
Abstract
Background:
Rib remodelling has emerged as a novel adjunct in aesthetic waist contouring. As patients increasingly seek alternatives to traditional procedures such as liposuction and abdominoplasty, rib modification techniques have evolved to meet aesthetic demands. Prior reviews grouped rib resection and remodelling together, limiting clarity on individual outcomes.
Methods:
A systematic review was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines to identify clinical studies reporting outcomes of rib remodelling procedures performed for cosmetic waist narrowing between January 2015 and March 2025. Searches were performed in PubMed, EMBASE, and Scopus. Included studies reported waist reduction, complications, or patient satisfaction and were categorised into five technique groups: Traditional rib resection, rib repositioning with osteosynthesis, dorsal osteotomy, ultrasound-assisted greenstick osteotomy, and RibXcar.
Results:
Nine studies met the inclusion criteria. Techniques varied in invasiveness, instrumentation, and anatomical approach. Reported waist reductions ranged from approximately 6–17 cm. Patient satisfaction was consistently high, especially with minimally invasive methods such as RibXcar and ultrasound-assisted osteotomies. Complication rates were low overall, with pneumothorax occurring only in traditional rib resection cohorts. The need for postoperative compliance, especially with corset use, was a common theme across techniques.
Conclusions:
Rib remodelling appears to be a safe and effective complement to traditional body contouring methods. Technique-specific organisation of outcomes offers greater clarity than prior reviews. However, most studies remain limited by retrospective designs and short follow-up. Prospective research is needed to confirm safety and efficacy over time.
Introduction
Achieving a narrow, exaggerated hourglass waist has led surgeons to explore modifications of the ribcage to complement traditional abdominal contouring procedures such as liposuction and abdominoplasty. While these methods can slim the waist, some patients seek further reduction that only altering the lower ribs can provide. 1 Over the past decade (2015–2025), several techniques have emerged to remodel ribs 11 and 12 for aesthetic purposes. Prior reviews, such as Ferreira et al. (2025), examined rib resection and remodelling broadly but grouped diverse approaches together and provided limited detail on technique-specific outcomes. Given the recent emergence of more refined and minimally invasive techniques, there is a need for a more detailed, technique-based analysis that distinguishes between surgical approaches and compares their outcomes. This systematic review evaluates published clinical outcomes, waist reduction measurements, complication rates, and patient satisfaction across major rib remodelling techniques reported between 2015 and 2025.
Methodology
This study was conducted as a systematic review in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. 2 The goal was to identify and evaluate peer-reviewed clinical studies reporting outcomes of rib remodelling techniques used for aesthetic waist contouring between January 2015 and March 2025. The review focused on adult patients undergoing elective rib modification for cosmetic purposes and excluded cases involving trauma, congenital anomalies, or oncologic surgery. Only English-language articles with full-text availability were considered. Studies were eligible if they included clinical outcomes such as waist circumference reduction, complication rates, or patient satisfaction. Animal studies, cadaveric investigations, editorials, and opinion pieces were excluded.
A comprehensive search was conducted in PubMed, EMBASE, and Scopus using terms such as ‘rib resection’, ‘rib remodelling’, ‘rib repositioning’, ‘greenstick osteotomy’, ‘RibXcar’, ‘waist narrowing surgery’ and ‘aesthetic body contouring’. The final search was completed on 12 April 2025. After removing duplicates, two reviewers independently screened titles and abstracts. Full texts of relevant articles were assessed to confirm eligibility, and any disagreements were resolved through discussion. From each included study, we extracted the publication year, study design, number of patients, technique performed, rib levels treated, waist circumference reduction, duration of follow-up, complication data, and any available measures of patient satisfaction.
To facilitate comparison, included studies were categorised into five main rib remodelling approaches based on surgical technique and anatomical modification: Traditional rib resection, rib repositioning with osteosynthesis, dorsal osteotomy (as described by Kudzaev), ultrasound-assisted greenstick osteotomy, and RibXcar. Because of methodological heterogeneity and a lack of standardised outcome reporting across studies, a meta-analysis was not performed. Instead, we used a descriptive approach to compare findings across these technique groups. When available, statistical significance values were recorded as reported in the source articles. To control for subjectivity, only quantitative or explicitly stated clinical outcomes from peer-reviewed sources were included. This study did not involve original data collection or patient contact, so Institutional Review Board approval and informed consent were not applicable.
No laboratory equipment or experimental reagents were used in this review. Apparatuses referenced in the reviewed studies, such as ultrasound devices and piezoelectric surgical tools, were standard clinical instruments, though manufacturer information was not consistently reported across publications and is therefore not detailed here.
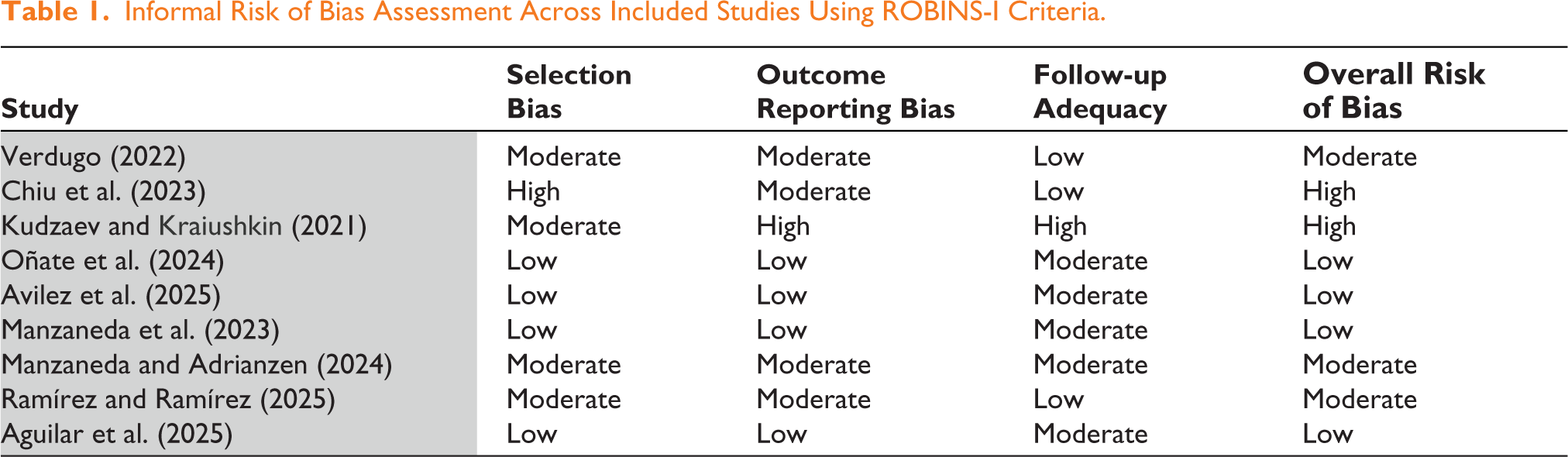
The risk of bias was informally assessed across included studies, focusing on selection bias, outcome reporting bias, and follow-up adequacy (Table 1). The evaluation was guided by the ROBINS-I framework; 3 however, a formal scoring tool was not used, given the predominantly descriptive design of many included studies. Studies by Oñate, Avilez, and Aguilar demonstrated a low overall risk of bias due to clear methodology, comprehensive reporting, and adequate follow-up.6,8–9 In contrast, earlier or smaller case series, such as those by Chiu and Kudzaev, exhibited a higher risk due to limited sample sizes and less detailed outcome tracking.5,7 Most studies relied on retrospective designs and self-reported satisfaction without blinding, introducing a moderate risk in patient-reported outcomes. Despite these limitations, the available evidence offers valuable insight into comparative effectiveness and safety across rib remodelling techniques.
Informal Risk of Bias Assessment Across Included Studies Using ROBINS-I Criteria.
Results
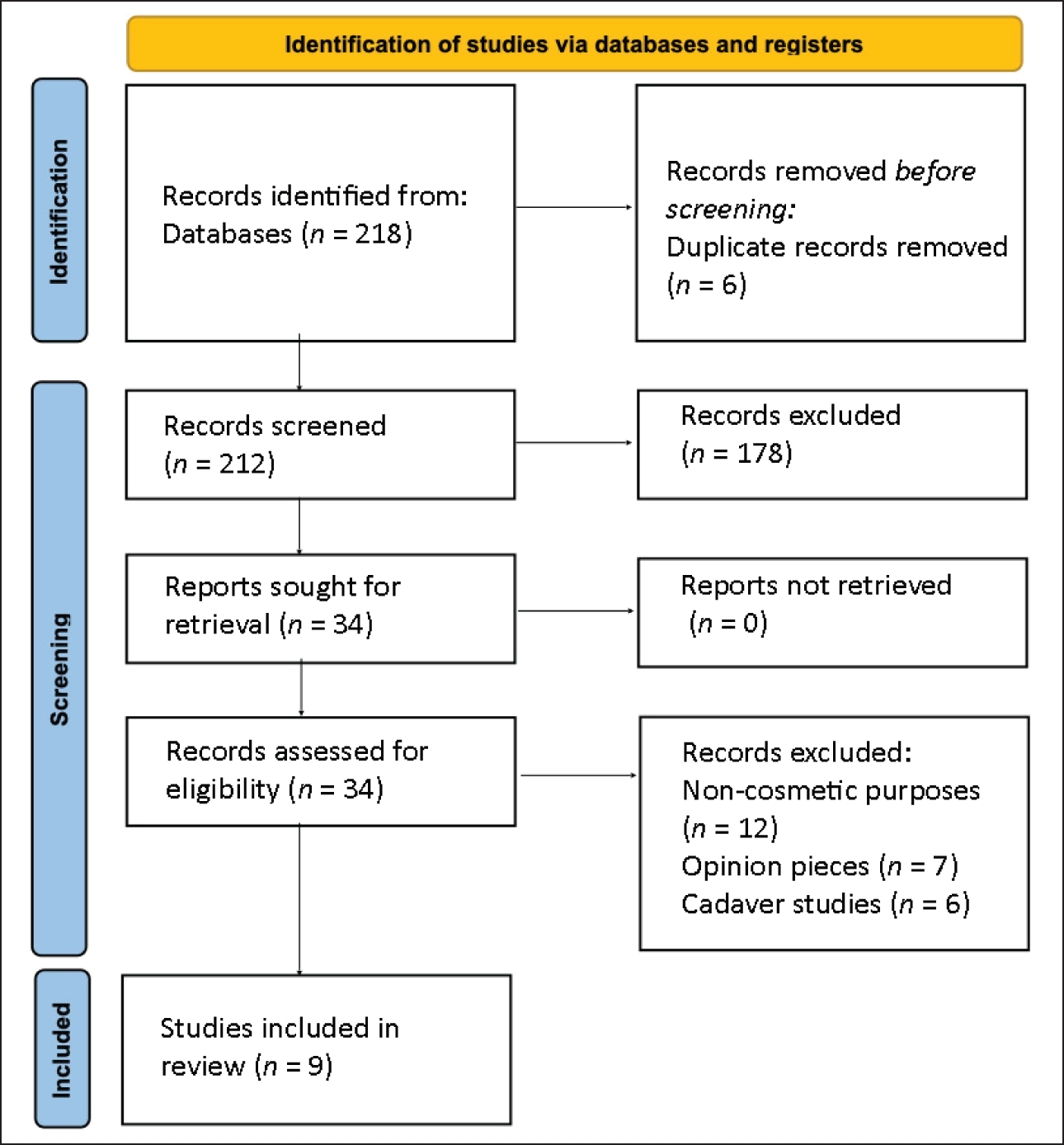
A total of nine studies met the inclusion criteria and were analysed in this review, as shown in the PRISMA flow diagram (Figure 1). These included prospective and retrospective case series published between 2015 and 2025, with sample sizes ranging from 5 to 220 patients. The techniques reviewed varied in invasiveness and methodology, allowing for comparative analysis across approaches. While differences in study design and outcome measures limit direct comparison, the available data provide a useful overview of clinical trends, effectiveness, and safety profiles for each rib remodelling technique.
PRISMA 2020 Flow Diagram for New Systematic Reviews, Which Included Searches of Databases and Registers. 2
Traditional Rib Resection (Floating Rib Removal)
Technique
Traditional rib resection involves surgically excising the 11th and 12th ribs (the ‘floating’ ribs) to reduce the lower ribcage circumference. Often, this is performed in conjunction with liposuction and/or abdominoplasty to maximise waist narrowing. 4 The procedure permanently removes the bony support at the waistline, allowing the sides of the waist to ‘collapse’ inward slightly, thereby decreasing waist girth.
Clinical Evidence
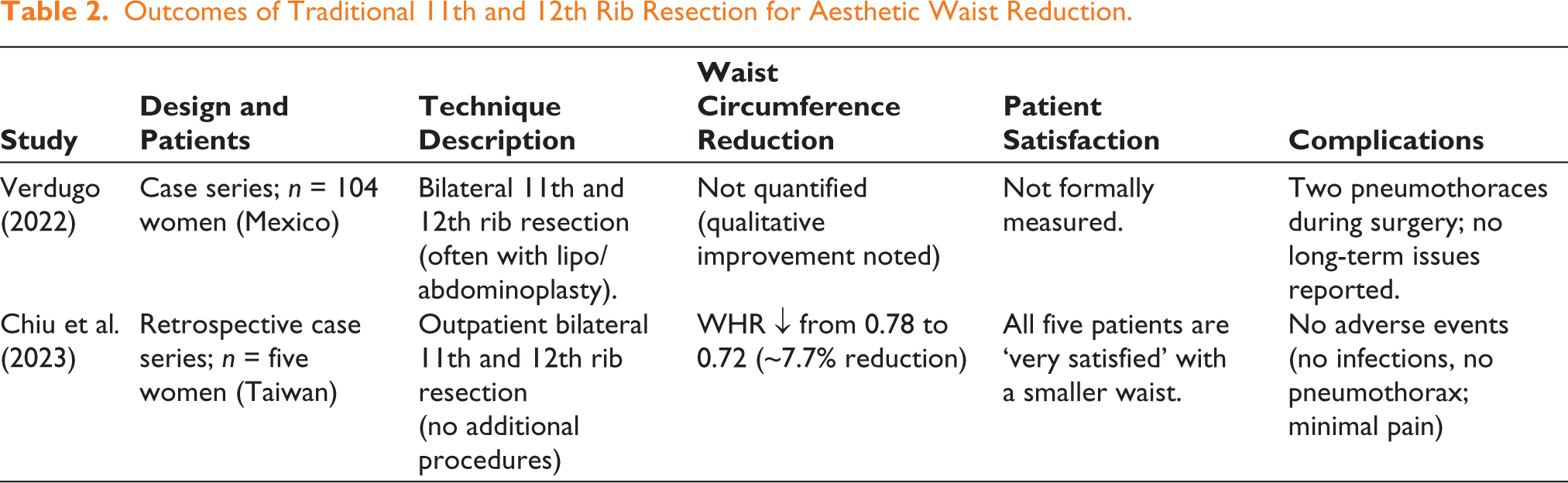
Published reports on cosmetic rib removal are limited but growing. A large case series by Verdugo reviewed 104 women over eight years who underwent cosmetic resection of ribs 11 and 12. 4 Most of these patients also had concurrent body contouring procedures (liposuction and/or tummy tuck), with only 10 patients undergoing isolated rib removal. Two intraoperative pneumothoraces were the only major complications reported in the 104 cases. The author described the rib removal technique as ‘not gory’ and having a low complication rate. While specific quantitative waist reductions were not detailed in the abstract, the procedure was indicated for patients who could not achieve their desired waist slimness through conventional surgery alone. Overall, Verdugo concluded that elective resection of the 11th/12th ribs is a safe adjunct for waist contouring when performed carefully.
Another report by Chiu et al. in Taiwan documented ‘anterior waist’ surgery, referring to cosmetic floating rib removal. 5 They retrospectively analysed five female patients who underwent outpatient bilateral resection of ribs 11 and 12 without other concurrent procedures. The mean waist-to-hip ratio in these patients improved from 0.78 pre-op to 0.72 post-op (a 7.7% reduction in the ratio). In practical terms, this corresponded to notable waist circumference reduction (exact waist cm change not explicitly reported, but the Waist-to-hip ratio (WHR) change implies a substantially smaller waist). Importantly, no adverse events were observed in this series, and all five patients reported being satisfied with their results. The authors highlighted that floating rib resection can effectively decrease waist size with a straightforward, reproducible technique and minimal complications. They dubbed the dramatic waist reduction the ‘ant waist’ effect and called for further studies, given the preliminary but positive outcomes.
Outcomes and Safety
These early clinical reports suggest that removing the 11th and 12th ribs can achieve waist circumference reductions on the order of several centimetres with high patient satisfaction and relatively low complication rates. Patients are often able to go home the same day and resume daily activities quickly. 5 The primary risks of rib resection are injury to underlying structures (pleura/lungs leading to pneumothorax, bleeding, etc.), but in experienced hands, these events appear infrequent.4,5 Table 2 summarises the key findings from the above studies on traditional rib resection.
Outcomes of Traditional 11th and 12th Rib Resection for Aesthetic Waist Reduction.
Rib Repositioning Techniques
Technique
Rib repositioning refers to methods that alter the orientation of the lower ribs without fully removing them. Typically, the surgeon performs an osteotomy on ribs 11 and 12 (and sometimes the 10th) and then repositions or pushes the rib segments inward to narrow the waist. The ribs may be stabilised in their new position using plates or other fixation (osteosynthesis) 6 or occasionally by suturing to other structures. This approach aims to achieve a permanent inward bend of the rib cage while maintaining the protective function of the ribs.
Clinical Evidence
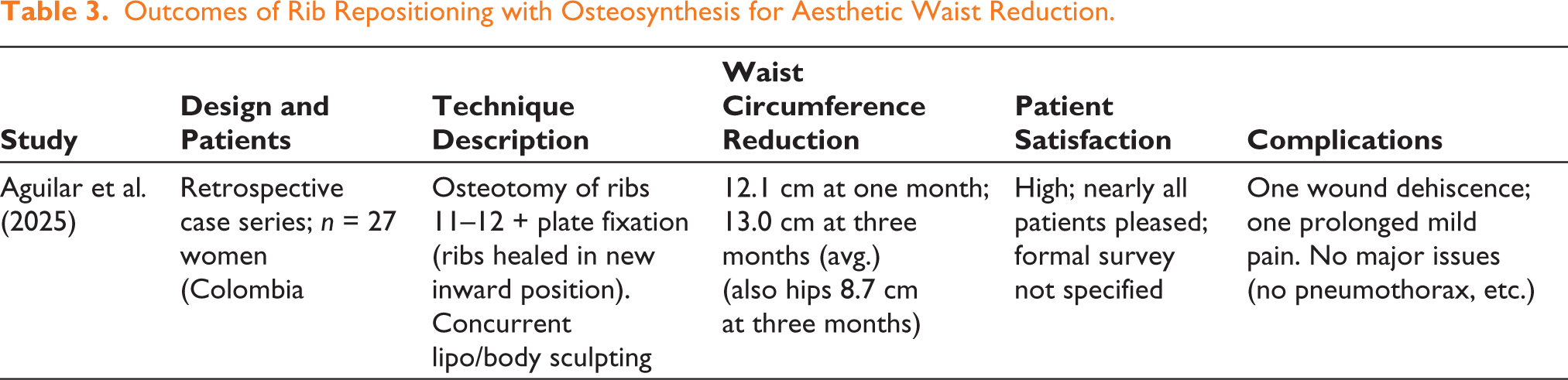
A recent study by Aguilar et al. described an osteotomy with osteosynthetic technique for aesthetic ribcage remodelling. 6 This was a retrospective analysis of 27 patients who underwent waist narrowing surgery between late 2022 and mid-2023. In this technique, the 11th and 12th ribs were cut (osteotomised) and then fixed in a more medial (inward) position using small plates and screws, allowing the ribs to heal in the new configuration (thus effectively ‘repositioning’ the ribs rather than removing them). The outcomes at 1 and 3 months post-op showed a significant waist circumference reduction: On average, 12.1 cm at one month and 13.0 cm at three months. This degree of waist reduction is quite substantial. Patients reported a high satisfaction rate with the procedure (specific survey not detailed, but qualitatively very positive). In terms of safety, only minimal complications were observed in the 27 patients: One case of minor wound dehiscence and one case of prolonged mild pain; no serious complications were reported. Pain scores dropped quickly (average pain 2.4/10 at week one, and 0.26/10 by one month), suggesting a manageable recovery. The authors concluded that rib osteotomy with internal stabilisation is an ‘innovative, safe, and reliable’ method for waist narrowing, yielding dramatic results without significant risk.
Outcomes and Safety
The rib repositioning technique with osteosynthesis described by Aguilar et al. demonstrated substantial reductions in waist circumference, with average measurements decreasing from 80.8 cm preoperatively to 68.8 cm at one month and 67.8 cm at three months post-op (P < .0001). Hip circumference also declined significantly, from 102.6 cm to 93.8 cm at three months, suggesting an overall contouring effect. Among the 27 patients, postoperative pain was minimal, with mean pain scores dropping from 2.4 at week one to 0.26 by the first month. Only two complications were reported: A case of minor wound dehiscence and another of moderate pain requiring additional NSAIDs, both resolving with conservative treatment. No respiratory or functional impairments occurred. Of the 24 patients who completed the Body-Quality of Life (QoL) questionnaire, all reported high to very high satisfaction, with a mean total score of 89.5 (95% CI, 85.6–93.4). Individual domain scores were similarly high, particularly for self-perception and social confidence. These findings indicate that rib repositioning with internal fixation is both effective and safe when performed in appropriate candidates, yielding dramatic waist contouring with minimal risk. Table 3 summarises the key outcomes of the rib repositioning approach with osteosynthesis.
Outcomes of Rib Repositioning with Osteosynthesis for Aesthetic Waist Reduction.
Kudzaev’s Dorsal Osteotomy (‘Greenstick’ Rib Fracture)
Technique
Dr Kazbek Kudzaev’s method, first described in literature in 2021, involves creating a partial-thickness break in the posterior (dorsal) part of the lower ribs rather than removing the ribs entirely. 7 Small incisions (~1 cm) are made along the back (near the scapular line). Using either an oscillating saw or a piezoelectric cutting tool, the outer cortex of ribs 11 and 12 is osteotomised (cut) while leaving the inner cortex intact. The surgeon then gently applies pressure to fracture the rib in a controlled ‘greenstick’ manner, allowing the rib to bend inward but remain in one piece. The fractures are left to heal in this inward-bent position. No hardware is used; instead, the patient wears a tight corset for ~two months post-op to support the chest and maintain the desired contour until the bones consolidate. Kudzaev intended to offer a less aggressive alternative to rib removal, preserving rib function while avoiding large scars and reducing risk to internal organs. This method is sometimes termed ‘corset waistplasty’ due to the required postoperative corset.
Clinical Evidence
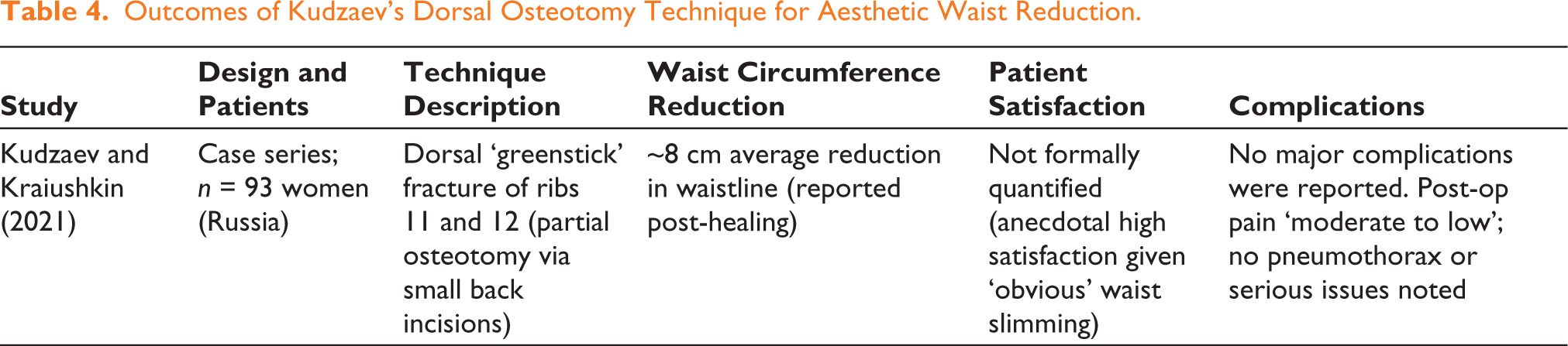
Kudzaev and Kraiushkin published their case series in 2021, reporting on 93 women (ages 19–43) who underwent this dorsal osteotomy technique for waist narrowing. 7 Of these, 14 patients had a follow-up of six months or more (others presumably had shorter follow-ups). They reported an average waistline reduction of approximately 8.0 cm following the procedure. Importantly, the authors emphasise that the method is relatively atraumatic with a short recovery and that it achieved an ‘obvious clinical effect’ on waist contour. They noted that all patients selected were healthy and highly motivated, and those with obesity (BMI >25) or significant medical issues were excluded to minimise risks.
Outcomes and Safety
Among 93 patients treated with Kudzaev’s dorsal osteotomy technique between 2018 and 2020, follow-up data were available for 14 patients at six months or longer. In this group, the average waist reduction was 8.0 cm, ranging from 4 to 15 cm. Patient satisfaction was generally high, although three individuals described their results as ‘a bit lower than expected’. Interestingly, satisfaction did not correlate directly with the magnitude of waist reduction. An earlier follow-up at 2–2.5 months in 48 patients confirmed visible improvement, though long-term outcomes were deemed inconclusive at that stage due to the effects of corset removal and other variables such as diet. Three patients required revision surgery due to inadequate initial results, all of whom had been noncompliant with postoperative corset use. No major complications were reported, and postoperative discomfort was described as moderate to low. Overall, the technique appears to be safe and effective in producing meaningful waist narrowing when adherence to postoperative protocols is maintained. This technique laid the groundwork for several subsequent innovations by other surgeons. Table 4 summarises the key outcomes of Kudzaev’s dorsal osteotomy technique.
Outcomes of Kudzaev’s Dorsal Osteotomy Technique for Aesthetic Waist Reduction.
Greenstick Osteotomy Remodelling with Modern Variations
Building on Kudzaev’s rib-preserving concept, 7 other surgeons have adopted greenstick rib osteotomy techniques and enhanced them with modern technology. The core idea remains the same: Fracture the lower ribs in a controlled fashion and use external compression (corsets or binders) to guide healing, but recent variations utilise ultrasound imaging and ultrasonic cutting tools to improve precision.
Ultrasound-assisted Rib Fracture (Oñate et al., 2024)
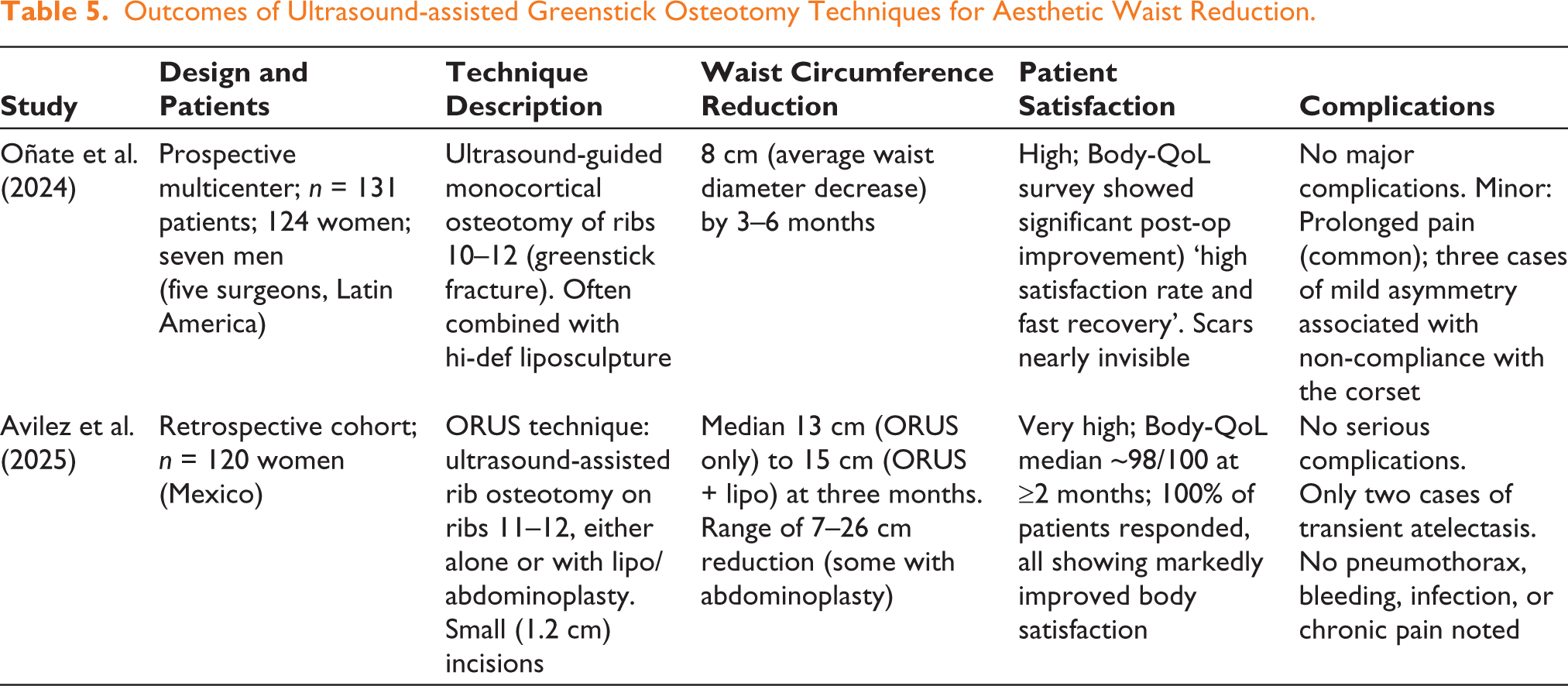
Oñate et al. introduced an ultrasound-guided method to perform greenstick fractures of the ribs for waist narrowing. In a prospective multicenter study, five surgeons treated 131 patients (95% female) using a standardised technique. Under real-time ultrasound imaging, an ultrasonic bone scalpel (or sometimes a specialised manual saw) was used to perform a monocortical costal corticotomy on the last two or three ribs (typically ribs 10, 11, ±12). Essentially, this reproduces Kudzaev’s method but with ultrasound guidance to avoid damage and an ultrasonic tip to precisely weaken the bone. After inducing greenstick fractures, patients wore a compressive corset garment to ensure proper inward healing. The results at follow-up showed a mean waist diameter decrease of ~8 cm (statistically significant, P <.05), very much in line with Kudzaev’s 8 cm figure.
Notably, no major complications occurred among the 131 patients. The most common minor issue was prolonged pain in some cases. Only three patients developed slight contour asymmetries of the waist, all of whom had been noncompliant with wearing their corsets consistently. Patients overall had a high satisfaction rate and fast recovery, as measured by a Body-QoL questionnaire administered postoperatively. The Body-QoL survey indicated significant improvements in self-perception and body satisfaction (with P < .0001 on satisfaction scales). The authors emphasise that because the incisions are very small (often <1 cm), scarring is almost invisible, contributing to the positive patient-reported outcomes. They dubbed this approach ‘ultrasonic- and ultrasound-assisted indentation surgery of the thorax’ and consider it safe, with minimal risks when proper technique and postoperative corseting are employed.
ORUS (Ultrasonic Osteomodeling) with Lipo/Abdominoplasty (Avilez et al., 2025)
Another group led by Avilez in Mexico City published results of an approach they call ORUS (Osteo Remodelling with Ultrasound). In their report, a total of 120 patients underwent rib osteotomy for waist contouring, subdivided into those who had rib osteotomy alone versus combined with liposuction or abdominoplasty. The technique is similarly based on controlled fractures of ribs 11 and 12 using ultrasound guidance. All patients were followed for at least three months. The waist circumference reductions were remarkable: Depending on the adjunct procedures, patients lost between 7 and 26 cm in waist circumference, with median losses of 13 cm (ORUS only) and 15 cm (ORUS + liposuction) by three months post-op. Even the lowest quartile of responders had ~7 cm waist loss, while the top end saw >20 cm reduction (especially when combined with abdominoplasty for those who had excess skin). This demonstrates a potentially additive effect of combining rib fracture techniques with traditional body contouring.
No serious complications were encountered in the 120 patients; importantly, there were zero cases of pneumothorax, hemothorax, organ injury, infection, or chronic nerve pain. Only two patients developed transient atelectasis (partial lung collapse) post-op, which was resolved with standard care. Patient-reported outcomes were excellent at ≥2 months post-op, and a validated Body-QoL questionnaire showed median scores ~97 out of 100, indicating patients were very satisfied across multiple domains (appearance, physical symptoms, sexual life, etc.). Every patient in the cohort responded to the survey, and virtually all rated their outcome highly (even the lowest score was 88/100). This study highlights that with proper technique and patient selection, ultrasound-assisted rib osteotomy can safely produce dramatic waist slimming. The required incisions were only ~1.2 cm in length, making the approach attractive to those concerned about scarring. Of note, patients were advised to wear compression garments, and one case was highlighted where a patient continued wearing a corset for comfort up to 18 months post-op, suggesting some patients find ongoing benefit in support (though not strictly required by that time).
In summary, modern greenstick osteotomy techniques, especially when combined with high-definition liposculpture, have demonstrated waist reductions on the order of 8–15 cm on average, with high patient satisfaction and few complications reported.8,9 The need for a postoperative corset or compression is a common theme to ensure even healing. Table 5 compares the clinical outcomes of the two large recent studies using ultrasound-assisted greenstick osteotomy techniques.
Outcomes of Ultrasound-assisted Greenstick Osteotomy Techniques for Aesthetic Waist Reduction.
RibXcar Technique (Ultrasound-guided Fracture Without Incisions)
Technique
RibXcar is a novel, minimally invasive method for waist contouring introduced in the last few years. The name comes from ‘rib X (fracture) with car (short for cortes in Spanish, meaning cuts)’ as described by its developers, and it essentially involves using an ultrasound probe and needle-based tools to fracture the ribs percutaneously. 10 Unlike the other osteotomy methods, which still require small incisions, RibXcar aims for a ‘scarless’ approach by accessing the ribs through tiny punctures (just enough to introduce instruments). 1 The surgeon uses ultrasound imaging to locate the rib and then performs a controlled monocortical fracture (usually on the lateral aspect of the rib) by drilling or punching through one cortex. By not completely breaking the rib in two, the continuity of the rib is maintained, and the partial fracture allows the rib to bend inward. The technique was initially applied to the free-floating ribs (11, 12), but expanding it to ‘false’ ribs (9, 10) required additional manoeuvres due to their attachment to the sternum cartilage. 9 Thus, a ‘false-to-floating’ conversion was devised for ribs 9 and 10: Essentially cutting their anterior cartilaginous attachment so that they behave such as floating ribs before performing RibXcar on them. 10
Clinical Evidence
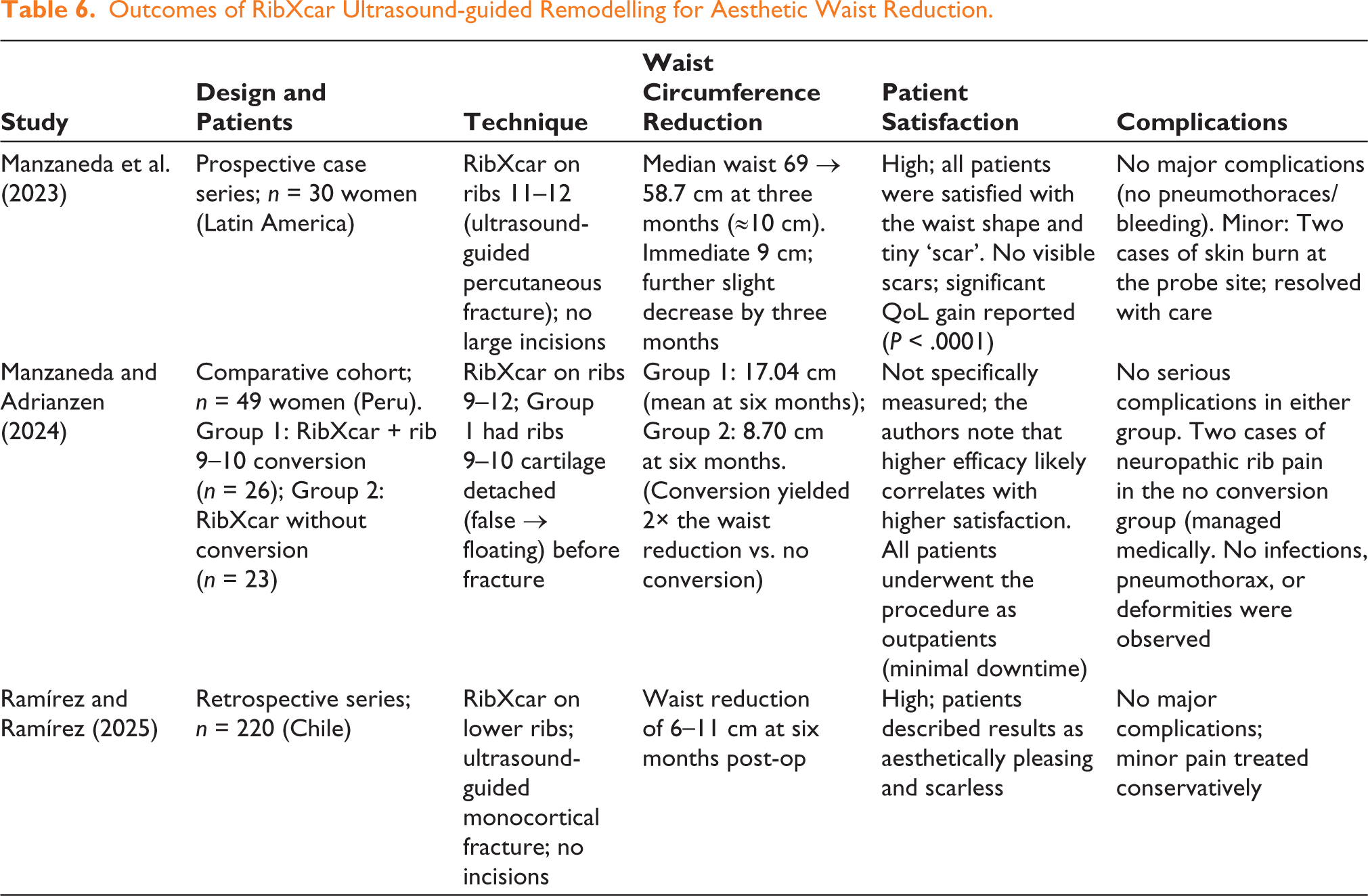
Manzaneda et al. have published a series of studies on RibXcar. In 2023, they reported the outcomes of 30 female patients (ages 18–35) who underwent ultrasound-guided monocortical rib fractures in a ‘scarless’ manner. Three board-certified surgeons in Peru, Colombia, and Mexico performed the procedures, indicating a multi-centre experience. All patients wore a special compressive corset for six months after the procedure. The surgery itself was very quick (mean ~31 minutes). No serious complications occurred; specifically, no pneumothorax, hemothorax, infections, or respiratory issues were seen. Two patients (out of 30) did experience small skin burns at the puncture sites (likely friction or device-related), which were minor and treated conservatively. The waist circumference results were significant: The median waist was 69 cm pre-op and dropped to 60 cm immediately post-op, further to 59 cm at one month, and 58.7 cm at three months. This represents a median reduction of about ~10 cm (≈4 inches) by three months. Ultrasound measurements of rib angles confirmed that the costal angle of each treated rib had decreased (i.e., ribs angled inward more) and that this change was maintained over three months. A simple satisfaction survey at three months found that patients were pleased with both their new waist shape and the virtually invisible puncture scars. Statistical analysis of satisfaction indicated a significant improvement post-procedure (P < .0001). The authors noted that the absence of a scar was a major positive for patients, distinguishing RibXcar from traditional rib surgery.
In 2024, Manzaneda and Adrianzen published a follow-up comparative study focusing on the false-to-floating rib conversion adjunct to RibXcar. They studied 49 women undergoing rib remodelling, split into two cohorts: 26 patients received RibXcar with conversion of ribs 9 and 10 (meaning the costal cartilage of ribs 9 and 10 was surgically detached, turning them into ‘floating’ ribs before fracturing), and 23 patients received RibXcar without conversion on ribs 9 and 10. All patients had ribs 11 and 12 treated as well, but the key difference was whether ribs 9–10 were pre-treated to free them. The rationale was that when ribs 9 and 10 remain anchored to the sternum, there is more resistance to inward movement and risk of suboptimal outcome. The results at six months strongly favoured adding the conversion: The group with conversion achieved a mean of 17.04 cm reduction in waist circumference, compared to 8.70 cm in the group without conversion (P < .05). In other words, patients whose false ribs were freed saw about double the waist slimming effect. The rib angle changes were also greater in the conversion group, confirming a more effective inward bend. Importantly, the enhanced result did not come with increased risk: No severe complications were noted in either group. Across all 49 patients, there were no surgical site infections, no pneumothoraces, and no hemothoraces. Two patients in the non-conversion group experienced neuropathic intercostal pain post-op. These nerve pain cases were successfully managed with medication and resolved within days. Notably, no patients in the conversion group had this issue (possibly because freeing the rib might reduce traction on nerves). The authors conclude that the false-to-floating conversion is a safe and effective complement to RibXcar, yielding significantly greater waist reduction without added complications. They termed the combined approach ‘Xonversion Ribs’ + RibXcar, and advocated its use when treating ribs 9 and 10.
In a large retrospective series by Ramírez and Ramírez (2025), 220 women underwent the RibXcar procedure, either alone or in combination with other body contouring surgeries. The mean patient age was 33.5 years, with an average Body Mass Index (BMI) of 24.3. Among these, 80 patients underwent RibXcar with abdominoplasty, 60 with liposculpture, and 80 had RibXcar alone. Across all cases, preoperative waist circumference averaged 77.9 cm and decreased to 66.2 cm at six months, reflecting a consistent reduction of 6–11 cm. No major complications were reported, and 93% of patients experienced an uneventful postoperative course. Minor issues, such as pain, were treated conservatively. Importantly, no scarring was observed, and the technique was deemed effective in achieving a slimmer waist and smoother transition from waist-to-hip. The study attributes the safety and precision of the procedure to ultrasound guidance and the use of the Manzaneda tool, which allows controlled monocortical rib fractures without large incisions. 11 By avoiding pleural violation and vascular injury, RibXcar demonstrated a strong safety profile in this large cohort, with high patient satisfaction, and favourable aesthetic outcomes.
Outcomes and Safety
Across all three studies, RibXcar produced consistent waist reductions of 6–17 cm, depending on whether rib conversion was performed.1,10–12 Follow-up durations of 3–6 months demonstrated that results were sustained over time. Patient satisfaction was high, driven by both the visual improvement in waist shape and the lack of visible scars. No serious complications such as pneumothorax or infection were reported. The use of ultrasound guidance and the avoidance of full rib disruption appear to contribute to the safety of the technique. Table 6 presents the outcomes of the three clinical studies evaluating the RibXcar ultrasound-guided remodelling technique.
Outcomes of RibXcar Ultrasound-guided Remodelling for Aesthetic Waist Reduction.
Discussion
This systematic review highlights a growing shift in aesthetic body contouring, where rib remodelling has moved beyond experimental practice and become a structured surgical approach for waist narrowing. While traditional floating rib resection remains effective for achieving modest reductions in waist circumference (~5–7 cm), its invasive nature and visible scarring have led many surgeons and patients to seek less disruptive alternatives. 5
Prior systematic reviews, including those by Ferreira et al. and Danilla and González-Arestizábal, offered broad overviews of rib-based procedures for waist narrowing.13,14 However, by analysing diverse approaches collectively, they limited the ability to draw conclusions about individual methods. The present review addresses this gap by categorising rib remodelling procedures into distinct groups and summarising reported outcomes such as waist reduction, patient satisfaction, and complications for each technique. This structure allows for a more focused comparison of reported outcomes and may help identify trends in safety, effectiveness, and patient satisfaction. Given the pace of innovation and the growing demand for these procedures, future research should include prospective designs, consistent outcome measures, and longer follow-up to inform evidence-based surgical planning.
The emergence of dorsal osteotomy techniques, such as Kudzaev’s method, 7 and their evolution into ultrasound-assisted approaches have significantly expanded the repertoire of rib-based contouring procedures. These newer techniques offer reductions ranging from 8 to over 15 cm while maintaining rib integrity and minimising complications.8,9 The adaptation of the piezotome into Manzaneda’s tool, along with the use of ultrasound guidance, represents important technical advancements that enhance surgical precision and contribute to greater safety and improved postoperative outcomes.1,11 Notably, RibXcar and its adaptations, such as the false-to-floating rib conversion, demonstrated some of the largest reductions (up to 17 cm) with high patient satisfaction and negligible scarring, reinforcing the appeal of scarless or minimally invasive techniques.10,12
A consistent theme across all techniques is the importance of postoperative compliance. In procedures that rely on corset-based remodelling, such as dorsal osteotomy or RibXcar, nonadherence significantly affected outcomes and, in some cases, necessitated revision surgery. 7 This emphasises a broader consideration in aesthetic surgery: The success of an intervention is not solely determined intraoperatively but also hinges on patient behaviour during recovery.
Despite the promise shown, the literature remains limited by retrospective designs, small sample sizes in some reports, and short follow-up periods. Many studies relied on patient-reported satisfaction without standardised metrics or blinding, introducing subjectivity and potential reporting bias. While the Body-QoL tool was used in some cohorts to quantify satisfaction and quality-of-life improvements, further validation across larger and more diverse populations is warranted. 9
Within the scope of the current evidence, rib remodelling appears to be a safe and effective adjunct to aesthetic waist contouring when patient selection and postoperative care are optimised. The findings of this review support its continued use and refinement, particularly in minimally invasive formats that balance efficacy with low risk and high patient satisfaction. These findings should be interpreted within the context of the available evidence. While limited by the descriptive nature of the included studies, they support the original aim of this review to clarify reported outcomes across rib remodelling techniques for aesthetic waist contouring.
Conclusion
Rib remodelling has become an increasingly utilised technique in aesthetic surgery, offering additional waist contouring options beyond traditional methods. This review organises reported outcomes by technique, allowing clearer comparison across approaches. While existing studies are limited in size and design, current evidence suggests these procedures can be performed safely with high patient satisfaction. Larger, prospective studies with longer follow-up are needed to strengthen the evidence base and guide clinical practice.
Footnotes
Authors’ Contributions (CRediT Taxonomy)
Yoalkris Elizabeth Salcedo: Conceptualisation, methodology, formal analysis, writing-original draft, visualisation.
Ashley Eliana Soriano-López: Data curation, writing, review, and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Presentation History
This review has not been presented at any scientific meeting to date.