
Abstract
Background
The Ross procedure (RP) is technically complex but offers superior hemodynamics and improved long-term survival compared to prosthetic aortic valve replacement, particularly in young adults. Despite these advantages, widespread adoption has been limited by concerns regarding technical complexity, operative risk, and the learning curve associated with Ross program development. This study evaluates the early experience of the first 50 RPs performed by a lead surgeon compared to propensity-matched surgical aortic valve replacement (SAVR).
Methods
The RP has historically been criticized for its higher operative complexity and perceived risk during the learning curve. To address this, we compared the first 50 RPs performed by a lead surgeon within a structured Ross program to 50 propensity-matched isolated SAVR patients. The primary outcome was 30-day mortality, while secondary outcomes included perioperative events, operative times, and valve hemodynamics.
Results
The Ross cohort was younger (42 vs 53 years, P < .01) and had lower rates of hypertension (40.0% vs 62.1%, P = .005). Twenty six cases (52%) were performed with structured two-attending mentorship. After propensity matching, no 30-day mortality was observed in either group. Ross procedures had longer cross-clamp times (183 [161-211] vs 83 [66-103] min, P < .01) but achieved lower mean aortic valve gradients (4 [3-4] vs 9 [7-12] mm Hg, P < .01) with similar lengths of stay (6 [5-7] days vs 6 [5-7] days, P = .81). Although several important perioperative technical events occurred during the Ross experience, including unplanned coronary bypass grafting and reoperation for autograft dysfunction, these events were recognized promptly and managed successfully without excess mortality or major morbidity.
Conclusions
Our early experience suggests that establishment of a modern Ross program is feasible with excellent early outcomes when supported by careful patient selection, structured mentorship, operative standardization, multimodality imaging, and robust institutional infrastructure. Importantly, transparent reporting of technical complications, lessons learned, and evolving perioperative strategies during the learning curve may help guide safe dissemination of the Ross procedure to additional centers.
This is a visual representation of the abstract.
Key Points
A dedicated Ross program can be established safely with structured mentorship, careful patient selection, and robust institutional infrastructure.
Early technical complications and return to bypass events did not translate into excess mortality or major morbidity when promptly recognized and managed.
Standardized multimodality imaging, pulmonary valve assessment, and strict postoperative blood pressure management were critical components of program development.
Transparent reporting of learning curve experiences and evolving operative strategies may help guide safe dissemination of the Ross procedure to additional centers.
Introduction
The Ross procedure offers several unique advantages for young adults requiring aortic valve replacement, including excellent hemodynamics, freedom from anticoagulation, and potential for growth in younger patients.1‐4 Multiple studies from experienced centers have demonstrated favorable long-term survival and quality of life compared to conventional prosthetic valve replacement.2,5‐7 However, its technical complexity and longer operative times have limited widespread adoption, with concerns about the potential risks and complications during the learning phase. There are also concerns about the additional costs to both patients and healthcare systems during this early experience. As a result, the procedure is performed primarily at specialized referral centers.4,8‐10
While established Ross centers have published excellent outcomes, there remains uncertainty about the feasibility of establishing new Ross programs. The learning curve, mentorship requirements, and institutional resources needed to launch a successful program remain poorly defined.11,12 This knowledge gap has likely deterred many surgeons and institutions from adopting the procedure, despite its potential benefits for appropriate patients.
Our study addresses this gap by evaluating the early outcomes of the first 50 Ross procedures (RPs) performed by a lead surgeon at our institution. While RPs were previously performed at our center at low frequency with excellent results, we sought to establish a more programmatic approach to create a Ross Center of Excellence. As described by El-Hamamsy and colleagues, 13 a true Ross Center of Excellence requires multiple integrated components: a reference Ross surgeon with dedicated expertise, cardiologists with specialized valve knowledge, multimodality imaging capabilities for detailed assessment, advanced ICU services, dedicated cardiac anesthesia, and a specialized Ross surgical clinic for longitudinal follow-up. By implementing structured mentorship with two-attending coverage for early cases and comparing results to propensity-matched surgical aortic valve replacements (SAVR), we sought not only to evaluate the feasibility of establishing such a program with appropriate institutional support, but also to transparently describe the early experience, technical challenges, evolving operative strategies, and multidisciplinary infrastructure involved in modern Ross program development. As increasing interest in the Ross procedure has led more centers to consider program development, there remains limited practical guidance regarding patient selection, operative standardization, mentorship structure, perioperative management, and mitigation of technical complications during the learning curve. We therefore hope that sharing the lessons learned during the first 50 cases of our program may help guide safe dissemination of the Ross procedure at other institutions.
Methods
Study Population
We conducted a retrospective cohort study analyzing the first 50 consecutive Ross procedures performed by a lead surgeon (JPB) at our institution between September 2022 and June 2024. The study was approved by the Mass General Brigham Institutional Review Board (Protocol No. 2024P002495, approved on 17 September 24). Informed consent was not required due to the retrospective nature of the study.
The study population included all adult patients who underwent the RP or isolated SAVR. We excluded patients who underwent concomitant cardiac procedures. For the control group, we included patients who were ≤60 years old and underwent elective isolated SAVR from 2015 onward.
Data were derived from the institution's prospectively maintained Ross database, and also incorporates Society of Thoracic Surgeons (STS) Adult Cardiac Surgery Database definitions and variables. Retrospective chart review was additionally performed for verification of operative details and Ross-specific variables not routinely captured in the STS dataset.
Definitions
The RP was performed as a full root replacement technique in all cases, which included harvesting the pulmonary autograft, excision of the diseased aortic valve, implantation of the pulmonary autograft in the aortic position, and reconstruction of the right ventricular outflow tract with a pulmonary homograft. 14 Early experience was defined as the first 50 consecutive cases performed by the lead surgeon (last author). Two-surgeon cases were defined as procedures where a second experienced cardiac surgeon assisted for critical portions of the operation.
During the first 26 cases, a second experienced attending cardiac surgeon was present during critical portions of the operation as part of a structured mentorship model. This primarily involved Dr Duke Cameron, who has extensive experience in complex aortic and root surgery. As operative standardization and surgeon experience increased, the later cases were performed without routine two-attending coverage. Standard operative times, including cardiopulmonary bypass and cross-clamp times, were recorded prospectively in our institutional database.
Preoperative Evaluation and Patient Selection
All patients underwent comprehensive transthoracic echocardiography and ECG-gated computed tomographic angiography (CTA) with multiplanar reconstruction to assess annular dimensions, root geometry, ascending aortic pathology, and coronary anatomy. Pulmonary valve assessment was additionally performed intraoperatively using multiview transesophageal echocardiography and direct epicardial imaging prior to autograft harvest. Additional studies including coronary angiography and transesophageal echocardiography were obtained selectively when indicated. 15
During the initial phase of program development, there was selection toward patients with predominantly stenotic or mixed aortic valve disease, relatively symmetric root geometry, preserved ventricular function, and favorable annular dimensions. However, patients with redo operations, endocarditis, aortic regurgitation, and root pathology were also included early in the experience.
Study Outcomes
Baseline characteristics included patient demographics, comorbidities, and aortic valve characteristics. The primary study outcome was 30-day mortality. Secondary study outcomes included postoperative morbidity (reoperation due to bleeding, renal failure, deep sternal wound infection, stroke, prolonged ventilation, pneumonia, new pacemaker placement, atrial fibrillation, ICU readmission, 30-day readmission) and valve hemodynamics.
Statistical Analysis
Continuous variables are presented as median [interquartile range] and categorical variables as number (percentage). Between-group comparisons for baseline characteristics used Wilcoxon rank-sum test for continuous variables and chi-square or Fisher's exact tests for categorical variables. Normality was assessed using skewness and kurtosis.
Propensity score matching was performed to balance baseline characteristics between RP and SAVR patients. The matching model included 15 clinically relevant preoperative variables: demographics (age, sex, race, BMI), cardiovascular risk factors (aortic stenosis, hypertension, prior valve surgery, cardiovascular disease, peripheral vascular disease), comorbidities (renal failure, diabetes, chronic lung disease, NYHA class, infective endocarditis, smoking status). Matching was conducted using a greedy matching algorithm with a 1:1 ratio and a caliper width of 0.15. The quality of matching was assessed using standardized mean differences, with values <0.2 indicating good balance between groups. 16
After matching, between-group comparisons were performed using Wilcoxon rank-sum test for continuous variables and chi-square or Fisher's exact tests for categorical variables. For the primary outcome of 30-day mortality and secondary outcomes, univariable logistic regression was conducted. Statistical significance was set at P < .05. Variables included in the analysis had less than 5% missing data. We performed complete case analysis for variables with missing data. All analyses were conducted using Python version 3.12.4.
Results
Patient Characteristics
In the unmatched cohort shown in Table 1, Ross patients (n = 50) were younger (41.5 [36.0-47.8] vs 53.0 [47.0-58.0] years, P < .001) and had lower rates of hypertension (40.0% vs 62.1%, P = .005) compared to controls (n = 340). Within the Ross cohort, bicuspid valve morphology was most common (70%), followed by tricuspid (16%) and unicuspid (14%) valves. Valve pathology included isolated aortic stenosis in 48% of patients, isolated aortic insufficiency in 28%, and mixed AS/AI disease in 24%. Active endocarditis was present in 6% of the Ross cohort and 26% had prior sternotomy.
Baseline Characteristics Before Matching.
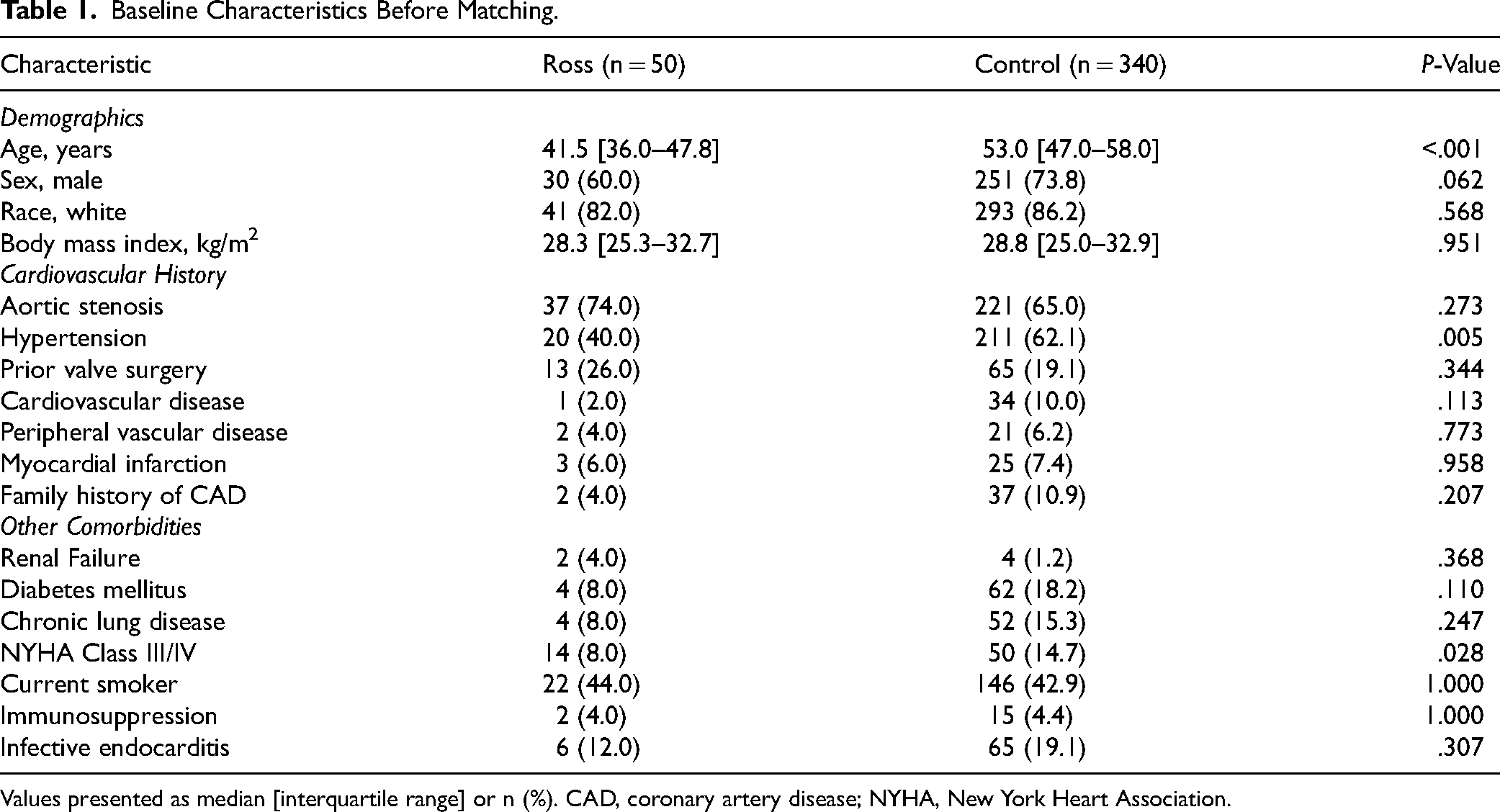
Values presented as median [interquartile range] or n (%). CAD, coronary artery disease; NYHA, New York Heart Association.
After propensity matching (Table 2), all baseline characteristics were well-balanced between groups (n = 50 each), with standardized mean differences <0.2 for all variables. The matched cohorts in Table 2 showed similar demographics including age (41.5 [36.0-47.8] vs 42.5 [35.0-52.8] years, P = .687), male sex (60.0% vs 58.0%, P = 1.000), and BMI (28.3 [25.3-32.7] vs 27.4 [24.7-32.4] kg/m2, P = .723).
Baseline Characteristics After Matching.
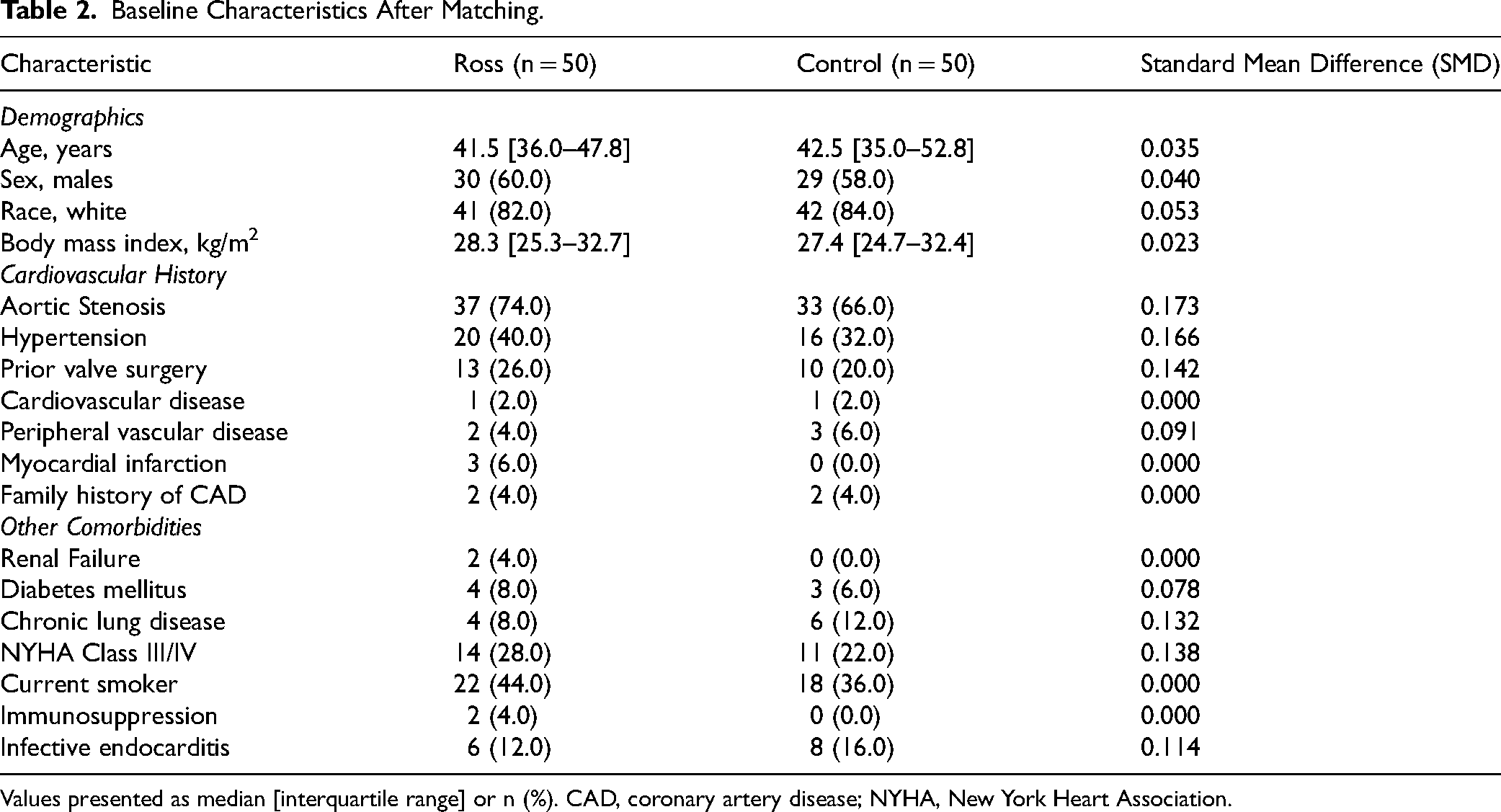
Values presented as median [interquartile range] or n (%). CAD, coronary artery disease; NYHA, New York Heart Association.
Operative Characteristics
Twenty six (52%) RPs were performed with a second experienced attending surgeon present during critical portions of the operation. As expected, Ross procedures were associated with significantly longer operative times compared to SAVR (Table 3), including longer cross-clamp time (183.0 [161.2-211.2] vs 83.0 [66.5-103.0] minutes, P < .001), cardiopulmonary bypass time (224.5 [216.0-259.0] vs 112.5 [96.0-136.5] minutes, P < .001), and total operative time (448.5 [415.2-522.8] vs 325.5 [279.2-379.5] minutes, P < .001). Selective annular stabilization strategies were utilized in 46% of Ross patients, while sinotubular junction stabilization was performed routinely in 100% of cases. No patients underwent routine full Dacron inclusion of the autograft.
Operative Characteristics.
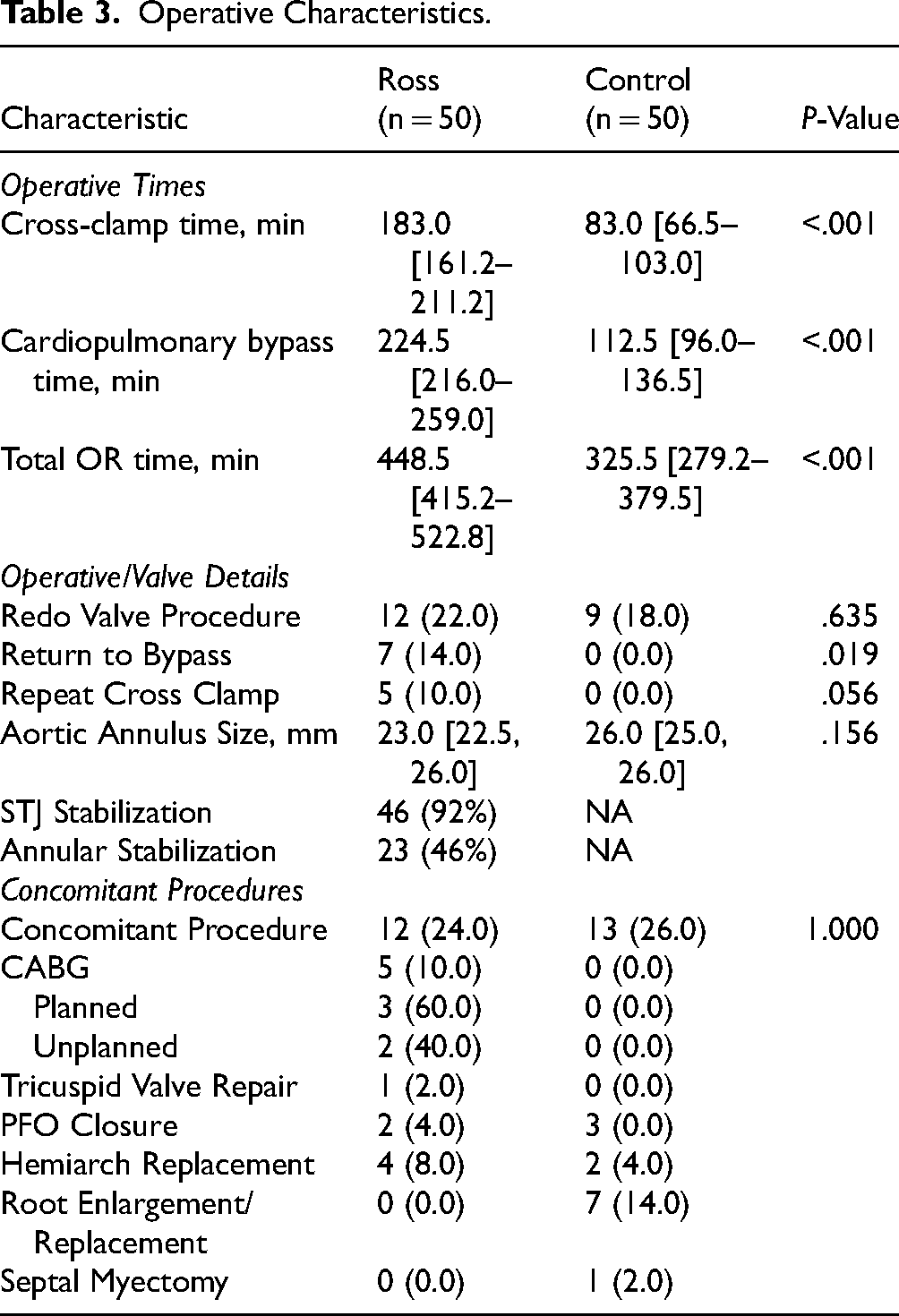
Seven patients (14%) in the RP group required return to bypass (RTB) for intraoperative complications, compared to none in the control group (P < .019). Of these RTB cases, four (57%) were for anastomotic bleeding, one for a severe protamine reaction, one for right ventricular failure requiring saphenous vein grafting due to a coronary button complication, and one for repair of a commissural leak. Five patients required repeat aortic cross clamping (Supplemental Table 1). All seven patients left the operating room in stable condition with well-functioning autografts.
Furthermore, five (10%) patients in the Ross group underwent concomitant coronary artery bypass grafting (CABG), compared to none in the matched control group. Of these five cases, three were planned (two for single-vessel right coronary artery disease and one was due to a preoperative right coronary artery occlusion from a previous bioprosthetic valve replacement), while two were unplanned (one for right heart failure secondary to an intraoperative coronary button complication and one for inadvertent coronary artery injury during autograft harvest). Both unplanned CABGs utilized saphenous vein grafts to the right coronary artery distribution and patients recovered without long-term ventricular dysfunction.
Evaluation of operative times across the first 50 Ross procedures demonstrated that cross-clamp times did not progressively decrease during the series, with mean cross-clamp times of 156 min for cases 1–10, 171 min for cases 11–20, 184 min for cases 21–30, 221 min for cases 31–40, and 218 min for cases 41–50. We believe this likely reflects increasing procedural complexity and expanding patient selection over time, including more redo operations, root pathology, and technically challenging anatomy as institutional and surgeon confidence with the Ross procedure increased.
Clinical Outcomes
There were no deaths at 30 days in either group (Table 4). There were no occurrences of stroke or deep sternal wound infection in either group. One Ross patient required new postoperative dialysis, compared to none in the SAVR group. This patient had normal renal function preoperatively but experienced a prolonged postoperative course requiring temporary dialysis support in the setting of volume overload and metabolic derangements, with eventual renal recovery prior to discharge. The Ross group also had a higher rate of postoperative blood product transfusion (28.0% vs 12.0%, P = .080), though this did not reach statistical significance due to the small sample size. Postoperative atrial fibrillation rates were similar (12.0% vs 16.0%, P = .773), as were readmission rates (8.0% vs 6.0%, P = 1.000) and permanent pacemaker placement (4.0% vs 2.0%, P = 1.000). Both permanent pacemakers in the RP group occurred in patients with unicuspid aortic valves who underwent both STJ and VAJ reinforcement during the RP.
Clinical Outcomes.
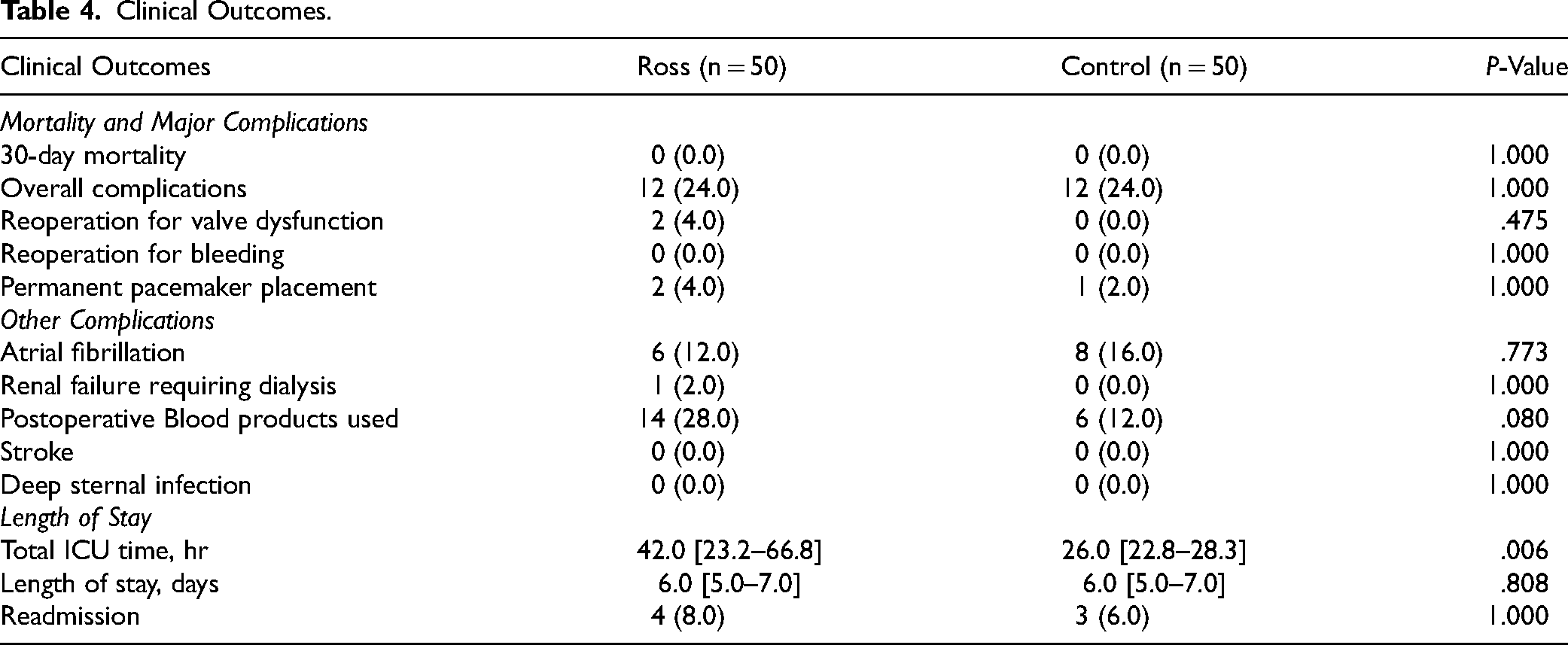
While total ICU time was longer in the Ross group (42.0 [23.2-66.8] vs 26.0 [22.8-28.3] hours, P = .006), the overall length of stay was similar between groups (6.0 [5.0-7.0] vs 6.0 [5.0-7.0] days, P = .808). As part of our protocol, all patients undergo transthoracic echocardiography the day before discharge, as the RP can demonstrate evolving findings in the early postoperative period. One patient, despite having trace neo-aortic insufficiency on intraoperative TEE, developed severe AR on predischarge TTE. After multidisciplinary discussion, decision was made to reoperate. The patient was found to have two commissural leaks. Despite attempted repair, the patient ultimately required autograft explant and mechanical aortic root replacement and was discharged in stable condition. This case led to two important practice changes: implementing routine epicardial echocardiography and modifying our valve inspection protocol prior to harvest, specifically to exonerate commissural fenestrations.
Hemodynamic Outcomes
As shown in Table 5, Ross patients demonstrated superior hemodynamics with significantly lower mean aortic valve gradients (4.0 [3.0, 5.0] vs 9.0 [7.0, 11.5] mm Hg, P < .001). There were no instances of greater than mild aortic regurgitation or paravalvular leak in either group after aortic valve replacement. The homograft demonstrated excellent early function with low mean gradients (4 [3, 5] mm Hg) and peak gradients (9 [6, 11] mm Hg), with no cases of greater than mild pulmonary regurgitation.
Hemodynamic Outcomes.
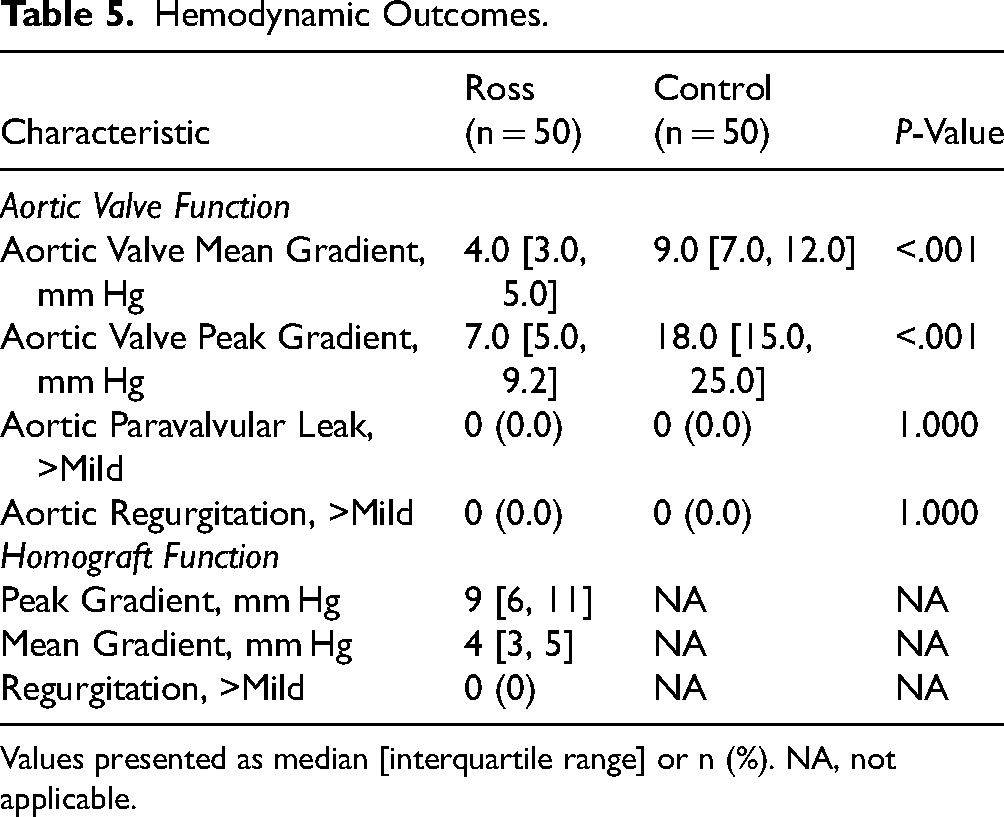
Values presented as median [interquartile range] or n (%). NA, not applicable.
Discussion
The principal findings of this study demonstrate that with proper training, mentorship, and robust institutional support, establishing a Ross program is feasible with excellent early outcomes. This is particularly important given the recent findings by Mazine et al demonstrating the volume/outcomes associated with the RP. 17 Despite significantly longer operative times and more RTB for intraoperative complications, we observed no mortality in our first 50 cases. The superior hemodynamics achieved with the pulmonary autograft reflect the known benefits of the Ross procedure, 6 and our experience suggests that with appropriate infrastructure and support, new programs can achieve good results from the outset.
Previous single-center studies have documented excellent outcomes with the Ross procedure at experienced centers.5,18‐22 Large series from established programs have demonstrated excellent durability and survival. El-Hamamsy et al 2 demonstrated superior survival and quality of life with the Ross compared to mechanical AVR in young adults. Similarly, Skillington's group 23 showed outstanding freedom from reoperation in their 20-year series. However, these studies represent mature programs with extensive experience. While their results highlight the long-term benefits of the Ross procedure, there remains limited data about the early experience of establishing new Ross programs, leaving uncertainty about the optimal approach to program development.
Our approach aimed to mitigate the challenges of initiating a Ross program through several key strategies. First, the last author obtained a significant amount of multinational and institutional training dedicated to learning the RP. Next, we utilized a structured mentorship program with two attending coverage for the first 26 cases, which included an experienced Ross surgeon. This approach allowed for real-time decision-making support and technical assistance during critical portions of these complex operations. The RP is a high cognitive load operation and, in our opinion, should be done with two surgeons in the early experience if not indefinitely. We performed a comprehensive global survey of Ross practices and found that nearly 50% of all RPs are performed by two attending surgeons. 24 Next, we identified early that consistent reliable pulmonary valve imaging by TEE was challenging and thus implemented routine epicardial echocardiography. This technique achieves high fidelity pulmonary valve imaging by placement of a probe directly onto the RVOT, and obviates the need for experienced pulmonary valve imagers. Next, careful patient selection was employed, focusing on young patients with appropriate root anatomy. Finally, we benefited from a highly experienced cardiac surgery team at a high-volume center with extensive experience in complex aortic valve and root surgery. Importantly, we established standardized protocols for perioperative and postoperative care, 25 ensuring the entire clinical team—from advanced practice providers to intensive care staff—understands the unique aspects of Ross patient management. This comprehensive approach likely contributed to our ability to achieve outcomes comparable to conventional SAVR.
While operative times were longer and there were more intraoperative issues requiring RTB, as expected for this more complex procedure, this did not translate into increased morbidity or length of stay. ICU length of stay was longer for Ross patients; however, this was largely attributable to the need for intravenous antihypertensive agents during the first 48 postoperative hours to maintain a systolic blood pressure less than 110mm Hg. As part of our standardized postoperative Ross protocol, patients underwent strict blood pressure management aimed at minimizing early autograft stress and promoting long-term durability. In general, systolic blood pressure was targeted to <110 mm Hg during the first six postoperative months. First-line outpatient therapy typically consisted of beta-blockade followed by angiotensin receptor blocker therapy when appropriate. 15 Importantly, operative times did not progressively decrease across the first 50 cases, which likely reflects increasing procedural complexity and expanding patient selection over time, including more redo operations, root pathology, and technically challenging anatomy as institutional and surgeon confidence with the Ross procedure increased. These findings suggest that procedural complexity rather than technical inefficiency may have been the dominant driver of operative duration during program maturation. The Ross procedure mandates dedication to precision and accuracy, and to the importance of executing each step of the operation without anastomotic issues cannot be overstated. As a result, we feel that with appropriate myocardial protection, cross-clamp time should not be the focus, rather flawless execution of each step of the operation. A series of groups have published methods to decrease operative times (woo et al, emani at al.) however, our opinion is that early in the experience of this operation, case duration should not be a priority.
These findings have important clinical implications for surgeons and institutions considering establishment of a Ross program. The historical concentration of Ross procedures at a few select centers has limited access to this beneficial operation for many patients. Our experience demonstrates that with appropriate preparation, mentorship, and institutional infrastructure, the procedure can be safely introduced at new centers. Our early experience represents the initial phase in developing a comprehensive Ross Center of Excellence, which ultimately includes advanced imaging, patient selection, systematic long-term follow-up, and surgical expertise. 13 This multidisciplinary foundation provides the framework for expanding access to the Ross procedure while maintaining optimal outcomes.
Several important lessons emerged during early program development. First, careful patient selection during the initial experience remains critical, particularly favoring patients with predominantly stenotic or mixed valve disease, preserved ventricular function, relatively symmetric root geometry, and favorable annular anatomy. Moreover, patients should be relatively free of comorbidity and carefully selected to ensure they can tolerate longer operative times and low postoperative blood pressure. Second, structured mentorship with experienced aortic surgeons and routine two-attending coverage during early cases likely contributed substantially to procedural safety and operative decision-making. Third, multimodality imaging and systematic pulmonary valve assessment, including direct epicardial imaging, became increasingly important after several early technical complications involving commissural leaks and pulmonary valve fenestrations. Finally, strict postoperative blood pressure management and operative standardization across the multidisciplinary care team were essential components of the program infrastructure.
Limitations
Importantly, this experience occurred within a high-volume academic cardiac surgery center with extensive expertise in complex aortic and valve surgery, advanced imaging capabilities, dedicated cardiac anesthesia and ICU support, and robust multidisciplinary valve infrastructure. Furthermore, the first 26 cases involved structured mentorship with Dr Duke Cameron, one of the world's most experienced aortic surgeons. Access to this level of institutional infrastructure and mentorship may not be broadly generalizable to all centers seeking to establish Ross programs. Additionally, this was a retrospective single-center study with a relatively small sample size, limiting statistical power and long-term interpretation of clinical outcomes.
Conclusion
Our early experience demonstrates that establishment of a modern Ross program is feasible with excellent early outcomes when supported by careful patient selection, structured mentorship, operative standardization, multimodality imaging, and robust institutional infrastructure. Transparent reporting of technical complications and evolving perioperative strategies during the learning curve is critical to safely disseminating the Ross procedure to additional centers. We hope the lessons learned from this early experience may help guide other institutions seeking to develop Ross centers of excellence.
Supplemental Material
sj-docx-1-hvs-10.1177_30494826261468490 - Supplemental material for Establishing a Ross Program: Early Experience and Outcomes of the First 50 Cases Compared to Propensity-Matched Aortic Valve Replacements
Supplemental material, sj-docx-1-hvs-10.1177_30494826261468490 for Establishing a Ross Program: Early Experience and Outcomes of the First 50 Cases Compared to Propensity-Matched Aortic Valve Replacements by Lucy Nam, Keshika Catakam, Ruby Singh, Arminder S. Jassar, Duke E. Cameron, Thoralf M. Sundt III and Jordan P. Bloom in Journal of the Heart Valve Society
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.