
Abstract
Background
The single-incision connective tissue grafting (SICTG) represents an advancement in periodontal plastic surgery, designed to achieve primary wound closure, reduce donor-site morbidity, and promote improved early healing compared with traditional trapdoor and double-incision techniques.
Objective
To describe the biological rationale of the SICTG technique and propose a biologically driven modification based on accumulated clinical experience aimed at improving surgical handling and tissue preservation.
Technique Description
The proposed modification builds upon established SICTG principles while incorporating refinements and technical innovations intended to enhance graft harvesting, facilitate tissue preservation, and maintain favorable wound stability. The approach is derived from clinical observations and biological considerations related to wound healing and vascular supply.
Conclusion
The modified-SICTG may offer practical advantages in surgical handling and donor-site management. However, it should be regarded as a technical proposal rather than a validated clinical protocol. Further systematic clinical trials are required to evaluate its effectiveness, safety, and long-term stability through controlled clinical outcome studies.
Keywords
Introduction
Connective tissue grafting remains the cornerstone of periodontal plastic surgery for root coverage, biotype modification, and gingival augmentation. The subepithelial connective tissue graft (SCTG), introduced by Langer and Langer 1 in 1985, demonstrated highly predictable outcomes. SCTG represents a major biologic and clinical shift that utilizes the separation of the epithelium from the underlying connective tissue graft (CTG), allowing better color, contour integration, predictable root coverage, and more versatile soft-tissue augmentation. However, traditional harvesting techniques such as the trapdoor and double-incision approaches were associated with donor-site complications, leaving larger wound areas, increased patient morbidity, pain, bleeding, and delayed healing.2, 3 These limitations created the need for a harvesting approach that would preserve palatal anatomy and vascularity while providing adequate CTG volume. Thus, the need for a technique that maintains graft integrity while reducing trauma led to the development of the single-incision concept.4, 5
Since its inception, subsequent clinical trials and technical refinements have consistently confirmed that single-incision connective tissue grafting (SICTG) and its modification variants optimize donor-site outcomes without compromising regenerative or root-coverage efficacy and are therefore regarded as the current most efficient standard protocol for palatal CTG procurement.6, 7 However, these methods are highly technique-sensitive, and minor deviations in design, depth of incision and dissection, or tissue handling can compromise graft integrity and postoperative outcomes. Clinicians often face challenges with maintaining control of dissection planes and achieving consistent graft dimensions, frequently resulting in grafts that are smaller or thinner than intended. Further, surgical variations in reported techniques and technical modifications, which despite the ongoing evolution of the approach, highlight the need for further standardization toward a biologically optimized and conceptually consistent harvesting protocol across operators. Variations in tissue thickness, blade angulation, and plane of dissection further contribute to unpredictable graft dimensions and donor morbidity. 7 Thus, the present paper intends to present the evolutionary development of SICTG and its successive refinements, highlighting their biological and surgical rationale, besides describing a technical proposal derived from accumulated clinical experience and providing a conceptual structural framework for its future clinical validation.
Evolution of Single-incision Connective Tissue Grafting Techniques
The evolution of CTG procurement has witnessed a paradigm shift from conventional multi-incision designs to biologically advanced single-incision techniques, which epitomize precision, predictability, and patient comfort. Since its inception, SICTG has undergone numerous modifications and refinements. In 1999, Hürzeler and Weng 2 first described a single horizontal incision to obtain the graft from the palatal donor site between the canine and first molar. The incision was initiated at 90° to the palatal bone to outline the graft, followed by blade angulation between 135° and 180° to undermine and elevate the connective tissue. The graft was then separated by precise incisions to the bone and removed through the same access incision using a partial-thickness flap, allowing primary closure and rapid healing. This approach demonstrated that complete grafts can be harvested without vertical releasing incision using a partial-thickness flap, thereby reducing postoperative morbidity. However, limited intraoperative visibility remained a challenge, prompting subsequent modifications. These limitations were overcome by refinements introduced by Lorenzana and Allen 3 in 2000, which improved the standardization of incision depth, ensured meticulous flap management, emphasized esthetics, and reduced morbidity. These two landmark publications established the biological and clinical foundation for SICTG, grounded in the principles of minimal tissue trauma and optimal vascularization. 3 Dembowska and Drozdzik 4 also used the SICTG technique for the procurement of CTG while including the palatal periosteum. Han et al. 5 reported that SICTG achieved successful root-coverage and increased keratinized tissue with greater gain, when the CTG was left partially uncovered rather than fully covered by the flap. Del Pizzo et al. 6 showed that SICTG provided faster epithelial healing and greater patient comfort than trapdoor and double-incision techniques due to smaller wounds and primary closure.
Ribeiro et al. 8 reported that SICTG was associated with normal intraoperative bleeding and absence of postoperative necrosis, hemorrhage, pain, or discomfort. Park 9 reported that SICTG enables the harvesting of large CTGs and predictable primary palatal closure, while subsequent studies10–12 have shown that repeated graft harvesting from the same donor can support predictable root coverage and staged management of multiple recessions without increased morbidity. Kumar et al. 11 described an altered SICTG using controlled partial-thickness incisions and a specialized blade (AVS) to harvest CTG of adequate thickness while minimizing flap tearing and donor-site trauma. Reino et al. 12 also provide an alteration of the SICTG technique, using a small elevator to carefully elevate 1–2 mm of full-thickness flap, which facilitates further flap dissection with a blade, and allows more accurate control over graft thickness. Fickl et al. 13 proposed variation in SICTG by adding a second horizontal incision to create an internal connective tissue shelf that supports the flap, improves wound adaptation, and preserves palatal vascularity for uneventful healing. Kim et al. 14 reported that SICTG yields grafts rich in deep lamina propria and preserves palatal blood supply by avoiding vertical incisions, thereby enhancing clot stability and early wound healing.
Procedural Proposal for a Modified-Single-incision Connective Tissue Grafting
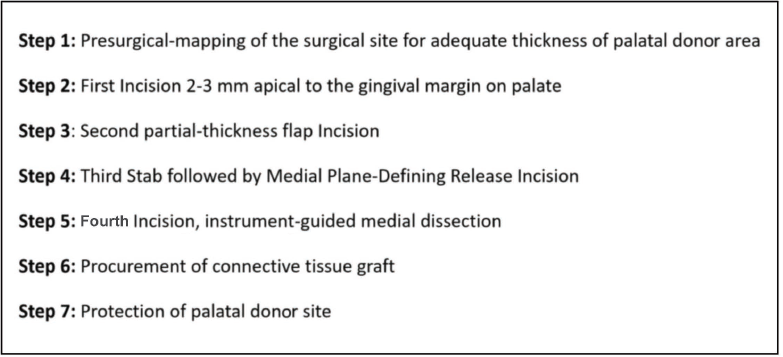
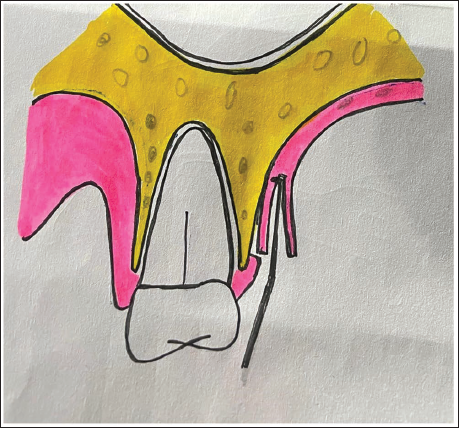
This proposed modified-SICTG technique involves mapping of the palatal tissue, depth-controlled first incision, second partial-thickness flap incision, medial plane-defining releasing incision, and instrument-guided medial dissection, which are essential for CTG procurement. These are explained in the following steps (Figure 1):
Schematic Diagram Showing Steps of Modified Single Incision Connective Tissue Grafting Technique.
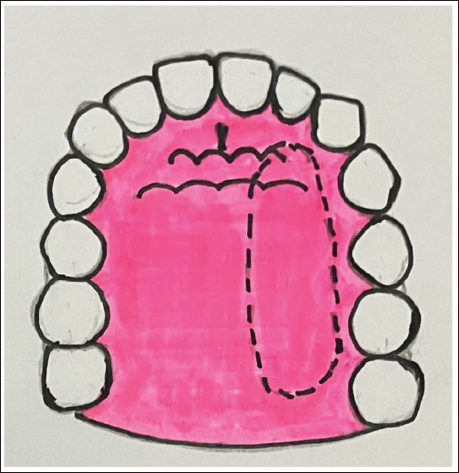
Step 1 (Mapping): Preoperative mapping using a minimally invasive #15 K-file to measure the thickness of the palate that enables the clinician to essentially identify bands of optimal thickness (2–3 mm) at various levels from the gingival margin on the palate, within a pragmatically considered safe zone between the canine and first molar. Do not pierce the portion of the area that is to be harvested as CTG. The proximal and medial extent of the graft must be determined before the start of the incision. Extend 1 mm in all three directions (required graft length +2 mm in proximal directions, graft width +1 mm medially). Mark the medial and proximal extents of the graft on the palate using an indelible pencil or surgical skin marker pen. Optionally, preoperative ultrasonic non-invasive mucosal thickness measurement planning results in planned and thickness-driven CTG procurement (Figure 2).
Pre-incisional Mapping of Palatal Mucosa for Connective Tissue Grafting (CTG) Procurement.
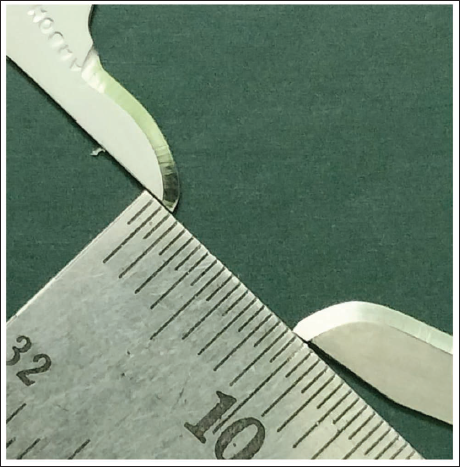
Step 2 (First Incision): Give the first incision 2–3 mm apical to the gingival margin in a horizontal direction using a #15C blade, while holding the blade perpendicular to the palate. The depth of the incision must be determined pre-surgically. A simple guide to measure the depth of the first incision is the bevel of the surgical blade, which is generally located around 0.5–0.7 mm from its edge (Figures 3–5).
Measuring the Dimension of the Bevel of Surgical Blade #15c and # 15.
First Incision to be Marked 2–3 mm Apical to Gingival Margin on Palatal Area from Canine to First Molar Area.
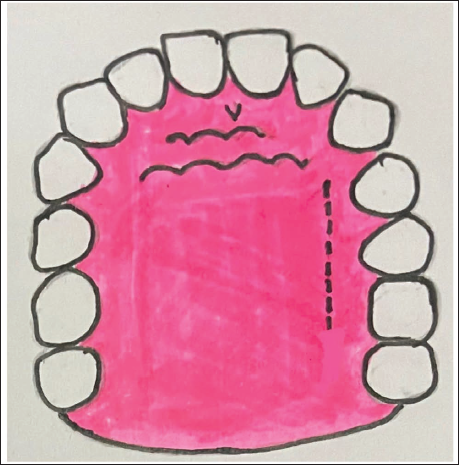
Controlled Depth of First Incision Upto Bevel of the Surgical Blade (0.5–0.7 mm).
Step 3 (Second Partial-thickness Flap Incision): From the deepest end of the first incision (i.e., barring 0.5–0.7 mm from the superficial/outer epithelial layer, with a small amount of layer of connective tissue), now turn the blade, so that it becomes almost parallel to the palate, and extend the incision medially while maintaining the thickness and avoiding any perforation (Figure 6). Always keep the blade slightly bent toward the CTG, not toward the epithelium, to prevent any chance of perforation. The best guide to maintain the medial extension of a partial-thickness flap can be determined using the length of the #15C blade as a guide, which is generally 8 mm. Most proximal ends (mesial and distal ends of grafts) of the grafts are then incised using #15C or micro- or cataract blade. 11
Second Incision (Superficial Dissection) Extend Medially.
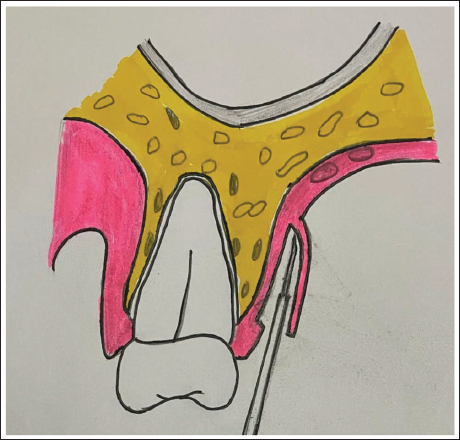
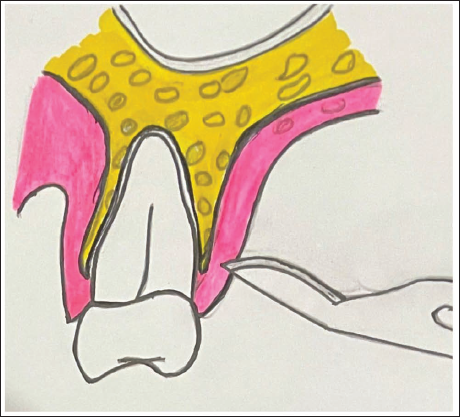
Step 4 (Third Stab Followed by Medial Plane-defining Release Incision): After proper elevation of a partial thickness flap, the first incision is subsequently deepened along the same line up to the palatal bone to create a localized full thickness access point (Figure 7). From the innermost aspect of the incision, raise a 2–3 mm mucoperiosteal full-thickness flap with periosteum from the extended horizontal incision line (Figure 8). This initial elevation of a limited 2–3 mm mucoperiosteal full-thickness flap is an intentional and essential step in the modified-SICTG and not intended to harvest the CTG but to establish a clearly visualized and controlled anatomical reference plane. By reflecting this small mucoperiosteal window, the clinician gains the ability to deliberately choose the subsequent dissection plane rather than relying on blind or arbitrary tissue separation. Following this controlled exposure, the CTG is separated medially along a plane parallel to the second partial-thickness incision. At this stage, the clinician may elect to proceed either superficial to the periosteum (to obtain a CTG with the periosteum preserved on the donor bed) or through the periosteum (to harvest a mucoperiosteal graft), depending on clinical requirements on the recipient sites. The use of either a blade or a periosteal elevator reflects this operator-controlled plane selection.
Third Stab Incision Till the Depth of Bone from Same First Incision.
Separation of Connective Tissue Grafting (CTG) Using Periosteal Elevator.
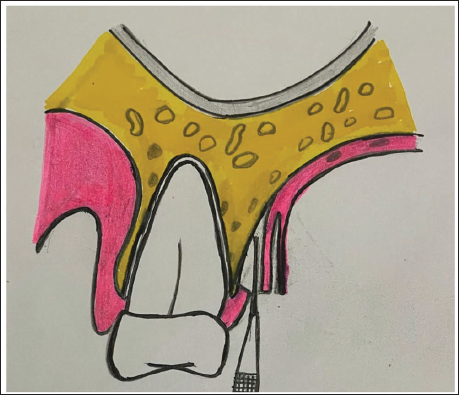
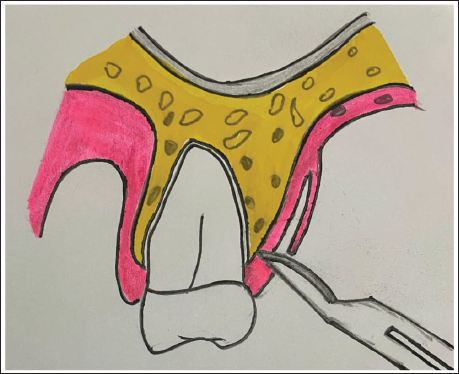
Step 5 (Fourth Incision, Instrument-guided Medial Dissection): Now insert the #17 end point of a #17/23 explorer to sever the medial-most part of the graft (Figure 9). The #17 tip is inserted from the undersurface partial thickness. It advances in a medial direction, keeping the terminal end in a plane parallel to the CTG rather than directing the sharp point toward the soft tissue. Once the instrument’s end reaches the medial-most extent of the graft, it is rotated approximately 90° to sever the CTG cleanly at its medial attachment by creating multiple perforation points at the medial end of the graft using the explorer. These small perforations can then be joined from one proximal end to another, allowing controlled and conservative release of the graft. Alternatively, clinicians may use the sharp end of the Howarth periosteal elevator or AVS blade 11 under a partial-thickness flap, and incise the graft medially from the palatal bone while pulling it laterally for harvesting CTG.
Fourth Incision, Instrument-guided Medial Dissection Using #17 End of Explorer.
Step 6 (Procurement): Once the CTG is severed from all directions, it can be harvested from the donor site using tissue forceps. It must be kept in a moist environment, either on a normal saline-dipped wet gauze piece or partially immersed in a saline solution. All efforts must be made to use CTG within 60 s of its procurement.
Step 7 (Protection): Following CTG procurement, the donor site is closed by primary suturing. Placement of platelet-rich fibrin (PRF) or a collagen dressing may be used as an optional protective adjunct to support clot stabilization and soft-tissue healing. Similarly, photobiomodulation (PBM) of the donor site may be applied as an optional postoperative adjunct to enhance patient comfort and tissue response, depending on availability and clinical preference.
Discussion
The accumulated experience with CTG procurement from the palate using single-incision techniques has addressed many early challenges, 7 but has also exposed their limitations, especially when viewed through the lens of modern, patient-centered, biologically driven dentistry. The proposed modified-SICTG technique has several advantages over previous methods, as it provides measurable guidelines for clinicians to follow when procuring CTG.
By pre-incisional mapping, clinicians can manage and easily control the depth of the first incision, thus avoiding irregular dimensions of graft thickness, and reduce the chances of over- or under-thick grafts. Further, a 0.5–0.7 mm guide for the first incision is directly corroborated by histological measurements, providing a safe and reproducible threshold for clinicians to perform partial thickness flap elevation without epithelial retention or flap perforation. Studies have confirmed that the epithelial surface contributes roughly 0.2–0.4 mm to the total palatal mucosal thickness.15–18 Therefore, starting the initial split-thickness dissection at 0.5–0.7 mm ensures that the incision reliably passes beneath the entire epithelial layer and enters the upper lamina propria, without compromising flap integrity. This depth is biologically appropriate because <0.4 mm risks cutting within the epithelial layer, leaving epithelial remnants or creating a fragile flap, and it is more prone to sloughing or perforation. Thus, mapping and surgical modification would help reduce complications and enhance the predictability of procuring the graft.
Another advantage of the modified-SICTG technique is the ability to selectively include or exclude periosteum in the harvested graft by adjusting the depth of the third incision in the second dissection plane. Subsequently, a medial plane defining releasing incision placed parallel to the second partial thickness flap incision is used to define the separation plane between the graft and the underlying palatal tissue. This essentially involves a preparatory step consisting of full-thickness reflection that enables precise, biologically guided mid-plane dissection and prevents thinning or irregular graft dimensions (an issue frequently encountered). This two-plane strategy reconciles the apparent distinction between full-thickness and partial-thickness steps and represents a key conceptual element of the modified-SICTG. The early single incision method included the periosteum, leaving the bone exposed, 3 whereas Del Pizzo et al. 6 demonstrated that preserving the periosteum enhances granulation and accelerates palatal healing. Conversely, Yadav et al. 19 reported that CTG harvested using the SICTG technique with periosteum offers the advantage of reduced operative time while providing comparable healing outcomes and pain perception to CTG harvested without periosteum.
A further critical aspect of CTG procurement with the single-incision technique is medial separation of the graft, which is often the most technically demanding step, particularly for less experienced clinicians. This may prolong harvesting and reduce the predictability of graft dimensions compared with the trapdoor and FDD methods. In this context, our modification advocates for tactile, instrument-guided medial dissection using a fine #17 explorer, introduced under the flap and advanced gently toward the mid-palatal aspect, which offers a practical solution. Kumar et al. 10 addressed this issue by developing an AVS blade. 11 The curved, blunt working ends of these instruments allow the operator to feel the medial attachment and sever it in a controlled manner, rather than relying on forceful traction on the graft. This not only facilitates safe medial detachment in an otherwise “blind” zone but also helps preserve the integrity and thickness of the overlying palatal flap, whose integrity is essential for primary closure and reduced morbidity. Lorenzana and Allen 3 highlighted flap preservation as a key advantage of the single incision technique.
Another notable advantage of the proposed modification is the incorporation of two additional steps into the clinical protocol, that is, preoperative donor site assessment and postoperative biologically driven wound management. Preoperative evaluation of palatal thickness using transgingival probing, CBCT, or ultrasound ensures that areas with adequate residual lamina propria are selected, thereby preventing inadvertent over-thinning of the donor flap and reducing postoperative complications such as sloughing or flap perforation. 20 This aligns with evidence demonstrating that palatal thickness varies considerably across individuals and sites, influencing graft quality and morbidity. 21 The second component, that is, enhanced postoperative donor-site management, draws from advancements in regenerative biomaterials. The optional use of PRF, collagen, and PBM has been shown to significantly accelerate palatal wound healing by promoting angiogenesis, reducing postoperative bleeding and discomfort, and enhancing mitochondrial activity.22–26
This technical manuscript proposed a modified-SICTG technique; however, it poses a few limitations. The method was performed in a few limited clinical settings by experienced operators, so its reproducibility in different clinical environments remains to be established. Further, key steps such as biplanar dissection and instrument-guided medial separation remain technique-sensitive. Since this is primarily a technical/clinical technique description, rather than a case report or a randomized controlled trial, future studies are required to include controlled clinical trials, multicenter validation, and histologic or imaging-based assessment of graft architecture to strengthen the evidence for this modified technique.
Conclusion
The current innovative modified-SICTG does not necessarily mean abandoning established principles. By integrating preoperative tissue mapping, controlled plane-specific dissection, flexible graft design, and optional regenerative wound support, this approach aims to provide a structured method for palatal connective tissue harvesting. It must be emphasized that the present work represents a technical and conceptual proposal derived from accumulated clinical experience and does not present a clinical case report or comparative outcome data, which must be interpreted as hypothesis-generating based on operative rationale. Therefore, its clinical advantage in terms of graft quantity, healing, morbidity, and patient-reported outcomes remains to be established. Prospective clinical studies are required to validate the safety, effectiveness, and reproducibility of this modified-SICTG approach before definitive clinical recommendations can be made.
Footnotes
Acknowledgments
The authors gratefully acknowledge Dr. Akanksha Dubey, Lecturer, Saraswati Dental College & Hospital, Lucknow, for meticulously creating the line diagrams that depict the procedural details presented in this manuscript. Her assistance significantly enhanced the clarity and visual understanding of the technique.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.