
Abstract
Objective:
This study aimed to investigate the factors involved in the development and progression of metabolic dysfunction-associated fatty liver disease (MASLD) in older adults from various aspects.
Methods:
Among general residents aged ≥60 years who participated in a health checkup project, 124 individuals in a normal group and 77 in an MASLD group were targeted in this study. Differences in nutrient intake, MASLD-related single nucleotide polymorphisms (SNPs), and oral and gut microbiota between the normal and MASLD groups were investigated. Furthermore, multivariate analysis was conducted to determine which cardiometabolic criteria were associated with the identified variables.
Result:
The MASLD group had increased oral Veillonella and Megasphaera and decreased gut Blautia. Oral Veillonella and Magasphaera were positively associated with body mass index (BMI), waist circumference, and systolic blood pressure. Gut Blautia negatively correlated with BMI, waist circumference, fasting blood sugar, HbA1c, triglycerides, and positively correlated with high-density lipoprotein cholesterol. However, no association was observed between nutritional intake and SNPs.
Conclusion:
Because oral and gut microbiota are strongly involved in MASLD in older individuals, improving oral hygiene and probiotics may prevent the onset and progression of MASLD by improving the oral and gut environment.
Introduction
The proportion of older adults in the population is rising, owing to an increase in the median age of the population, which is associated with an increase in life expectancy. Population aging and the increase in lifestyle-related diseases, including those in Japan, place a heavy burden on healthcare costs and resource allocation.
Fatty liver is asymptomatic; however, it can cause cardiovascular disease and hepatitis, and is a risk factor for cirrhosis and liver cancer. Furthermore, recent studies have shown that fatty liver is associated not only with obesity but also with diabetes mellitus, dyslipidemia, hypertension, and atherosclerosis, and is considered a hepatic phenotype of lifestyle-related diseases (Castillo-Núñez et al., 2024; Leite et al., 2014). Non-alcoholic fatty liver disease (NAFLD) was renamed metabolic dysfunction-associated fatty liver disease (MASLD) in 2023 (Rinella et al., 2023). With the name change from NAFLD to MASLD, the diagnostic criteria now explicitly require fatty liver along with at least one of the following five cardiometabolic criteria: obesity, hypertension, diabetes, low high-density lipoprotein (HDL) cholesterol, and high triglycerides. This further highlights the strong association between MASLD and metabolic syndrome. As a metabolic disorder, MASLD is increasing globally, with a prevalence of 30% (Riazi et al., 2022).
Age-specific patterns of liver diseases have not yet been defined (Frith et al., 2009). However, liver function declines with age and is accompanied by a variety of anatomical features, such as reduced liver size due to decreased hepatic blood flow, or physiological changes, such as decreased free radical scavenging systems and increased inflammatory responses (Anantharaju et al., 2002; Singh et al., 2011). Consistent with these changes, alanine aminotransferase levels have been reported to decrease with age (Dong et al., 2012; Xu et al., 2011).
Diet, genetic polymorphisms, and the oral and gut microbiota play significant roles in the development and progression of MASLD. The Mediterranean and Japanese diets, which are rich in vegetables and low in meat, have been shown to be effective in preventing and treating MASLD (Gelli et al., 2017; Matsumoto et al., 2023). In recent years, genome-wide association studies have identified many single nucleotide polymorphisms (SNPs) in NAFLD susceptibility genes. In 2008, Romeo reported the patatin-like phospholipase domain-containing 3 (PNPLA3) gene (Romeo et al., 2008). In addition to PNPLA3, several MASLD-related SNPs have been identified (Dong et al., 2007; Kawaguchi et al., 2018; Li et al., 2021; Liu et al., 2016; Speliotes et al., 2011; Tong & Wang, 2020; Wang et al., 2016). The link between the gut microbiota and liver is known as the gut-liver-axis, and there are many reports on the relationship between gut microbiota and MASLD (Aron-Wisnewsky et al., 2020). Furthermore, the oral microbiota is involved in the development and progression of MASLD via inflammatory cytokines and the transfer to the gut microbiota (Chen et al., 2023b; Mei et al., 2024).
Due to the decline in physical function associated with aging, factors involved in the development and progression of MASLD are expected to differ between younger and older patients. Although there are many studies on the characteristics of NAFLD in older adults, none have investigated the nutritional intake, genetics, and oral and gut microbiota together. Additionally, with the renaming of NAFLD as MASLD in 2023, epidemiological studies on the factors involved in the development and progression of MASLD in older adults are an important issue in an aging society. We conducted a cross-sectional study to investigate how nutritional intake, genetic polymorphisms, and oral and gut microbiota affect MASLD in a general community population aged ≥60 years.
Materials and Methods
Study Participants
This study was conducted as part of the “Iwaki Health Promotion Project,” a community-based health promotion project targeting the general Japanese population. The project targets residents of the Iwaki area of Hirosaki City, Aomori Prefecture, and is conducted as a regular health checkup every June (Nakaji et al., 2021). A total of 1,056 adults (aged 19–88 years) who voluntarily responded to a public call participated in the study. The participants were excluded if they were aged ≤59 years, unable to consent to genetic testing, unable to accurately assess fatty liver due to transient elastography failure or had missing values on any of the measures. Additionally, participants who had undergone gastrectomy or were taking gastric suppressants were excluded because their gut microbiota was significantly altered by decreased gastric acid secretion. Participants taking antibiotics were also excluded because antibiotic use can significantly alter the composition of the gut microbiota. Based on previous reports, steatotic liver disease (SLD) was diagnosed with a cut-off value of 248 dB/m for the controlled attenuation parameter (CAP) value using FibroScan (Echosens, Paris, France) (Karlas et al., 2017). Approximately 124 participants were included in a normal group after excluding individuals with positive hepatitis B surface (HBs) antigen, positive anti- hepatitis C (HCV) antibody, or excessive alcohol consumption (>30 g/day for men and 20 g/day for women) from the non-SLD group. In the SLD group, 77 patients who met the diagnostic criteria were included in the MASLD group (Rinella et al., 2023). We analyzed 201 patients (124 in the normal group and 77 in the MASLD group) (Figure 1).

Study enrollment flowchart.
Transient Elastography
The CAP and liver stiffness measurements (LSM) were performed using a FibroScan 530 (Echosens, Paris, France) with M and XL probes. All the tests were performed by five professionally trained hepatologists. Measurements were excluded if the number of measurements was <10 or if the interquartile range ratio was >0.30, because they were unreliable. In a previous study, a CAP values ≥248 dB/m was defined as fatty liver (Karlas et al., 2017).
Clinical Parameters
Nutrient intake was calculated based on the results of the Brief Self-Administered Diet History Questionnaire (BDHQ), a simple dietary assessment questionnaire developed in Japan. The BDHQ is a four-page self-administered questionnaire that estimates the monthly dietary intake of 58 commonly consumed foods and beverages in Japan by asking about the frequency of intake of the selected foods (Sasaki et al., 1998). Participants were given the BDHQ in advance, and each participant was interviewed individually on the project day. Questionnaires were collected after the participants’ responses were verified. Nutrient intake per 1000 kcal was calculated using the BDHQ.
The following clinical parameters were measured on the same day of the project visit: sex, age, height, body mass index (BMI, calculated by dividing the weight in kilograms by the squared height in meters), waist circumference, HBsAg or anti-HCV test results, and levels of aspartate aminotransferase, alanine aminotransferase, gamma-glutamyl trans-peptidase, glucose, hemoglobin A1c (HbA1c), high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, and triglycerides.
The Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) was calculated using the following formula: fasting blood glucose (mg/dL) × fasting insulin (μU/mL)/405.
The fatty liver index (FLI) was calculated as follows:
MASLD Diagnosis
MASLD was diagnosed as fatty liver without drinking habits or other liver diseases, plus ≥1 of the following items: obesity, hyperglycemia, high blood pressure, high triglyceride, and reduced HDL cholesterol. The specific criteria included a BMI of ≥23 kg/m2 or waist circumference of ≥94 cm for males and ≥80 cm for females; fasting blood glucose ≥100 mg/dL, postprandial blood glucose ≥140 mg/dL, HbA1c ≥5.7%, or undergoing treatment for type 2 diabetes mellitus; blood pressure ≥130/85 mmHg or currently undergoing antihypertensive treatment; triglycerides ≥150 mg/dL or currently undergoing treatment for dyslipidemia; and HDL cholesterol ≤40 mg/dL for males and ≤50 mg/dL for females (Rinella et al., 2023).
DNA Preparation and SNP Genotyping
Single nucleotide polymorphisms genotypes were determined using whole-genome sequencing with imputation from the Japonica Array (Toshiba, Tokyo, Japan), which consists of population-specific SNP markers designed from the 1070 whole-genome reference panels and TaqMan polymerase chain reaction [PCR] (Kawai et al., 2015; Nagasaki et al., 2015). Whole-genome sequencing and imputation were performed by Takara Bio Corporation (Shiga, Japan) and Toshiba Corporation, respectively. By using the Japonica Array, DNA was purified from peripheral whole blood using a QIAamp®96 DNA Blook Kit (QIAGEN, Hilden, Germany) and extracted from the plasma pellets for whole-genome sequencing. To date, several NAFLD susceptibility genes have been identified. In this study, we analyzed 12 SNPs that have been frequently reported to be associated with NAFLD in previous studies (Dongiovanni & Valenti, 2016; Kawaguchi et al., 2018; Speliotes et al., 2011). The participants were genotyped for 12 SNPs associated with NAFLD: PNPLA3-rs 738409 (risk alleles G), PNPLA3-rs 2896019 (risk alleles G), LYPLAL1-rs12137855 (risk alleles C), GCKR-rs1260326 (risk alleles C), AGTR1-rs3772622 (risk alleles C), PPP1R3B-rs4240624 (risk alleles A), GATAD2A-rs4808199 (risk alleles A), MTP-rs1800591 (risk alleles T), PEMP-rs7496 (risk alleles T), MnSO-rs4880 (risk alleles G), TM6SSF2-rs58542926 (risk alleles T), and DYSF-rs17007417 (risk alleles T).
Measurements of Microbiota
The oral and gut microbiota data were measured using the following procedure: the participants were provided with saliva and fecal sample kits (TechnoSuruga Laboratory Co., Ltd., Shizuoka, Japan) in advance, and saliva and stool samples were collected at home and submitted on the day of the project visit. We extracted DNA from the bead-beaten fecal suspensions using an automated nucleic acid extraction system (Precision System Science). The MagDEA DNA 200 (GC) reagent kit (Precision System Science) was used for automated nucleic acid extraction. Universal primer sets were used to amplify the V3-V4 regions of the 16S rRNA gene. Solution preparation and condition setting for PCR amplification were performed as described previously (Takahashi et al., 2014). Polymerase chain reaction fragments purified using PCR Cleanup Filter Plates (Merck Millipore, Burlington, MA, USA) were quantified by real-time quantitative PCR (qPCR). To read DNA sequences, purified PCR fragments were analyzed by paired-end sequencing of 2 × 300 cycles on a MiSeq™ system (Illumina, San Diego, CA, USA). Paired-end reads were processed as follows: adapter sequences and low-quality bases (Q <20) at the 3′ end of the reads were trimmed using Cutadapt (version: 1.13). Reads containing ambiguous bases N or shorter than 150 base pairs were excluded from the analysis. The paired-end reads that met the criteria were merged into a single read called a “merged read.” Merged reads shorter than 370 bp or longer than 470 bp were excluded using the fastq_mergepairs sub-command in VSEARCH (version 2.4.3) (Rognes et al., 2016). Merged reads containing ≥1 sequencing errors were excluded. After removing the chimeric reads detected using the uchime_denovo subcommand of VSEARCH, the remaining merged reads were clustered with a minimum sequence similarity of 97% to obtain operational taxonomic units (OTUs). Phylogenetic classification of the OTUs was performed using the RDP classifier (commit hash: 701e229dde7cbe53d4261301e23459d91615999d) based on representative reads (Wang et al., 2007). Predictions with a confidence score <0.8 were treated as unclassified. The relative abundance of each bacterial species in the oral and gut microbiota was calculated by dividing the read count of each genus by the total read count. Of the bacterial species measured, 500 types of oral bacteria and 545 types of gut bacteria were extracted.
Statistical Analysis
Categorical variables are presented as frequencies and continuous variables as medians and interquartile ranges. The Chi-square and Mann–Whitney U tests were used to compare the two groups. The microbiota was compared using the linear discriminant analysis effect size (LEfse) (Segata et al., 2011). A multiple regression model with MASLD-related items and oral and gut microbiota was used for the predictive analysis. Independent variables included sex, age, smoking habits, and exercise habits. Before multiple regression analyses, all continuous parameters were log-transformed (natural logarithm) to approximate a normal distribution. Statistical analyses were performed using R software (R Foundation for Statistical Computing, version R-4.1.1) and Statistical Package for the Social Sciences version 28.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set at P < 0.05.
Study Approval
This study was conducted according to the ethical standards of the Declaration of Helsinki and approved by the Ethics Committee of Hirosaki University School of Medicine (approval number and date: 2018-012, approved on May 11, 2018). Informed consent was obtained from all the participants.
Results
Participant Characteristics
Table 1 shows the characteristics of the participants. The median age was 67.0 years in the control group and 68.0 years in the MASLD group, with no significant difference between the two groups. Compared to the normal group, the MASLD group showed higher values for BMI, waist circumference, fasting blood sugar, HbA1c, HOMA-IR, systolic blood pressure, diastolic blood pressure, triglycerides, CAP value, LSM value, FLI, alanine aminotransferase, and γ-glutamyl transpeptidase, while HDL cholesterol was lower. There were no significant differences between the two groups in terms of sex, exercise habits, or smoking status.
The characteristics of the participants.
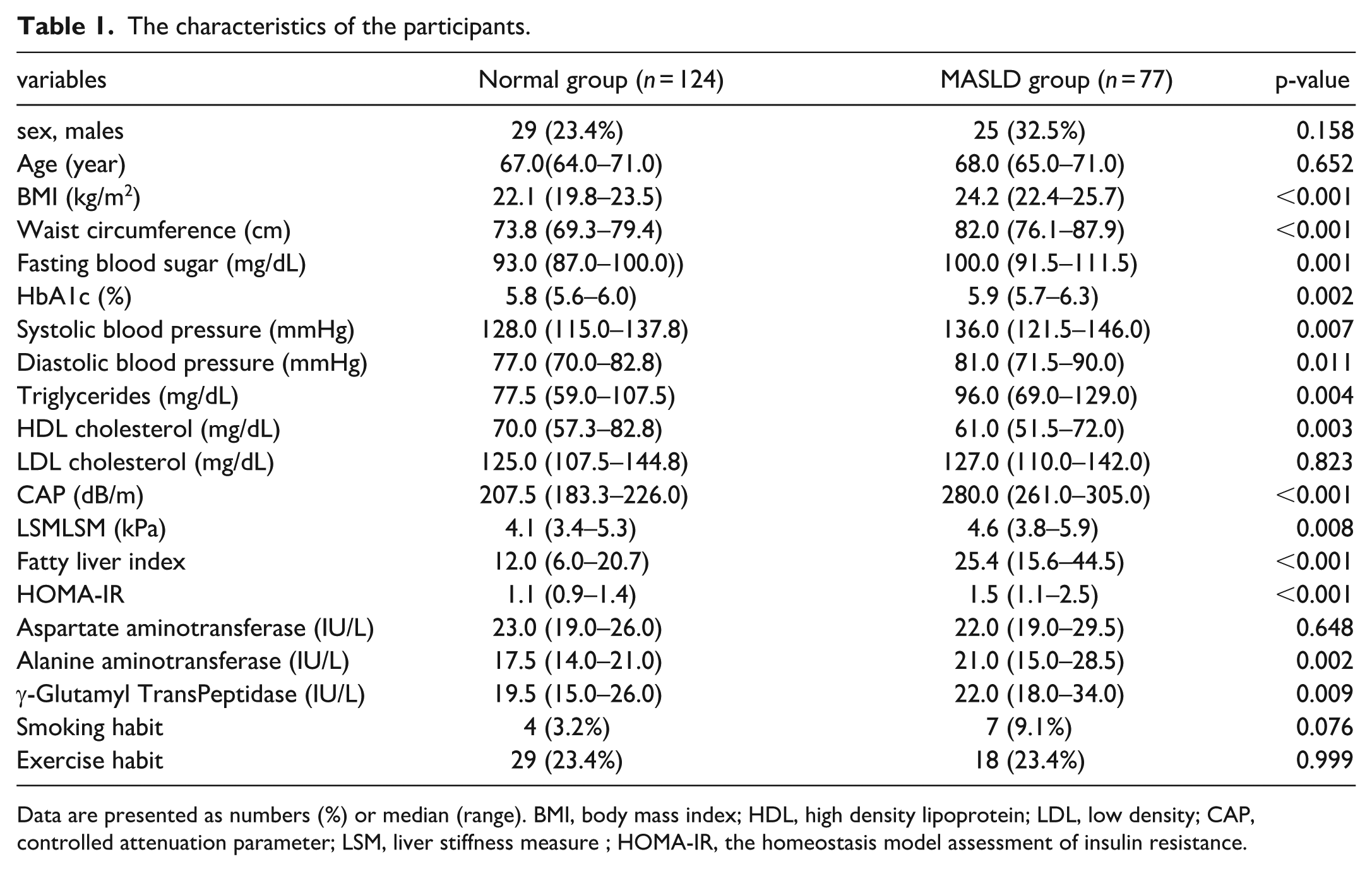
Data are presented as numbers (%) or median (range). BMI, body mass index; HDL, high density lipoprotein; LDL, low density; CAP, controlled attenuation parameter; LSM, liver stiffness measure ; HOMA-IR, the homeostasis model assessment of insulin resistance.
Nutrient intakes of the participants are shown in Table 2. Total energy intake and each nutrient intake per 1000 kcal did not differ between the two groups.
Nutrient intakes of the subjects in the normal and MASLD groups.
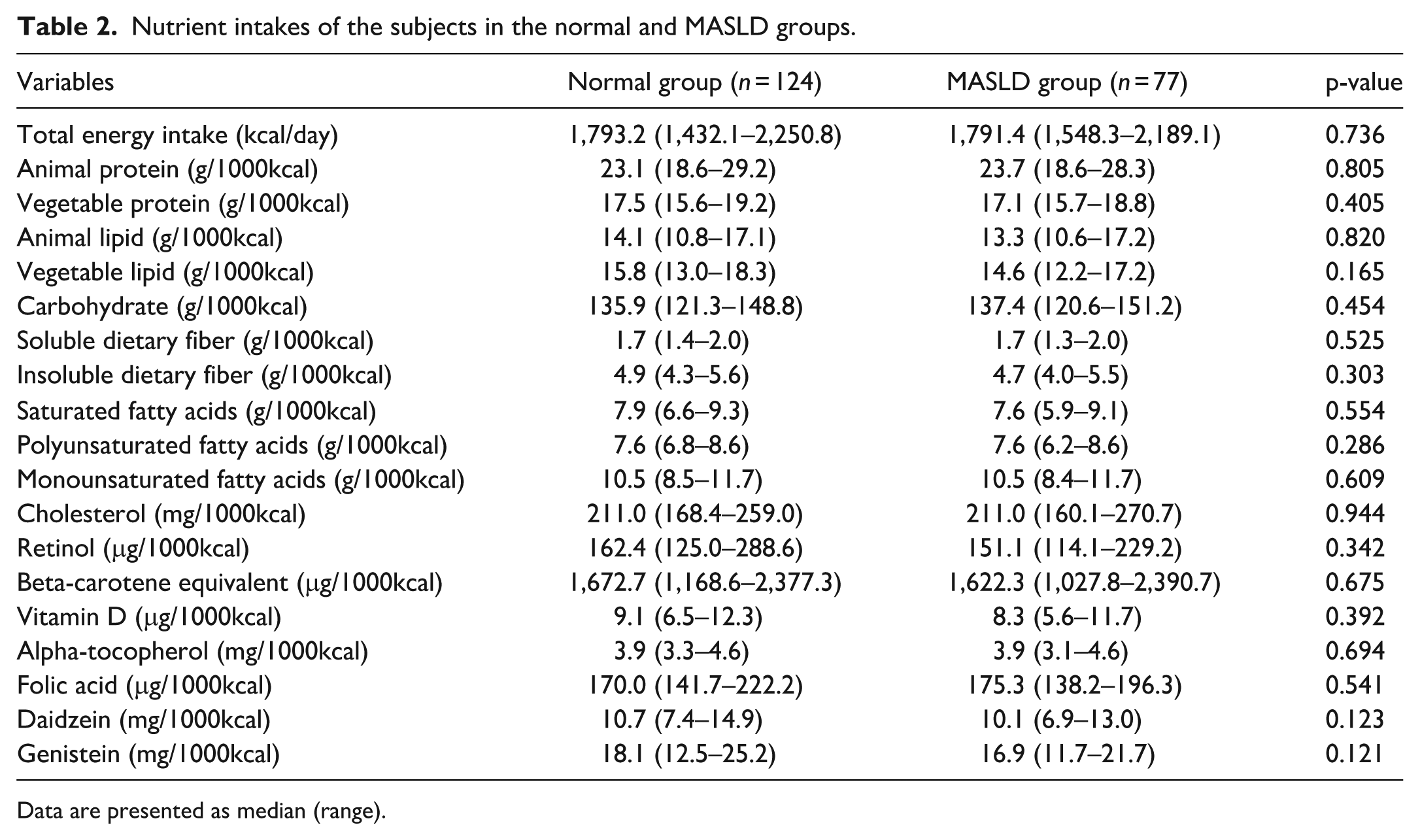
Data are presented as median (range).
Retention frequencies of MASLD-related SNPs in the normal and MASLD groups are shown in Table 3. No significant differences were observed between the two groups for any of the 12 SNPs measured.
The retention frequencies of MASLD-related SNPs in the normal and MASLD groups.
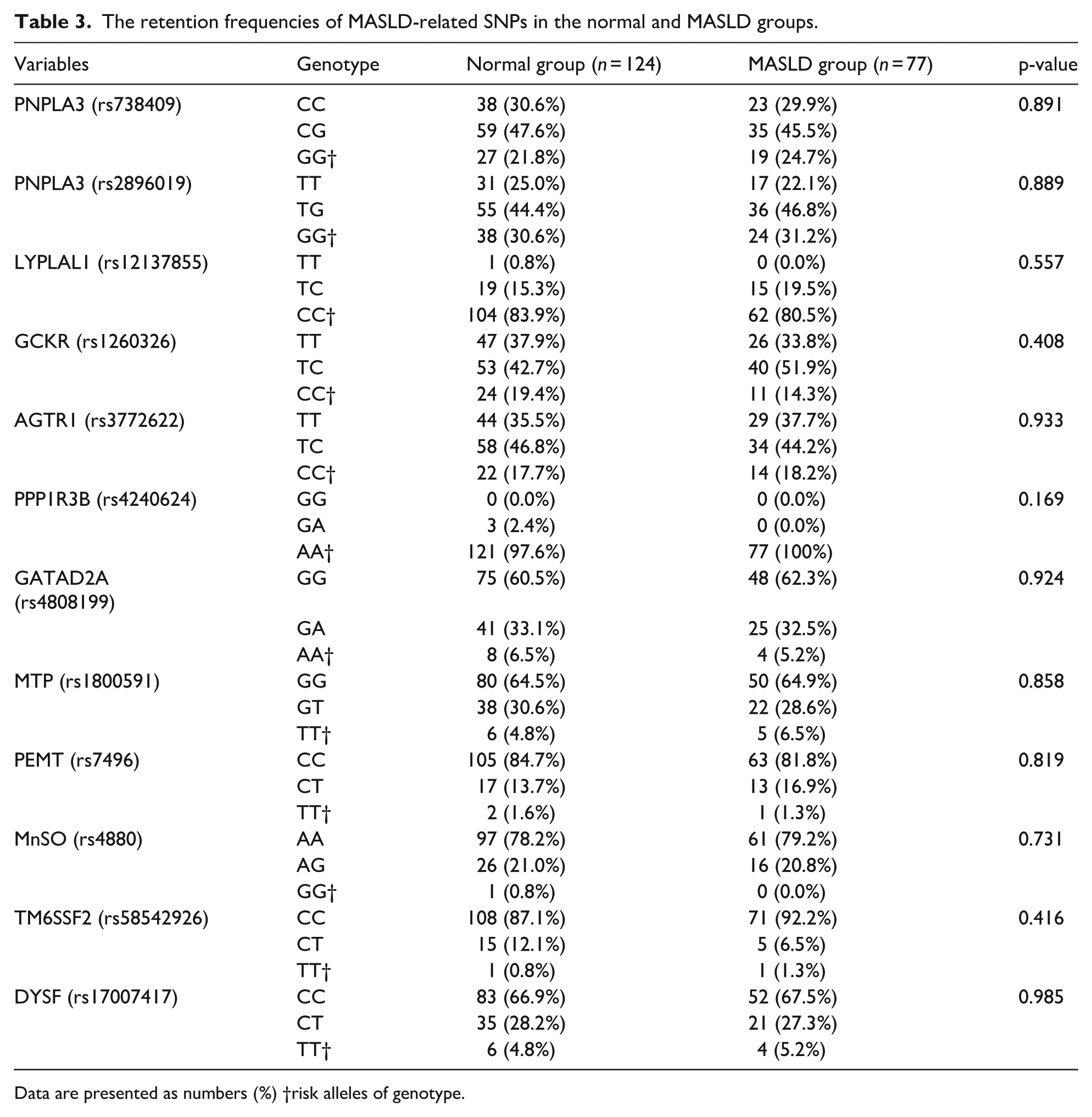
Data are presented as numbers (%) †risk alleles of genotype.
Figure 2 shows the differences in the diversity of the oral and gut microbiota. The Chao-1 and Shannon indices, indices of alpha diversity, showed no difference between the two groups in both the oral and gut microbiota. No difference in principal coordinate analyses, an index of β-diversity, in the oral microbiota, but significant differences were observed between the two groups in the gut microbiota.
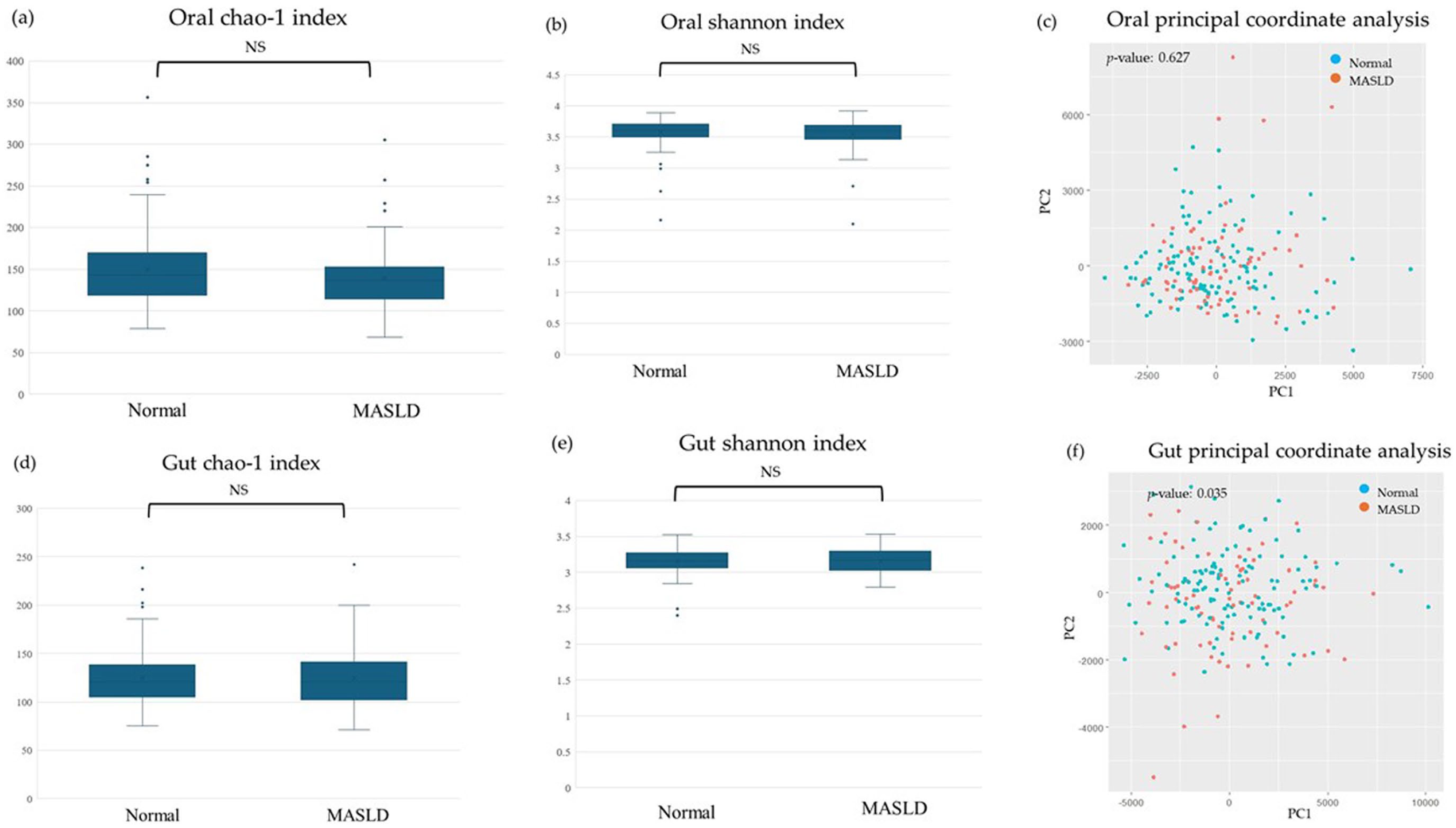
Comparison of the diversity of microbiota between normal and MASLD groups: (a) Oral chao-1 index, (b) Oral shannon index, (c) Oral principal coordinate analysis, (d)Gut chao-1 index, (e) Gut shannon index, (f) Gut principal coordinate analysis.
Comparison of MASLD and Bacterial Species Relationships
Figure 3 shows the differences in oral and gut bacterial species between the normal and MASLD groups using LEfSe. In the oral cavity, the MASLD group showed an increase in seven bacterial species and a decrease in nine. In the gut, the MASLD group showed an increase in six species and decrease in 10.
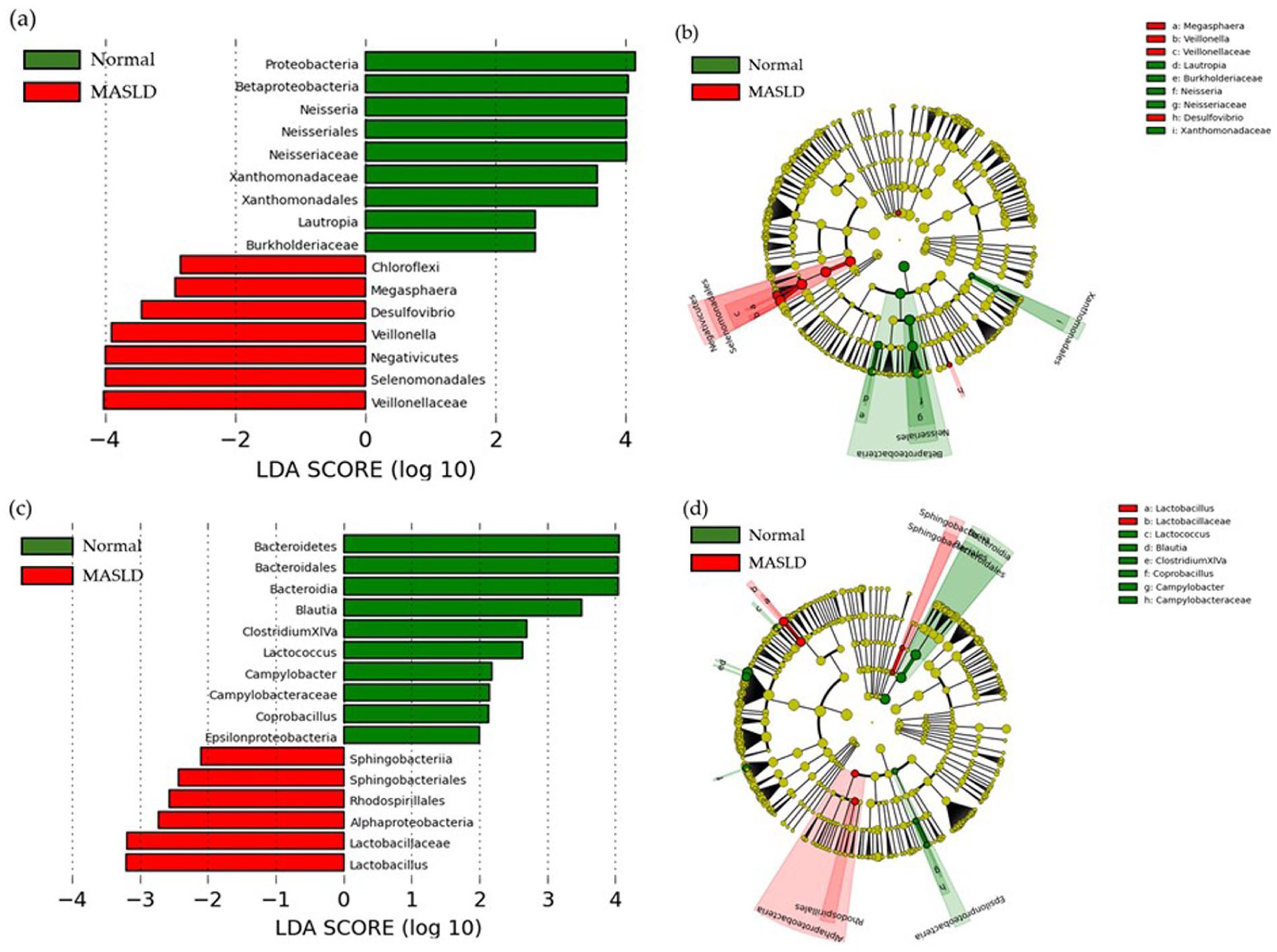
The LEfSe results of the microbiota between normal and MASLD groups: (a) The linear discriminant for oral microbiota, (b) The cladogram report for oral microbiota, (c) The linear discriminant for gut microbiota, (d) The cladogram report for gut microbiota.
Relationship between MASLD-Related Items and Oral and Gut Microbiota
Table 4 and 5 summarize the multiple regression analysis was performed, where the dependent variables were MASLD-related items and independent variables were sex, age, smoking, and exercise habits in addition to the oral and gut microbiota at genus level, which were found to be associated with LEfSe. In the oral cavity, CAP levels positively correlated with Veillonella and Desulfovibrio, and negatively correlated with Lautropia. Veillonella and Megasphaera were positively correlated with BMI, waist circumference, systolic blood pressure, and the FLI (Table 4). In the gut, Blautia negatively correlated with CAP levels, BMI, waist circumference, fasting blood sugar, HbA1c, HOMA-IR, triglycerides, and FLI (Table 5). Additionally, Campylobacter negatively correlated with BMI and waist circumference, Clostridium XlVa negatively correlated with waist circumference, and Lactobacillus positively correlated with HbA1c. However, the relative abundance of gut bacterial species other than Blautia was extremely low (<0.3%).
Multiple Regression Analysis of Relationship Between MASLD-related Items and Oral Microbiota.
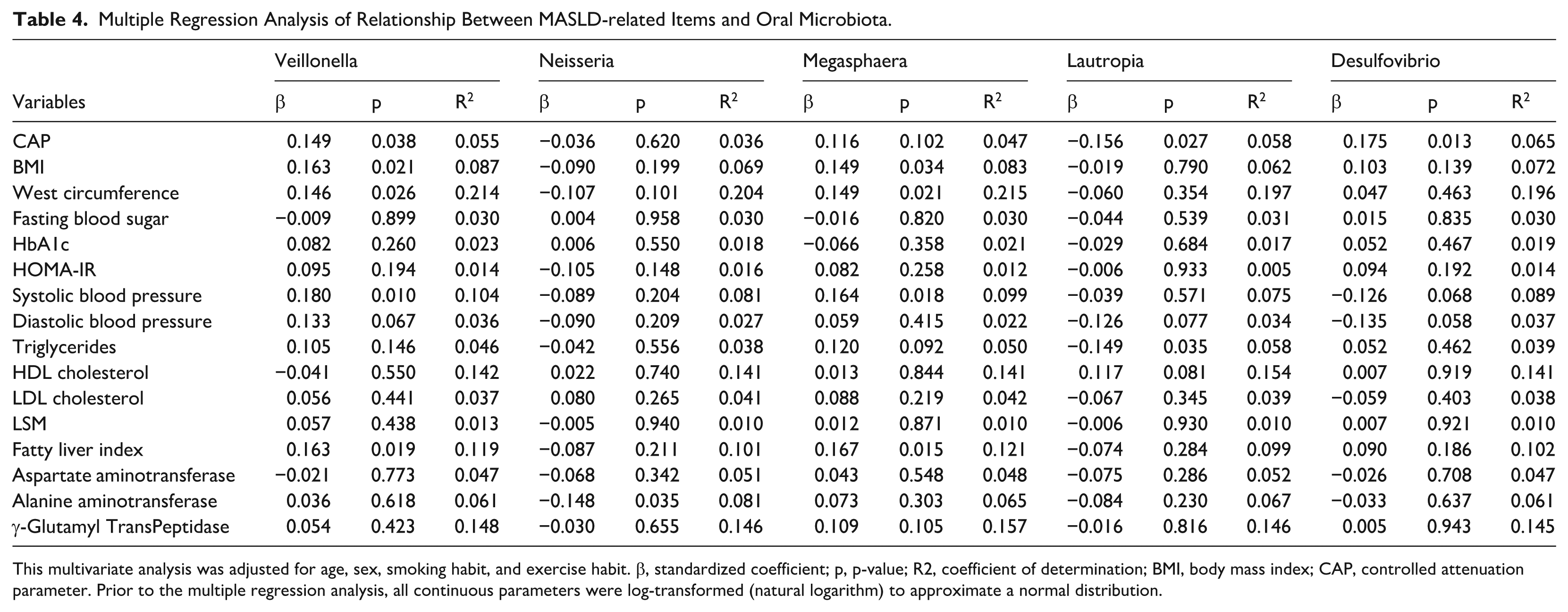
This multivariate analysis was adjusted for age, sex, smoking habit, and exercise habit. β, standardized coefficient; p, p-value; R2, coefficient of determination; BMI, body mass index; CAP, controlled attenuation parameter. Prior to the multiple regression analysis, all continuous parameters were log-transformed (natural logarithm) to approximate a normal distribution.
Multiple regression analysis pf relationship between MASLD-related items and gut microbiota.
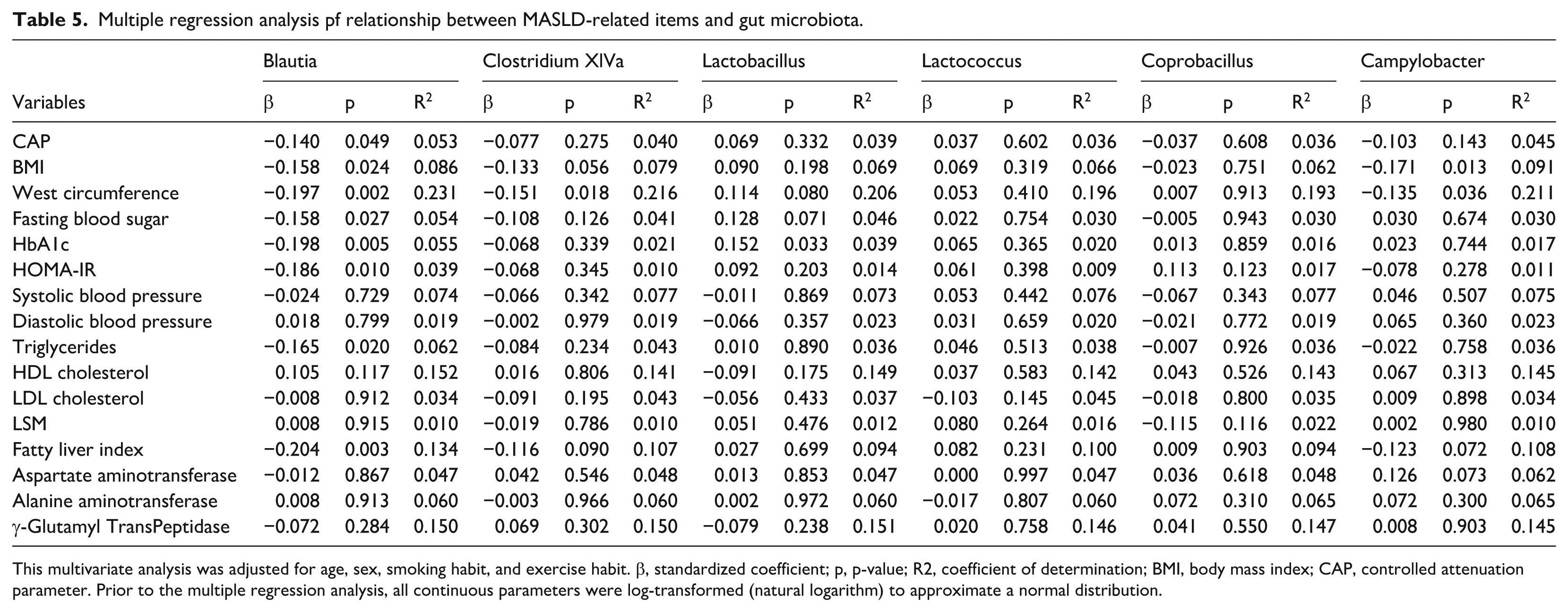
This multivariate analysis was adjusted for age, sex, smoking habit, and exercise habit. β, standardized coefficient; p, p-value; R2, coefficient of determination; BMI, body mass index; CAP, controlled attenuation parameter. Prior to the multiple regression analysis, all continuous parameters were log-transformed (natural logarithm) to approximate a normal distribution.
Discussion
In this study, we found that the oral and gut microbiota of patients with MASLD aged ≥60 years differed from those of healthy older patients and were associated with obesity, blood pressure, blood glucose, and lipid levels, as well as liver fat content. However, no differences were observed in nutrient intake or genetic polymorphisms.
In this study, the MASLD group had increased oral Veillonella and Magasphaera compared to the normal group. Additionally, multivariate analysis, adjusted for con-founding factors, showed that Veillonella and Megasphaera were positively associated with BMI, waist circumference, and systolic blood pressure. Veillonella is a strictly anaerobic, gramnegative coccus frequently isolated from the human oral cavity. It plays a significant role in the formation of oral biofilms and contributes to dental caries and periodontal disease (Zhou et al., 2021). Veillonella accounted for a high proportion of 9.0% of the oral microbiota in this study participants. Veillonella is also present in the gut, and gut Veillonella is increased in patients with cirrhosis (Oh et al., 2020). Additionally, a high relative abundance of gut Veillonella has been reported to increase the risk of NAFLD (Zhai et al., 2023). In this study, multivariate analysis adjusted for confounding factors showed that oral Veillonella was positively correlated with BMI, waist circumference, systolic blood pressure, FLI, and CAP. Previous studies indicated that oral Veillonella migrates to the gut, induces inflammation, and contributes to the exacerbation of obesity and hypertension (Aranaz et al., 2021; Chen et al., 2023a).
Megasphaera belongs to the family Veillonellaceae, the same family as Veillonella, and primarily inhabits the oral cavity (Marchandin et al., 2010). The function of the Megasphaera is still unknown, but there are reports that gut Megasphaera is enriched in NAFLD cirrhosis (Hoozemans et al., 2021). Additionally, our study found that Megasphaera, like Veillonella, was positively correlated with BMI, waist circumference, and systolic blood pressure in a multivariate analysis. Megasphaera belongs to the Veillonellaceae family as Veillonella, and may exert effects similar to Veillonella.
Previous studies have examined the relationship between Veillonella, Megasphaera, and liver diseases in the gut, but not in the oral cavity. The findings of our study indicate that oral Veillonella and Megasphaera could play a role in the pathogenesis and progression of MASLD, with obesity and hypertension as potential underlying mechanisms.
In contrast, no association was found between the gut Veillonella and Megasphaera in our study. This may be because most patients with MASLD in this study had mildly active disease, whereas previous studies included patients with advanced liver disease, such as those with cirrhosis. Additionally, the relative abundance of Veillonella and Megasphaera in our study participants were 9.04% and 0.31% in the oral cavity, respectively, whereas gut relative abundances were extremely low at 0.047% and 0.002%, respectively. Because this study included the general population without advanced cirrhosis, the relationship between gut Veillonella and Megasphaera, which are generally detected at a very low relative abundance, may not have been statistically significant.
In this study, we found that the MASLD group had decreased gut Blautia compared to the normal group.Furthermore, Blautia was negatively correlated with CAP levels, BMI, waist circumference, fasting blood sugar, HbA1c, HOMA-IR, triglycerides, and FLI. In animal studies, the oral administration of Blautia increased intestinal short-chain fatty acids and suppressed fatty obesity (Shibata et al., 2023). Epidemiological studies have reported increased gut Blautia in individuals with a smaller visceral fat area (Ozato et al., 2019). Additionally, it has been widely reported that gut Blautia are decreased in patients with MASLD, and the underlying mechanism is thought to be a reduction in the suppressive effect of increased gut acetic acid concentration by Blautia on hepatic steatosis and fibrosis (Hrncir et al., 2021). Our findings indicate that the protective effect of gut Blautia against MASLD, which has been previously observed in other populations, extends to the older population.
In this study, genetic polymorphisms did not differ between the normal and MASLD groups. Among the many MASLD-related SNPs, PNPLA3-rs738409 (C>G) has been reported to be involved in the onset and progression of conventional MASLD in many ethnic groups, including Japanese (Kawaguchi et al., 2012; Kotronen et al., 2009). However, PNPLA3-rs2896019 (T>G) has also been reported to be involved in fatty liver (Kitamoto et al., 2013). The risk allele carriers of PNPLA3 in patients with MASLD in this study was 24.7% for rs738409 GG genotype and 22.1% for rs2896019 GG genotype, which were lower than 38.3% and 41.3% reported in previous studies (Hotta et al., 2010; Kitamoto et al., 2013). This discrepancy may be due to several factors, including differences in the diagnostic criteria for patients with MASLD. Unlike previous studies that used liver biopsy to diagnose fatty liver, we used FibroScan. These differences may be responsible for the inconsistent results obtained. Additionally, older adults exhibit a decline in the anatomical and physiological functions of the liver due to aging (Anantharaju et al., 2002; Bertolotti et al., 2014; Singh et al., 2011). This study also found that the oral and gut microbiota were associated with MASLD, but the oral and gut microbiota were greatly affected by aging, with the diversity and proportion of species in older adults differed greatly from those in young to middle-aged individuals (Ghosh et al., 2022; Kazarina et al., 2023). It is possible that the effect of SNPs was relatively small owing to the physical characteristics unique to older adults, and no differences were observed.
Our study found no differences in nutritional intake between the normal and MASLD groups. We also found no significant differences in exercise habits between the two groups. Despite the lack of differences in nutritional intake and exercise habits, the older adults with MASLD had a higher BMI, blood pressure, lipid levels, and blood glucose levels than the healthy older adults. These results suggest that dietary and exercise habits play a minor role in the development and progression of MASLD in the older adults, and that lifestyle modification alone may not be sufficient to treat the disease.
This study has several limitations. First, the study population was geographically limited to one region in Japan. Therefore, the results of this study cannot be generalized to all ethnic groups. Second, the number of remaining teeth and oral hygiene status, such as the presence of periodontal disease, were not assessed. The number of remaining teeth in older adults is reduced due to periodontitis, and a large proportion of them wear artificial teeth, such as dentures or implants, which may be related to the oral microflora. Third, fatty liver and liver fibrosis were diagnosed using FibroScan instead of a liver biopsy. Invasive liver biopsy, which is performed as part of a physical examination of the general population, was not feasible in this study.
Conclusions
Through this study of the older general population, we found that oral Veillonella and Megasphaera, which belong to the family Veillonellaceae, exacerbated the onset and progression of MASLD in older individuals, whereas gut Blautia had an inhibitory effect. However, no association was observed between nutritional intake and genetic polymorphisms. In older adults, improving oral hygiene and probiotics may prevent the onset and progression of MASLD by improving the oral and intestinal environments.
Footnotes
Acknowledgements
This study was based on the Iwaki Health Promotion Project of the Hirosaki University Graduate School of Medicine in collaboration with the Aomori Health Evaluation and Promotion Center and Hirosaki City Office of the Department of Health Promotion. This study was supported by TechnoSuruga Laboratory Co., Ltd. (Shizuoka, Japan).
Ethical Considerations
This study was conducted according to the ethical standards of the Declaration of Helsinki and approved by the Ethics Committee of Hirosaki University School of Medicine (approval number and date: 2018-012, approved on May 11, 2018).
Consent to Participate
Informed consent was obtained from all the participants.
Consent for Publication
Not applicable.
Author Contributions
SS, CI, TM, and SN conceptualized and designed the study. SS, CI, KY, TS, and KF performed FibroScan measurements. SS and CI performed the data analysis. SS, HS, and SF conceptualized the manuscript. All the authors have approved the manuscript for publication. All the authors have read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JSPS KAKENHI (grant number 22K17386), JST, and COI Grant Numbers JPMJCE1302, JPMJCA2201, and JPMJPF2210.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data presented in this study are available upon request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.