
Abstract
Background:
Immersive technologies (ImTs), including virtual, augmented, or mixed reality, are increasingly used to support periprocedural pediatric patients, but clinical adoption varies widely across children’s hospitals and specialties. Multiple determinants for the adoption of ImT in health care have been identified; however, these have not been well characterized in pediatric perioperative settings.
Aims:
Among Society for Pediatric Anesthesia Improvement Network (SPAIN) member institutions, we describe the current state of pediatric perioperative ImT use, identify barriers and facilitators to ImT adoption, and report perceived implementation-related factors.
Methods:
We conducted a multi-institutional cross-sectional survey of pediatric perioperative practices via key contacts from SPAIN. Survey responses underwent mixed-methods analyses informed by the Consolidated Framework for Implementation Research.
Results:
Among 27 eligible institutions, 24 (89%) provided responses, 13 of which reported ImT use. Of these, 8 (62%) reported existing institutional infrastructure or governance to support ImT. Use patterns were highly heterogeneous, but use was commonly paired with the presence of champions, technology expertise, and available resource support. Use cases included anxiety reduction, distraction, and procedural support. Barriers, facilitators, and potential strategies for successful implementation were highlighted.
Conclusions:
ImT is used variably across pediatric anesthesia practices affiliated with SPAIN. These findings provide a descriptive snapshot of current practice and highlight factors commonly associated with adoption. Further work is needed to more rigorously characterize the implementation processes and evaluate strategies that may support integration of ImT into routine care in diverse clinical settings.
Keywords
Introduction
Immersive technologies (ImTs), including virtual reality (VR), mixed reality (MR), and augmented reality (AR), are increasingly used in health care as adjuncts to procedural sedation, anxiolysis, analgesia, distraction, and patient education. 1 A growing evidence base supports the adoption of ImT in pediatric practice, particularly for distraction therapy, training and education, adjunctive support during painful procedures and anesthesia, and psychosocial management.2–6 ImT can improve patient adaptation to clinical environments, reduce pain and anxiety, offer anticipatory guidance, and provide distraction during procedures, such as inhalation induction, intravenous catheter placement, suturing, orthopedic interventions, and dressing changes.3–10 Newer information suggests additional therapeutic benefit for unique patient populations, such as those with cerebral palsy, ophthalmologic conditions, traumatic brain injury, attention-deficit/hyperactivity disorder, autism spectrum disorder, and Down syndrome. 11
Despite this growing evidence base, adoption of ImTs into routine pediatric perioperative practice remains inconsistent across institutions.5,12–14 Several mechanisms may underlie the therapeutic effects of ImT. Gate control theory of pain and related models propose that immersion and presence redirect attention away from discomfort, activating attention-modulation pathways and emotional regulation circuits.1,9 Electroencephalography and functional magnetic resonance imaging have been used to correlate subjective improvements with objective findings in patients using therapeutic ImT.9,15 These technologies are broad in complexity and scope and include a vast array of digital therapeutic tools. ImT delivery hardware varies widely, including projectors; interactive mirrors, sound, and lighting systems; tablets; head-mounted displays; and other multisensory devices with associated software, in both active and/or passive formats. 1 Reported adverse events are uncommon and include infection, eye strain, and VR sickness, with epilepsy experts noting a low likelihood of ImT-induced seizures.8,16–18 The diversity of platforms, clinical use cases, and institutional resources introduces complexity that may limit reliable integration of ImT into routine clinical workflows. Similar barriers to adoption of immersive and digital health technologies have been described in a variety of health care domains, including cost, awareness, workflow integration, and the need for specially trained personnel.19–21
Implementation science (IS) is the study of methods to promote systematic uptake of evidence-based practices into routine care; this discipline aims to reduce the average 17-year gap between discovery and widespread clinical adoption.13,22,23 Pediatric perioperative care represents a high-acuity, workflow-intensive environment with numerous potential points of impact for ImT; however, the determinants of adoption and integration of these technologies in this setting have not been well characterized to date. Understanding real-world implementation patterns is critical for translating ImT from experimental and niche into routine care.
Pediatric anesthesia collaborative networks may support the study of implementation approaches for emerging technologies by harmonizing practice patterns, sharing resources, and disseminating best practices. 24 The Society for Pediatric Anesthesia Improvement Network (SPAIN) is a national multicenter collaborative focused on advancing perioperative outcomes through pragmatic research. In this context, we conducted a cross-sectional survey to describe current patterns of ImT use across pediatric perioperative settings, identify perceived barriers and facilitators for ImT adoption, and explore possible implementation strategies. These findings provide a descriptive overview of current practice and may inform future work aimed at understanding how ImT can be integrated into diverse practice settings.
Methods
Framework
IS frameworks can help demystify the gap between evidence and clinical practice and identify determinants that influence adoption of new technologies.13,22,23 Hundreds of process theories, models, and frameworks are described for IS. The Consolidated Framework for Implementation Research (CFIR) informed the conceptual approach to identifying potential determinants of ImT implementation, including barriers and facilitators related to the innovation, individuals involved, and the clinical environment. 25 A plethora of implementation strategies exist, such as education and communication techniques, stakeholder engagement, strengthening partnerships, and developing outcome measures.13,22,23 Finally, implementation outcomes can be assessed by using a defined taxonomy for implementation outcomes, including feasibility, fidelity, penetration, acceptability, uptake, and sustainability, 26 which can be used to facilitate an iterative cycle of change that can bring evidence to practice. These concepts informed survey development and interpretation of results.
While survey development was informed by CFIR domains, this study did not include any formal framework-based coding or domain-level analysis. The framework was used as a conceptual guide for question development and interpretation. In other words, the study was an exploratory cross-sectional descriptive survey, rather than a formal implementation analysis.
Study design and setting
We conducted a multi-institutional cross-sectional survey of pediatric perioperative practices at 27 institutions; these sites were identified via membership in SPAIN, a collaborative of the Society for Pediatric Anesthesia that focuses on advancing pediatric perioperative outcomes through pragmatic research and implementation efforts. This study was not designed as a consensus-based or Delphi process. The study was reported in accordance with the Checklist for Reporting of Survey Studies.27
Survey development
The survey was designed to identify practice patterns and describe implementation determinants among participating institutions. The invitation to participate in the survey was distributed via email and included a list of definitions related to ImT (Appendix). The 14-question survey was estimated to take 10–15 min to complete and was divided into three sections: (1) current ImT utilization; (2) implementation barriers, facilitators, and strategies; and (3) contextual institutional information. Survey questions were informed by CFIR constructs to capture characteristics of the technology, individuals involved in implementation, and inner-setting factors within clinical environments. Outer setting influences were assessed through questions on external partnerships and financial models. Items included structured response formats (e.g., “select all that apply” and ranked responses) with opportunities for free-text input. The survey underwent iterative refinement with input from the authors, SPAIN executive board members, and colleagues with expertise in pediatric anesthesia, perioperative care, and survey methodology to ensure clarity and relevance.
Participants and recruitment
Eligible representatives of 27 SPAIN institutions were invited to participate via email in May 2025. Invitations were distributed to designated institutional contacts, with the option to forward the invitation to other colleagues also involved in these initiatives at their institution. Survey reminders were sent to participants in July, August, and September 2025. The survey was closed on October 31, 2025. Respondents were encouraged to answer the questions to the best of their ability even if their site did not have an active ImT program.
Data collection
Qualtrics was used to distribute the survey and collect data from May 9 through October 31, 2025. The survey could not be submitted unless all questions were completed. Participants were asked to provide basic information about their role and clinical site; they could optionally provide contact information for follow-up. Responses were aggregated at the institutional level. When multiple responses were received from a single institution, responses were reviewed for agreement and pooled. No discrepancies between respondents from the same institution were identified.
Data analysis
Descriptive statistics were used to report quantitative results for adoption prevalence, technology types, use cases, and institutional characteristics.
Ranked responses for barriers, facilitators, and strategies were assigned weighted scores based on rank order, with higher scores assigned to higher priority rankings. For example, if a respondent indicated that a barrier was the most significant and ranked it first, that response category received a weighted score of 5, whereas the barrier they felt was least impactful (ranked fifth) received a weighted score of 1. Weighted scores were summed across institutions to identify the most influential factors.
Responses to the open-ended survey item underwent descriptive content review. Two reviewers (K.S.H., J.H.) independently read all responses, noted themes, and reconciled their summaries by consensus. No formal coding or thematic analysis was conducted. Findings are reported as descriptive observations intended to contextualize the quantitative results rather than as fully developed qualitative themes.
Ethical approval
The study was determined to be exempt from institutional review board review.
Results
Among 27 SPAIN institutions invited to participate in the survey, responses were received from 24 institutions (89%) during the study period, with 27 individual respondents. These 27 respondents were predominantly physician anesthesiologists (n = 23, 85%), with others including child life specialists (n = 2), a physician assistant (n = 1), and a certified registered nurse anesthetist (n = 1). Adoption of ImT varied substantially across institutions.
Of the 24 institutions, 13/24 (54%) reported active adoption of ImT (Table 1). Of these 13, 7 (53%) reported using VR, and the others used a combination of ImT types (including AR, MR, and artificial intelligence [AI]-enabled platforms). A majority (7/13, 53%) also reported using a combination of independent software vendor technology and custom institutional technology solutions. Only one site relied solely on custom institutional software. Use cases were heterogeneous across institutions, but most included management of anxiety and procedural distraction (both 11/13, 85%), as well as acute procedural analgesia (8/13, 62%). Additional reported applications included anticipatory guidance, relaxation, staff training, and psychosocial interventions. ImT use frequently extended beyond anesthesiology, with 11/24 (46%) institutions reporting ImT use by other specialties.
Institutional Immersive Technology Use Patterns from Survey Section 1 (N = 24)
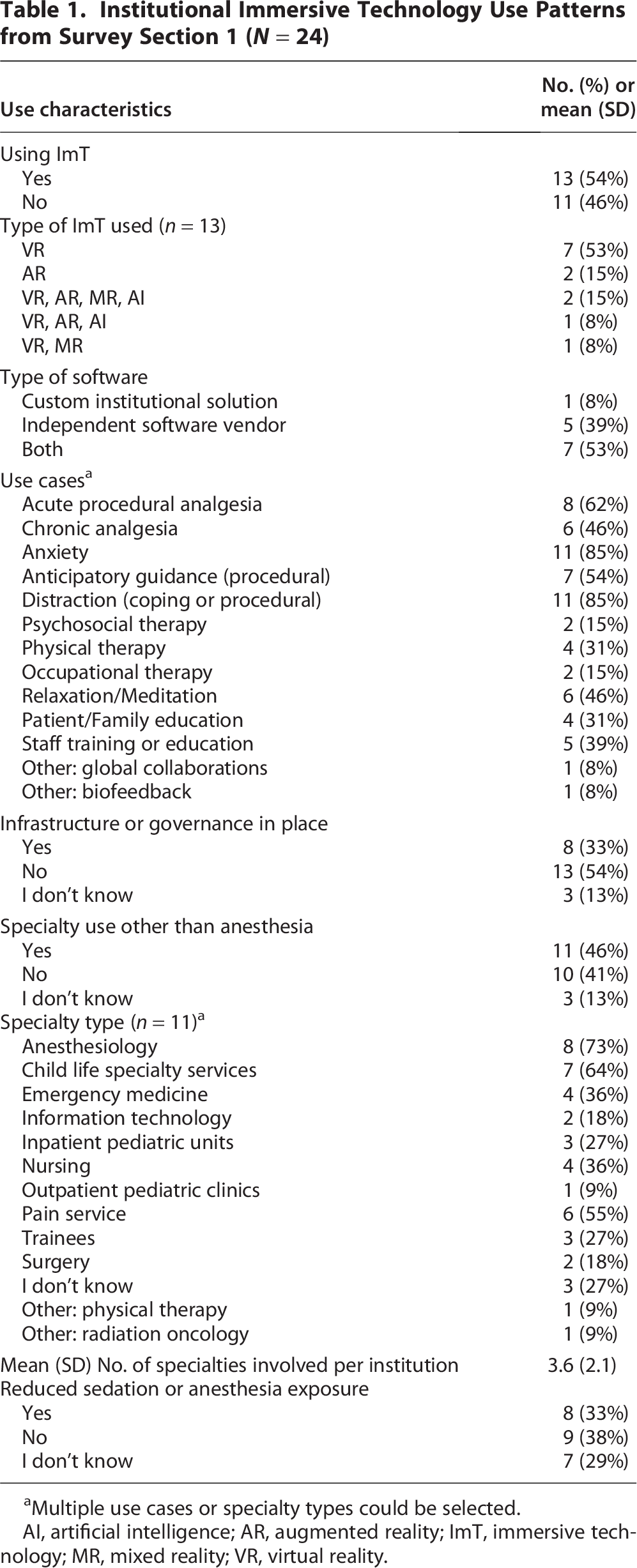
Multiple use cases or specialty types could be selected.
AI, artificial intelligence; AR, augmented reality; ImT, immersive technology; MR, mixed reality; VR, virtual reality.
Most institutions (16/24, 67%) reported no existing infrastructure or governance structures to support ImT implementation, although 8/13 (62%) institutions using ImT reported some form of organization around these technologies. These findings may reflect variability in the maturity of ImT programs across institutions.
Some respondents reported perceived reductions in anesthesia or sedation requirements. Among institutions using ImT, 8/13 (62%) reported reduced sedation or anesthesia exposure from ImT, compared with 8/24 (33%) overall. However, these responses were perception-based and included a substantial proportion of “I don’t know” responses, limiting interpretability.
Responses regarding implementation barriers and facilitators showed substantial variation across all categories (Fig. 1A and B). The most highly ranked barriers included lack of funding, absence of local champions, limited staff familiarity with the effectiveness of ImT, insufficient support staff, and logistical challenges such as device storage and management (Table 2). Key facilitators included the presence of child life gaming and technology specialists, availability of local champions, ease of access to hardware and software, familiarity with supporting evidence, and accessible funding.
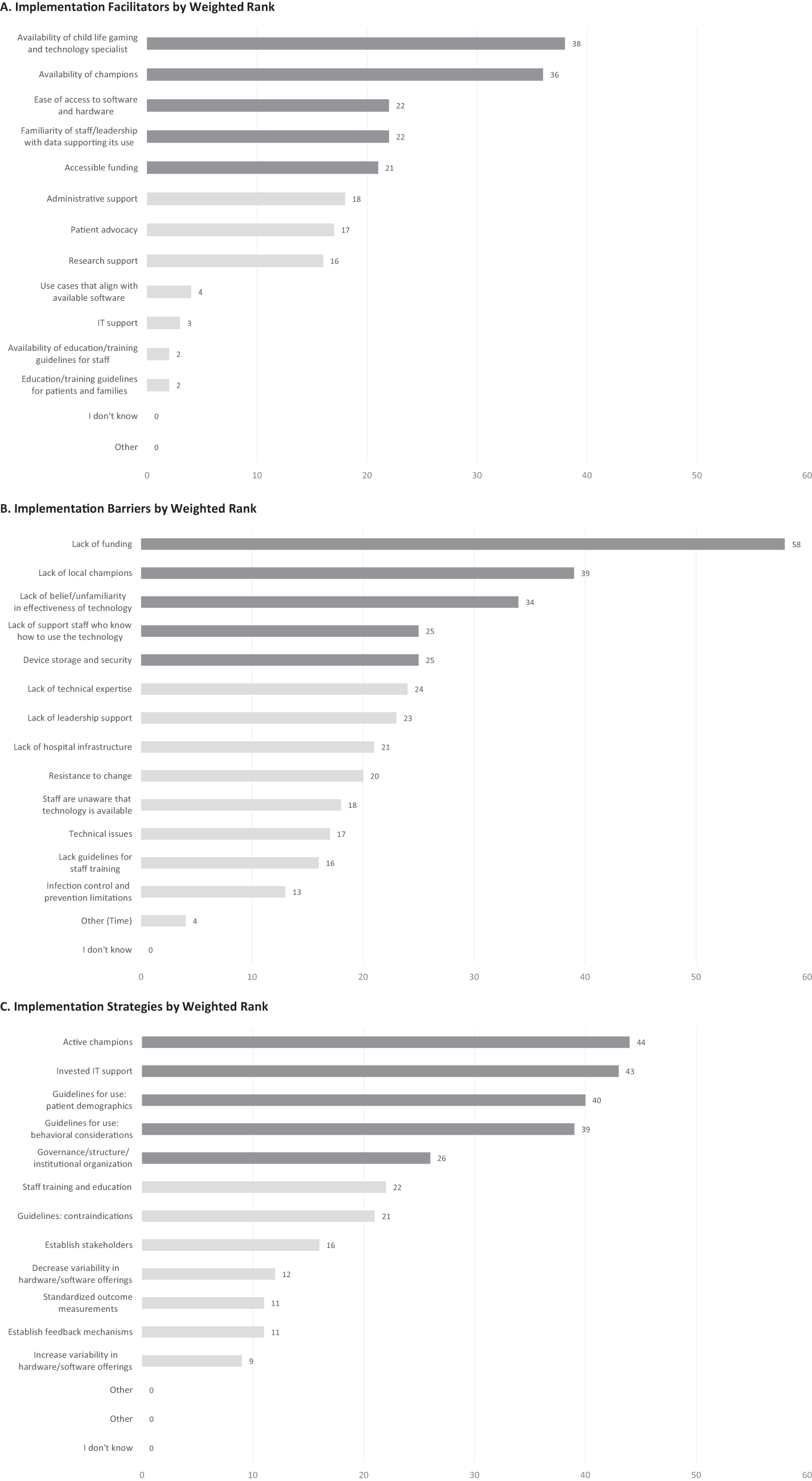
Barriers, facilitators, and strategies for immersive technology use as perceived by survey respondents. Weighted scores (X axis) are presented in order of most to least important. The Y axis shows the specific barrier, facilitator, or strategy (as listed in the survey item). The top-five responses in each category are designated as dark gray bars.
Top-Five Barriers, Facilitators, and Strategies with Coded Open-Ended Responses from Survey Sections 2 and 3
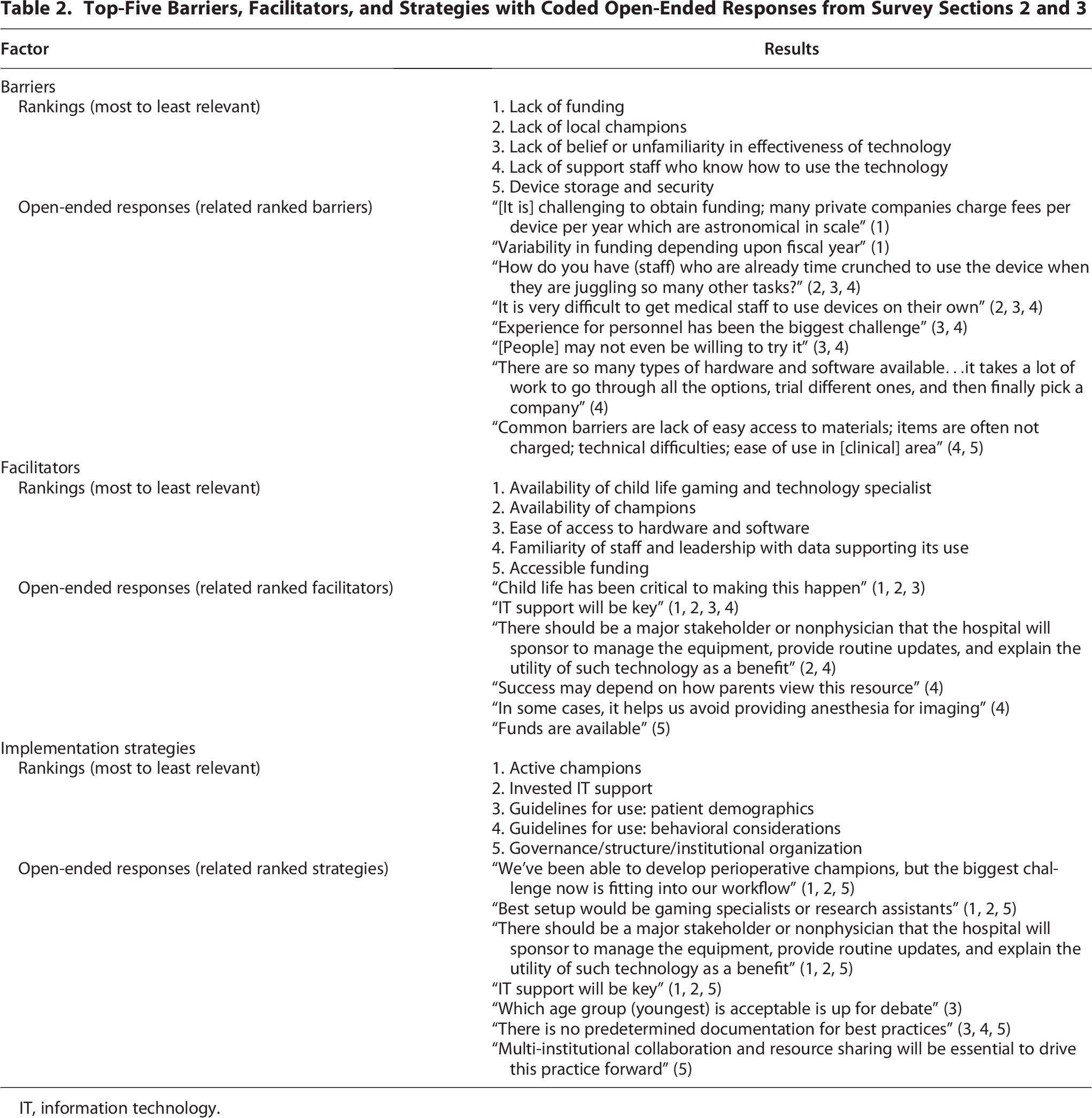
IT, information technology.
Respondents demonstrated greater agreement regarding potential implementation strategies (Fig. 1C). The highest ranked strategies included development of active champions, investment in information technology support, establishment of guidelines for patient selection, and creation of institutional governance structures to support ImT programs.
Free-text responses were limited (n = 9) but provided additional context for quantitative findings. For example, one respondent noted that “many private companies charge fees per device per year which are astronomical,” while another highlighted workflow constraints: “How do you have (staff) who are already time crunched to use the device when they are juggling so many other tasks?” (Table 2). These responses emphasized the importance of dedicated personnel, as well as institutional support for funding, training, and workflow integration. Reported challenges included staff time constraints, variability in technology platforms, and difficulties integrating ImT into existing workflows.
Discussion
To our knowledge, this study provides one of the first multi-institutional descriptions of current patterns of ImT use across pediatric perioperative practices in the United States and offers insights into how these technologies are being integrated into clinical care. Despite an abundance of literature supporting its use in perioperative and periprocedural practices leading to multiple positive outcomes, only a slim majority of these leading pediatric institutions use ImT in their practices, and adoption is variable. In addition, the infrastructure needed to support these efforts is not common, despite findings that these tools commonly cross disciplines and clinical contexts. Limited qualitative responses provided an illustrative context as they highlighted the potential roles of that child life technology specialists, clinical champions, and governance structures in supporting ImT use. However, the qualitative reporting cannot be interpreted as comprehensive or generalizable because of limited responses. The level and degree of integration of ImT into clinical workflows varied widely, and adoption appeared to be largely driven by specific use cases and local champions rather than through intentional implementation planning. This is consistent with prior observations that perioperative research in general often lacks implementation focus. 13 These findings may suggest that ImT remains in an early stage of adoption in many of these institutions, where evidence of benefit is increasing but structured pathways for implementation and integration remain underdeveloped. These findings should be interpreted as descriptive, perception-based observations rather than measures of institutional performance, outcomes, or effectiveness, which our study was not designed to assess.
Implementation planning is an important consideration as new tools and technologies are introduced to clinical practice. In this study, CFIR served as a conceptual guide for survey design and interpretation rather than a formal analytic structure. The literature suggests that ImT may reduce or negate the need for anesthesia in certain procedures, although not yet on a systems-level scale, perhaps due to challenges in defining and capturing outcomes related to the use of ImT.1,4,5 In this study, 8 of 24 institutions reported perceived reductions in anesthesia or sedation requirements; however, these findings are based on self-report and were accompanied by a substantial portion of uncertain responses (7 of 24 responses indicated lack of knowledge of any effect on sedation practice). These findings should be interpreted cautiously, as these are perception-based observations rather than evidence of clinical effect. Nevertheless, ImT may function as a behavioral support tool in clinical settings; however, further research is needed to evaluate the extent to which ImT may influence sedation practices and related clinical outcomes in real-world settings.
The identified factors involved in the integration of ImT into clinical workflows frequently included the benefit of local champions and child life gaming and technology specialists in driving successful use cases, and the absence of these roles was associated with challenges. Increasing evidence points to the utility of technology champions or, in the case of pediatrics, child life gaming and technology specialists, in diverse clinical contexts.2,4,18 These roles may be increasingly important as technology options expand and each new tool requires a process to learn, introduce, and onboard it into clinical practice. Funding was identified as a common issue, but our survey was not designed to distinguish whether this refers to the smaller goal of obtaining hardware and software or the larger goals of content creation, infrastructure, staffing, or workforce development. Participants identified potential strategies that reflect a perceived need for structured guidelines, technology support, institutional governance and infrastructure, and champion support to promote these initiatives. Recent publications support these needs, but respondents suggested that institutional organization to implement them may be variable or underdeveloped.1,4,8,14,15,25 Importantly, these findings reflect respondent perceptions and should be interpreted within the cross-sectional descriptive scope of the study, which included limited informal qualitative analysis. Nevertheless, collaborative research networks such as SPAIN may provide an opportunity to study implementation approaches for new technologies by enabling shared protocols, pooled expertise, and multi-institutional evaluation of implementation processes.
Limitations
At the same time, involvement in collaborative networks like SPAIN may suggest more robust academic engagement, networking, and implementation awareness than broader pediatric practices, and the homogeneous nature of SPAIN-affiliated institutions therefore also limits the generalizability of these results. Our study is also limited by bias of several types. Self-reporting, information (recall), and response bias are possible given that our survey respondents were chosen from a homogeneous pool of pediatric perioperative physicians involved in SPAIN but not necessarily involved with the ImT initiatives (if present) at their institution. Nonresponse bias may also be present if institutions with active ImT programs were more likely to participate, despite the overall response rate of 24/27 institutions (89%). We attempted to mitigate these sources of bias by opening the survey to colleagues of SPAIN representatives, but only three institutions provided more than one respondent. Again, these results must be interpreted with the recognition that one or two individuals from each institution were represented, generally from the specialty of anesthesiology. In other words, institutional aggregation may mask internal variation, and we may have missed respondents from other disciplines or specialties who carry more in-depth knowledge of their institution’s ImT practice. Responses were not validated, and our data were not audited. In addition, the cross-sectional design of the survey, especially on the topic of dynamic digital technologies, which are evolving rapidly, limits the long-term validity of this data. For example, AR and MR modalities with AI integration are becoming more powerful, will continue to evolve, and may be important for the future of clinical ImT.1,4 Their increasing use, however, is not reflected in these data, which showed most institutions using VR alone. In addition, the nuances of different ImT technology types were not explored in this study; at most, participants were asked to identify what type(s) of technology their institution utilized. The definition of ImT is intentionally broad in our survey to allow for a field-level overview of adoption patterns across SPAIN. However, this limits interpretability because different hardware and software require distinct resources and strategies that are not fully captured by grouping them under a single umbrella term. Yet, the reality of clinical implementation for each of these tools may take varying paths, as AR and VR and MR and AI likely all have overlapping, but distinct clinical integration needs.
Future directions
While substantial evidence supports the effectiveness of ImT in this population, comparatively less is understood about how to best implement these technologies in clinical practice, highlighting a need for further exploration of implementation strategies. Further work is needed to examine these modalities separately to better characterize implementation and adoption of each type of technology. Development of standardized approaches to ImT program implementation, including best practices for patient selection, workflow integration, staffing models, and governance, will be important. Future studies of ImT may benefit from heightened focus on identifying site-specific factors to facilitate implementation by using frameworks from the field of IS to describe implementation determinants, strategies, and outcomes that work in specific contexts. Specifically, pooled data from well-established pediatric ImT programs would be helpful in clarifying common implementation determinants and strategies that have led to successes. Future work could include structured consensus approaches, such as Delphi methodology, to better define shared implementation priorities across institutions. In addition, hybrid observational-implementation or effectiveness-implementation approaches may help elucidate both the clinical impact of emerging technologies and implementation processes.16,26 As ImT continue to evolve, the ongoing evaluation of safety, usability, and scalability will be essential to guide broader adoption.17,22
Conclusions
Adoption of ImT across pediatric perioperative practices remains variable among SPAIN-affiliated institutions, with commonly reported facilitators including local champions, technical expertise, and institutional support. These findings provide a multi-institutional, perception-based snapshot of current practice and highlight areas where institutions may encounter challenges or opportunities when considering integration of ImT. Further work is needed to better characterize how specific types of technologies may be successfully implemented across contexts and to evaluate their ongoing impacts on clinical workflows.
Authors’ Contributions
K.S.H. contributed to study conceptualization, survey development, data collection, data analysis, interpretation, and article drafting. A.F. contributed to study design, survey refinement, and article revision. G.L. contributed to survey refinement and article revision. K.S. contributed to study design, survey refinement, and article revision. All authors reviewed and approved the final article.
Footnotes
Acknowledgments
The authors thank Hannah Van Pelt for her assistance with survey coordination and dissemination and Jeffrey Huang, MD, MS, for his assistance in review of the survey questions and methods for qualitative analysis.
Artificial Intelligence Disclosure
Generative AI (ChatGPT 5.0) was used for brainstorming and outlining after completion of data collection. No AI tools were used for data analysis. All content was reviewed and approved by the authors, who take full responsibility for the integrity and accuracy of the work.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No external funding was received for this study.
Abbreviations Used
Appendix
Immersive technology (ImT): Technology aimed at simulating a different reality (umbrella term).
Head-mounted display (HMD): A type of device that utilizes a small visual display usually mounted within a wearable headset, helmet, or eyeglasses. These devices come from a variety of manufacturers and sources and may exhibit slight differences from one another. They can be used for VR, AR, and MR.
Extended reality (XR): The spectrum of virtual, augmented, and mixed reality experiences (umbrella term).
Virtual reality (VR): A fully virtual experience, in which you are separated from your true reality. Requires use of a VR headset (a type of HMD).
Examples: fully immersive gameplay, avatar-based socializing, virtual entertainment via HMD
Augmented reality (AR): Virtual elements overlayed on the real world. In this setting you can view your physical and virtual surroundings at the same time.
Examples: Smartphone/tablet applications, photo filters, live language translations, real-time diagnostics, gaming, guided navigation
Mixed reality (MR): Combines elements of physical and digital worlds, allowing them to interact with each other; you can view and interact with simulated objects in the real world. Usually requires an HMD and/or VR headset.
Examples: 3D asset collaboration, semi-immersive gameplay, enhanced marketing
Artificial intelligence (AI): computer systems capable of performing complex tasks that historically only a human could do and may incorporate adjustments based on learned experience.
Examples: Predictive algorithms, facial identification, self-driving cars, recommendation algorithms