
Abstract
This is a visual representation of the abstract.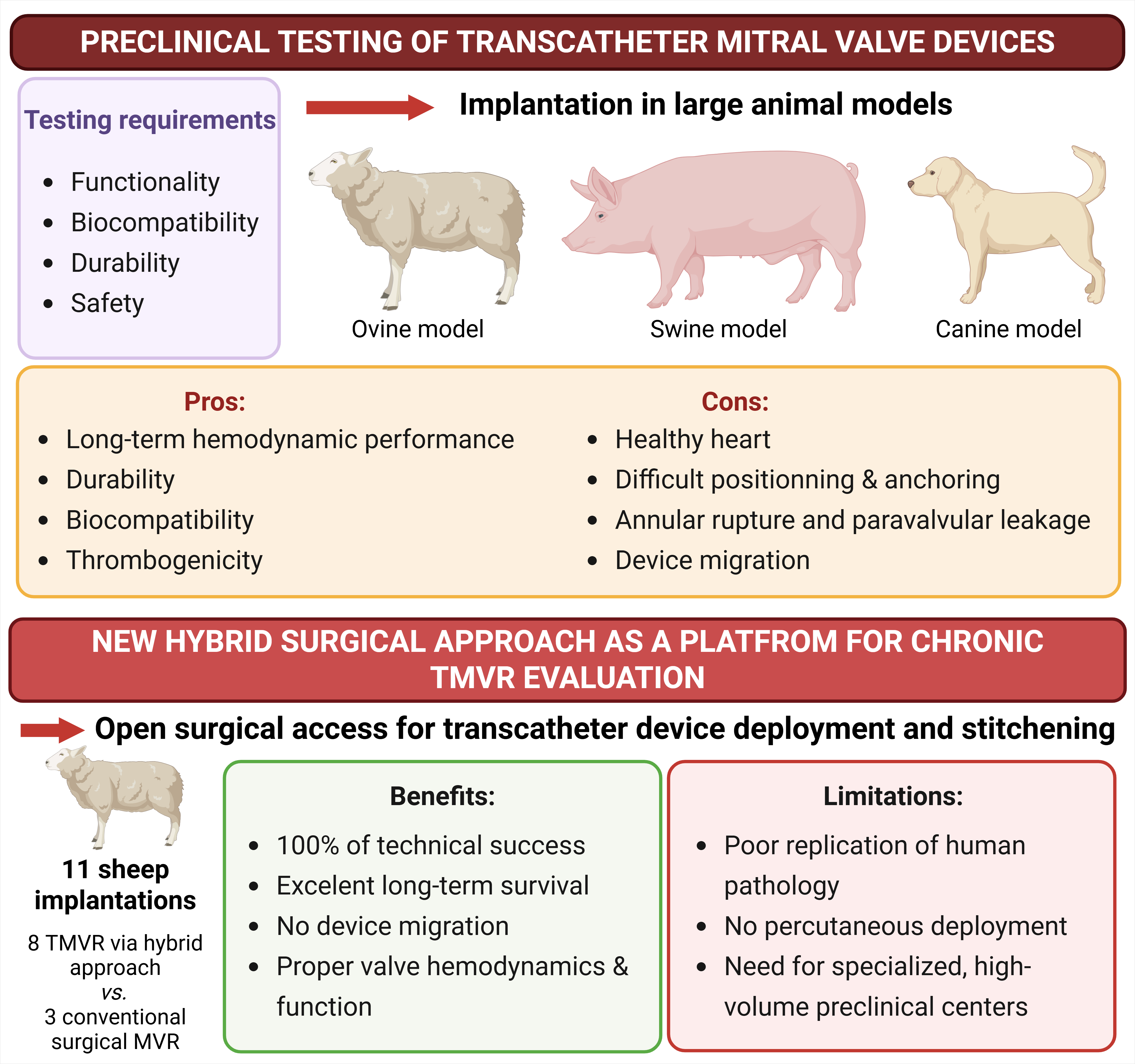
Over the past two decades, transcatheter valve interventions have profoundly transformed the management of valvular heart diseases: the success of transcatheter aortic valve implantation (TAVI) has reshaped treatment paradigms, extending minimally invasive solutions from inoperable to low-risk patients and accelerating innovation in device design, delivery systems, and procedural strategies. 1 In comparison to TAVI, transcatheter mitral valve replacement (TMVR) remains a far more complex challenge, especially due to the complex anatomy of the mitral valve, the dynamic geometrical changes of the mitral annulus during cardiac cycle, and the close relationship of the mitral valve with the left ventricular outflow tract (LVOT) increasing the risk of LVOT obstruction.2,3 Nowadays, several TMVR devices have been developed, all with particular anchoring mechanisms and deployment procedures, associated with specific benefits and drawbacks.2,3
Despite these obstacles, the clinical need of TMVR is substantial. Many patients with severe mitral valve disease are poor surgical candidates, and current transcatheter mitral valve repair techniques are not applicable. As a result, TMVR technologies are rapidly emerging and may represent a potential game changer in the coming years. However, this technological acceleration comes with a critical prerequisite: robust and reliable preclinical validation (Figure 1).
Benefits and limitations of the new hybrid approach for the chronic evaluation of TMVR devices. TMVR: transcatheter mitral valve replacement. Created in BioRender. 4
A central limitation of TMVR preclinical development is the absence of a diseased mitral valve in large animal models. In humans, annular calcification, leaflet pathology, and subvalvular remodeling provide natural anchoring mechanisms for transcatheter devices. In contrast, the implantation in healthy animal, particularly in sheep, poses fundamental challenges: device fixation, stability, and long-term performance may be compromised by the animal model itself rather than intrinsic device failure. This issue has historically resulted in early mortality and confounded interpretation of chronic performance data in preclinical testing.
In this context, the study by Carney et al addresses a critical methodological gap by proposing an innovative hybrid surgical approach for TMVR implantation in a non-diseased ovine model (Figure 1). The objective of the study was not merely to test a specific device, but to develop a reproducible strategy that allows secure implantation and long-term evaluation of TMV under physiological hemodynamic conditions.
Using a hybrid approach that combines open surgical access with transcatheter valve deployment under direct visualization, coupled with a stitched device, the authors successfully implanted the Abbot next-generation Cephea in eight sheep, with three additional animals receiving a surgically implanted bioprosthetic valve (Mosaic, Medtronic) as controls. All 11 procedures were technically successful, with no device-related intraoperative failures. Importantly, survival was excellent, with 100% survival at 30 days and 88% at the 20 weeks, the single early euthanasia (at day 58) being related to a surgical wound infection without device dysfunction. The authors did not report any device migration during long-term follow-up.
Hemodynamic performance and valve function assessed over the follow-up were reassuring. Echocardiographic and invasive assessments demonstrated comparable valve function between the hybrid TMVR group and surgical control group. Notably, a higher degree of mitral regurgitation was observed early after implantation in TMVR, particularly at the 30-day evaluation, whereas this difference was no longer present at long-term follow-up, with only a mild degree of regurgitation observed in some cases, comparable in both groups. On the other hand, mitral valve gradients were higher in the surgically implanted control group, both at rest and under dobutamine stress, suggesting favorable hemodynamic performance of the transcatheter device within this controlled implantation framework. Post-mortem analysis further confirmed good valve positioning, biocompatibility, and the absence of significant extracardiac damage attributable to the device.
Beyond the performance of a single prosthesis, the major contribution of this work lies in the validation of a hybrid implantation strategy as a platform for chronic TMVR evaluation. By minimizing model-related adverse events and ensuring stable device fixation, this approach enables meaningful long-term data acquisition, an essential step for regulatory approval and clinical translation.
Nevertheless, several limitations must be acknowledged. As with all animal studies, the ovine model does not fully replicate human (patho)physiology, particularly mitral valve pathology, and the extrapolation of tissue-device interactions remain imperfect. Other large animal models can be used: indeed, pigs presented similar cardiovascular anatomy and function as compared to human, as well as close human genetic resemblance, offering a proper physiological platform to test valve prosthetic devices, while the important limitation related to the significant growth of conventional pigs during long-term follow-up could be circumvented through the use of minipigs, such as Yucantan.5,6 However, the translation of the current approach developed in an ovine model to other large animal models would need to be tested and validated. Moreover, this hybrid approach, although allowing durability testing of percutaneous devices, is not a fully percutaneous deployment and therefore does not reproduce the procedural challenges of classical transcatheter implantation. In addition, the reproducibility of this strategy is inherently dependent on the availability of a highly specialized, multidisciplinary team with extensive experience in cardiopulmonary bypass and open-heart surgery applied to a large animal model, which may limit its applicability outside selected high-volume preclinical centers. However, this limitation may also be viewed as a strength: by isolating device performance from delivery-related confounders, the model places the prosthesis in a physiological hemodynamic environment that is otherwise difficult to achieve in healthy animals. The use of a surgically implanted bioprosthetic valve as a control group is logical and defensible, representing a gold-standard for durability and reproducibility. Still, differences in valve design, sewing cuffs, and effective orifice areas may partially explain some of the observed hemodynamic differences. The presence of mild mitral regurgitation in both groups also warrants discussion, particularly regarding whether this finding is related to the implantation technique, the absence of annular pathology, or intrinsic device characteristics. Finally, the systematic post-mortem assessment of valve tissue and extracardiac organs, while comprehensive, raises important questions about the clinical relevance of histopathological findings observed in healthy animals.
This study should be viewed within the specific development pathway of the Abbott Cephea TMVR system. To date, publicly available data on the Cephea platform have been largely limited to early clinical feasibility reports and its inclusion in broader reviews of the TMVR landscape, with little published information addressing chronic preclinical performance. The first-in-human experience with the Cephea transseptal system demonstrated procedural feasibility and acceptable acute hemodynamic outcomes in high-risk patients, supporting the translational potential of the device. 7 However, as comprehensive TMVR reviews point out, most contemporary TMVR systems—including Cephea—have progressed towards clinical evaluation with a limited amount of large animal-derived chronic data, reflecting the intrinsic challenges of anchoring transcatheter mitral prostheses in non-pathological anatomy.2,3 Prior experimental work has underscored how model-related factors, rather than device failure, often confound preclinical TMVR evaluation in large animals. 8 In this context, the hybrid implantation strategy reported by Carney et al represents a pivotal addition to the Cephea preclinical evidence base, providing a structured and reproducible framework for prolonged in vivo assessment of valve performance under physiological hemodynamic conditions.
In conclusion, Carney et al present a technically elegant and scientifically rigorous solution to one of the most persistent obstacles in TMVR preclinical validation. Their hybrid surgical approach provides a valuable and reproducible framework for long-term evaluation of transcatheter mitral valves in large animal models. As TMVR technologies continue to evolve, such methodological advances will be essential to bridge the gap between innovation and safe clinical translation.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.