom use, 22.9% did so concurrently, and 2.1% sought CAM after discontinuing kratom. Respondents tended to believe that kratom was safer than (59.6%) or equally as safe (13.7%) as medications, with 5.0% unsure and 1.2% believing kratom was less safe.
Discussion
Among this sample of individuals who reported kratom use, whether for non-therapeutic/recreational or therapeutic/self-treatment purposes, kratom was rarely initiated prior to alternative treatments/substances. Those endorsing the use of other psychoactive substances typically initiated kratom after discontinuing the other substance(s) or while still using them. Only three respondents (1.9%) reported concurrent kratom use to enhance the effects of another substance, whereas previous research identified 14% using it in this manner. 24 Thus, despite its current non-controlled status and accessibility in the US, these findings do not suggest kratom is a common first psychoactive substance used or a “gateway” to other substance use. Instead, kratom appeared to more commonly be used as an adjunct or alternative to other psychoactive substances.
While some respondents indicated that their kratom use was largely unrelated to their other substance use, managing withdrawal, reducing cravings, cutting down or quitting their use of other substances, or losing access to another substance were all among the most commonly endorsed reasons for using kratom alongside or after discontinuing other substances. This is in line with previous research indicating that people more often use kratom to reduce their frequency of substance use or mitigate dependence and withdrawal from other substances.20,27 Given the opioid epidemic and opioid agonist effects of kratom, this has most often been studied in relation to opioid use disorder (OUD) and opioid sparing. Previous observational research identified that approximately 10-20% of people who used kratom did so to manage withdrawal or reduce opioid use, though this was observed at higher rates among people seeking SUD treatment. 28 In a study of individuals at a residential treatment facility, 69% of those who had used kratom did so to curtail their non-prescribed opioid use and 64% as a substitute for opioids. 20 While a relatively low number of respondents to this survey endorsed non-prescribed opioid use compared to other substances, 50% of those that endorsed previous opioid use indicated that they used kratom to reduce opioid cravings and 40% endorsed using it to manage opioid withdrawal. This was considerably more commonly reported with non-prescribed opioids than the other substances assessed, with the exception of alcohol which was similar. Previous observational research has also indicated that some individuals use kratom to help reduce alcohol or stimulant use or withdrawal symptoms. 6 In this survey, approximately half of those currently or previously using alcohol endorsed using kratom to help reduce/quit alcohol use or manage withdrawal, while approximately 10-20% reported the same for their stimulant use.
Cannabis was the most common substance use reported in this study, which has also been observed in previous kratom research. 25 This is not surprising given cannabis is the most used federally illegal drug in the US. As such, this finding may not necessarily be indicative of a link to kratom use. 29 Respondents who had discontinued cannabis use reported a variety of reasons for initiating kratom. While many reported their use of kratom and cannabis was unrelated or for different purposes, others noted not liking the side effects or the way cannabis made them feel, as well as no longer having access to cannabis or having concerns regarding the legal ramifications of its use. Thus, it seems that for some who have tried cannabis, kratom may be viewed as an alternative psychoactive substance preferred for its different effects, adverse effect profile, or legal status. A lower proportion cited using kratom to reduce cravings or manage withdrawal associated with cannabis than the other substances assessed in this study. Thus, it seems the relationship between kratom and cannabis use may be different than with opioids, stimulants, alcohol, or sedatives.
Similar patterns were observed among those endorsing pertinent medical conditions that kratom might be used to self-treat. Kratom was typically initiated concurrently with or after discontinuing medical treatment for those conditions. Given that this study and previous research have identified that kratom is most commonly used for therapeutic/self-treatment purposes, 12 these findings may indicate that ensuring people with underlying pain, substance use, and mental health conditions have access to effective treatments may reduce their desire to try kratom. Unfortunately, these conditions are often stigmatized and result in reduced access to care. Many patients with SUD do not receive treatment, despite effective medications available for opioid, alcohol, and tobacco use disorders.30,31 Perhaps not surprisingly, respondents reported initiating kratom prior to receiving SUD treatment more often than any other diagnosis included in this study. This was followed closely by pain, which is typically among the most cited therapeutic reasons for using kratom and is also a stigmatized condition in which many patients struggle to access effective treatments.10,12,24,32,33 In these cases, it is possible that kratom is an appealing option since it is available without a prescription. Kratom may be more affordable/accessible than traditional healthcare for those who are uninsured/underinsured, have other access barriers, or desire to avoid potentially stigmatizing healthcare interactions. Accordingly, lack of insurance, cost, and opinions of others were cited as reasons why some survey respondents stopped receiving treatment for their medical conditions from their HCP. This is in line with previous research assessing the temporal relationship between kratom use and medical care, which has identified that difficulty obtaining adequate treatment for mental health, pain, or SUD, as well as discrimination or stigma experienced within a healthcare setting, influenced individuals’ decision to try kratom.24,33 Conversely, research has shown that kratom use was less likely among people prescribed buprenorphine for opioid use disorder. 25
While the quality of and access to medical care may influence kratom use patterns, it is likely that some might continue kratom use because of a preference for CAM approaches or kratom specifically. In the present study, more than one-third of respondents indicated that they had previously sought treatment from CAM providers, and more than half noted they preferred natural/holistic treatments and felt kratom was safer than Western medicine. Furthermore, nearly a third of respondents discontinued their medical treatment because they felt it was ineffective and almost half of those initiating kratom in addition to their medical treatment did so because they felt kratom was more effective. Previous research has similarly indicated that people who use kratom generally believe it to be safe and relatively effective for self-treating various ailments. One study asked people who used kratom to rate the safety and effectiveness of kratom on a 100-point scale; respondents rated the perceived average safety as 90/100, while effectiveness ratings as an opioid, stimulant, or alcohol substitute or to manage withdrawal or depressive symptoms ranged from 67-76/100. 24 However, while anecdotal reports from people who use kratom indicate that it may provide some relief for various medical conditions, it is important to recognize that considerably more clinical research is needed to accurately assess its potential benefits and risks before it could be recommended for any medical treatment.6,12
This is particularly true given the rapidly changing kratom market. While it has been used for centuries in Southeast Asia as an herbal medicine, this use consisted of chewing or drinking tea from fresh kratom leaves. 1 These natural, whole-leaf kratom formulations contain relatively small amounts of the primary active alkaloid mitragynine, which acts as a weak partial agonist at the mu opioid receptors, and has activity at the adrenergic and serotonergic receptors. As its US popularity has grown, kratom product diversity has greatly expanded. Until recently, kratom has primarily been consumed in the US as dried leaves ingested as tablets, teas or powders, but it is now available as edibles, vapes, tinctures, liquid shots and other novel formulations and may be combined with additional active ingredients like kava.1,12 More concerningly, a number of semi-synthetic kratom derivatives have entered the market that contain much higher mitragynine levels or alkaloids like 7-hydroxymitragynine or mitragynine pseudoindoxyl, which are not found in detectable amounts in fresh, whole-leaf kratom. Unlike mitragynine, 7-hydroxymitragynine and mitragynine pseudoindoxyl function as potent opioid receptor agonists, thus profoundly changing the pharmacology and relative risk. 1 However, given that they are typically still marketed as kratom products, many consumers likely do not fully appreciate these differences or the inherent risks associated. In the present study, 38.3% of respondents reported using kratom extract products with higher concentrations of mitragynine and 16.9% reported using kratom products containing isolated mitragynine, 7-hydroxymitragynine, or mitragynine pseudoindoxyl. Not only are these products much more potent opioid receptor agonists, they are also under-regulated and under-studied and likely to confer considerable risks to those using them, particularly if they do not appreciate the differences in pharmacology or dosing. 1 Unfortunately, previous research has indicated that most people who use kratom do not identify it as an opioid or recognize that there is limited regulation to ensure consistency among products or that kratom products may be adulterated with other substances. 25 Thus, it was concerning that most respondents believed kratom was safer than medications, which have considerably greater research to support their safety and efficacy. This would seem to indicate that consumers likely underappreciate the risks associated with kratom use, particularly with regard to the newer, more potent products being used by more than one-third of the survey respondents.
Limitations
While this survey provided novel insights into when and why people initiate kratom, there were limitations to this study. To identify potential survey respondents, a nonprobability sampling technique was utilized, with research participation solicited by sharing the survey link with members of the American Kratom Association and the Global Kratom Coalition. Beyond sharing the survey link with their members, these organizations held no role in this study, and had no input on the study design, data analysis, or manuscript development. However, the sampling frame may have had a selection bias towards those who have had positive experiences with kratom, which could limit generalizability. Additionally, despite multiple attempts to solicit study participation, the targeted sample size was not met. No financial incentive was offered to complete this survey, which likely impacted study recruitment. While the top-line results displayed that a considerable minority initiated kratom prior to other substances or medical treatments, the number of respondents indicating various reasons for kratom initiation are relatively small and should be corroborated with future larger studies. Further, the sampling method prevented an accurate estimation of response rate. The sample consisted almost exclusively of people who currently used kratom and may not reflect those who tried but discontinued kratom. Given the nature of the questionnaire and reliance on self-reporting, recall and social desirability bias were also possible. The survey sample was relatively small, which may reduce external validity. Some respondents could not establish temporal relationships when queried, contributing to missing (or unclear) data. This finding may help inform sample size calculations for future similar research. With regards to the temporal relationship between kratom use and medical diagnoses, this study did not specifically assess whether the respondent was using kratom as a self-treatment for specific diagnoses. In this survey, respondents provided a fair number of free-text responses regarding reasons for initiating kratom products, which were categorized by the authors after the data collection, and were included in the Supplemental Appendixes. As a result, these data should be viewed as exploratory and provide valuable information for future surveys exploring this topic. Qualitative research to further explore this topic may provide additional insight as well, including further inquiry into findings observed from free-response answers and culturally hidden practices that may not have been explored with this survey tool. Finally, responses were not required, and approximately one-fifth of respondents did not provide full demographic information.
Conclusion
This study builds on previous research assessing motivations for kratom use by providing important insight into the temporal relationship between kratom initiation and past or future substance use or medical treatment. In this study, kratom was rarely the first psychoactive substance or medical treatment tried. Rather, most survey respondents who reported kratom use initiated it concurrently with or after discontinuing other psychoactive substances or medical treatments from their HCPs. Ensuring optimal management of underlying pain and mental health conditions may help reduce the desire to use kratom for some, but these data also suggest that for others, kratom may play a role in a patient’s preferred holistic treatment approach. These findings can assist HCPs in counseling patients on the potential risks associated with kratom use, though it is important that providers remain informed regarding the evolving market of kratom-derived products and create a safe space where people who use kratom feel comfortable discussing their use. While this study provides novel insights, larger follow-up studies are warranted to confirm these results.
Supplemental Material
Supplemental Material - An Initial Survey Assessing the Temporal Relationship of Kratom Initiation With Medical Treatment and Substance Use
Supplemental Material for An Initial Survey Assessing the Temporal Relationship of Kratom Initiation With Medical Treatment and Substance Use by Jordan R. Covvey, Oliver Grundmann, Nina Vadiei, Kirk E. Evoy in Substance Use: Research and Treatment
Supplemental Material
Supplemental Material - An Initial Survey Assessing the Temporal Relationship of Kratom Initiation With Medical Treatment and Substance Use
Supplemental Material for An Initial Survey Assessing the Temporal Relationship of Kratom Initiation With Medical Treatment and Substance Use by Jordan R. Covvey, Oliver Grundmann, Nina Vadiei, Kirk E. Evoy in Substance Use: Research and Treatment
Supplemental Material
Supplemental Material - An Initial Survey Assessing the Temporal Relationship of Kratom Initiation With Medical Treatment and Substance Use
Supplemental Material for An Initial Survey Assessing the Temporal Relationship of Kratom Initiation With Medical Treatment and Substance Use by Jordan R. Covvey, Oliver Grundmann, Nina Vadiei, Kirk E. Evoy in Substance Use: Research and Treatment
Footnotes
Acknowledgements
We thank the American Kratom Association (AKA) and Global Kratom Coalition (GKC) and its members for distributing the survey among their membership.
Ethical Considerations
This study was deemed Exempt Research by the University of Texas Health San Antonio institutional review board (protocol 00001351).
Consent to Participate
Informed consent information was provided prior to the survey, with the option of not participating or discontinuing the survey at any point after beginning.
Author Contributions
KEE: Conceptualization, Methodology; Project Administration, Writing – original draft, Writing – review and editing; JRC: Methodology, Statistical Analysis, Writing – review and editing; NV: Conceptualization, Methodology, Writing – review and editing; OG: Methodology, Statistical Analysis, Writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: OG is retained as an independent expert witness in kratom-involved legal cases. The other authors have no conflicts of interest to disclose.
Data Availability Statement
Data available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.