
Abstract
Introduction
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) can relieve end-stage arthritis and pain in patients with metastatic disease, but this population faces increased perioperative risk because of malignancy and treatment-related immunosuppression. Frailty indices such as the 5-Factor Modified Frailty Index (mFI-5) and Risk Analysis Index (RAI) may improve preoperative risk stratification. This study compared their ability to predict postoperative outcomes after primary THA/TKA.
Methods
The ACS-NSQIP database (2015-2020) was reviewed for patients with metastatic disease undergoing primary THA or TKA. Frailty scores were calculated using RAI and mFI-5. Multivariable regression estimated odds ratios (ORs) for adverse outcomes, and discriminatory accuracy was assessed with area under the curve (AUC).
Results
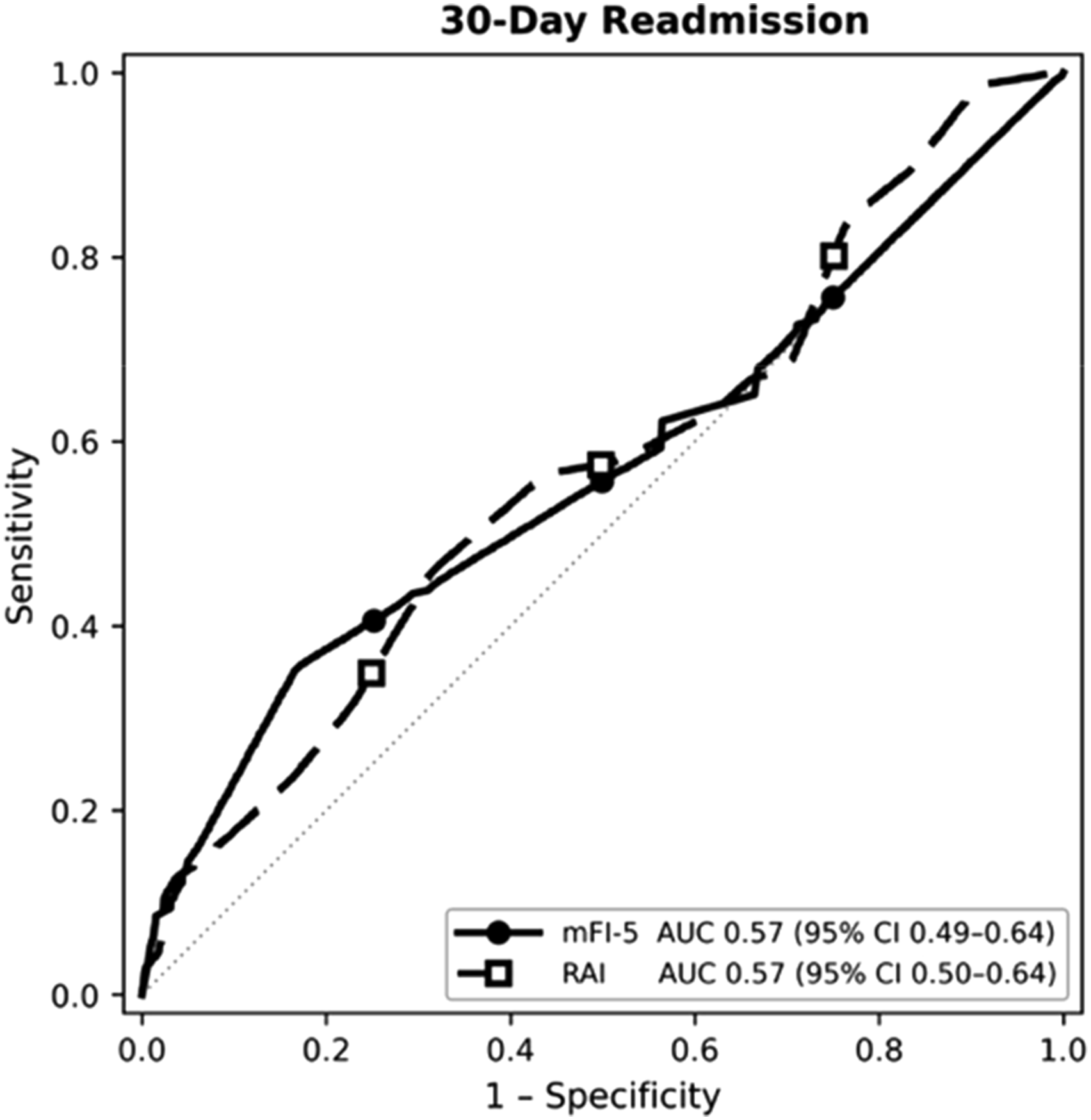
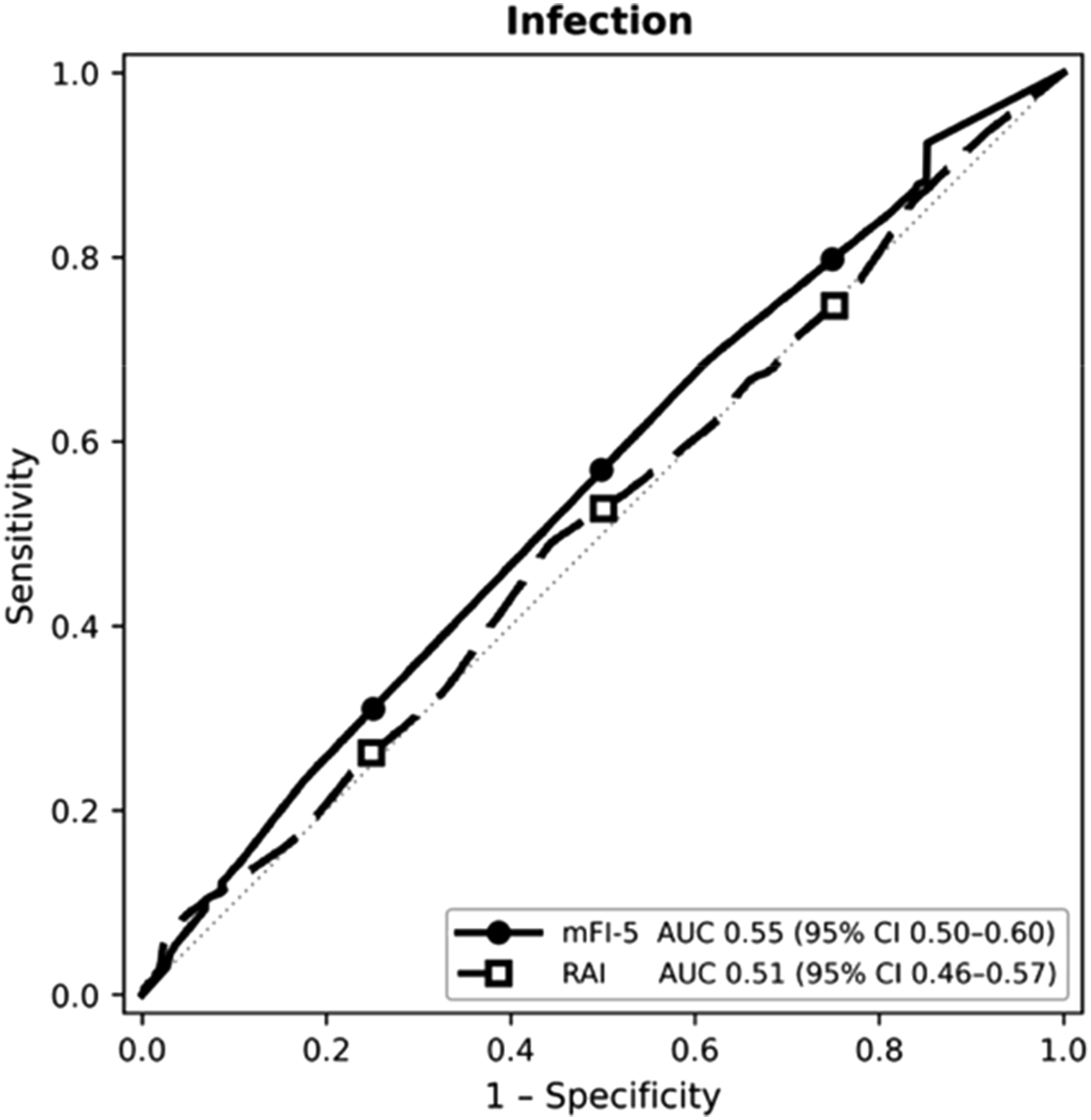
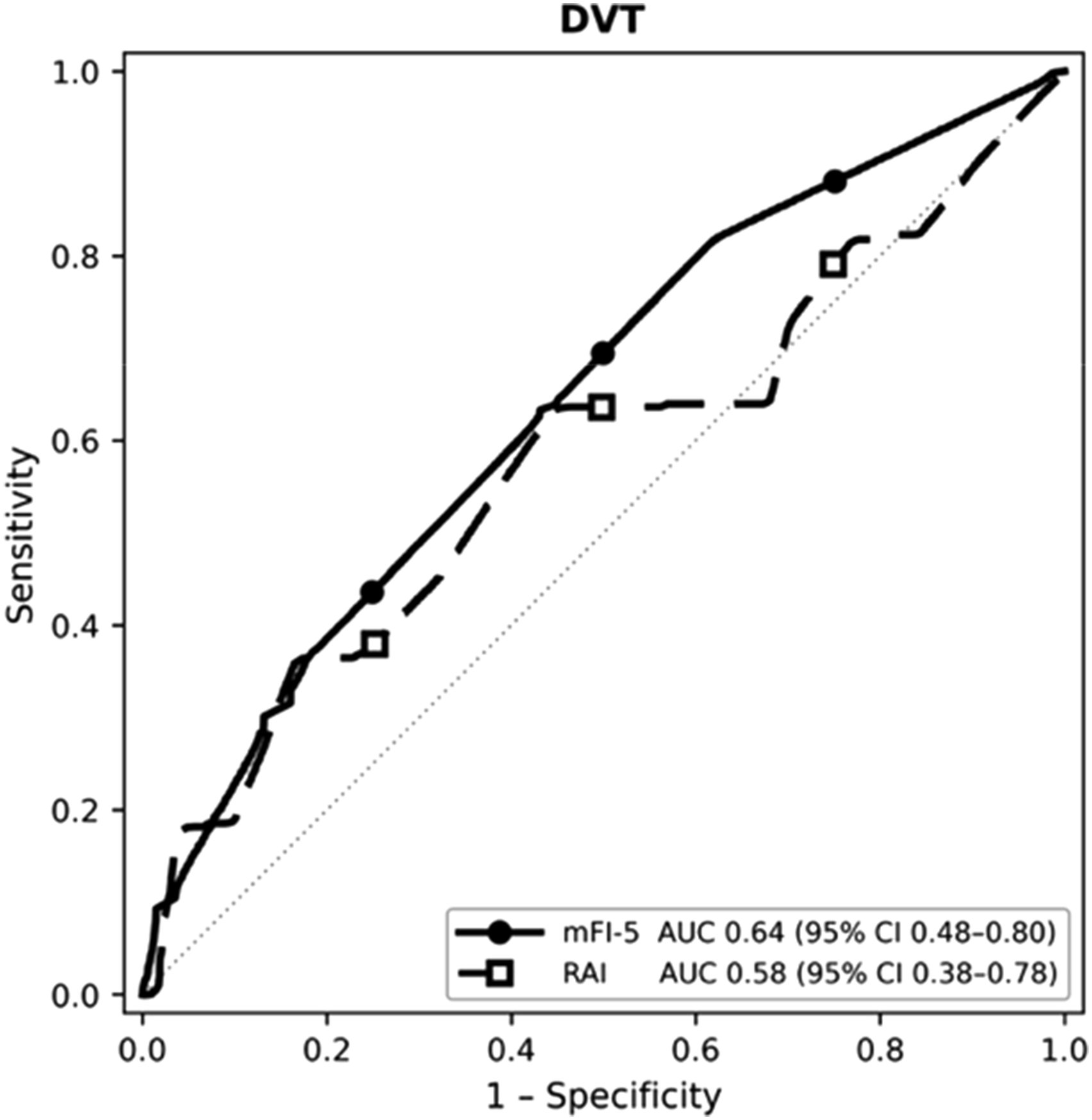
Among 1115 patients (median age 69 years), median length of stay was 2 days, 4.9% had major complications, and 22.6% required non-home discharge. RAI independently predicted extended length of stay and non-home discharge and showed the strongest discrimination for mortality. mFI-5 predicted 30-day readmission and modestly outperformed RAI for this outcome. Procedure-specific analyses showed RAI best predicted mortality after THA and extended length of stay after TKA. Overall, both indices demonstrated only modest discrimination.
Conclusion
Frailty assessment may improve risk stratification in metastatic patients undergoing primary THA/TKA.
Keywords
Introduction
Total joint arthroplasty (TJA) remains one of the most effective interventions for alleviating pain and restoring function in patients with end-stage joint disease. The number of TJA has been increasing annually, with 544 000 hip replacements and 790 000 knee replacements occurring annually in recent years within the US. 1 Patients with metastatic disease present one of the more challenging considerations when contemplating TJA, as these patients are often compromised by widespread systemic disease and, as a result, may require TJA to address disabling joint disease. 2 Should TJA proceed in these patients, it often entails a careful balancing of benefits such as pain relief and improved mobility with risk of intra- and postoperative complications, prolonged recovery, and reduced postoperative survival, given the patients’ general frailty.3-7 Given this complexity, preoperative frailty assessment has emerged as a critical adjunct in evaluating surgical candidacy and optimizing outcomes for patients with metastatic disease undergoing TJA.
Frailty indices have been shown to predict preoperative stratification of surgical candidates for various surgical procedures in the literature.5,8,9 Several frailty indices have been used to predict outcomes following orthopedic surgery. The mFI-5 is the traditional frailty index that incorporates 5 major clinical variables: hypertension, congestive heart failure, comorbid diabetes, chronic obstructive pulmonary disease, and partially or fully dependent functional status.3-7 The Risk Analysis Index-Revised (RAI) is a more comprehensive frailty assessment that incorporates a broad array of clinical factors, including age, sex, cancer history, unintentional weight loss, poor appetite (nutritional status), renal failure, congestive heart failure, dyspnea/shortness of breath, non-independent living status, functional status/activities of daily living, and cognitive decline.8-11 RAI has been compared to mFI-5 and has demonstrated superior predictive ability for postoperative complications in orthopedic surgery, such as spine surgery, traumatic injuries, and TJA, among others.12-16
Although frailty is clinically recognized as an important factor when considering surgical interventions, few studies have explored frailty in the context of TJA in patients with metastatic disease. Therefore, this study aimed to compare the discriminatory accuracy of the RAI and mFI-5 in predicting short-term postoperative outcomes among patients with metastatic disease undergoing primary total hip or knee arthroplasty. We hypothesized that the RAI, given its multidimensional assessment of frailty, would outperform the mFI-5 in identifying patients at highest risk for adverse postoperative events.
Methods
Data Source
The American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database was designed in 1994 by the Veterans Health Administration to improve the quality of healthcare delivery. In compliance with the NSQIP Data Use Agreement, we queried the NSQIP database from 2015 to 2020, encompassing roughly 6 million de-identified patient records and over 200 variables related to patient demographics, medical history, and postoperative outcomes.
Patient Population, Baseline Characteristics, and Outcomes
Inclusion criteria for this study were patients aged 18 years or older with disseminated cancer included using the built-in NSQIP variable “disseminated cancer” undergoing primary THA (CPT 27130) and TKA (CPT 27447). Patients undergoing fixation for pathologic fractures and primary bone tumors or sarcomas were excluded.
Variables of Interest and Primary Outcome
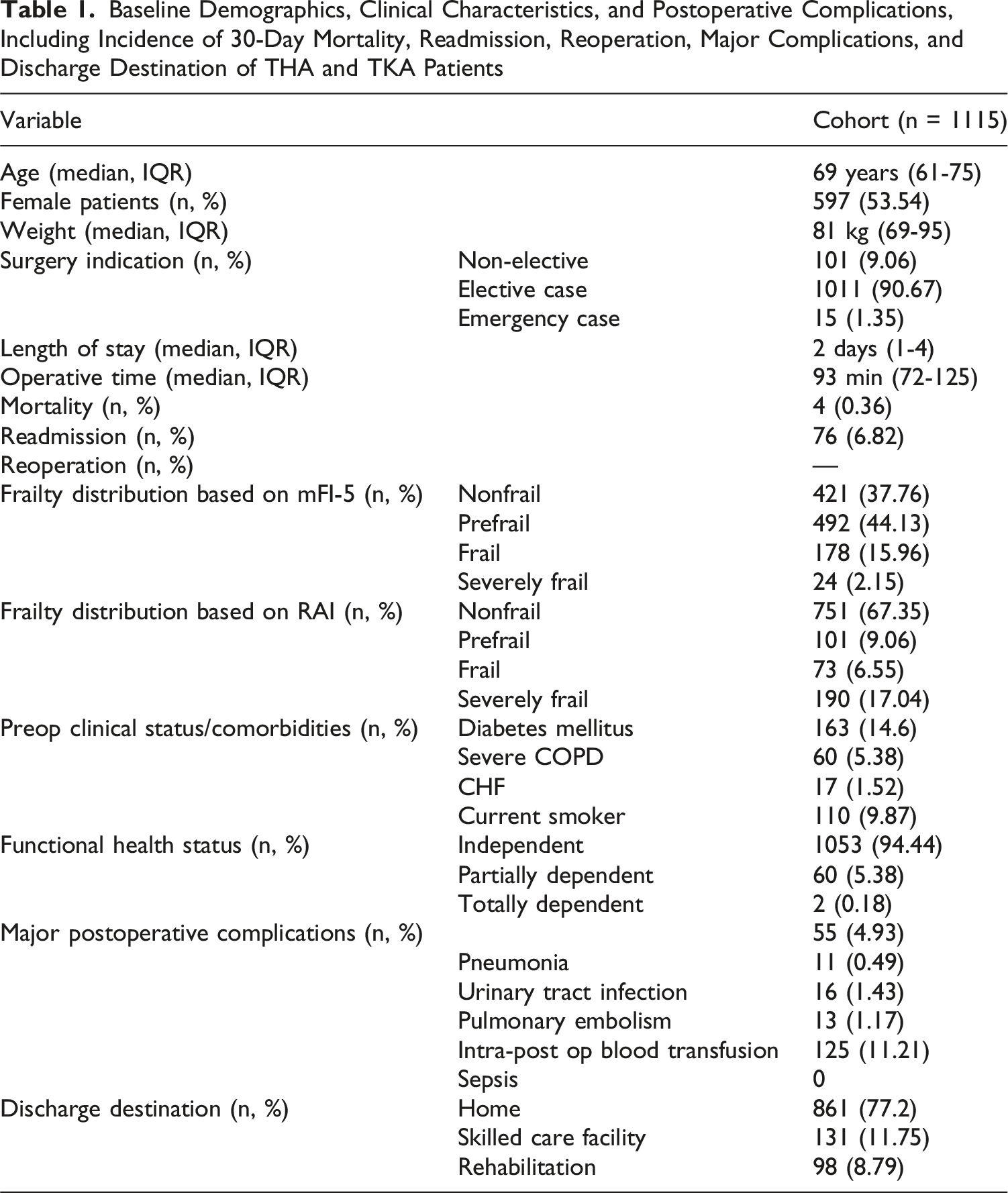
Baseline Demographics, Clinical Characteristics, and Postoperative Complications, Including Incidence of 30-Day Mortality, Readmission, Reoperation, Major Complications, and Discharge Destination of THA and TKA Patients
Frailty Measures
Frailty was measured using the mFI-5 and RAI. The mFI-5 includes the following variables: congestive heart failure, COPD, hypertension, diabetes, and non-independent functional status. One point was assigned for each diagnosis, and the total number of points for each patient was calculated. Patients were grouped into 3 categories based on their frailty score: 0 = nonfrail, 1 = prefrail, and ≥ 2 = frail. Frailty as rated by the RAI was assessed using the RAI scoring system, adapted from previous studies by Arya and Hall et al.17,18 The RAI incorporates multiple weighted variables, which encompass domains of frailty including sex, age, cancer diagnosis (excluding melanoma), weight loss (unintentional weight loss of 4.5 kg over 3 months), renal failure, CHF, poor appetite, shortness of breath at rest, residence status (independence of living), cognitive decline, and activities of daily living (Table 1). RAI frailty tiers were delineated as follows: robust ≤ 10, normal 11-20, frail 21-30, and very frail ≥ 31.
Statistical Analysis
Patients were grouped according to frailty status, and demographic characteristics were assessed using the Chi-Square test for categorical variables and the Kruskal-Wallis test for continuous variables. Categorical variables were presented as counts with percentages, and continuous variables were presented as medians with interquartile ranges. We initially conducted univariate regression for each variable and the binary outcomes. Backward stepwise P-value removal was used to build the final model, and model fit was assessed using the area under the curve (AUC). Only variables that were significant at or below 0.05 were retained in the final model. Receiver operating characteristic (ROC) curve analysis, including the AUC/C-statistics, was used to quantify the discrimination of each model. Differences in predictive performance (c-statistic) were assessed using the DeLong test. All statistical analysis was performed using the Statistical Package for Social Sciences (SPSS, Version 29; IBM, Inc., Armonk, NY). For all purposes, a P-value <0.05 was considered statistically significant.
Results
Patient Population Baseline Characteristics
A total of 1115 patients (53.5% female) undergoing primary TJA for metastatic disease were included (Table 1). The median age was 69 years (IQR 61-75 years), and the median weight was 81 kg (IQR 69-95 kg). Active smoking within the prior year was reported in 9.9% (n = 110) of patients. The most common comorbidities included hypertension requiring medication (n = 620, 55.6%), type 2 diabetes mellitus (n = 163, 14.6%), and severe COPD (n = 60, 5.4%). Most patients were functionally independent preoperatively (94.4%) and underwent elective procedures (90.7%).
Frailty stratification by mFI-5 identified 421 (37.8%) nonfrail, 492 (44.1%) prefrail, 178 (16.0%) frail, and 24 (2.2%) severely frail patients. Frailty classification by RAI demonstrated 751 (67.4%) nonfrail, 101 (9.1%) prefrail, 73 (6.6%) frail, and 190 (17.0%) severely frail. The median operative time was 93 min (IQR 72-125 min), and the median hospital stay was 2 days (IQR 1-4 days). Major postoperative complications occurred in 55 patients (4.9%), including pneumonia (1.0%), pulmonary embolism (1.2%), and urinary tract infection (1.4%). Blood transfusion was required in 125 (11.2%) cases. Readmission within 30 days occurred in 76 patients (6.8%), while mortality during index hospitalization was 0.36% (n = 4). The majority of patients (861) were discharged home (77.2%), with 131 patients (11.8%) discharged to skilled nursing facilities and 98 patients (8.8%) to rehabilitation (Table 1).
Multivariable Analysis
Multivariable Analysis Controlling for Extended Length of Stay (eLOS), Non-Home Discharge (NHD), 30-Day Readmission, Mortality, Infection, and Deep Vein Thrombosis (DVT) for Each Cohort for Each Primary Outcome. Results Are Presented as Odds Ratio (OR) and 95% Confidence Interval
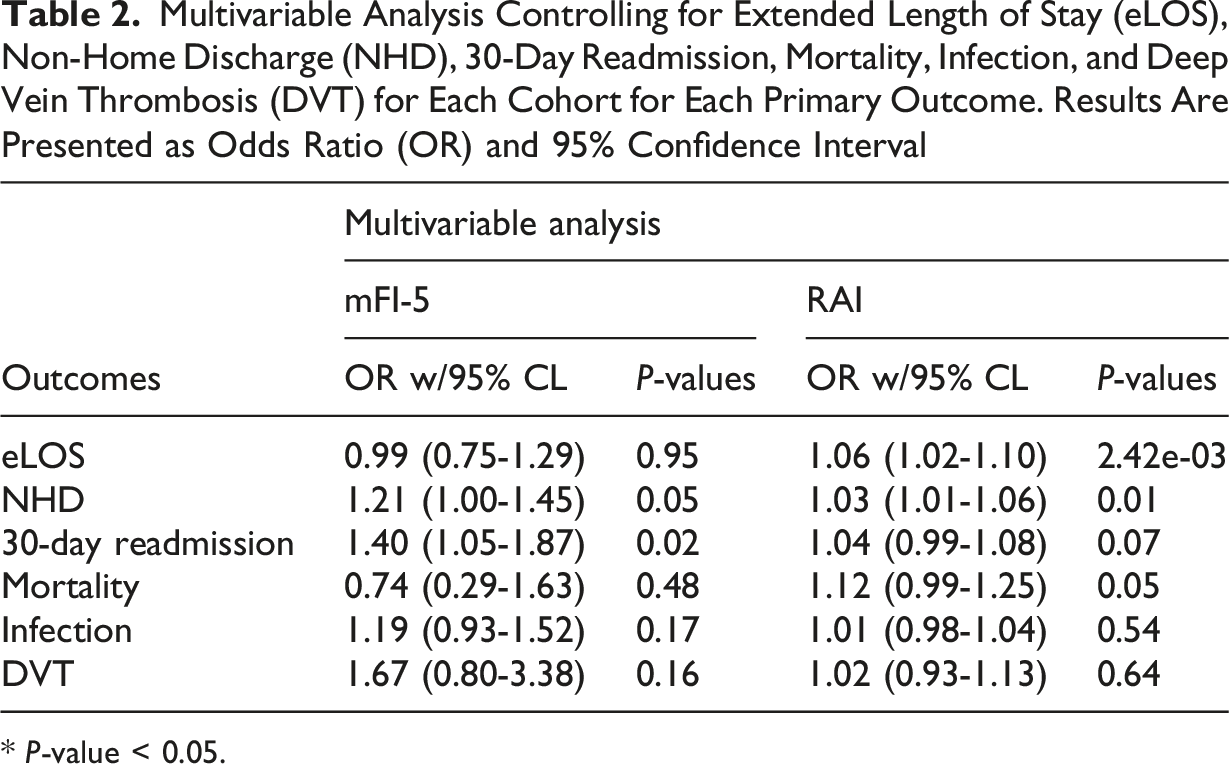
* P-value < 0.05.
When stratified by procedure, distinct patterns were observed. Among THA patients (n = 685), RAI was independently associated with mortality (OR 1.20, 95% CI 1.03-1.39; P = 0.02) and NHD (OR 1.04, 95% CI 1.01-1.07; P = 0.02). Among TKA patients (n = 430), RAI was significantly associated with eLOS (OR 1.11, 95% CI 1.02-1.22; P = 0.02), and mFI-5 was a significant predictor of 30-day readmission (OR 2.12, 95% CI 1.13-4.03; P = 0.02). Neither frailty tool was associated with mortality, infection, or DVT in the TKA subgroup.
ROC Analysis
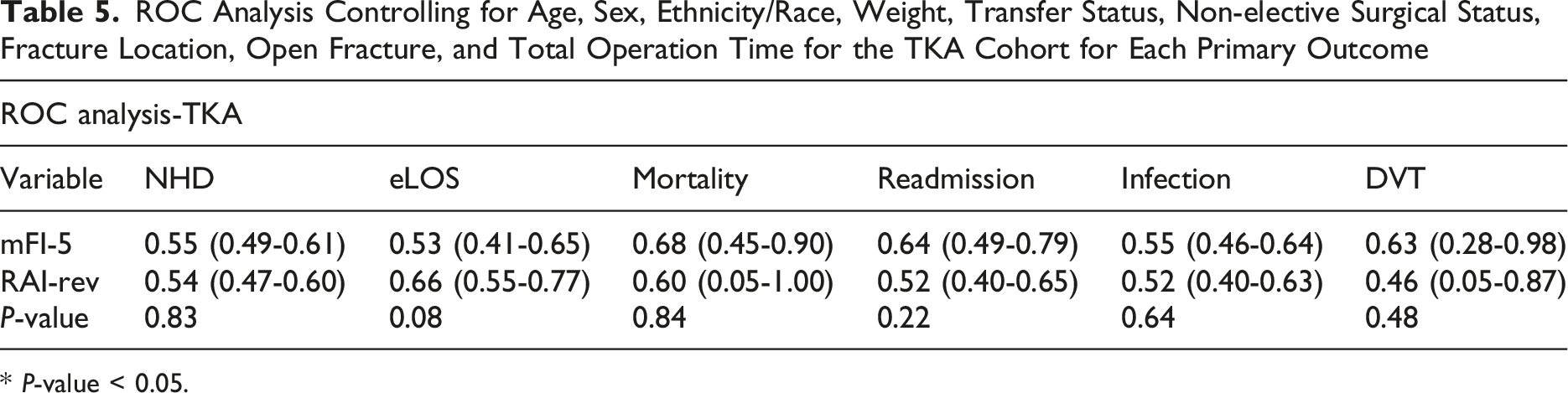
ROC Analysis Controlling for Age, Sex, Ethnicity/Race, Weight, Transfer Status, Non-elective Surgical Status, Fracture Location, Open Fracture, and Total Operation Time for Each Cohort for Each Primary Outcome
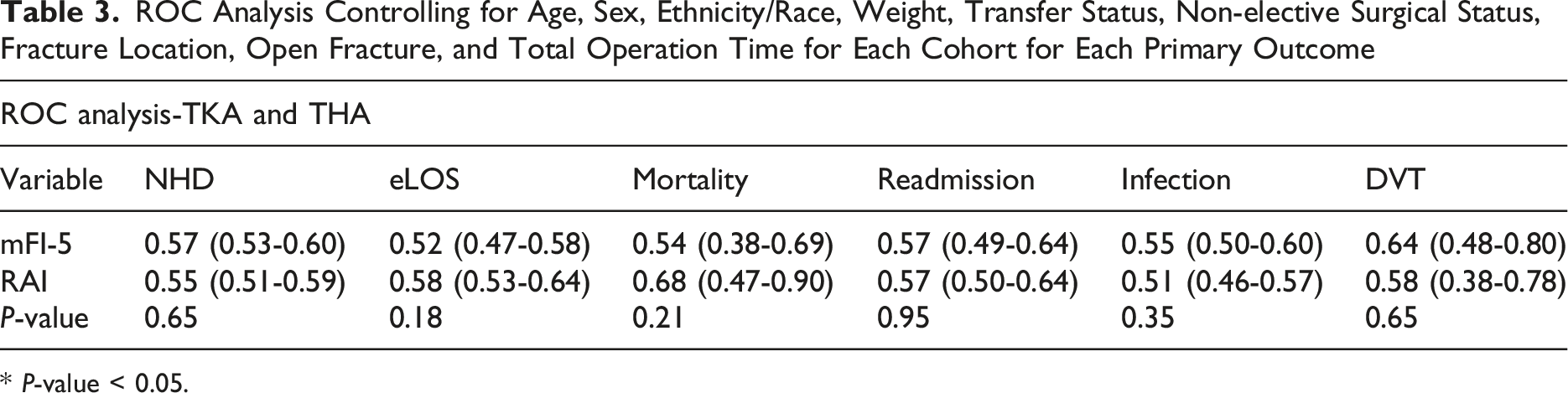
* P-value < 0.05.
ROC Analysis Controlling for Age, Sex, Ethnicity/Race, Weight, Transfer Status, Non-elective Surgical Status, Fracture Location, Open Fracture, and Total Operation Time for the THA Cohort for Each Primary Outcome
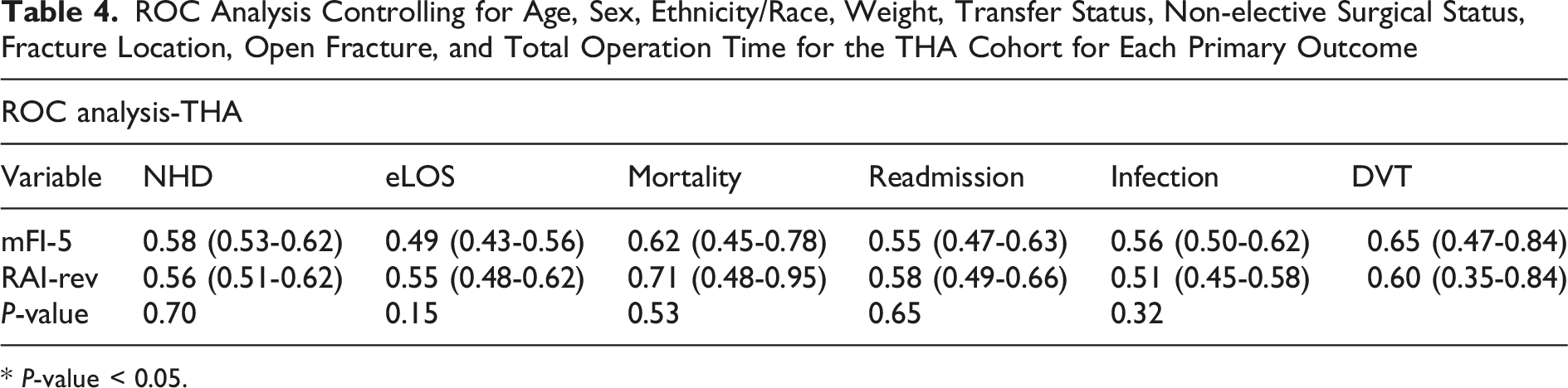
* P-value < 0.05.
ROC Analysis Controlling for Age, Sex, Ethnicity/Race, Weight, Transfer Status, Non-elective Surgical Status, Fracture Location, Open Fracture, and Total Operation Time for the TKA Cohort for Each Primary Outcome
* P-value < 0.05.
Summary of Frailty Distribution, Outcomes, and Predictive Performance. Composite summary of frailty classification, postoperative outcomes, and predictive accuracy among patients with disseminated cancer undergoing total hip or knee arthroplasty. Figure 1 shows frailty distribution between RAI and mFI-5
Summary of Frailty Distribution, Outcomes, and Predictive Performance. Composite summary of frailty classification, postoperative outcomes, and predictive accuracy among patients with disseminated cancer undergoing total hip or knee arthroplasty. Figure 2 demonstrates increasing rates of prolonged length of stay (eLOS > 75th percentile), non-home discharge (NHD), readmission, and complications with greater frailty severity
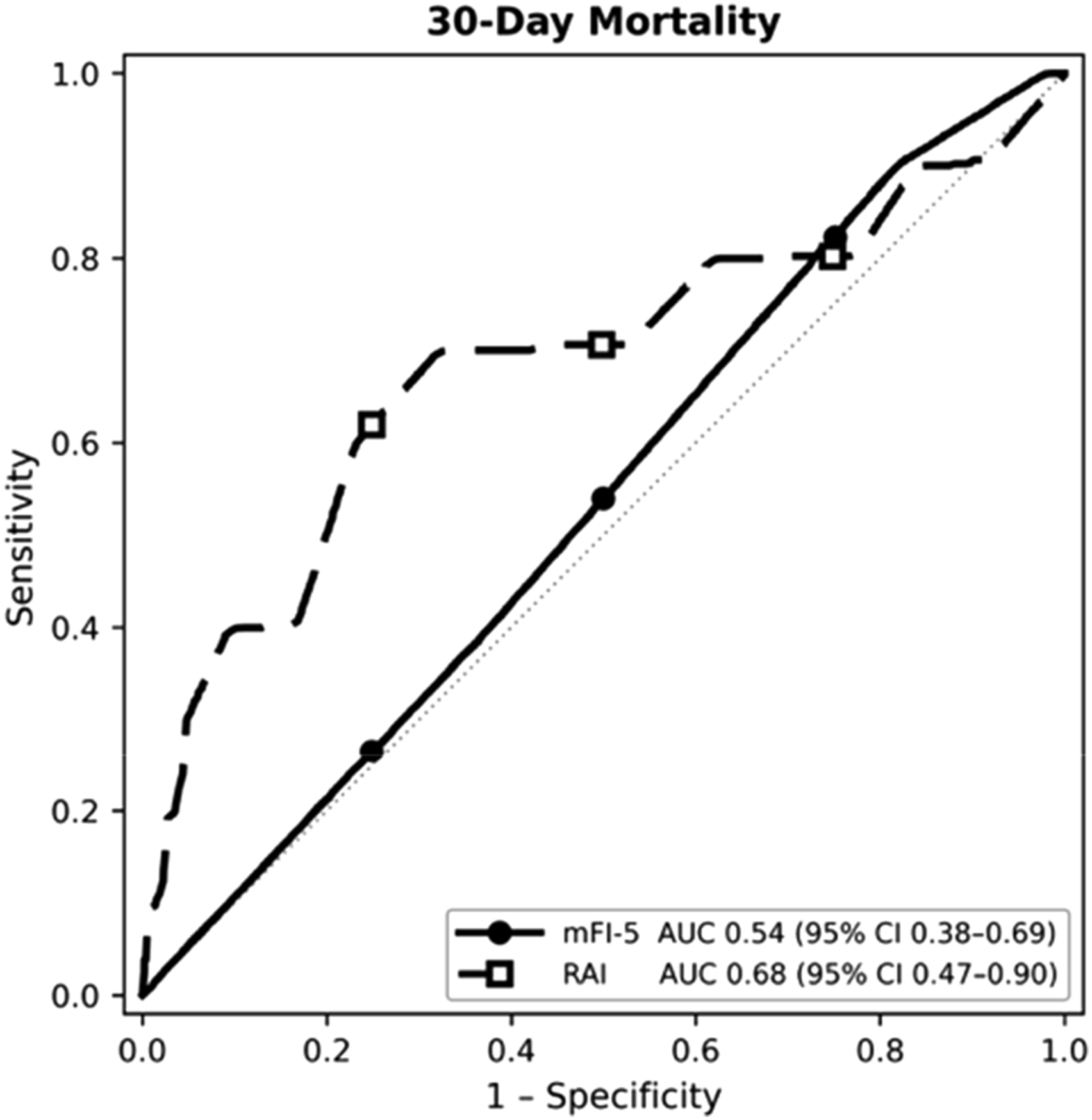
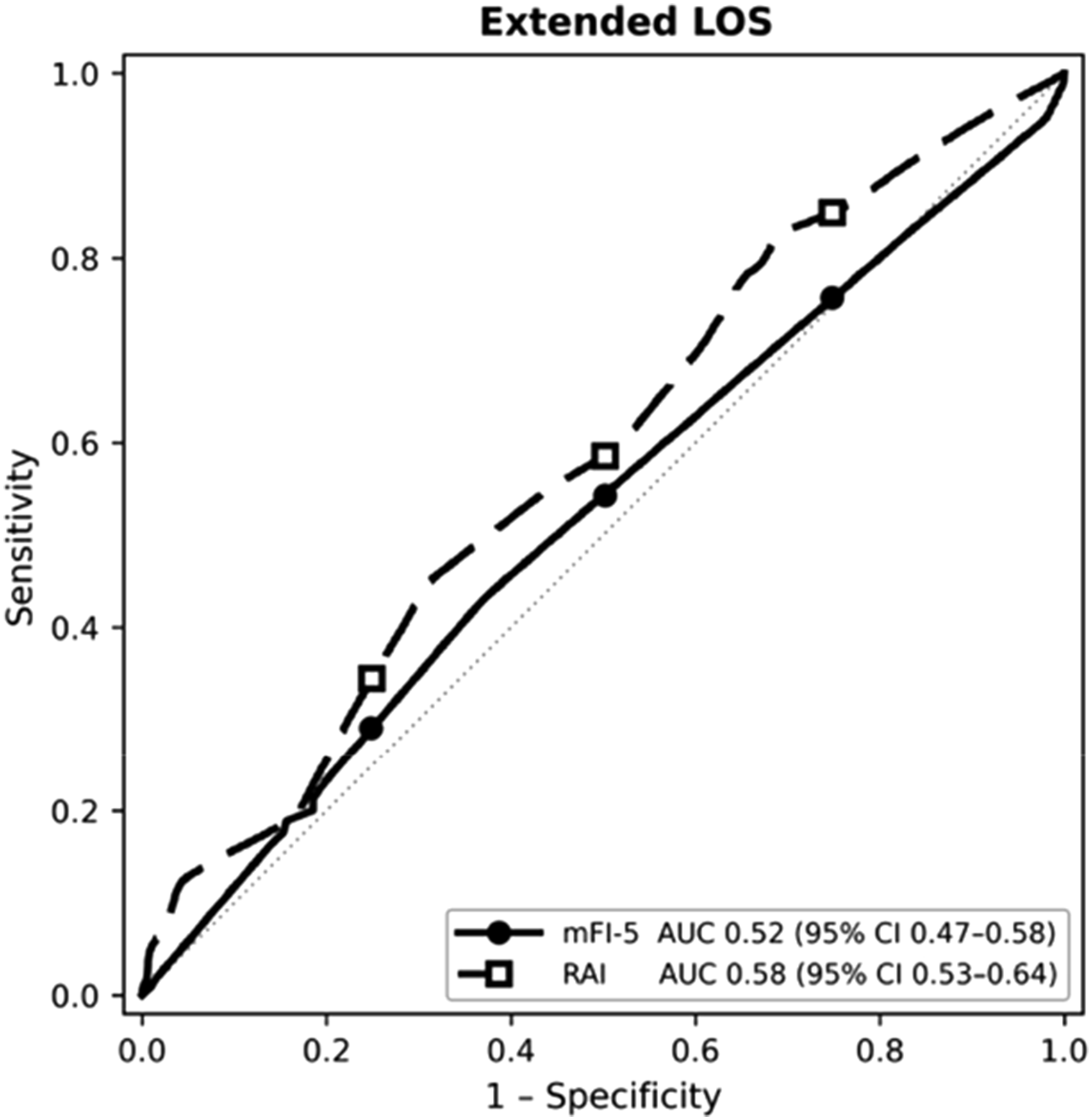
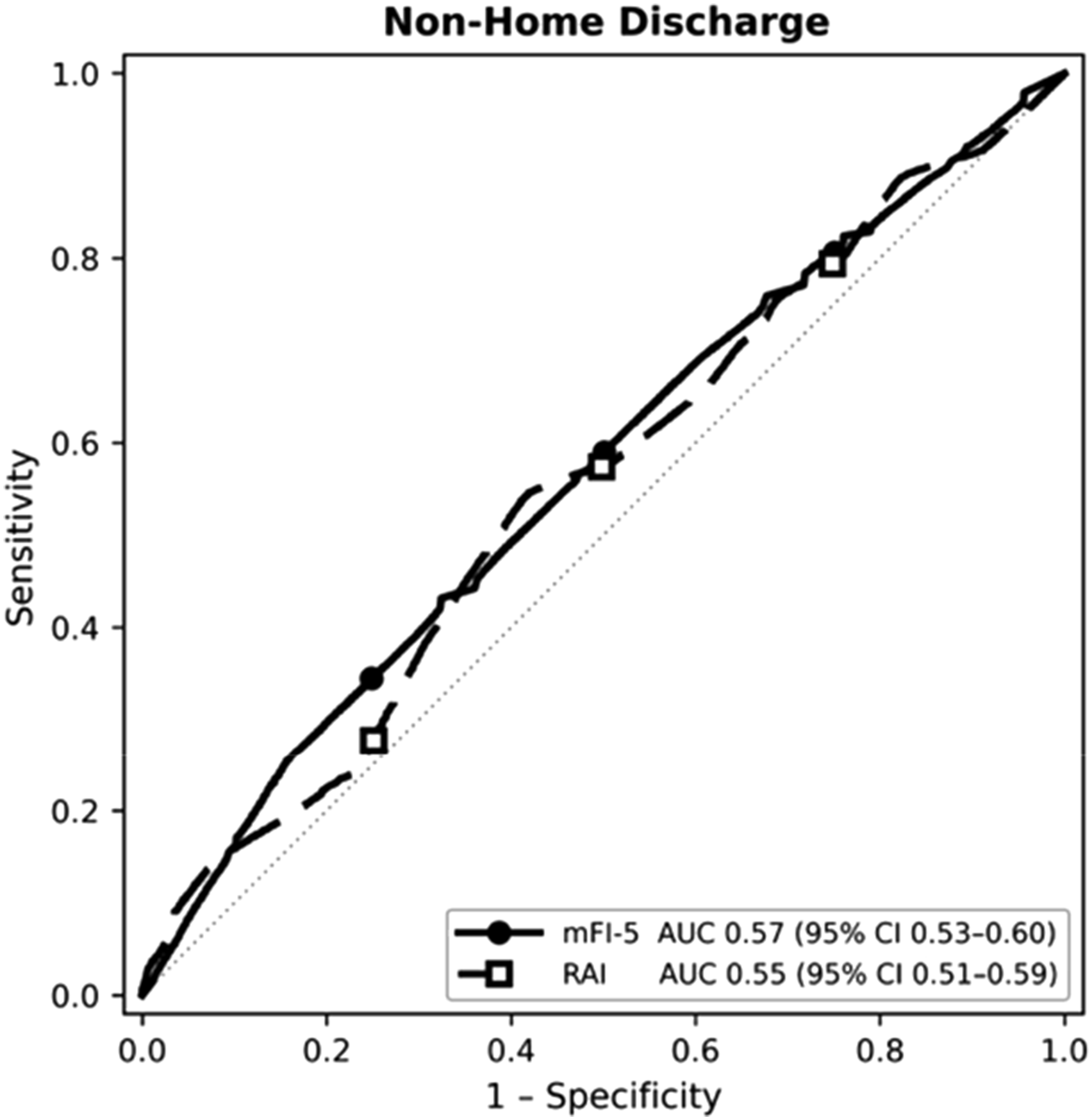
Summary of Frailty Distribution, Outcomes, and Predictive Performance. Composite summary of frailty classification, postoperative outcomes, and predictive accuracy among patients with disseminated cancer undergoing total hip or knee arthroplasty. Figure 1 shows frailty distribution between RAI and mFI-5. Figures 3-5 present ROC curves comparing mFI-5 and RAI for predicting NHD, eLOS, and mortality
Summary of Frailty Distribution, Outcomes, and Predictive Performance. Composite summary of frailty classification, postoperative outcomes, and predictive accuracy among patients with disseminated cancer undergoing total hip or knee arthroplasty. Figure 1 shows frailty distribution between RAI and mFI-5. Figures 4 present ROC curves comparing mFI-5 and RAI for predicting NHD, eLOS, and mortality
Summary of Frailty Distribution, Outcomes, and Predictive Performance. Composite summary of frailty classification, postoperative outcomes, and predictive accuracy among patients with disseminated cancer undergoing total hip or knee arthroplasty. Figure 1 shows frailty distribution between RAI and mFI-5. Figures 3-5 present ROC curves comparing mFI-5 and RAI for predicting NHD, eLOS, and mortality
Summary of Frailty Distribution, Outcomes, and Predictive Performance. Composite summary of frailty classification, postoperative outcomes, and predictive accuracy among patients with disseminated cancer undergoing total hip or knee arthroplasty. Figure 1 shows frailty distribution between RAI and mFI-5. Figure 6 summarizes multivariable odds ratios and 95 % CIs for adverse outcomes, with asterisks denoting P < 0.05
Discussion
Patients with metastatic disease who undergo primary TKA or THA represent a uniformly vulnerable cohort in whom even routine arthroplasty carries substantial perioperative risk. With approximately 400,000 new cases of malignant metastasis diagnosed annually in the United States, accurate risk stratification is crucial for predicting postoperative complications, readmission, NHD, and mortality in patients undergoing total joint arthroplasty.19,20 Our study found that higher RAI-defined frailty independently predicted eLOS and NHD, with a borderline association with mortality, whereas mFI-5 most strongly predicted 30-day readmission, particularly in the TKA subgroup. ROC analysis further demonstrated that RAI provided the highest discrimination for mortality (AUC 0.68 overall; 0.71 after THA) and eLOS after TKA (AUC 0.66), while mFI-5 modestly outperformed RAI for readmission (AUC 0.64 vs 0.57). These results support RAI as a clinically useful frailty-based predictor of perioperative complications and resource-intensive recovery, with mFI-5 providing complementary information for readmission risk, and both indices are best applied as supportive tools within a broader risk stratification framework.
Our study found that frailty as determined by RAI was a stronger predictor of NHD and eLOS compared with mFI-5. This may be explained by the clinical characteristics RAI includes. RAI incorporates domains such as unintentional weight loss, poor appetite, cognitive decline, residence status, and dependence in activities of daily living, which are features heavily influenced by metastatic disease, cancer-related cachexia, and treatment-related deconditioning. 11 These domains are closely linked to functional recovery, rehabilitation potential, and the ability to discharge home safely, which likely explains the stronger association between higher RAI scores and both NHD and eLOS. In contrast, mFI-5 is based on “traditional” medical comorbidities such CHF, COPD, diabetes, hypertension, and functional dependence. These are comorbidities that predispose patients to cardiopulmonary and metabolic complications that commonly precipitate early unplanned readmissions. 21 Thus, mFI-5 may better capture the cumulative burden of chronic disease and baseline functional limitation in metastatic patients in the context of 30-day readmission, while the broader functional and nutritional domains within the RAI more accurately reflect the physical recovery required for safe discharge home. Notably, the RAI’s inclusion of cognitive and nutritional elements, often impaired in metastatic patients, likely contributes to its superior prediction of post-acute care needs and discharge disposition.11,16
These distinctions have meaningful clinical implications for perioperative decision-making and resource allocation. In practical terms, our findings suggest that elevated RAI scores can be used to identify metastatic arthroplasty patients at heightened risk for prolonged hospitalization, NHD, and mortality, whereas mFI-5 may be most helpful for anticipating early unplanned readmissions. However, our findings also suggest that frailty assessment in metastatic arthroplasty should not be viewed as a definitive tool to direct management but rather as a framework to anticipate different types of risk. High RAI scores may be useful for counseling patients and families regarding expectations for prolonged hospitalization, likelihood of NHD to skilled nursing or rehabilitation facilities, and the potential need for intensive post-acute support.2,22 In this context, integrating RAI into preoperative management could initiate earlier engagement of physical therapy, social work, and case management, as well as consideration of prehabilitation and nutritional optimization to mitigate functional decline. 23 While mortality is inherently less modifiable, NHD, eLOS, and readmission are more responsive to proactive perioperative planning, for which frailty screening serves as a practical tool to prioritize limited rehabilitative and supportive resources.
When considered in the context of prior research, our findings both corroborate and expand upon established evidence regarding frailty and surgical outcomes. In the realm of spine surgery, Bowers et al reported that the RAI had superior discrimination for predicting postoperative mortality and morbidity compared to the mFI-5, particularly in trauma, tumor, and infection subcohorts. 16 Similarly, Owodunni et al found that the RAI outperformed both mFI-5 and age alone in predicting 30-day mortality after spine surgery, with a dose-dependent relationship between frailty and adverse outcomes. 8 Conversely, Pierce et al found that the mFI-5 is an effective predictor of postoperative events following spine surgery, with increasing frailty scores associated with higher odds of complications, readmission, and mortality. 24 In arthroplasty populations, Traven et al demonstrated similar results that the mFI-5 is a strong independent predictor of postoperative complications, surgical site infections, readmission, and 30-day mortality after primary hip and knee arthroplasty. 25 Nonetheless, RAI’s adequate discrimination for mortality after THA in our analysis aligns with prior frailty literature and emphasizes its value even when absolute predictive precision is limited. This suggests that while frailty remains central to risk stratification, generic indices utilized in broader surgical cohorts may underperform when applied to patients with advanced metastatic cancer undergoing arthroplasty.
The novelty and clinical importance of our study apply to frailty assessment in metastatic arthroplasty, a setting that is biologically and clinically distinct from standard TJA. Patients undergoing arthroplasty in the context of disseminated malignancy are affected by cancer-related cachexia, sarcopenia, systemic inflammation, and treatment-related toxicities that alter their recovery trajectory. 11 Chemotherapy, targeted therapies, radiation, chronic corticosteroids, and endocrine treatments can impair immune function, wound healing, and cardiopulmonary reserve, while disease-related immobility and neurologic compromise further diminish baseline function. 26 Traditional frailty indices such as mFI-5 do not explicitly capture nutritional depletion, cytokine-driven inflammation, or exposure to immunosuppressive regimens, and even RAI, though it incorporates weight loss, poor appetite, cognitive decline, and ADL dependence, only partially reflects these domains. The fact that RAI, with broader nutritional and cognitive components, demonstrated comparatively better performance for NHD, eLOS, and mortality supports the notion that cancer-related frailty is driven by multifaceted vulnerability that extends beyond typical comorbidities. These observations highlight an opportunity to further develop frailty instruments that integrate oncology-specific variables such as cancer stage, treatment intensity, inflammatory and nutritional biomarkers, and performance status to more accurately characterize risk and inform shared decision-making for patients with metastatic disease being considered for TJA.
Limitations
This study has several limitations. First, the analysis is retrospective and relies on registry data, which introduces the potential for selection bias, unmeasured confounding, and miscoding or misclassification that are intrinsic to large administrative databases. 27 Second, NSQIP does not provide specific oncologic details such as primary tumor type, metastatic burden, cancer stage, specific systemic therapies or radiation regimens, timing of oncologic treatment relative to surgery, or validated performance status measures; the absence of this cancer-specific information likely attenuates the power of each frailty index and may partially account for the modest discriminatory accuracy observed. Furthermore, outcomes are limited to the 30-day postoperative period and do not capture longer-term endpoints such as functional recovery, implant survival, disease progression, late complications, or overall survival, which are critically important in the metastatic arthroplasty population. Additionally, readmissions and complications occurring outside NSQIP-participating hospitals may be incompletely captured, and we were unable to account for institutional protocols, surgeon experience, or perioperative care pathways that could influence discharge disposition and resource use. Finally, both RAI and mFI-5 were operationalized using variables available within NSQIP and may not fully reflect their performance when implemented in a prospective, clinic-based setting, underscoring the need for external validation and for future studies incorporating more detailed oncologic and patient-reported data.
Conclusion
In patients with metastatic disease undergoing primary total hip and knee arthroplasty, increasing frailty was independently associated with key postoperative outcomes, underscoring its clinical relevance in this medically complex population. Across indices, the RAI demonstrated more consistent and clinically meaningful associations, modestly outperforming on eLOS, NHD, and mortality compared to mFI-5, which was more effective in identifying patients at increased risk for 30-day readmission. Although both indices exhibited only modest discriminatory accuracy overall, an AUC of 0.71 for mortality after THA suggests that RAI provides adequate discrimination for the most severe endpoint in this cohort. Despite their modest accuracy, the consistent associations between frailty scores and resource utilization outcomes highlight their practical value in guiding perioperative planning, expectation setting, and shared decision-making for patients with metastatic disease. Frailty assessment continues to grow in importance as an accessible tool for characterizing postoperative risk in medically vulnerable patients. Future research should focus on prospective, cancer-specific cohorts incorporating laboratory markers, nutritional metrics, and oncologic treatment variables, as such integrated models may substantially improve risk prediction and better tailor perioperative decision-making.
Footnotes
Acknowledgements
We would like to thank Dr. Christian Bowers and the Bowers Frailty lab for their valued guidance and assistance on this project.
Consent to Participate
This study was performed under a Health Insurance Portability and Accountability Act-compliant Participant Use Data File which is considered exempt from institutional review board approval. Patient/guardian consent was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.