
Abstract

Since the name of this journal begins with ‘Design’ and emphasizes inter-disciplinary integration and innovation, it is easy for many experts and scholars from non-design fields to be confused with the attribution of design research results. The basic requirements of scientific research include objectivity and justification, seeking truth from facts, focusing on problems and gaps, and discovering and reinventing knowledge, to name a few. However, the ‘grand design’ research emphasized by DAH journal is more inclined to those with the following attributes: human-centric, benevolence-based, holistic-oriented, and co-creating values, among others. Therefore, it is necessary to introduce the types of design research articles DAH is aiming for, to help readers understand and recognize their significance, as well as to attract high-quality submissions and citations.
Design is often seen as a means of ‘solving problems’, where designers diagnose issues for businesses and propose solutions, much like the act of treating a patient. Medicine has long led the development and application of many related technologies and designs. Medicine can be applied as a framework to point out the directions of design research and core concerns. According to ‘Baidu Health · Medical Popular Science (2026.5.10)’, medicine is divided into five major categories: ‘Clinical Medicine’, which involves disease diagnosis, treatment, and patient management; ‘Rehabilitation Medicine’, which assists patients in restoring physical function and improving quality of life; ‘Basic Medicine’, which studies disease mechanisms and medical principles; ‘Preventive Medicine’, which focuses on disease prevention and health promotion; and ‘Special Medicine’, which addresses health problems in specific scenarios, for example: ‘Military medicine’, which involves battlefield first aid and nuclear, biological, and chemical protection; ‘Aerospace medicine’, which studies the effects of the space environment on the human body; ‘Sports medicine’, which prevents and treats athlete injuries and enhances performance; and ‘Forensic medicine’, which assists in judicial examinations.
Although each category has its focus, they are interrelated (Figure 1). Clinical Medicine addresses treatments for existing diseases (restoring health), Rehabilitation Medicine restores patient functions (returning to health), Preventive Medicine reduces disease occurrence (maintaining health), Basic Medicine provides theoretical support (mastering health), and Special Medicine addresses specific needs (protecting health). Assuming that a state of health with no illness or pain is defined as a zero value (or normal quality, neutral zone), most of the above medical classifications aim to address various ‘negative weak or diseased problems’, attempting to use medical means to turn negative into zero so as to restore or maintain health. It can be noted that the zero value symbolizing a state of health and well-being is not an independent existence, but rather a continuum or ‘tolerance interval’ that can encompass both Weak and Fit. Design Research Types Based on Medical Taxonomy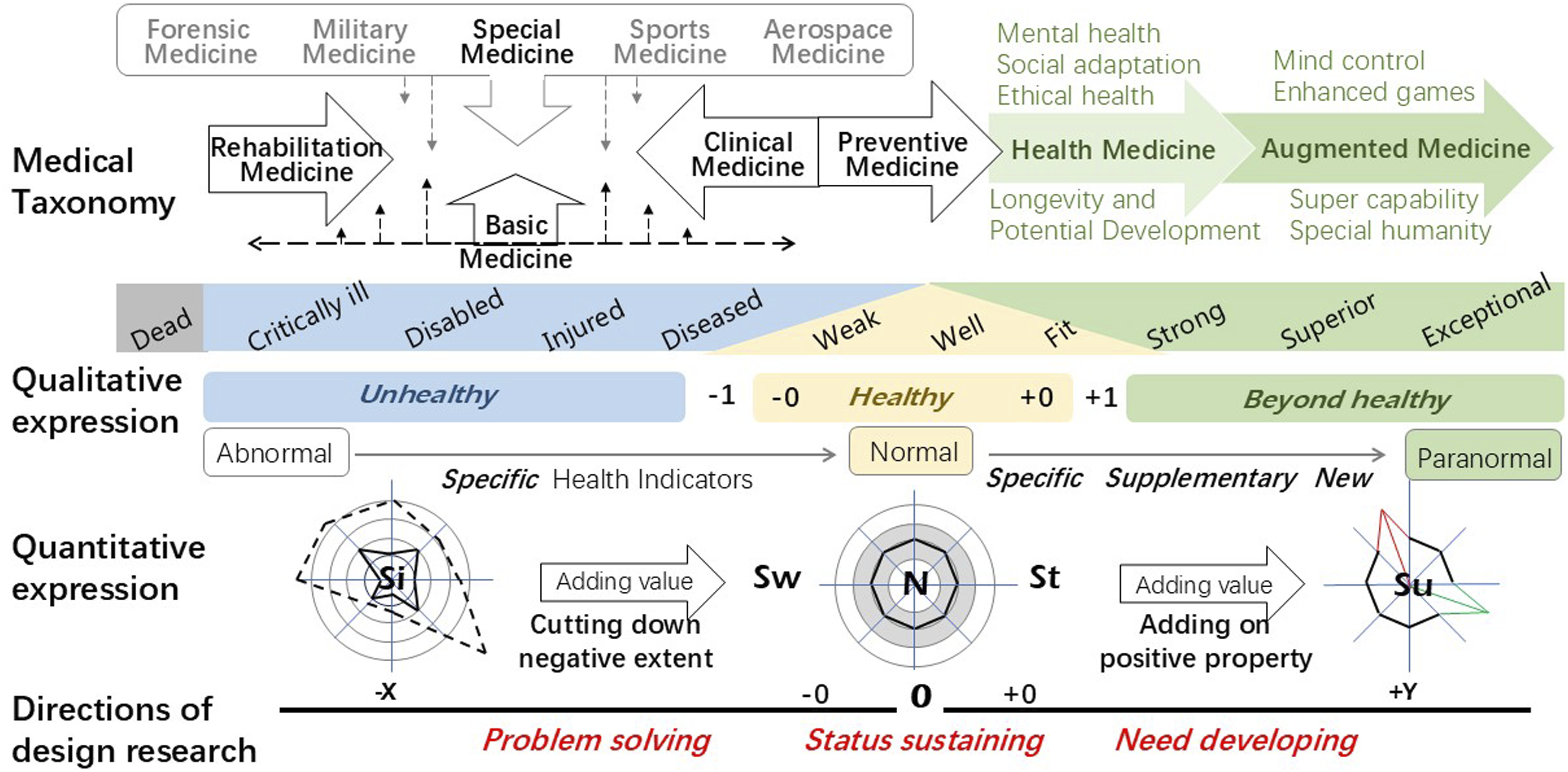
Although sports medicine aims to enhance athletic performance, athletes performing under ‘normal’ conditions without drugs or assistive devices are still not developing in the ‘positive value zone’. The World Health Organization first proposed in the 1946 ‘World Health Organization Constitution’ that ‘health is not merely the absence of disease or infirmity but a state of complete physical, mental, and social well-being’. American scholar Engel, George L., published an article titled ‘The Need for a New Medical Model’ in the journal Science in 1977, which influenced people’s understanding of the concept of health, shifting the focus from the previous emphasis on a single or a few specific physiological health models toward a diversified ‘comprehensive health model’, suggesting that human health, besides physical health, also includes mental health, social adaptation, and ethical health. In 1987, Dr. Xuesen Qian, the founder of China’s aerospace industry, proposed the concept of the fourth type of medicine, ‘Health Medicine’. Its core goals include health, longevity, and potential development, covering modern health practices such as traditional Chinese medicine, cosmetic medicine, psychological adjustment, wellness tourism, dietary therapy, and exercise. Looking at the overall development trend, based on the ‘Normal state’ of ‘health and wellness’ of the body itself, it develops toward the ‘Norm state’ of ‘Strong and Superior’, and even progresses toward the ‘Paranormal’ level of ‘Excellence and Exceptional’ that explores potentials and extremes, extending into a trend of ‘Augmented Medicine’. Specific examples include brain-computer interface technology that enables mind control, as well as the ‘Enhanced Sports Games’ held in Las Vegas, USA, on May 24, 2026. The former is still conducting various human experiments in the global medical community, targeting the restoration of normal functions in individuals with functional impairments or losses, such as the blind regaining sight (going from negative to zero) and in the future, it is expected to add and enhance various human abilities, like adding wings to a tiger (positively adding value). The latter, however, is widely debated due to moral and ethical health issues attributed to being ‘sports competitions not based on universal values such as honesty, fairness, and justice’. Initially, the ‘Enhanced Sports Games’ only included three events: short-distance swimming, sprinting, and weightlifting. Under strict scientific and medical supervision, participants are allowed to use performance-enhancing drugs or assistive devices legitimately, enabling athletes to explore the limits of the human body ‘beyond what the Creator designed’.
From the distribution of functions across various types of medicine, the basic overall pattern can be observed. The meaning represented by ‘0’ can be quantitatively described as the ‘zero value’ of having no injury or illness, or qualitatively understood as the ‘normal quality’ of having no health problems. The normal range can include some hidden and undeveloped ‘Weak’, all ‘Well’, and some ‘Fit’ that have yet to manifest. In terms of quantity, it corresponds to the relationship of ‘−0, 0, +0’, existing in the form of a ‘spectrum’ or ‘field’. ‘Zero value’ therefore refers to a state of health that is ‘normal or standard’. The ‘negative value region’ focuses on ‘solving problems’ through due means, such as first aid, medical treatment, and restoring health; the ‘positive value region’ centers on ‘creating opportunities’ through strengthening, optimization, and adding new functions. It progresses from maintaining single-dimensional physical health to developing multi-dimensional ‘comprehensive health’, and further, from quantitative changes to qualitative changes, expanding or generating physical abilities or potential beyond the normal human range with assistance from new high technologies. Despite that it has also been criticized and debated for ‘transpassing’ the existing boundaries of moral and health norms.
Obviously, design is not only limited to ‘solving problems’ but can also ‘create opportunities’, which relates to another common definition of design, namely, ‘design is a value-adding activity’. However, how does one ‘add’? What kind of ‘value’ is added? What is the ‘quality’ of the added value? How should the ‘adding’ be carried out in the design activity? How should ‘value’ be defined? What kind of relationship exists between ‘value’ and ‘quality’? All these questions become core essential issues that need to be deeply explored in the definition of ‘design as a value-adding activity’.
If the ‘0’ point can be defined as a neutral state (normal state) represented by the numerical value 0, then the left side of a numerical line (or numerical interval) with 0 as the midpoint can be defined as the ‘negative value/quality area’, and the right side can be defined as the ‘positive value/quality area’. Although ‘value’ and ‘quality’ are two completely different concepts, the relationship between them can also be analyzed using the doctor-patient model.
Assume that the medical team has several diagnostic indicators for a patient’s health condition. The average values of each diagnostic indicator for healthy normal individuals are defined as the ‘0’ value. The central ring of the five-ring indicator is defined as the position of the normal index average, and the ring range marked in gray is considered the qualified zone. Indexes that exceed or fall short of this range are considered symptoms that require treatment.
For quantitative description, a comprehensive symptom index can be defined through weight setting and calculation, and the patient’s comprehensive symptom index can be measured. Thus, medical staff designed treatment plans and therapies based on the symptoms, prescribed remedies, and medicines, and carried out ‘value-added activities’ related to treatment methods, attempting to alleviate more severe symptoms and ultimately restore health. After recovering from a serious illness, applying supplements, exercise, or value-added activities of ‘health medicine’ continuously improves health indicators, gradually optimizing condition from the Weak into the Well. During the course from severe illness to recovery, all treatment methods are value-added activities aiming at alleviating or eliminating symptoms. Essentially, it is a ‘value-added’ activity of ‘reducing negative values’, a ‘cutting down negative extent’ action carried out on a known problem subject.
From normal health to being optimized as a physically fit individual, this process shows that the value-added activities are carried out on indicators already defined as ‘healthy’ (rather than pathological or abnormal conditions). It is equivalent to being within the ‘0 to +0’ range on the 0-value spectrum, and the focus of the design of value-added activities is on ‘maintaining health and continuing wellness’. Importantly, health is not the goal, but an important means to achieve an ideal life. In the process of value-added activities from the normal state to the paranormal state, clearly value-added work has gone beyond merely improving the level of problems within the original set indicators, and instead makes breakthroughs within the existing indicator framework, adding, transforming, or creating new types of indicators, developing more diverse dimensions, and thereby expanding to form a new indicator framework. Essentially, it is a ‘quality-enhancing’ activity of ‘adding on new properties’.
From the above discussion, it can be summarized that design research can be generally divided into three directions: problem-solving (toward well and fit), status sustaining (maintaining health and longevity), and need developing (reinventing and empowering quality potential). Design research articles for each direction are expected to include ideally the following elements: humanity, benevolence, value, and holistic view, using a multidisciplinary, cross-domain innovative design approach.
Footnotes
Author Contributions
Ding-Bang Luh: Conceptualization, Methodology, Investigation, Writing-draft, Writing-review & editing.
Data Availability Statement
The original contributions presented in the study are included in the article material; further inquiries can be directed to the corresponding author.
Declaration of Competing Interest
Ding-Bang Luh is the editorial board members. The author was not involved in the peer review or editorial evaluation of this manuscript and had no access to materials or information pertaining to the review process. The author declares that he has no competing interests in this paper.