
Abstract
Background and Aim:
Oral lichen planus (OLP) is a chronic inflammatory disease that can show potential for malignant transformation, unlike cutaneous lichen planus (CLP). The exact molecular reasons behind this difference are not well known. This study aimed to evaluate the expression of 3 biomarkers namely MDM2, SOX2, and Ki-67 in OLP and CLP to assess their relationship with cell proliferation and possible malignant potential.
Methods:
This retrospective study was carried out at Sina Hospital in Tabriz, Iran, from April 2022 to June 2023. Fifty paraffin-embedded tissue samples were analyzed, including 25 oral and 25 cutaneous lichen planus cases. Sections were stained immunohistochemically for MDM2, SOX2, and Ki-67. Two pathologists, blinded to patient information, evaluated the slides. Expression was classified as negative, low, or high. Data were analyzed in SPSS version 26 using descriptive statistics and Fisher’s Exact Test, with a P-value ⩽ .05 considered significant.
Results:
In CLP, all samples were negative for Ki-67, while SOX2 and MDM2 were positive at low levels in only 8% of cases. In OLP, Ki-67 was low in 16%, SOX2 in 20%, and MDM2 was high in 40% of samples. A significant correlation among the 3 markers was seen in OLP (P < .001), but not in CLP. SOX2 expression differed significantly between erosive and non-erosive OLP (P = .047).
Conclusion:
OLP, especially its erosive form, shows higher molecular activity compared with CLP. The coordinated expression of MDM2, SOX2, and Ki-67 supports their role in cell proliferation and malignant potential. MDM2, in particular, may serve as an early indicator for identifying OLP cases at higher risk of malignant transformation.
Introduction
Lichen planus (LP) is a chronic immune disorder that causes inflammation of the skin, mucous membranes in the mouth or genitals, and in rare cases of the nails and scalp. Cutaneous lichen planus (CLP) generally manifests as polygonal, purplish, and flat topped papules and plaques. Wickham’s striae are seen on the papules and the most common locations are the wrists, lower back, and ankles. 1
Clinically, oral lichen planus (OLP) is usually characterized by bilateral or symmetrical white lesions affecting the oral mucosa, gingiva, and tongue, although some patients may present with erythema, blisters, or ulcers. 2 Both variants share a lichenoid histological pattern marked by a band-like lymphocytic infiltrate and basal keratinocyte degeneration. 3
OLP is most commonly diagnosed in individuals over 50 years of age and occurs more frequently in female patients, with an increasing incidence after 40 years of age. 4 Overall, OLP is one of the most common forms of oral mucosal disease, affecting an estimated 0.5% to 2% of the global population. 5
On the other hand, CLP has low prevalence, in the range of 0.2% to 1% of the adult population and is usually self-limiting and can resolve on its own in 6 to 12 months. However, in some cases, it can persist or recur, especially in the case of hypertrophic or subtypes that are atypical. 6 CLP does not show a significant preference for any gender and cases can be seen in younger age groups. 7
The exact etiology of LP remains incompletely understood, but evidence strongly supports a cell-mediated autoimmune mechanism. Tissue damage is predominantly mediated by cytotoxic CD8+ T lymphocytes inducing apoptosis of basal keratinocytes in the oral epithelium.8,9 OLP is therefore classified by the World Health Organization (WHO) as a potentially malignant oral disorder. 5 By contrast, malignant transformation in CLP is rare but has been documented, particularly in hypertrophic and ulcerative skin variants. 10
At the molecular level, LP lesions demonstrate dysregulation of key pathways involved in cell proliferation, apoptosis, immune signaling, and epithelial homeostasis. 11
Although OLP and CLP have comparable histopathological features, they are different regarding environmental triggers and clinical behavior. Potential risk factors for malignant transformation associated with OLP include atrophy/erosion, and chronic mucosal exposure to tobacco, alcohol, mechanical trauma, and microbes.2,12 CLP, on the other hand, is believed to be primarily an immune phenomenon in the skin with some reports showing improvement with UV exposure.5,11 UV radiation impacts skin through both immunosuppressive and pro-apoptotic effects. This happens through the modification of T-cell responses and the keratinocyte p53 pathways. This immunosuppression may partially explain the skin lesions of lichen planus having a lower proliferative activity compared to the lesions in the mucosa.13-15
SOX family transcription factors play important roles in tumor initiation and cancer progression. Increasing evidence suggests that SOX proteins contribute to immune escape by downregulating tumor antigen presentation, modifying immunosuppressive cell populations, and regulating immune checkpoint protein expression on tumor cells. SOX2 overexpression promotes programed death ligand 1 (PD-L1) expression on tumor cells, thereby facilitating immune evasion. Additionally, SOX2 may promote a more immunosuppressive tumor microenvironment through the recruitment and activation of regulatory T cells.16,17
Ki-67 is a well-established marker of cellular proliferation, expressed during the active phases of the cell cycle (G1–M) but absent in the resting phase (G0). 18 Ki-67 expression is largely confined to the parabasal cell layer of the epithelium, with elevated levels indicating increased proliferative activity. Numerous studies have examined Ki-67 expression in premalignant and malignant oral lesions.19,20 For example, Harbeck et al 21 reported that patients with tumors exhibiting high Ki-67 expression (⩾20%) were more likely to experience disease recurrence within 2 years compared with those showing low Ki-67 expression. Accordingly, Ki-67 serves as a marker of proliferation and a widely used prognostic indicator.
Moreover, p53 is a key regulator of apoptosis and the cell cycle, and its inactivation facilitates uncontrolled cellular proliferation and tumorigenesis. Mouse double minute 2 homolog (MDM2), an E3 ubiquitin ligase, promotes the proteasomal degradation of p53, thereby attenuating its tumor-suppressive function. 2
In oral lichenoid lesions (OLL), high Ki-67 expression (12.5%) in the basal, parabasal, and spinous epithelial layers, as well as in subepithelial lymphocytic infiltrates, has been observed in cases with severe oral epithelial dysplasia (OED). 22 Overall, erosive OLP cases exhibiting marked OED demonstrate higher Ki-67 expression, reflecting increased proliferative activity and greater dysplasia severity, as well as an elevated risk of malignant transformation. 22 Furthermore, Islam et al 23 reported co-expression of SOX2 and OCT4 in lichenoid lesions and leukoplakia, supporting their classification as precancerous conditions. MDM2 has also been shown to be upregulated in both OLP and oral squamous cell carcinoma (OSCC) compared with controls.
In CLP, Ki-67 is consistently expressed in lesional epidermis, reflecting a proliferative response to chronic inflammation; however, its expression does not reliably distinguish CLP from other proliferative dermatoses, such as mycosis fungoides. Moreover, elevated Ki-67 indices in cutaneous lesions have not been consistently associated with malignant transformation. 24 The roles of MDM2 and SOX2 in CLP remain underexplored.
The objective of this study is to assess the expression of Ki-67, SOX2, and MDM2 in OLP and CLP and to evaluate their potential roles as markers of cellular proliferation and prognostic indicators of malignant transformation.
Material and Methods
Study Design and Setting
This retrospective cross-sectional analytical study was conducted at the Department of Pathology, Sina Hospital, Tabriz, Iran, between April 2022 and June 2023. The primary aim was to assess the levels of 3 proteins—MDM2, SOX2, and Ki-67—in patients diagnosed with lichen planus.
Participants, Sample Collection, and Histopathological Confirmation
Archived paraffin-embedded biopsy specimens from adults aged 18 to 60 years with a histopathological diagnosis of lichen planus, collected between April 2022 and June 2023, were retrospectively analyzed. A total of 50 samples were included, comprising 25 cases of CLP and 25 cases of OLP. Among the oral cases, 8 were classified as erosive and 17 as non-erosive OLP. Specimens were selected by simple random sampling from pathology archives. All slides were re-evaluated prior to immunohistochemical analysis. The diagnosis of lichen planus was confirmed by the presence of hyperkeratosis, saw-tooth rete ridges, basal cell degeneration, and a dense band-like subepithelial lymphocytic infiltrate. Erosive OLP was defined by epithelial ulceration or epithelial atrophy with surface fibrin deposition and inflammatory exudate, whereas non-erosive OLP showed intact epithelium without ulceration. Inclusion criteria were age between 18 and 60 years and a confirmed histopathological diagnosis of lichen planus. Cases with a history of malignancy or evidence of epithelial dysplasia in the examined specimen were excluded.
Immunohistochemistry and Tissue Processing
The tissue samples were sectioned into thin slices (4 microns thick) and placed onto slides. The slides were dried at 60°C overnight, paraffin was removed, and the tissue was rehydrated. To facilitate protein detection, the slides were heated in a citrate buffer at 95°C for 20 minutes. To prevent natural enzyme activity from affecting the results, we treated the slides with 3% hydrogen peroxide for 10 minutes. Afterward, we added primary antibodies for MDM2, SOX2, and Ki-67, following the manufacturer’s protocol. Following a washing step, secondary antibodies were applied, and chromogen was used to develop the staining. Finally, hematoxylin was used as a counterstain to enhance visualization.
Microscopic Evaluation
All slides were examined under light microscopy at ×40 magnification by 2 independent pathologists blinded to clinical data. No digital image analysis software or artificial intelligence–based tools were used.
Ki-67 expression was assessed by counting nuclear staining in 100 epithelial cells per high-power field. Samples with <50% positive nuclei were classified as low expression, while those with ⩾50% positive nuclei were considered high expression.
SOX2 nuclear staining was evaluated across multiple high-power fields using a combined extent and intensity scoring system. Extent was scored as 0 (<5%), 1 (5%-25%), 2 (25%-50%), 3 (50%-75%), and 4 (>75%). Intensity was graded as weak (1), moderate (2), or strong (3). The sum of extent and intensity scores was used to categorize expression as low (0-3) or high.4-7
MDM2 expression was determined based on the percentage of positively stained nuclei and graded as + (1%-25%), ++ (25%-50%), or +++ (>50%). For statistical analysis, + cases were considered low expression, whereas ++ and +++ were classified as high expression.
Data Analysis
Data were analyzed using SPSS version 26. Descriptive statistics (frequency, percentage, mean, standard deviation) were calculated. Fisher’s exact test and linear-by-linear association were used for comparison of categorical and ordinal variables. Comparisons were performed between CLP and OLP overall, and separately between erosive and non-erosive OLP subtypes. A P-value < .05 was considered statistically significant. Due to limited sample size, multivariate regression analysis was not performed.
Ethical Considerations
This study was approved by the Ethics Committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1401.322, approved 24/07/1401). As this was a retrospective study on archived specimens with no patient identifiers, informed consent was not needed.
Results
Statistical Analysis
We used straightforward stats like frequencies and percentages to give an overview of the data. In order to find out whether there were any correlations between the levels of the biomarkers, we used Fisher’s Exact Test. If the P-value was ⩽.05, then we considered the finding to be significant. We performed all the analysis on SPSS software.
Objective 1: Biomarker Levels in Skin Lichen Planus
According to Table 1 and Figure 1, no trace of Ki-67 was found in any of the 25 skin samples. Also, most of the samples (92%) did not exhibit very low or no SOX2 and MDM2 at all, but only a fraction of them (8%) showed trace of these markers. No marker was found at high levels, meaning the skin lesions overall were very low in cell proliferation and molecular activity.
Expression Levels of SOX2, MDM2, and Ki-67 in Tissue Samples of Patients With Cutaneous Lichen Planus.


Expression levels of SOX2, MDM, and Ki-67 in tissue samples of patients with cutaneous lichen planus.
Objective 2: Biomarker Levels in Oral Lichen Planus
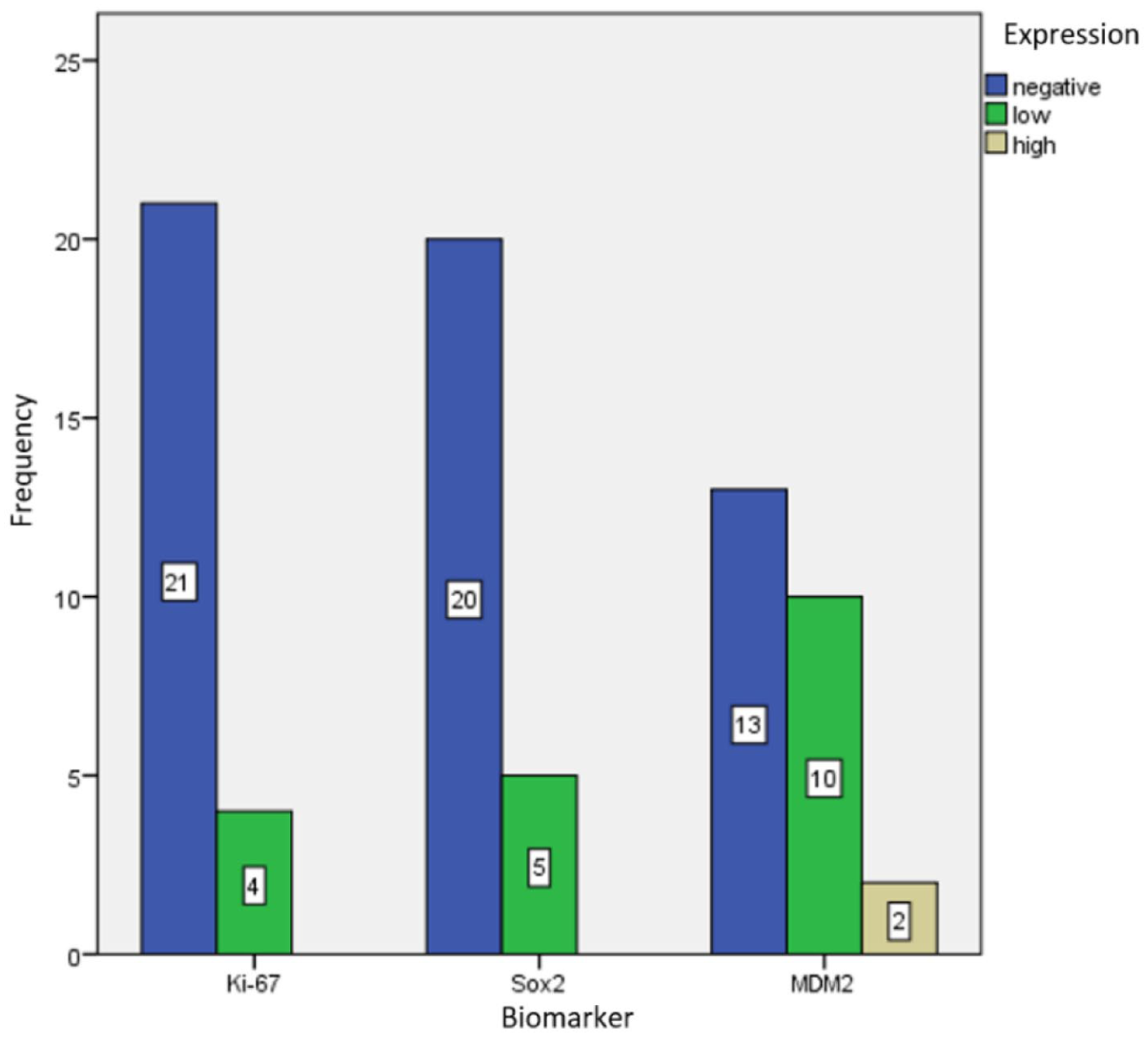
We found a distinct pattern when analyzing the oral tissue samples, as shown in Table 2 and Figure 2. For Ki-67, expression was mostly negative (84%) and low in the remaining samples (16%). For SOX2, 80% of samples were negative, while 20% showed low expression of this biomarker. In contrast, a notable proportion of samples were positive for MDM2 expression (40%), whereas 52% were negative and 8% showed low expression. Representative immunohistochemical staining patterns of Ki-67, SOX2, and MDM2 in OLP are shown in Figure 3.
Expression Levels of SOX2, MDM2, and Ki-67 in Mucosal Tissue Samples of Patients With Oral Lichen Planus.

Expression levels of SOX2, MDM2, and Ki-67 in mucosal tissue samples of patients with oral lichen planus.

Immunohistochemical staining patterns of Ki-67, MDM2, and SOX2 in LP: (A) Ki-67 showing basal layer nuclear expression, (B) Ki-67 demonstrating low nuclear expression (<50% positive nuclei among 100 counted cells at high-power field), (C) MDM2 with low nuclear expression (+, 1%-25% positive nuclei), (D) MDM2 with high nuclear expression (++/+++, >25% positive nuclei), and (E) SOX2 showing nuclear expression in epithelial cells.
Objective 3: Comparison of Erosive Versus Non-Erosive Oral Lichen Planus
Our observation showed that erosive and non-erosive subtypes were significantly different in terms of SOX2 expression level, as shown in Table 3 (P = .047). While none of the samples for both subtypes were positive for SOX2, the majority of non-erosive subtype samples were negative for this biomarker (87%) compared with only 20% of negative cases of erosive subtype samples. Ki-67 and MDM2 expression levels varied between groups but variations weren’t statistically significant.
Expression Levels of MDM2, SOX2, and Ki-67 in Non-Erosive and Erosive Types of Oral Lichen Planus.

Fisher’s Exact Test (Linear-by-Linear Association).
Objective 4: Correlations in Skin Tissue
There was no direct correlation between the expression levels of of Ki-67, SOX2, and MDM2 in the skin samples (Table 4). They seem to be independent of each other in these lesions.
Summary of the Results Assessing the Correlation Between the Expression Levels of MDM2, SOX2, and Ki-67 in Cutaneous Lichen Planus.

Fisher’s Exact Test (Linear-by-Linear Association).
Objective 5: Oral Tissue Correlations
There were significant differences, however, between the expression of the 3 markers in oral tissue samples (P < .001). The concentrations of MDM2 were significantly higher than SOX2 and Ki-67, and SOX2 were higher than Ki-67 as well (Table 5).
Summary of the Results Assessing the Correlation Between the Expression Levels of MDM2, SOX2, and Ki-67 in Oral Tissue Samples of Patients With Oral Lichen Planus.
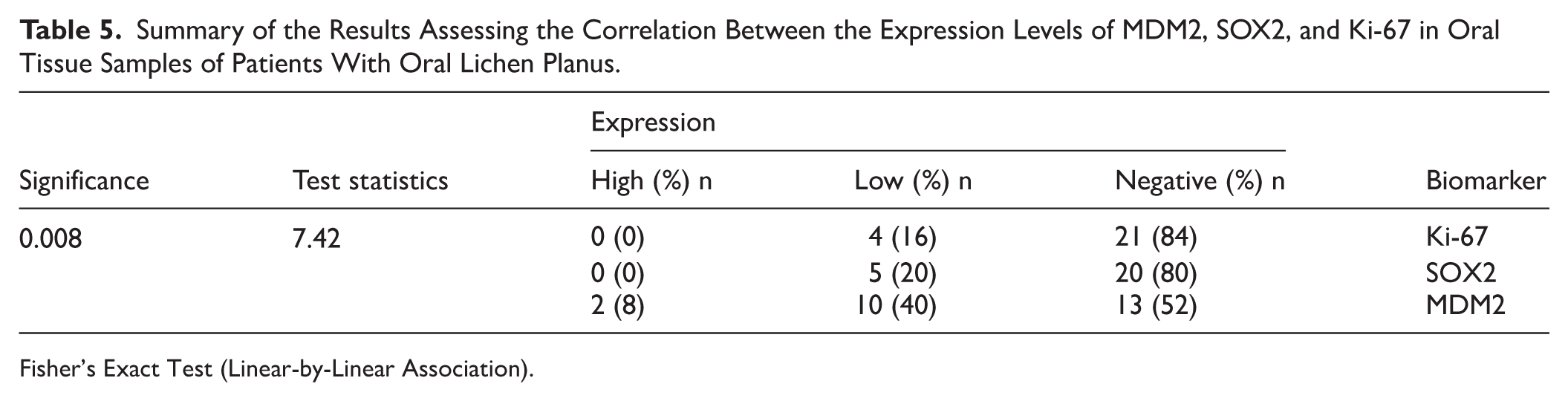
Fisher’s Exact Test (Linear-by-Linear Association).
Objective 6: Skin Versus Oral Lesions
Direct comparison of oral and skin lesions did not exhibit statistically significant differences in the levels of expression for Ki-67, SOX2, or MDM2 (Tables 6-8). It is important to note that while increased MDM2 appeared in oral lesions in 40% of cases, none of the cutaneous cases were positive for this biomarker.
Comparison of Ki-67 Levels in Cutaneous and Oral Lichen Planus.

Comparison of SOX2 Expression Levels in Cutaneous and Oral Lichen Planus.

Comparison of MDM2 Expression Levels in Cutaneous and Oral Lichen Planus.

Figure 2 Expression levels of MDM2, SOX2, and Ki-67 in tissue samples of patients with CLP. The majority of CLP specimens show negative expression for all 3 biomarkers, with few samples exhibiting low-level SOX2 and MDM2 expression, indicating low proliferative and molecular activity in skin lesions.
Figure 2 Expression levels of MDM2, SOX2, and Ki-67 in tissue samples of patients with OLP. OLP samples showed higher biomarker expression than CLP, suggesting proliferative and malignant activity in oral mucosal lesions
Discussion
OLP is a long-standing inflammatory disorder with well-documented risk of malignant change, 2 which distinguishes it clinically from cutaneous LP (CLP). This study compared the expression of 3 critical biomarkers—MDM2, SOX2, and Ki-67—to find how they correlated with OLP pathogenesis and malignancy. According to our results, OLP exhibits a more dynamic molecular microenvironment than CLP, given that all 3 biomarkers were expressed in this pathology, specifically erosive subtypes. This distinctive expression pattern in OLP lesions suggests linked pathogenic pathways to disease progression.
The most striking result was the pronounced molecular distinction between OLP and CLP. While the majority of CLP specimens were shown to have molecular quiescence and negative biomarker expression, OLP lesions had evidence of active biomarker activity. Notably, 48% of OLP cases were positive for MDM2 (40% Low + 8% High), 16% were low Ki-67 positive, and 20% were low SOX2 positive. This molecular dichotomy implicates that OLP is a distinct pathological entity from CLP based on proliferative and neoplastic processes confirming its status as a potentially malignant disorder. 12
Our Ki-67 findings must be considered with caution. Although our results reflect a numerical distinction in Ki-67 expression between OLP and CLP (16% vs 0%), this difference was not statistically significant (P = .569). Scientific literature is contradictory regarding Ki-67 in OLP. Mutafchieva et al did not show any significant distinction in Ki-67 expression between OLP and normal oral mucosa. 25 However, the highest quality evidence currently on hand, on the basis of systematic review and meta-analysis by Bahramian et al with 593 patients and 12 studies, provides significant clarification: Ki-67 expression in OLP is considerably lower than that of oral epithelial dysplasia (Odds Ratio = 0.297, P < .001). However, it is still elevated compared to normal mucosal homeostasis. 26
The pro-oncogenic molecular signature that we discovered is in agreement with a major systematic review. This systematic review of over 7000 OLP samples reiterated that OLP epithelium consistently exhibits characteristics of cancer hallmarks, including permanent proliferative signaling and apoptosis resistance, induced by an inflammatory tumor-supportive environment. 27 The large body of evidence supports our interpretation that the molecular alterations observed constitute a true pathogenic deviation toward malignancy.
This molecular distinction gains further support from recent large-scale genetic evidence. 22 Of particular note, a population study that excluded leukoplakia patients demonstrated a 13.6-fold increased risk of tongue cancer in OLP patients (Odds Ratio = 13.6; 95% CI: 9.6-19.3). 6 This data provides epidemiologic evidence for our molecular findings and recognizes OLP as a clinically relevant precancerous condition.
Within OLP, there was an evident molecular risk gradient between subtypes. Erosive OLP demonstrated the highest dysregulated biomarker profile, as revealed by detectable levels of Ki-67 and SOX2 and significantly elevated MDM2 expression. The increased frequency of SOX2 expression in the erosive type of OLP, although low, is consistent with findings by Zisis et al 28 that SOX2 was still present in this variant. Zisis et al29,30 also reported nuclear SOX2 expression within the basal and parabasal epithelial layers of potentially malignant oral lesions, and this expression was reported to increase progressively from non-dysplastic lesions to dysplasia and well differentiated oral squamous cell carcinoma. This progressive increase suggests that SOX2 is activated quite early during the process of oral carcinogenesis and is associated with the degree of epithelial dysplasia. In addition, SOX2 expression has also been reported in the endothelium of dysplastic lesions and OSCC which suggests that SOX2 may have a role in the microvascular remodeling and the progression of the lesions. The role of SOX2 as a potential biomarker for oral carcinogenesis is supported by its role in OSCC. SOX2 protein expression was found to be significantly higher in larger tumor sizes, lymph node metastasis and was an independent predictor of poorer survival in OSCC patients according to Ghazaghi et al. 24 Therefore, the increase of SOX2 expression in erosive OLP is a biomarker of inflammation and a greater potential for malignancy and is not simply a reactive epithelial response.
Furthermore, they also suggest future research on the co-expression patterns of SOX2 with other SOX family members
MDM2 was one of the most important biomarkers in our investigation. Its proven role as an E3 ubiquitin ligase that degrades the tumor suppressor p53 via the proteasome places it at the center of cell cycle regulation and apoptosis. 31 The significant MDM2 expression in erosive OLP indicates potential disruption of p53-mediated tumor surveillance, an established oncogenic process. This finding is in agreement with Jana et al, who demonstrated significantly increased p53 and p21 expression in dysplastic OLP compared with nondysplastic lesions and concluded increased cellular stress and malignant potential. 32 The concurrent expression of both p53 and its regulator MDM2 may represent a marker for disordered tumor suppressor control, potentially enabling survival of genetically altered keratinocytes and thus increasing the risk of malignant transformation. Thus, MDM2 can be considered as a more sensitive indicator of malignancy potential in OLP than proliferation markers such as Ki-67.
The significant association among MDM2, SOX2, and Ki-67 expression patterns specifically in OLP suggests potential synergistic action in driving pathology. As established by Wade et al, p53 impairment by MDM2 has the potential to provide a permissive environment for increased proliferation. 31 In our study, this may mechanistically align with the observed Ki-67 expression (proliferation marker) and SOX2 expression (stemness marker) in OLP.
Limitations of the study include its retrospective design and sample size limitations that affected some comparisons. Prospective larger cohort studies should validate these findings and establish the prognostic value of these biomarkers, particularly MDM2.
Conclusion
This study demonstrates that OLP, particularly its erosive variant, possesses a distinctive molecular profile with coordinated expression patterns of MDM2, SOX2, and Ki-67, which is in stark contrast with CLP’s molecular quiescence. The strong biomarker association, with a primary role of MDM2, highlights mechanisms driving proliferation, stemness, and inhibition of tumor suppressors. Supported by genetic and epidemiologic evidence, these findings reaffirm OLP’s malignant potential. Clinically, the assessment of these markers, specifically MDM2 in erosive lesions, could be used to identify high-risk patients who require increased follow-up and oral cancer surveillance, potentially enabling earlier detection and improved outcomes
Footnotes
Author Contributions
MS: Manuscript drafting, Lab experiments, Data analyses. FS: Manuscript drafting. BMa: Manuscript drafting. BR: Manuscript drafting. NHZ: Manuscript drafting, Manuscript revision. AR: Manuscript drafting. AJ: Manuscript revision–Study design. AV: Study supervision–Study design.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon request from corresponding author.*
Code Availability
All codes are available upon request.
AI Use
During the preparation of this manuscript DeepSeek-R1 was used to improve readability and language.