
Abstract
Transcatheter aortic valve implantation (TAVI) has transformed the treatment landscape for patients with aortic stenosis across a broad spectrum of patient populations. Despite its success, several post-procedural complications remain of utmost consideration, many of which are directly tied to the mechanical interactions between the implanted valve stent and the patient's anatomy. Predictive computational modeling has long held the promise of informing these decisions pre-operatively, offering a virtual simulation environment in which device-tissue interactions can be explored prior to the TAVI procedure itself. The fundamental obstacle to the clinical translation of these predictive modeling tools, such as finite-element analysis (FEA) and computational fluid dynamics, is their expensive nature. Full patient-specific pipelines for modeling TAVI can require several days to weeks to complete, thus becoming incompatible with pre-operative clinical decision-making timelines.
The study presented by Hossen et al represents a meaningful step towards addressing this gap. 1 By training a graph neural network (GNN) architecture on FEA simulation-derived contact pressure and stresses from a large cohort of TAVI patients (n = 55), the authors demonstrate that a data-driven surrogate model can accurately reproduce patient-specific aortic wall stress profiles with high-fidelity, generating predictions for a new patient case within seconds. Such metrics are directly relevant to procedural risk, and the real-time modeling strategies presented in this study are precisely what is needed to translate biomechanical modeling into clinically actionable insights.
This work arrives at a particularly opportune moment in the field of predictive computational modeling, in which the idea of a cardiovascular “Digital Twin” (DT) is becoming increasingly popular. Broadly, this paradigm merges real-time clinical data with computational modeling to continuously simulate patient-specific cardiovascular function. Central to its realization are the development of two distinct paradigms for computational model acceleration that are maturing in parallel and beginning to find significant clinical applications in cardiovascular biomechanics: physics-driven model reduction and data-driven surrogate modeling. Understanding their complementary strengths and limitations, and most critically, the promise of hybrid approaches that draw on both, is essential towards realizing the DT paradigm (Figure 1).
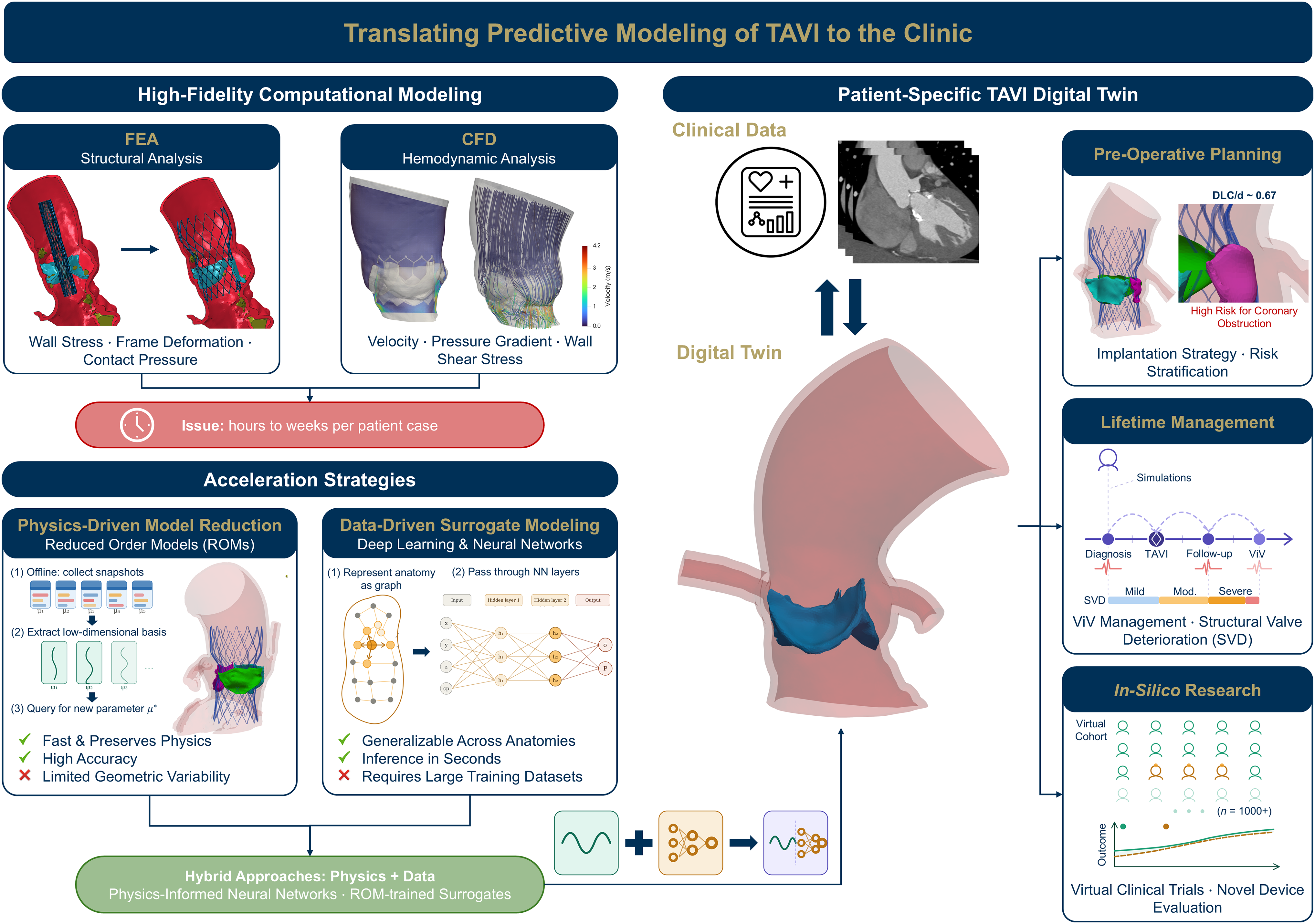
Overview of the translational pathway from high-fidelity biomechanical models of TAVI to the patient-specific digital twin via the use of physics- and data-driven model acceleration strategies. TAVI, transcatheter aortic valve implantation.
Physics-driven model reduction: Preserving physics and reducing costs
Physics-driven approaches to model reduction such as reduced order models (ROMs) seek to compress the computational degrees of freedom required to solve a physical system, while ensuring that the governing equations that define the physics (mass conservation, momentum balance) are preserved. Techniques such as Proper Orthogonal Decomposition construct a low-dimensional basis from a set of high-fidelity “snapshot” simulations that parametrically span the problem of interest, enabling new parameter configurations to be simulated at a fraction of the original computational costs. 2 Recent work in the context of TAVI has demonstrated that such ROMs can enable real-time valve stent deformation simulations and thus capture device-specific mechanical behavior with significant speed-ups relative to full-order FEA. 3 Since these methods operate within the framework of the governing physics, their key strength lies in physical consistency and accuracy. Their primary limitations, however, are the cost and complexity of the offline training phase, as well as the non-generalizable nature of traditional reduced models which often struggle with patient-specific anatomical variability.
Data-driven surrogate modeling: Learning the map without physics
Data-driven approaches such as the GNN framework developed by Hossen et al take a fundamentally different route. Rather than simplifying the physical equations, they learn a direct input-output mapping from training data without explicitly encoding the governing physics. The power of such approaches lies in its flexible and generalizable nature. Deep learning architectures, and in particular graph-based methods, are well-suited to handle anatomical variations across patient cohorts. Such data-driven surrogate models have now been demonstrated across a range of biomechanics applications, including wall shear stress estimation in coronary arteries, as well as high-speed predictions of ventricular mechanics.4,5 Once these models are trained, inference is computationally trivial and comes at a fraction of traditional simulations. The primary limitations are complementary to those of physics-based ROMs, in that data-driven models require extremely large, representative training datasets, and that they extrapolate poorly outside the training regime.
The case for hybrid approaches and real-world translation
Naturally, the most robust path to clinically deployable computational modeling for cardiovascular applications lies not in either paradigm alone, but in hybrid frameworks that integrate physics with data. For instance, physics-informed neural networks embed the governing physics directly into the neural network training, thus providing physically consistent, real-time vascular flow simulations. 6 Similarly, ROM-augmented surrogate models can enable structural deployment simulations to be performed within milliseconds while retaining physical fidelity. 7 These hybrid strategies also offer natural pathways towards uncertainty quantification, i.e., the model's confidence in its own predictions. Overall, ROM-based approaches provide physically grounded simulations, while methods such as neural networks provide geometrical flexibility and inference speeds that traditional ROMs struggle to achieve.
While these acceleration methodologies remain largely in the research domain, several real-world examples already demonstrate the translation of computational modeling into clinical practice. For instance, HeartFlow's FDA-approved FFR-CT platform enables hemodynamic simulations to derive non-invasive estimates of fractional flow reserve, with strong diagnostic performance. 8 In the structural heart space, FEops’ HEARTguideTM enables patient-specific planning for TAVI via artificial intelligence (AI)-driven predictive simulations and has shown strong prospective clinical evidence of the platform's planning utility. 9 Similarly, DASI simulations’ FDA-approved precision TAVI platform employs hybrid physics-based AI simulations to predict device-anatomy interactions, with recent work demonstrating its effectiveness in evaluating the risk of coronary obstruction. 10 The work presented by Hossen et al can be contextualized as the next generation of the same translational efforts, seeking to further reduce computational burden and extend real-time predictive modeling capabilities.
Beyond planning: Enabling lifetime management and large-scale in-silico studies
It is worth emphasizing that the clinical impact of computational acceleration extends beyond pre-operative surgical planning. Real-time biomechanical modeling can enable lifelong management of patients, including evaluating the need for future valve-in-valve procedures or the risk of structural valve degeneration. This is precisely the critical value of the DT paradigm, opening the door to new categories of collaborations between scientists and clinicians (who serve as the “human-in-the-loop” of the DT). Large-scale in-silico studies in the form of virtual clinical trials can systematically evaluate the mechanistic relationships between anatomy and procedural outcomes as well across entire patient registries with rigorous statistical power. Novel devices or modified deployment strategies can also be evaluated computationally across diverse virtual populations, as evidenced by the ENRICHMENT trial for mitral valve repair. 11 The same acceleration paradigms that enable real-time pre-procedural planning can therefore also be used to power a new generation of mechanistic research, thus reducing the time and costs of randomized clinical trials.
Looking forward
The study presented by Hossen et al serves as a demonstration of this broader vision. Important challenges remain that must be addressed, such as the need for richer geometric feature representations, explicit physics-informed training strategies, and prospective clinical validation. Nevertheless, the trajectory towards the development of patient-specific cardiovascular DTs is clear. The convergence of high-fidelity computational biomechanics, physics-driven model reduction, geometric deep learning, and large-scale clinical imaging datasets is creating the conditions for a transformation in how clinical teams can plan for and evaluate structural heart interventions.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L. P. Dasi is a stakeholder in DASI Simulations.